Introduction
Asthma is a common chronic inflammatory disease of
the airways, and is characterized by reversible airflow
obstruction, bronchospasm and various recurring symptoms, including
wheezing, chest tightness, coughing and shortness of breath
(1). Furthermore, asthma affects
both adults and children, and may occur in all populations and
locations across the globe (2).
Statistics showed that approximately 300 million people suffered
from asthma worldwide, and approximately 250,000 annual mortalities
are attributed to asthma, most of which are preventable (3). It has been reported that the prevalence
of asthma in the population aged 0–17 years is 9.5%, which is
higher than that of adults aged 18 and over (7.7%) for the period
2008–2010 in the United States (4).
Additionally, research has also shown that 11% of 12-year-old
schoolchildren may suffer from severe asthma (4). Currently, there are no specific
treatments for asthma and long-term standard treatment may reduce
the recurrence of asthma, but evidence has also suggested that
early intervention is essential for the patients with asthma
(5–8). However, the diagnosis of asthma in
children is difficult and easily misdiagnosed, which may result in
under treatment of asthmatics or overtreatment of transient wheezes
and lead to lung function impairment (9). Therefore, a correct and timely
diagnosis of asthma in children is the first step towards effective
management and treatment of asthma, which may reduce the potential
harm due to misdiagnosis (10).
Previous findings showed that the presence of
inflammation has become one of the most important markers in the
diagnosis of asthma (11). Moreover,
a variety of phenotypes of chronic asthma with persistent
inflammation have been recognized, and a link between bacterial
infections and refractory asthma has emerged (12,13).
Mycoplasma pneumoniae (MP), an extracellular pathogen
lacking a cell wall, is a common causative agent of pneumonia in
children and young adults (14).
Most MP infections are limited to respiratory tract, with 3–10% of
patients developing clinical pneumonia; approximately 25% of
patients with MP infections also suffer a variety of
extra-pulmonary manifestations (15). Although the mechanism of MP
pathogenesis remains to be elucidated, one of the known important
components thereof is the induction of various cytokines and
chemokines (16). Host immune
factors may influence the outcome of infection, and previous
findings showed that asthmatic children were lacking in cellular
and humoral responses to MP infection (17,18). MP
may infect the upper and lower respiratory tract, causing pneumonia
or bronchitis, and may be involved in the initiation and recurrence
of asthma exacerbations (19,20). It
has been suggested that MP infection leads to changes of a variety
of serum immune parameters, such as MP immunoglobulin M (MP-IgM),
MP immunoglobulin E (MP-IgE), interleukin-18, eosinophils (EOS)
count and others (21–23). Prior evidence has also shown that MP
may link to new-onset asthma, exacerbations of asthma, chronic
worsening of asthma and long-term decrements in pulmonary function
(24,25). However, defining a clear relationship
between MP infection and asthma has been difficult, and the precise
role and pathogenic mechanisms of MP in asthma risk are
unclear.
In the current case-control investigation, we
analyzed the serum-specific MP-IgM antibody levels and EOS count in
asthmatic children in order to investigate the association between
MP infection and the risk of asthma among children. Furthermore, we
conducted a meta-analysis to test and verify the results of the
case-control study.
Materials and methods
Ethics statement
The protocol of this study was carried out with the
approval of the Institutional Review Board of Linyi People's
Hospital (Shandong, China). Children were enrolled in this study
after obtaining informed written consents from their parents. All
the study procedures were in line with the Declaration of Helsinki
(26).
Study participants
Between January 2013 and December 2014, a total of
139 children (87 males and 52 females; mean age, 6.65±2.28 years;
range, 0–15 years) previously diagnosed with asthma were recruited
from the Respiratory Care Department of Linyi People's Hospital and
assigned into an experimental group. All the asthma patients were
divided into three groups according to age: Group A (age <3
years, n=42); group B (age range, 3–8 years, n=45) and group C (age
>8 years, n=52). In addition, 115 healthy children (68 males and
47 females; mean age, 6.39±2.34 years; range, 1–12 years), without
any history of respiratory tract infection, from the Medical Center
were enrolled as the control group. The diagnosis of asthma was
based on physician assessment according to the national guidelines
published by the Subspecialty Group of Respiratory Diseases Society
of Pediatrics of Chinese Medical Association in 2008 (27). The disease course of asthma in the
patients was 6–20 days. The inclusion criteria were the following:
i) Patients with recurring wheezing, short breath, chest distress
or cough, which were mostly related to allergen contact, cold air,
physical or chemical stimulation, viral respiratory tract
infections and exercise; ii) patients that had wheezing breath
sounds and a prolonged or interrupted expiratory flow; and iii)
patients that had a notable curative effect on inhaled
bronchodilators. Patients were excluded if they had severe heart
disease, severe pulmonary disease and kidney disease, or had a
history of allergic bronchial asthma. The diagnostic criteria of MP
infection include: MP-IgM antibodies were positive; MP
immunoglobulin G (MP-IgG)-negative antibodies changed into positive
or the IgG antibody titers were elevated >4-fold (28).
Sample collection and detection (serum
MP-IgM expression detection and EOS counting)
Venous blood (2 ml) was drawn in the morning after
an overnight fast at 7th day of the disease course of asthma from
all the children in the experimental and control groups. The
collected samples were centrifuged at 1,500 × g for 15 min to
separate the serum. Enzyme-linked immunosorbent assay (ELISA) was
used to measure the positive rate of MP-IgM in children, using a
Serodia Myco II kit (Fujirebio Inc., Tokyo, Japan). Serum IgM level
(>750 U/ml) was considered to be a positive MP-IgM antibody
level, suggesting MP infection. The EOS count was detected by a
routine blood cell analyzer.
Treatments
Children with MP-IgM negative antibodies received
β-lactam antibiotics (penicillin or cephalosporin). Patients with
acute asthma were treated with bronchodilators or hormone therapy.
Additionally to routine therapy, children with MP-IgM-positive
antibodies received sequential therapy including 10 mg/kg/day
azithromycin. Patients took azithromycin continuously for 3–5 days
until the body temperature dropped. After the clinical symptoms and
signs were largely dissipated, patients were treated with an oral
administration of 10 mg/kg/day azithromycin continuously for 3 days
a week, over a course of 3 weeks. Blood and urine routine
examinations, as well as liver function test were performed during
the administration. When any unusual symptoms appeared, the
medicine causing the effect was stopped.
Serum parameters of MP infection
The positive rate of MP-IgM and EOS count in the
experimental and control groups were recorded. The comparison on
the differences of MP-IgM-positive rate and EOS count between two
groups was performed. The comparison on the differences of
MP-IgM-positive rate and EOS count of asthma patients among the
different age groups was performed.
Statistical analysis
Categorical data are expressed as numbers and
percentages, and were analyzed using χ2 test. Continuous
variables with normal distribution were expressed as mean ±
standard deviation (SD). The t-test was used to measure the
differences between two groups of continuous variables. P<0.05
was considered to indicate a statistically significant
difference.
A comprehensive search was conducted for relevant
studies published in PubMed (1966–2014), Cochrane Library
(2005–2014), Wanfang database (1990–2014), Google Scholar and
Chinese National Knowledge Infrastructure (1990–2014) databases
using the following search terms: (‘Mycoplasma pneumoniae’
or ‘MP’) and (‘asthma’ or ‘bronchial asthma’) and (‘child’ or
‘children’). The references of the eligible articles or textbooks
were also reviewed to check through manual searches to identify
other potential studies. Data from published studies were extracted
independently by two authors to provide the necessary information.
Any disagreement was resolved by discussion between the authors. A
fixed or random effect model was used to measure the odds ratios
(ORs) and its 95% confidence intervals (CIs) to evaluate the
associations between MP infection and asthma. The significance of
the pooled estimate was made using the Z-test (29). Cochran's Q-statistic was applied to
estimate the heterogeneity among studies, and P<0.05 was
considered to be statistically significant (30). The I2 test was also used
to quantify the heterogeneity (range from 0 to 100%) (31). Random-effect model (DerSimonian-Laird
method) was used when P<0.05 or I2 >50%.
Fixed-effects model (Mantel-Haenszel method) was used when there
was no statistical heterogeneity (32). Data for the meta-analysis were
analyzed by the Comprehensive Meta-Analysis version 2.0 software
(Biostat Inc., Englewood, NJ, USA). Begg's funnel plot and Egger's
test were performed to assess the publication bias of articles in
all comparison models.
Results
Baseline characteristics of study
population
Table I shows the
baseline characteristics of subjects in the experimental and
control groups. No significant difference was observed in gender,
age, body mass index (BMI), and exposure to environmental tobacco
smoke (ETS) between children with asthma and healthy controls (all
P>0.05). Children with asthma had a higher rate of family
history of asthma when compared with the control group, but with no
significant difference (14.4 vs. 7.0%, P=0.060). Furthermore, the
rates of children in urban families and the rate of exposure to
dust in the experimental group were higher than those in the
control group, but with no significant difference (urban family:
61.2 vs. 53.9%, P=0.245; exposure to dust: 23.7 vs. 20.9%,
P=0.418).
 | Table I.The demographic characteristics of
the children with asthma and healthy controls. |
Table I.
The demographic characteristics of
the children with asthma and healthy controls.
| Groups | Case group
(n=139) | Control group
(n=115) | P-value |
|---|
| Gender (M/F) | 87/52 | 68/47 | 0.574 |
| Age (years) | 6.65±2.28 | 6.39±2.34 | 0.372 |
| BMI
(kg/cm2) | 19.8±2.1 | 20.2±2.5 | 0.167 |
| ETS, n (%) | 91 (65.5%) | 66 (57.4%) | 0.187 |
| Family history of
asthma, n (%) | 20 (14.4%) | 8 (7.0%) | 0.060 |
| Urban family, n
(%) | 85 (61.2%) | 62 (53.9%) | 0.245 |
| Exposure to dust
environment, n (%) | 33 (23.7%) | 24 (20.9%) | 0.418 |
Positive rate of serum IgM
antibodies
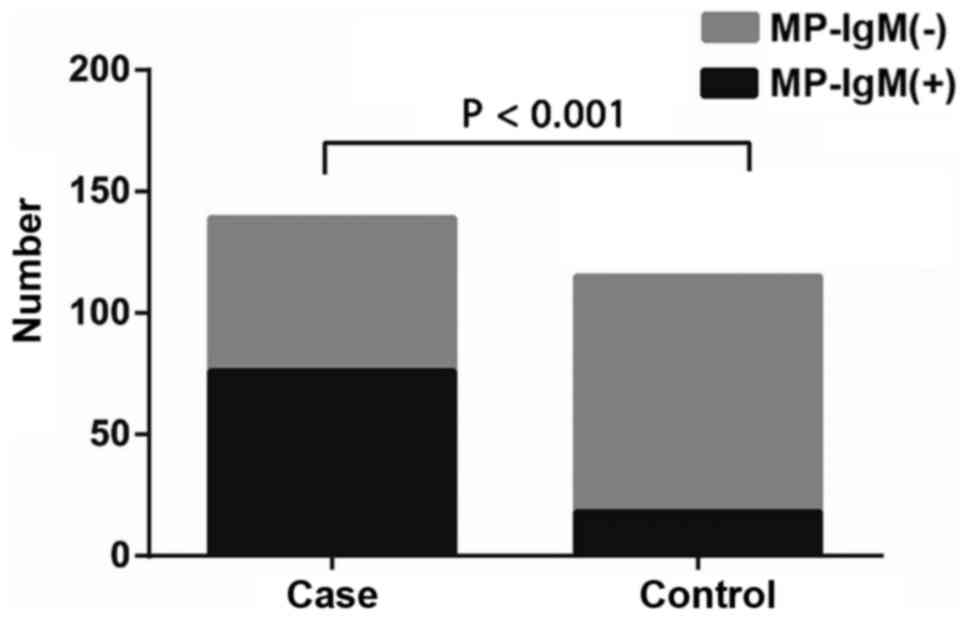
Of all subjects, 54.7% (76/139) of asthma patients
and 15.7% (18/115) of the control group were found to be positive
for MP-IgM antibodies. The positive rate of MP-IgM in the
experimental group was significantly higher than that in the
control group (54.7 vs. 15.7%, χ2 41.11, P<0.001)
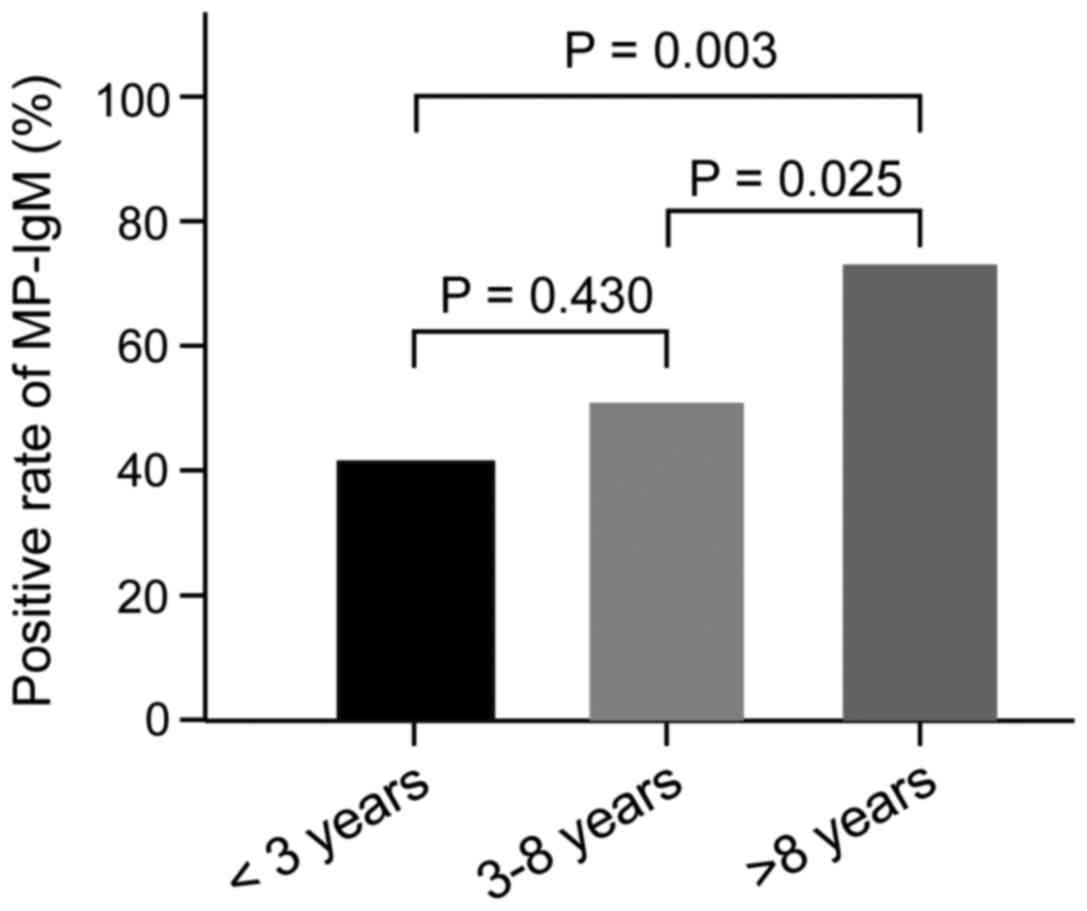
(Fig. 1). ELISA results showed that
17 (40.5%) patients in group A, 22 (48.9%) patients in group B and
37 (71.2%) patients in group C were detected to be MP-IgM
antibody-positive. There was no significant difference in the
positive rate of MP-IgM between groups A and B (40.5 vs. 48.9%,
χ2 0.62, P=0.430). However, the positive rates of MP-IgM
in groups A and B were significantly lower than those in group C,
respectively (group A vs. group C: 40.5 vs. 71.2%,
χ2=8.95, P=0.003; group B vs. group C: 48.9 vs. 71.2%,
χ2=5.02, P=0.025) (Fig.
2).
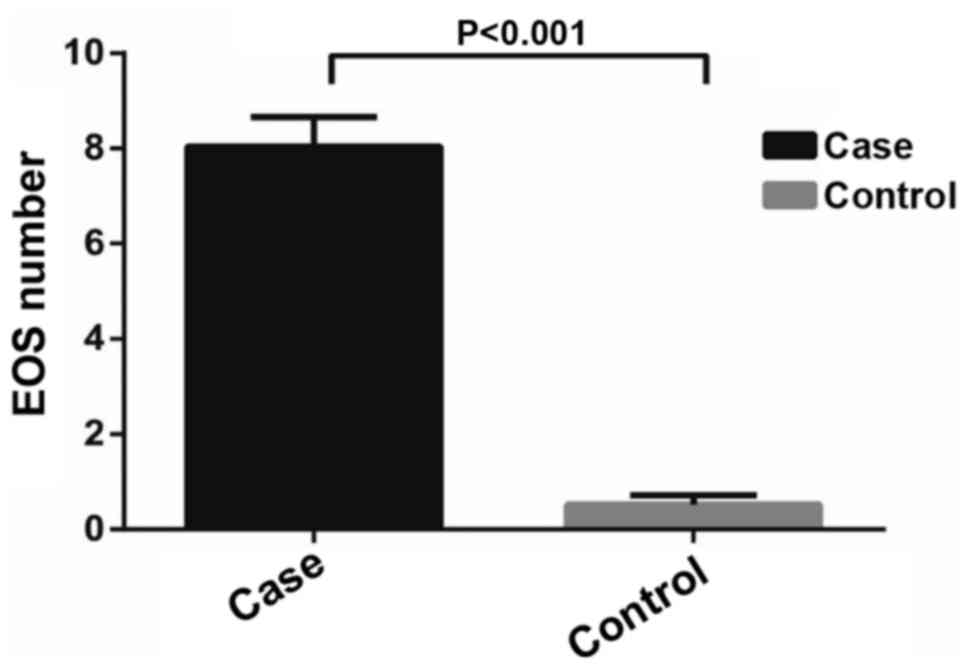
Association of EOS count with asthma
risk
The results showed that the blood EOS count in
asthma patients was markedly higher than those in healthy controls
(8.04±0.62 109/l vs. 0.52±0.20 109/l,
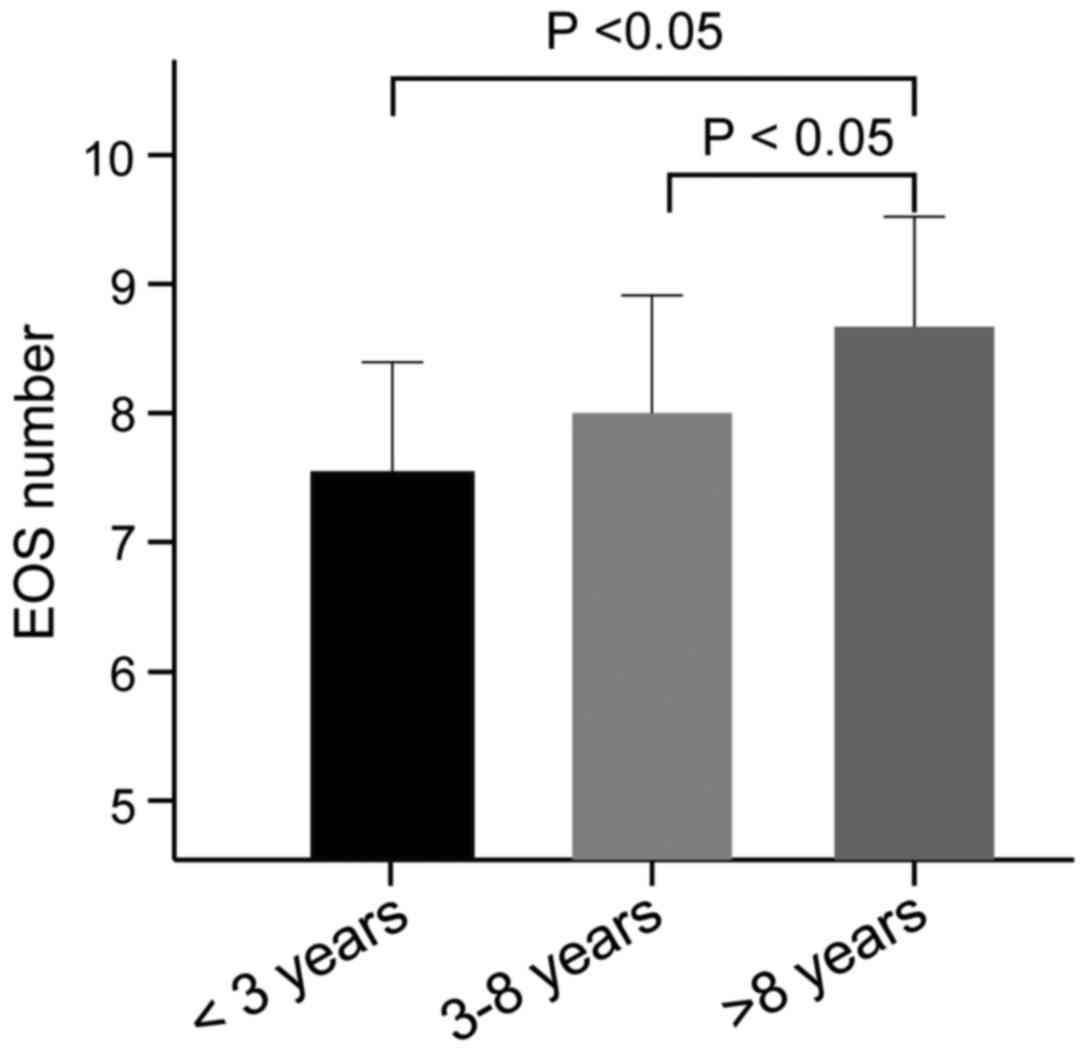
t=124.8, P<0.001) (Fig. 3).
According to the different age groups of asthma patients, we found
that the blood EOS count in groups A, B and C was (7.56±1.62)
109/l, (8.01±1.32) 109/l and (8.65±1.09)
109/l, respectively. No significant difference in the
blood EOS count was observed between groups A and B (t=1.43,
P=0.158). Nevertheless, the blood EOS count in groups A and B were
significantly lower than that in group C, respectively (group A vs.
C: t=3.89, P<0.05; group B vs. C: t=2.62, P<0.05) (Fig. 4).
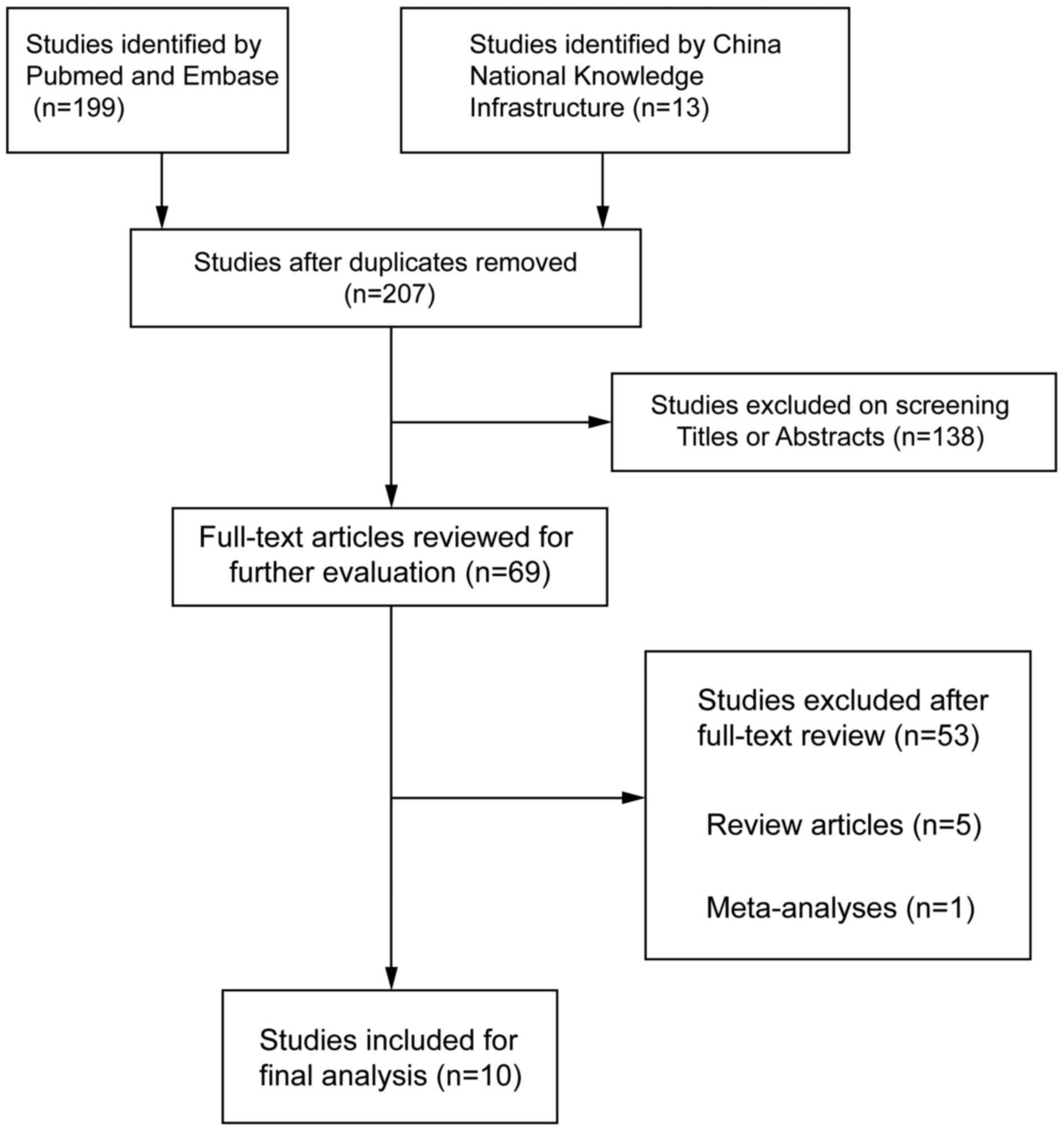
Results of meta-analysis
A total of 207 articles associated with the searched
keywords were identified. Of these studies, 138 were excluded based
on the titles and abstracts; another 59 studies were eliminated
after reviewing the full text. Eventually, 10 studies met our
inclusion criteria for this meta-analysis (25,33–41):
H.-E. Zeng-Hong, Correlation Between Mycoplasma Pnenumonia
Infection and Pediatric Asthma, 2011; Jiang Hua, Mycoplasma
pneumoniae Infection and Bronchial Asthma in Children, 2013;
Zhao Zhi-Yun, Observation on Infection Results and Correlation
Between Childhood Asthma and Mycoplasma pneumoniae, 2014;
Liu Chunxiang, Association of Mycoplasma pneumoniae
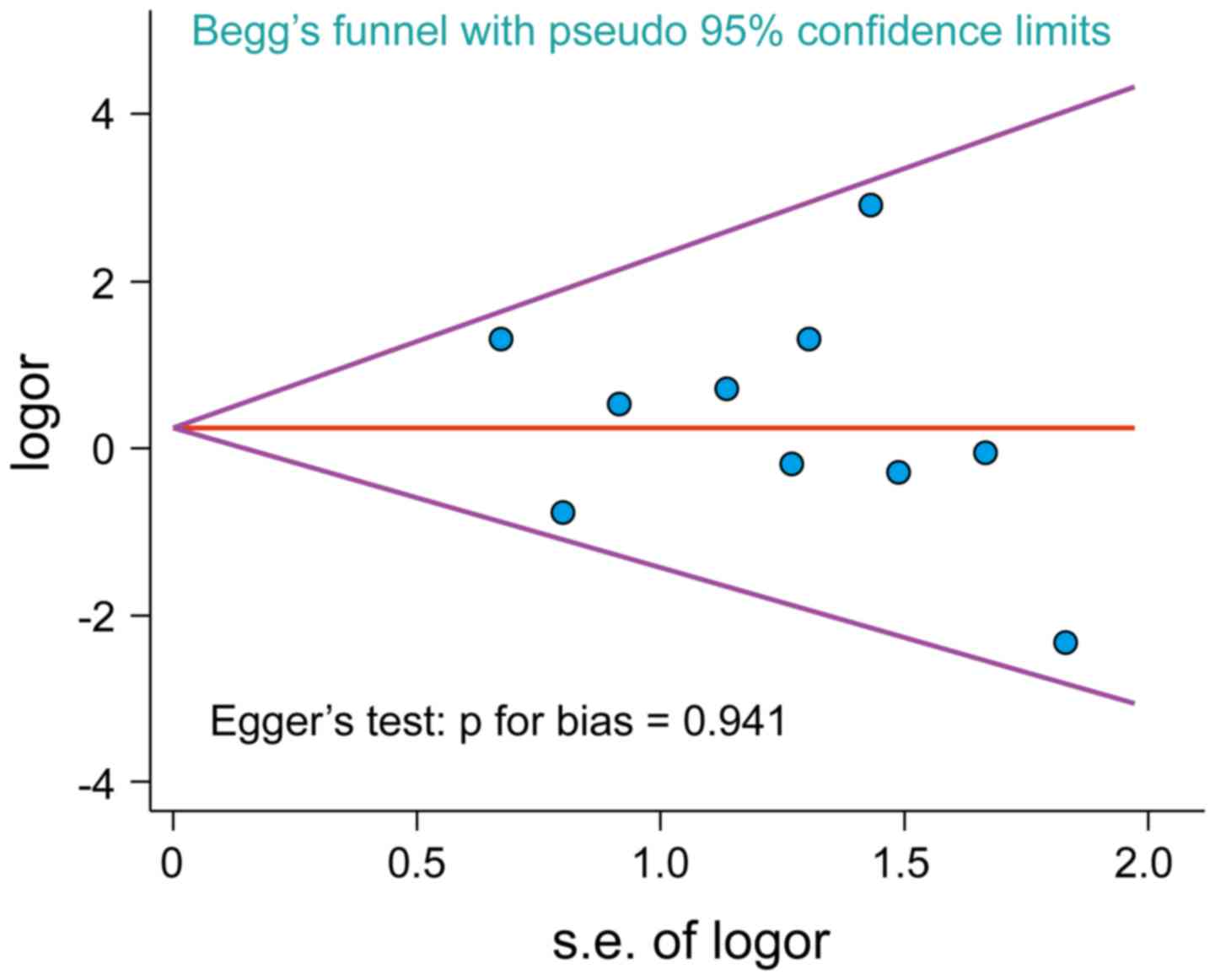
Infection and Pediatric Asthma, 2009) (Fig. 5). Egger's test and Begg's funnel plot
were used to statistically assess the funnel plot symmetry. The
results suggested no evidence of publication bias for the included
10 studies (Fig. 6). These 10
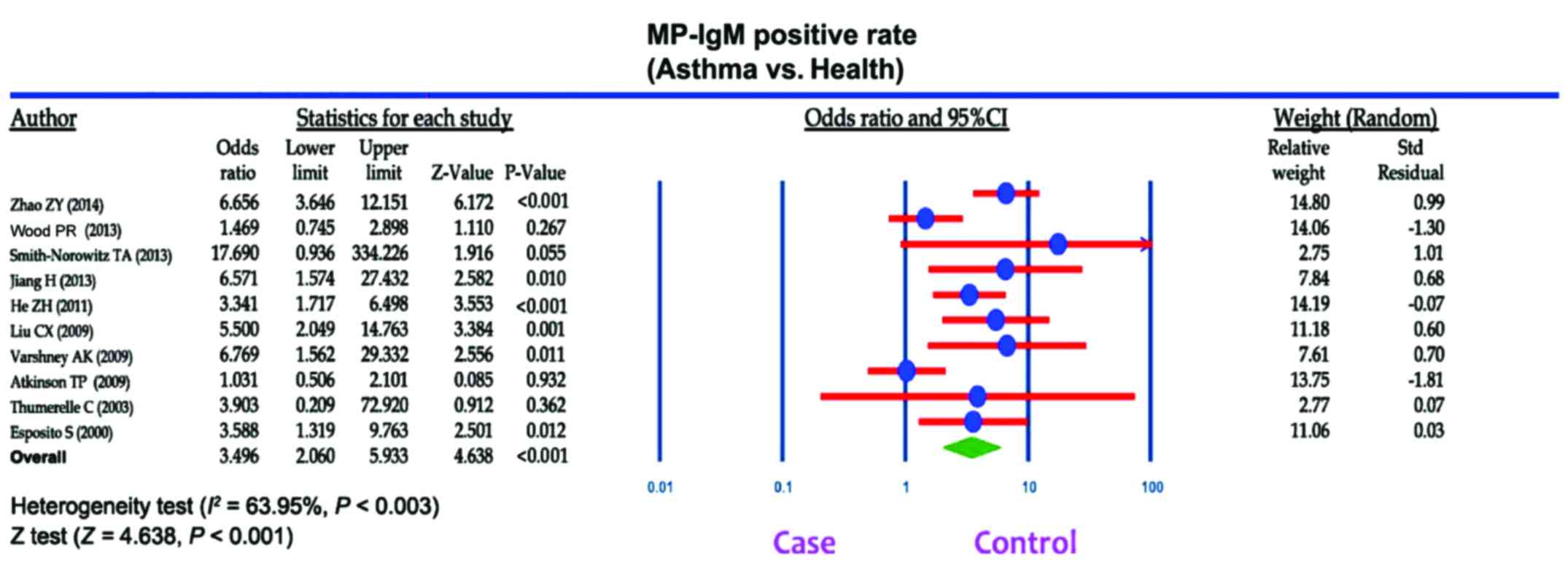
case-control studies were composed of 795 asthma patients and 630
healthy controls. Publication year of articles included ranged from
2000 to 2014. There was significant heterogeneity observed
(I2=63.95%, Ph<0.05); thereby the random
effects model was carried out. Meta-analysis results showed that
the MP-IgM-positive rate in asthma patients were markedly higher
than that of healthy controls (OR=3.496, 95% CI=2.060–5.933,
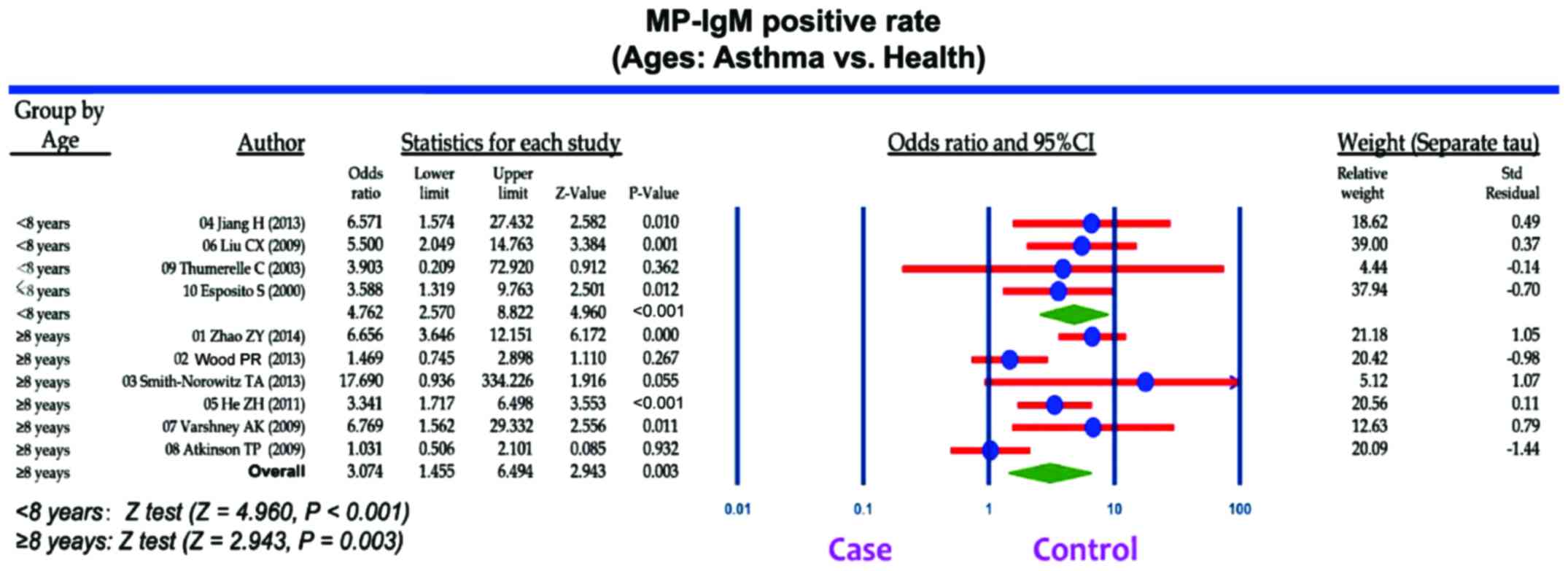
P<0.001) (Fig. 7). Age-stratified
analysis presented that the MP-IgM-positive rate in both children
≥8 and <8 years were significantly higher than that of healthy
controls (average age, ≥8 years: OR=3.074, 95% CI=1.455–6.494,
P=0.003; average age, <8 years: OR=4.762, 95% CI=2.570–8.822,
P<0.001) (Fig. 8).
Discussion
MP is a highly specialized bacterium that functions
as an obligate parasite in the respiratory tract of humans, which
may be involved in establishing a chronic infection (36). Furthermore, research has shown that
MP infects the upper and lower respiratory tract which may be
associated with the occurrence of bronchitis and asthma; however,
the underlying mechanism is not completely understood (42,43). In
this regard, we performed a case-control study and a meta-analysis
to explore the correlation of MP infection with the increased risk
of asthma. This study found that MP-IgM-positive rate was higher in
asthmatic children when compared with healthy controls, indicating
that elevated MP-IgM-positive rate may be involved in the
development of asthma among children. Generally, the elevated
MP-IgM-positive rate can be used as an early diagnostic criterion
of the initial acute MP infection (44). As a specific antigen, MP can induce
immediate or delayed hypersensitivity reaction, and may result in
allergic airway inflammation and induce the production of IgE and
IgM, which may mediate type 1 allergic reaction. Therefore, MP may
lead to the development of asthma (45). Additionally, MP infection is
associated with significant specific IgM responses in addition to
specific IgG and IgE responses; thus, the production of specific
MP-IgM may have a role in the exacerbation of asthma (17,46).
High positive levels of MP-IgM antibodies were found in patients
who were infected with MP during asthma exacerbation (37). We suspected that the possible
explanations of how MP affects the airway included the production
of specific MP-IgM antibodies in addition to direct effects on
airway epithelium, inflammatory reaction on airways and alteration
in the autonomic nervous system (36). Smith-Norowitz et al found that
the IgM-positivity was apparently higher in asthmatic patients as
compared to the healthy controls, and suggested that the increased
specific MP-IgM responses may play an important role in MP
infection in asthma development (35). Previous report by Varshney et
al highlighted that MP may play a crucial role in the onset of
asthma in predisposed children and be a trigger for recurrent
wheezing (37). Consistent with
previous studies, our study also demonstrated that the MP infection
accompanied with higher MP-IgM-positive rate may be involved in the
development of asthma. Additionally, we conducted a meta-analysis
to confirm the associations and found that the asthmatic children
had a higher MP-IgM-positive rate, indicating that a higher
MP-IgM-positive rate may be associated with an increased
susceptibility to asthma.
Another important finding in our study revealed that
the levels of EOS in asthmatic children were significantly higher
than those in the non-asthmatic controls. This leads us to believe
that patients with asthma may suffer from allergy inflammation and
the elevated EOS count may be crucial in the pathogenesis of
asthma. EOS is thought to have a key pro-inflammatory role in the
pathogenesis of asthma as its mediators are identified in
asthmatic, but not healthy lungs. The suppression of eosinophil
infiltration in various clinical diseases by glucocorticoids may be
correlated with an amelioration of symptoms and disordered airway
function (47). Characterized as an
eosinophilic airway inflammation, asthma is often considered to be
associated with a higher peripheral blood EOS count, and the EOS
may play an important role in the pathogenesis of bronchial asthma
(48,49). Additionally, airway
hyper-responsiveness has been reported to be closely correlated
with the presence of EOS (50,51).
Early studies found that the respiratory tract infections with a
higher EOS count had a higher risk of asthma when compared with the
respiratory tract infectors with normal EOS count, suggesting that
the EOS count is an important clinical index in predicting the
development of asthma (52,53). Furthermore, we found that the
asthmatic children aged >8 years had higher MP-IgM-positive rate
and EOS count as compared to the asthmatic children aged <3
years and asthmatic children aged 3–8 years. We suspected that
these differences may be correlated with the clinically significant
alterations in lung function. However, the underlying mechanism
involved remains unclear; therefore, further studies based on the
involvement of mechanistic pathways in asthma in children of
different ages should be conducted.
In conclusion, the present study suggests that
asthmatic children have a higher MP-IgM-positive rate and EOS count
when compared with non-asthmatic controls, indicating that MP
infection may promote the production of IgM in asthmatic children.
Deficient host defense mechanisms in children with asthma may
contribute to a higher prevalence of MP-IgM, which likely reflects
an increased susceptibility to asthma. However, with our own
limitations, such as small sample size and the inclusion and
exclusion criterion of the meta-analysis may affect the statistical
power of this study. Future large-scale prospective studies are
needed to confirm the correlations and predictive value of MP
infection with asthma risk.
Acknowledgements
We would like to acknowledge the reviewers for their
helpful comments on this study.
References
|
1
|
Urbano FL: Review of the NAEPP 2007 Expert
Panel Report (EPR-3) on Asthma Diagnosis and Treatment Guidelines.
J Manag Care Pharm. 14:41–49. 2008.PubMed/NCBI
|
|
2
|
Centers for Disease Control and Prevention
(CDC): Vital signs: asthma prevalence, disease characteristics, and
self-management education: United States, 2001 - 2009. MMWR Morb
Mortal Wkly Rep. 60:547–552. 2011.PubMed/NCBI
|
|
3
|
Croisant S: Epidemiology of asthma:
prevalence and burden of disease. Adv Exp Med Biol. 795:17–29.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Akinbami LJ, Moorman JE, Bailey C, Zahran
HS, King M, Johnson CA and Liu X: Trends in asthma prevalence,
health care use, and mortality in the United States, 2001–2010.
NCHS Data Brief. 1–8. 2012.PubMed/NCBI
|
|
5
|
Holgate ST: A look at the pathogenesis of
asthma: the need for a change in direction. Discov Med. 9:439–447.
2010.PubMed/NCBI
|
|
6
|
Corren J, Lemanske RF Jr, Hanania NA,
Korenblat PE, Parsey MV, Arron JR, Harris JM, Scheerens H, Wu LC,
Su Z, et al: Lebrikizumab treatment in adults with asthma. N Engl J
Med. 365:1088–1098. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hafkamp-de Groen E, Mohangoo AD, de
Jongste JC, van der Wouden JC, Moll HA, Jaddoe VW, Hofman A, de
Koning HJ and Raat H: Early detection and counselling intervention
of asthma symptoms in preschool children: study design of a cluster
randomised controlled trial. BMC Public Health. 10:5552010.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
National Asthma Education and Prevention
Program: Expert Panel Report 3 (EPR-3): Guidelines for the
Diagnosis and Management of Asthma-Summary Report 2007. J Allergy
Clin Immunol. 120:(Suppl 5). S94–S138. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cave AJ and Atkinson LL: Asthma in
preschool children: a review of the diagnostic challenges. J Am
Board Fam Med. 27:538–548. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Busse WW: Asthma diagnosis and treatment:
filling in the information gaps. J Allergy Clin Immunol.
128:740–750. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dahlén SE, Dahlén B and Drazen JM: Asthma
treatment guidelines meet the real world. N Engl J Med.
364:1769–1770. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Locksley RM: Asthma and allergic
inflammation. Cell. 140:777–783. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Busse WW: The relationship of airway
hyperresponsiveness and airway inflammation: Airway
hyperresponsiveness in asthma: its measurement and clinical
significance. Chest. 138:(Suppl 2). 4S–10S. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bébéar C, Pereyre S and Peuchant O:
Mycoplasma pneumoniae: susceptibility and resistance to
antibiotics. Future Microbiol. 6:423–431. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Khan FY and Sayed H: Rhabdomyolysis
associated with Mycoplasma pneumoniae pneumonia. Hong Kong
Med J. 18:247–249. 2012.PubMed/NCBI
|
|
16
|
van der Poll T and Opal SM: Pathogenesis,
treatment, and prevention of pneumococcal pneumonia. Lancet.
374:1543–1556. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Waites KB, Balish MF and Atkinson TP: New
insights into the pathogenesis and detection of Mycoplasma
pneumoniae infections. Future Microbiol. 3:635–648. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Narita M: Pathogenesis of extrapulmonary
manifestations of Mycoplasma pneumoniae infection with
special reference to pneumonia. J Infect Chemother. 16:162–169.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hong SJ: The role of Mycoplasma
pneumoniae infection in asthma. Allergy Asthma Immunol Res.
4:59–61. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Watanabe H, Uruma T, Nakamura H and
Aoshiba K: The role of Mycoplasma pneumoniae infection in
the initial onset and exacerbations of asthma. Allergy Asthma Proc.
35:204–210. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wang M, Wang Y, Yan Y, Zhu C, Huang L,
Shao X, Xu J, Zhu H, Sun X, Ji W, et al: Clinical and laboratory
profiles of refractory Mycoplasma pneumoniae pneumonia in
children. Int J Infect Dis. 29:18–23. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wenzel S, Ford L, Pearlman D, Spector S,
Sher L, Skobieranda F, Wang L, Kirkesseli S, Rocklin R, Bock B, et
al: Dupilumab in persistent asthma with elevated eosinophil levels.
N Engl J Med. 368:2455–2466. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Schleich FN, Seidel L, Sele J, Manise M,
Quaedvlieg V, Michils A and Louis R: Exhaled nitric oxide
thresholds associated with a sputum eosinophil count ≥3% in a
cohort of unselected patients with asthma. Thorax. 65:1039–1044.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Atkinson TP and Waites KB: Mycoplasma
pneumoniae infections in childhood. Pediatr Infect Dis J.
33:92–94. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wood PR, Hill VL, Burks ML, Peters JI,
Singh H, Kannan TR, Vale S, Cagle MP, Principe MF, Baseman JB, et
al: Mycoplasma pneumoniae in children with acute and
refractory asthma. Ann Allergy Asthma Immunol. 110:328–334. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Holt GR: Declaration of Helsinki - the
world's document of conscience and responsibility. South Med J.
107:4072014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Subspecialty Group of Respiratory Diseases
Society of Pediatrics; Chinese Medical Association; Chinese Journal
of Pediatrics Editorial Board: Guideline for the diagnosis and
optimal management of asthma in children. Zhonghua Er Ke Za Zhi.
46:745–753. 2008.(In Chinese). PubMed/NCBI
|
|
28
|
Zhang YM and Liu XY: Advance in the
diagnosis and treatment of Mycoplasma pneumoniae pneumonia
and related complications. Zhongguo Dang Dai Er Ke Za Zhi.
13:358–360. 2011.(In Chinese). PubMed/NCBI
|
|
29
|
Chen H, Manning AK and Dupuis J: A method
of moments estimator for random effect multivariate meta-analysis.
Biometrics. 68:1278–1284. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Jackson D, White IR and Riley RD:
Quantifying the impact of between-study heterogeneity in
multivariate meta-analyses. Stat Med. 31:3805–3820. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Peters JL, Sutton AJ, Jones DR, Abrams KR
and Rushton L: Comparison of two methods to detect publication bias
in meta-analysis. JAMA. 295:676–680. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zintzaras E and Ioannidis JP:
Heterogeneity testing in meta-analysis of genome searches. Genet
Epidemiol. 28:123–137. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Atkinson TP, Duffy LB, Pendley D, Dai Y
and Cassell GH: Deficient immune response to Mycoplasma
pneumoniae in childhood asthma. Allergy Asthma Proc.
30:158–165. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Esposito S, Blasi F, Arosio C, Fioravanti
L, Fagetti L, Droghetti R, Tarsia P, Allegra L and Principi N:
Importance of acute Mycoplasma pneumoniae and Chlamydia
pneumoniae infections in children with wheezing. Eur Respir J.
16:1142–1146. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Smith-Norowitz TA, Silverberg JI,
Kusonruksa M, Weaver D, Ginsburg D, Norowitz KB, Durkin HG,
Hammerschlag MR, Bluth MH and Kohlhoff SA: Asthmatic children have
increased specific anti-Mycoplasma pneumoniae IgM but not
IgG or IgE-values independent of history of respiratory tract
infection. Pediatr Infect Dis J. 32:599–603. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Thumerelle C, Deschildre A, Bouquillon C,
Santos C, Sardet A, Scalbert M, Delbecque L, Debray P, Dewilde A,
Turck D, et al: Role of viruses and atypical bacteria in
exacerbations of asthma in hospitalized children: a prospective
study in the Nord-Pas de Calais region (France). Pediatr Pulmonol.
35:75–82. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Varshney AK, Chaudhry R, Saharan S, Kabra
SK, Dhawan B, Dar L and Malhotra P: Association of Mycoplasma
pneumoniae and asthma among Indian children. FEMS Immunol Med
Microbiol. 56:25–31. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
He ZH, Zhang JT and Sun YF: Correlation
between mycoplasma pnenumonia infection and pediatric asthma. Chin
J Nosocomiol. 21:4733–4734. 2011.(In Chinese).
|
|
39
|
Jiang H: Mycoplasma pneumoniae
infection and bronchial asthma in children. Chin J Med Guide.
15:1275–1276. 2013.(In Chinese).
|
|
40
|
Liu CX: Analysis of the relationship
between bronchial asthma and Mycoplasma pneumoniae
infection. Chin J Postgrad Med. 32:49–50. 2009.(In Chinese).
http://d.g.wanfangdata.com.cn/Periodical_ysjxzz200915022.aspx
|
|
41
|
Zhao ZY: Observation on infection results
and correlation between childhood asthma and Mycoplasma
pneumoniae. J Clin Pulm Med. 8:1497–1498, 1522. 2014.(In
Chinese).
|
|
42
|
Guilbert TW and Denlinger LC: Role of
infection in the development and exacerbation of asthma. Expert Rev
Respir Med. 4:71–83. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Rollins DR, Beuther DA and Martin RJ:
Update on infection and antibiotics in asthma. Curr Allergy Asthma
Rep. 10:67–73. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Ke LQ, Wang FM, Li YJ and Luo YC:
Epidemiological characteristics of Mycoplasma pneumoniae
pneumonia in children. Zhongguo Dang Dai Er Ke Za Zhi. 15:33–36.
2013.(In Chinese). PubMed/NCBI
|
|
45
|
Burton OT and Oettgen HC: Beyond immediate
hypersensitivity: evolving roles for IgE antibodies in immune
homeostasis and allergic diseases. Immunol Rev. 242:128–143. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Defilippi A, Silvestri M, Tacchella A,
Giacchino R, Melioli G, Di Marco E, Cirillo C, Di Pietro P and
Rossi GA: Epidemiology and clinical features of Mycoplasma
pneumoniae infection in children. Respir Med. 102:1762–1768.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Green RH, Brightling CE, McKenna S,
Hargadon B, Parker D, Bradding P, Wardlaw AJ and Pavord ID: Asthma
exacerbations and sputum eosinophil counts: a randomised controlled
trial. Lancet. 360:1715–1721. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Fleming L, Wilson N, Regamey N and Bush A:
Use of sputum eosinophil counts to guide management in children
with severe asthma. Thorax. 67:193–198. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Nakagome K and Nagata M: Pathogenesis of
airway inflammation in bronchial asthma. Auris Nasus Larynx.
38:555–563. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
van Rensen EL, Evertse CE, van Schadewijk
WA, van Wijngaarden S, Ayre G, Mauad T, Hiemstra PS, Sterk PJ and
Rabe KF: Eosinophils in bronchial mucosa of asthmatics after
allergen challenge: effect of anti-IgE treatment. Allergy.
64:72–80. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Tantisira KG, Colvin R, Tonascia J, Strunk
RC, Weiss ST and Fuhlbrigge AL: Childhood Asthma Management Program
Research Group: Airway responsiveness in mild to moderate childhood
asthma: sex influences on the natural history. Am J Respir Crit
Care Med. 178:325–331. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Apter AJ: Advances in adult asthma
diagnosis and treatment and HEDQ in 2010. J Allergy Clin Immunol.
127:116–122. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Laviolette M, Gossage DL, Gauvreau G,
Leigh R, Olivenstein R, Katial R, Busse WW, Wenzel S, Wu Y, Datta
V, et al: Effects of benralizumab on airway eosinophils in
asthmatic patients with sputum eosinophilia. J Allergy Clin
Immunol. 132:1086–1096. 2013. View Article : Google Scholar : PubMed/NCBI
|