Introduction
Asthma is a common, chronic heterogeneous
respiratory disease affecting 1–18% of the population worldwide; in
China it has a prevalence of 1.24% (1,2).
Characterized by variable symptoms of wheezing, shortness of
breath, chest tightness and/or cough, and by variable expiratory
airflow limitation, asthma can be subdivided into four
subcategories according to the severity of symptoms and airflow
limitation, including mild intermittent, mild persistent, moderate
persistent and severe persistent (2,3).
Although 50–75% of asthma patients are categorized
as having mild asthma, few studies have focused on these subtypes,
particularly mild intermittent asthma (4). From the earliest to the latest
guidelines, short acting β2-agonist (SABA) as required is the only
treatment recommended for patients with mild intermittent asthma,
which is mostly based on expert opinions (2,5).
However, studies have shown that airway inflammation was also
detected in patients with mild intermittent asthma, which may cause
airway remodeling and disease progression (6,7). This
lead us to theorize the benefits and risks of the most important
controller medication to date, inhaled corticosteroid (ICS), in
these patients.
Hence the present meta-analysis aimed to analyze the
effects of ICS on lung function, airway hyper-responsiveness (AHR),
symptom control, airway inflammation and adverse effects in
patients with mild intermittent asthma.
Materials and methods
Study selection criteria
Our inclusion criteria for considering studies for
this review were as follows: i) Randomized controlled trials (RCT);
ii) studies assessing patients with intermittent asthma that may be
defined as using SABA only, few symptoms (daytime symptoms ≤2
times/week and nocturnal symptoms ≤2 times/month), forced
expiratory volume in 1 sec (FEV1) predicted ≥80%, and peak
expiratory flow (PEF) variability ≤20%. For studies only describing
some of these criteria and not implying other types of asthma,
three independent researchers discussed and came to an agreement
whether this study should be included; iii) ICS as the intervention
compared with placebo or other therapies or ICS in combination with
other therapies vs. other therapies alone; and iv) outcomes of
studies reflecting lung function, AHR, airway inflammation, symptom
control or adverse effects of the drugs in patients with
intermittent asthma.
Exclusion criteria
We excluded studies that recruited mixed groups of
participants (patients with mild intermittent and persistent
asthma) and those that did not report the outcomes separately.
Search strategy and study
selection
MEDLINE (https://www.ncbi.nlm.nih.gov/pubmed) and EMBASE
(https://www.embase.com/) databases were initially
searched from inception to June 2016 using the following terms: i)
‘asthma’ OR ‘antiasthma’ OR ‘anti asthma’ OR ‘respiratory sounds’
OR ‘wheez’ OR ‘bronchial spasm’ OR ‘bronchospasm’ OR (‘bronch’ AND
‘spasm’) OR ‘bronchoconstrict’ OR ‘bronchoconstriction’ OR
(‘bronch’ AND ‘constrict’) OR (‘bronchial hyperreactivity’ AND
‘respiratory hypersensitivity’) OR (‘bronchial’ OR ‘respiratory’ OR
‘airway’ OR ‘lung’ AND (‘hypersensitive’ OR ‘hyperreactiv’ OR
‘allerg’ OR ‘insufficiency’) OR (‘dust’ OR ‘mite’ AND (‘allerg’ OR
‘hypersensitiv’); ii) ‘inhaled’ AND ‘corticosteroid’ OR
‘beclometasone’ OR ‘budesonide’ OR ‘ciclesonide’ OR ‘fluticasone’
OR ‘mometasone’ OR ‘triamcinolone’ OR ‘ics’; and iii) ‘mild’ OR
‘intermittent’ OR ‘infrequent’; iv) combination of points i, ii and
iii mentioned above; iv) combination of point iv mentioned above
and ‘randomized controlled trial’.
China National Knowledge Internet (CKNI) database
was also searched from inception to June 2016 using Chinese terms
matched to the English terms outlined. Abstracts of citations
resulting from this search were imported into a bibliographic
database and hand-searched by two reviewers for duplicate
publications, which were removed. Citations were initially excluded
if it was clear that the study: i) Was not concerned with the
treatment of chronic mild asthma in humans; ii) was not an RCT or
iii) did not include a treatment arm with ICS.
Where uncertainty existed, the full text version of
the publication was retrieved, and more detailed checks were
conducted against our eligibility criteria. A third researcher
evaluated the decision of inclusion or exclusion in discussion with
the two reviewers. We also manually searched through the systematic
reviews for any other articles that may be potentially
suitable.
Study characteristics and data
extraction
We used preformatted tables to record study design
and participant characteristics, description of mild intermittent
asthma, pharmacological agent (dose, device and frequency), and
duration of follow-up. Two reviewers independently extracted data
on relevant outcomes, including FEV1, forced vital capacity
(FEV1/FVC), the concentration of methacholine when there was a fall
in FEV1 ≥20% (PC20 FEV1), fractional exhaled nitric oxide (FeNO),
number or percentage of sputum eosinophil and drug-related adverse
effects. If an intention-to-treat analysis was not used by the
researchers, and it was not shown in the results how many
participants were in each group at the time of the final evaluation
of that outcome, the number of patients in each group was
calculated by subtracting the number of patients who discontinued
or were lost to follow-up from those randomized to each group. Any
discrepancies were resolved through the involvement of a third
reviewer after rechecking the source papers.
Assessment of risk of bias
Two reviewers independently assessed the
methodological quality of the included studies. The risk of bias
was evaluated using the Jadad scale of 0–5 (8). Funnel plots were used to assess
publication bias and sensitivity analyses were conducted using the
highest quality studies (Jadad score ≥3).
Statistical analysis
A pooled treatment effect across trials was
calculated using RevMan 5.1.6 (Cochrane, UK). For continuous
outcomes, a weighted mean difference (WMD) or standardized mean
difference (SMD) was calculated, as appropriate. For dichotomous
outcomes, a relative risk (RR) was calculated. Pooled treatments
effects were expressed with their 95% confidence intervals (95%
CI). Heterogeneity of effect size across pooled studies was
calculated. P<0.05 was considered to indicate a statistically
significant difference.
Statistical heterogeneity was assessed using the
I2 statistic with I2>50% indicating a
substantial level of heterogeneity. In accordance with the
recommendations of the Cochrane Handbook, we derived any standard
deviations from 95% CIs or P-values (8). Measures of AHR, such as the provocative
concentration of challenge substance required to produce 20% fall
in FEV1 (PC20 FEV1) was often reported as geometric means, and data
for such outcomes was pooled after the data was log
transformed.
Sensitivity analyses were performed on the basis of
methodological quality. Results were re-analyzed using studies of
only the highest quality (Jadad scores 3–5). Subgroup analyses
based on ICS treatment duration and patient age (children or
adults) were conducted.
Results
Study characteristics and search
results
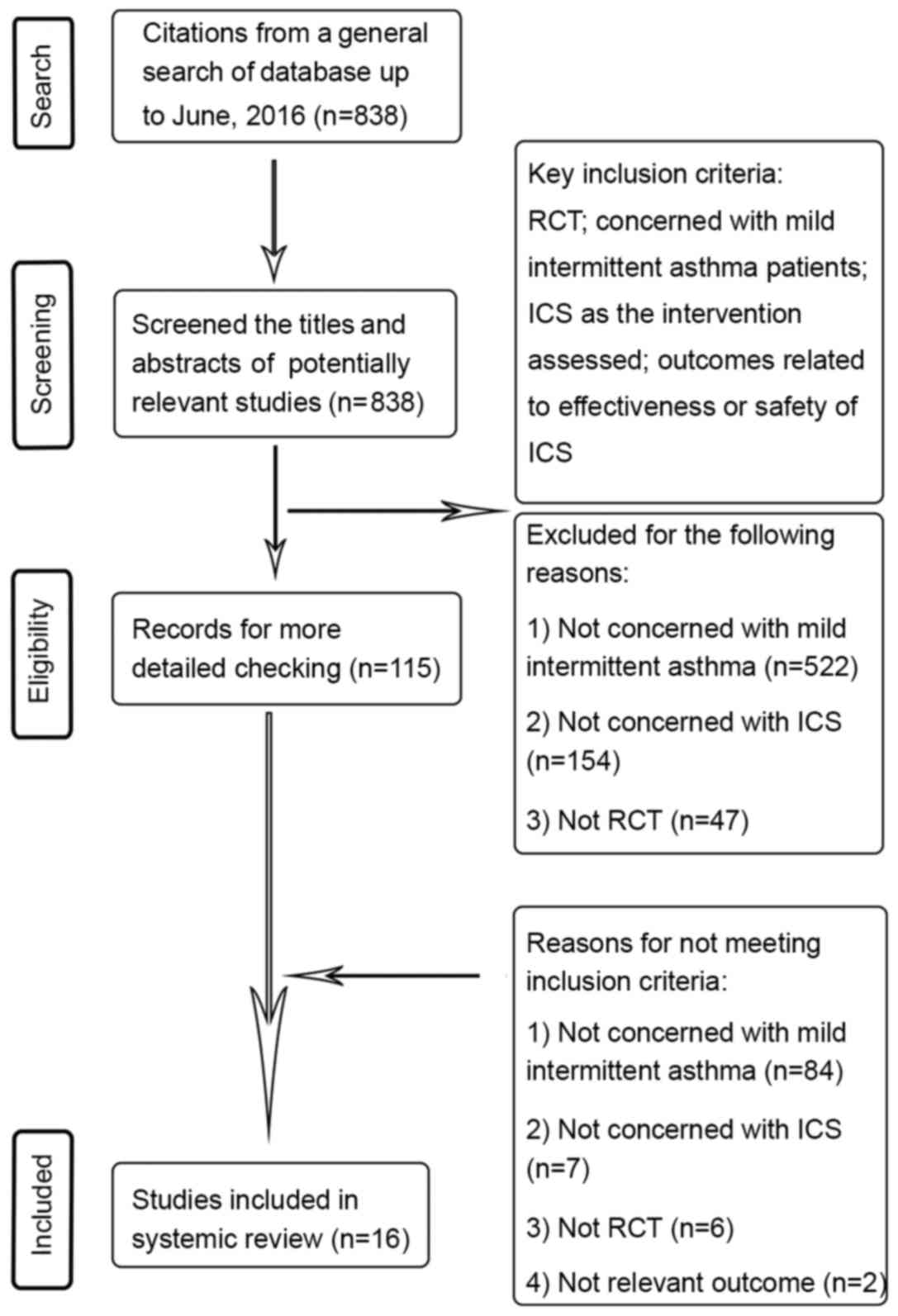
In total, 838 potentially relevant articles were
screened and 16 studies were included in this systemic review. The
process of study selection is shown in Fig. 1. Of all the included studies, only
one study (9) was conducted in
children and the remaining 15 studies were conducted in adults
(10–24). At the time of enrollment, the
patients of the majority of studies were not treated with
corticosteroids regularly. The ICS used in these studies included
budesonide (BUD; 7 studies), fluticasone propionate (FP; 5
studies), and beclometasone dipropionate (BDP; 4 studies). The
characteristics of studies are shown in Table I.
 | Table I.Characteristics of the included
studies. |
Table I.
Characteristics of the included
studies.
| Author/(Refs.)
year | Location | Inclusion
criteria | Intervention | Treatment
duration | Male patients
(%) | Mean age
(years) | Mean FEV1%
predicted | Non.smoker patients
(%) |
|---|
| Jatakanon et
al (10), 1999 | Imperial College
School of Medicine at National Heart and Lung Institute, UK | i) Non-smoking
stable allergic asthmatic patients who required only short-acting
β-agonist; ii) history of intermittent wheezing and chest
tightness | i) BUD: 100 µg
daily (n=8); ii) BUD: 400 µ daily (n=7); iii) BUD: 1,600 µ (n=10);
iv) placebo (n=6). Delivery method: Turbohaler DPI. Parallel and
crossover design. | 4 weeks | 74.2 | 29.9 | 93.4 | 100.0 |
| Boulet et al
(11), 2009 | Multicenter
Canada | i) Mild asthma; ii)
use of a short-acting µ2-agonist alone (<3 times/week) | i) FP: 3-month
course of 250 µg/day followed by 9-month maintenance treatment of
100 µg/day (n=24); ii) placebo: Matched inhalers with FP to
preserve the blinding (n=33). Delivery method: Diskus MDI
(metered.dose inhaler). Parallel design. | 12 months | 36.8 | 26.6 | 98.0 | 80.7 |
| Bousquet et
al (12), 2003 | Multiple centers,
Europe | Mild intermittent
asthma according to GINA | i) 1,600 µg BDP
daily by nebulizer (n=10); ii) 3,200 µ BDP daily by nebulizer
(n=10); iii) 800 µ BDP daily by MDI (n=10); iv) placebo (n=10).
Parallel design. | 3 weeks | NR | 26.3 | NR | NR |
| Ponce, et al
(9), 2009 | Children Hospital
Eva Samano de Lopez Mateos, Mexico | Mild intermittent
asthma according to GINA | i) Salbutamol as
required and BUD: 200 µg 1 pf twice daily 400 µg/day) for children
aged 6.14 years, 200 µg 1 pf once daily (200 µg/day) for children
aged 1.5 years (n=9); ii) salbutamol as required n=18); iii)
salbutamol as required and ML: 5 mg daily for children aged 6.14
years, 4 mg daily for children aged 1.5 years (n=6); iv) salbutamol
as required and ML and BUD n=17). Delivery method: Inhalation.
Parallel design. | 3 months | 50.0 |
7.2 | NR | NR |
| Dahlén et al
(13), 2009 | Karolinska
University Hospital, Sweden | Non-smoking
subjects with intermittent allergic asthma (GINA) treated only with
a short.acting β2.agonist p.r.n | i) Formoterol: 4.5
µg 2 pfs once daily (n=15); ii) BUD/formoterol: 160 µg/4.5 µg 2 pfs
once daily (n=15); iii) placebo: 2 pfs daily (n=15). Delivery
method. Turbuhaler DPI. Crossover design. | 7 days | 53.3 | 30.5 | 105.2 | 100.0 |
| Ehrs et al
(14), 2010 | Unit of Lung and
Allergy Research, Sweden | i) Diagnosis of
asthma; ii) regarding themselves as free of symptoms | i) FP: 250 µg 1 pf
twice daily (500 µg/day; n=36); ii) placebo: 1 pf twice daily
(n=34). Delivery device: Accuhaler DPI. Parallel design. | 3 months | 30.0 | 38.5 | 89.9 | 47.1 |
| Gyllfors et
al (15), 2006 | Karolinska
University Hospital, Sweden | Mild atopic asthma
treated only with a short-acting β2-agonist as required ≤2
times/week | i) FP: 500 µg 1 pf
twice daily (1,000 µg/day; n=13); ii) placebo: 1 pf twice daily
(n=13). Delivery method: Diskus DPI. Crossover design. | 2 weeks | 23.1 | 31.0 | 101 | 100.0 |
| Haahtela et
al (16), 2006 | Multiple centers,
Europe | Mild intermittent
asthma according to GINA 2005 guidelines | i) BUD/formoterol:
160/4.5 µg as required (n=44); ii) formoterol: 4.5 µg as required
(n=43). Delivery method: Turbuhaler DPI. Parallel design. | 6 months | 30.4 | 37.0 | 100.9 | 83.7 |
| Reddel et al
(17), 2008 | Woolock Institute
of Medical Research and University of Sydney, Australia | i) An established
history of asthma; ii) FEV1 >90% predicted; iii) symptoms ≤2
times/week; iv) sambutamol use ≤2 times/week | i) FP: 125 µg 1 pf
twice daily (250 µg/day; n=23); ii) placebo: 1 pf twice daily
(n=21). Delivery method: MDI. Parallel design. | 11 months | 36.4 | 39.3 | 99.2 | 75 |
| Rüdiger et
al (18), 2013 | University Hospital
Basel, Switzerland | Patients with
symptom-free asthma | i) BUD, 400 µg
single dose (n=8); ii) control: Placebo (n=8). Delivery method:
Inhalation. Crossover design. | Single dose | Not reported | 32.0 | NR | NR |
| Mendes et al
(19), 2004 | University of Miami
School of Medicine, | Mild intermittent
asthma as defined by GINA 2002 USA | i) FP + ML: FP 220
µg 1 pf twice daily (440 µg daily) + 10.mg ML tablet p.o. once
daily (n=12); ii) FP + placebo: FP 220 µg 1 pf twice daily (440 µg
daily) + placebo tablet p.o. once daily (n=12); iii) placebo + ML:
Placebo 1 pf twice daily + ML 10 mg p.o. once daily (n=12); iv)
placebo + placebo: Placebo 1 pf twice daily + placebo tablet p.o.
once daily (n=12). Crossover design. | 2 weeks | 16.7 | 39.8 | 95.4 | 100.0 |
| Pizzichini et
al (20), 1996 | St. Joseph's
Hospital, Canada | Mild asthma with
little or no symptoms, treatment only with inhaled β2-agonist when
needed | i) BDP: 500 µg once
(n=8); ii) salmoterol: 100 µg once (n=8); iii) placebo: 0 µg once
(n=8). Delivery method: Nebuhaler. Crossover design. | Single dose | 37.5 | 30.6 | 90.8 | 75 |
| Lim et al
(21), 1999 | Imperial College
School of Science and Medicine at the National Heart and Lung
Institute, UK | Mild stable asthma
treated with only inhaled β2-adrenergic agonist aerosol albuterol
for intermittent relief of wheezing | i) BUD: 800 µg
b.i.d. (n=14); ii) placebo: Matched with BUD b.i.d. (n=14).
Delivery method: Turbohaler DPI. Crossover design. | 4 weeks | 42.9 | 28.6 | 95.6 | 100.0 |
| Stanković et
al (22), 2007 | Clinic for Lung
Diseases and Tuberculosis, Serbia | Mild intermittent
asthma according to GINA 2006 guideline | i) BDP: 250 µg/day
and short.acting β2 agonists (Ventolin) as required as rescue
medication (n=45); ii) control: Only short-acting β2 agonists
(Ventolin) as required as rescue medication daily (n=40). Delivery
method: Inhalation. Parallel design. | 6 months | 37.6 | 34.8 | NR | 78.8 |
| Tamaoki et
al (23), 2008 | Multiple centers,
Japan | Mild intermittent
asthma fulfilling ATS criteria and GINA 2006 | i) BDP: 100 µg 1 pf
twice daily (200 µg/day) via MDI using a spacing chamber (n=38);
ii) pranlukast: 225 mg b.i.d. p.o. (n=36). Parallel design. | 2 months | 27.0 | 37.0 | 84.8 | NR |
| Wongtim et
al (24), 1995 | Chest and Allergy
Clinic, Chulalongkorn Hospital, Thailand | i) Mild asthma with
exacerbation of cough and wheezing ≤1–2 times/week; ii) nocturnal
attack ≤1–2 times/month | i) BUD: 200 µg/pf,
2 pfs each time, twice daily (800 µg daily; n=10); ii) placebo: 0
µg 2 pfs twice daily (0 µg daily; n=10). Delivery method:
Turbuhaler DPI. Parallel design. | 2 months | 50.0 | 33.0 | NR | NR |
Study validity
Validity assessment of the studies is shown in
Table II. The majority of studies
had Jadad scores of ≥3, with 3 studies exhibiting scores <3.
Similar results were observed after the exclusion of low quality
trials (Jadad scores <3). Funnel plot analysis demonstrated that
there may be publication bias in studies assessing FEV1 change,
although this type of bias may exist in studies assessing other
measurements due to the low number of studies (data not shown).
| Table II.Study validity and outcomes. |
Table II.
Study validity and outcomes.
| Author/(Refs.),
year | Randomization | Allocation
concealment | Blinding of
participants and personnel | Number of patients
discontinued or lossed to follow-up, N (%) | Outcomes | JADAD score |
|---|
| Jatakanon et
al (10), 1999 | Yes; method not
stated | Method not
stated | Adequate | 1 (3.2) | Lung function;
airway responsiveness; sputum measurement | 4 |
| Boulet et al
(11), 2009 | Yes; method not
stated | Adequate | Adequate | 12 (17.4) at 3
months post.treatment; 25 (36.2) at 6 months post-treatment; 31
(44.9) at 9 months post-treatment; 38 (55.1) at 12 months
post-treatment | Methacholine airway
responsiveness; induced sputum; respiratory symptoms; peak
expiratory flows; asthma exacerbations | 4 |
| Bousquet et
al (12), 2003 | Yes; method not
stated | Method not
stated | Adequate | None | Airway
responsiveness; lung function; adverse events | 4 |
| Ponce et al
(9), 2009 | Yes; method not
stated | Method not
stated | Not blind | Not stated | Number of children
with disappearing symptoms or symptoms that decreased by ≥70% | 1 |
| Dahlén et al
(13), 2009 | Yes; method not
stated | Method not
stated | Adequate | Not stated | Airway
responsiveness to methacholine; FeNO; sputum measurements; lung
function; asthma symptoms | 3 |
| Ehrs et al
(14), 2010 | Yes; method not
stated | Method not
stated | Yes; method not
stated | None | FEV1 (% predicted)
and FVC; FEV1 (% predicted) after inhalation of the
bronchodilators; PD20FEV1; FEV1 decrease after dry air hyperpnoea;
exhaled NO; AQLQ scores | 3 |
| Gyllfors et
al (15), 2006 | Yes; method not
stated | Method not
stated | Yes; method not
stated | 1 (7.1) | FeNO; urinary-LTE4;
airway responsiveness | 3 |
| Haahtela et
al (16), 2006 | Yes; using a
computer program to generate random sequences | Method not
stated | Adequate | 6 (6.5) | FeNO; FEV1; number
of inhalations of study medication; asthma symptom | 5 |
| Reddel et al
(17), 2008 | Yes; randomization
was by computer-generated sequences | Randomization code
remained concealed until analysis | Adequate | 12 (27.3) | Morning PEF;
morning FEV1; symptom score; β2-agonist use; waking due to asthma;
symptom-free days; reliever-free days; FVC; asthma-related quality
of life; FeNO; airway responsiveness; total fluticasone dose | 5 |
| Rüdiger et
al (18), 2013 | Yes; method not
stated | Method not
stated | Adequate | 3 (37.5) | Serum level of ACTH
and cortisol 60 min after drug inhalation | 4 |
| Mendes et al
(19), 2004 | Yes; method not
stated | Method not
stated | Adequate | Not stated | FEV1; FVC;
FEV1/FVC; MEF50; airway blood flow | 3 |
| Pizzichini et
al (20), 1996 | Yes; method not
stated | Method not
stated | Adequate | Not stated | FEV1;
methochacholine responsiveness; airway inflammation markers | 3 |
| Lim et al
(21), 1999 | Yes; method not
stated | Method not
stated | Adequate | Not stated | Lung function;
PC20; eNO; airway inflammation | 3 |
| Stanković et
al (22), 2007 | Yes; method not
stated | Method not
stated | Not blind | 11 (11.5) | FEV1/FVC; FVC; PEF;
diurnal PEF variability; bronchoprovocative test | 2 |
| Tamaoki et
al (23), 2008 | Yes; method not
stated | Method not
stated | Not blind | 11 (12.9) | Asthma symptoms;
pulmonary function; use of relief medication; sputum analysis | 2 |
| Wongtim et
al (24), 1995 | Yes; method not
stated | Method not
stated | Adequate | None | Lung function;
airway responsiveness; symptom score | 4 |
Lung function
FEV1
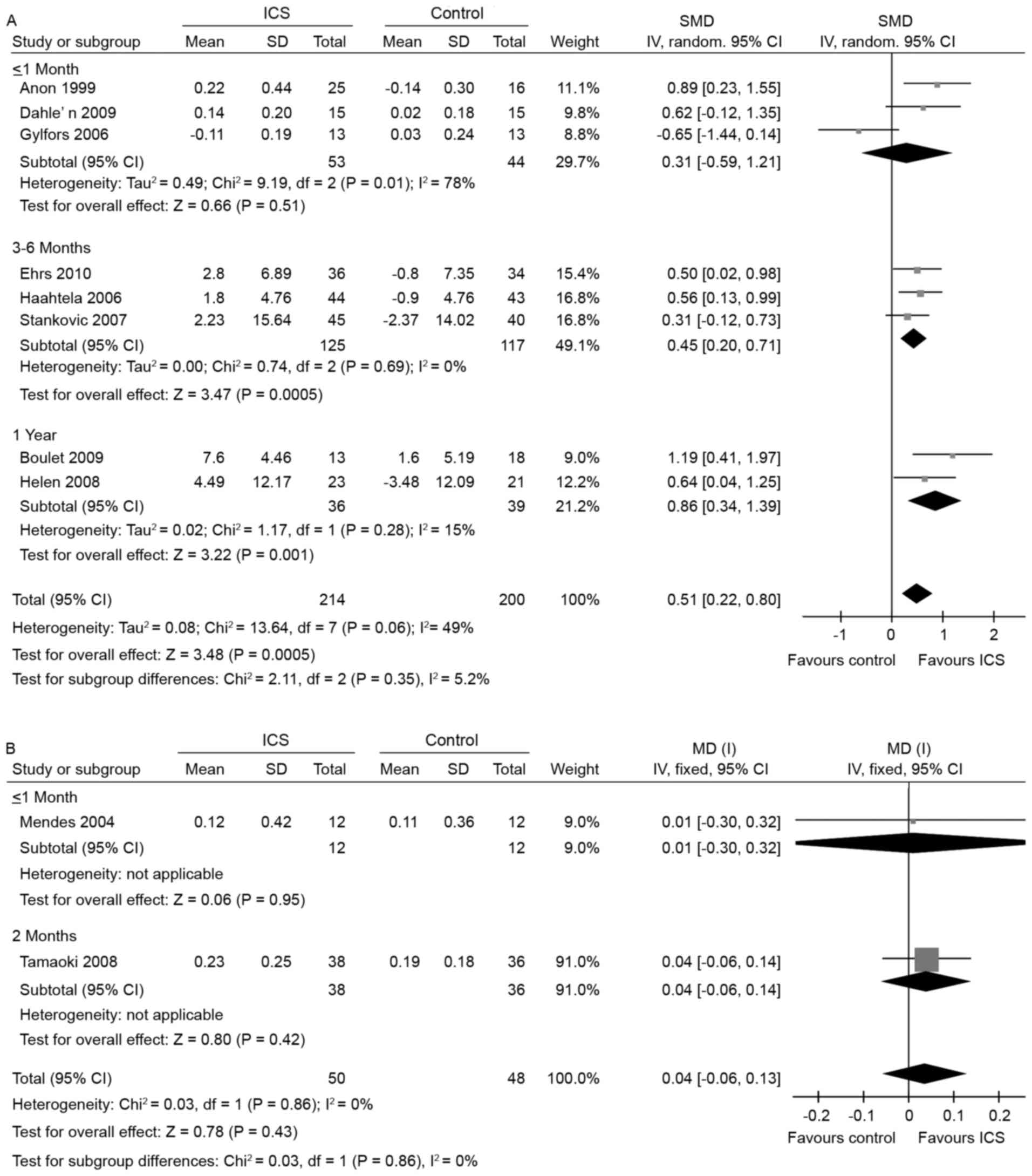
A significant improvement in FEV1 was noted after
3–6 months of ICS treatment vs. placebo (3 studies; SMD, 0.45; 95%
CI, 0.20 to 0.71; I2=0%; Fig.
2A) (14,16,22).
Consistent with the results observed after 3–6 months of treatment,
after 1 year of treatment, a further improvement in FEV1 was noted
in the ICS groups as compared with placebo (2 studies; SMD, 0.86;
95% CI, 0.34 to 1.39; I2=15%; Fig. 2A) (11,17). The
overall effect of ICS on FEV1 change was also significant when
compared with the effect of placebo (8 studies; SMD, 0.51; 95% CI,
0.22 to 0.80; I2=49%; Fig.
2A) (10,11,13–17,22).
When compared with leukotriene receptor antagonists
(LTRA), more than 2 months ICS treatment had no advantage on FEV1
improvement (19,23) (2 studies; WMD, 0.04l; 95% CI, −0.06
to 0.13; I2=0%; Fig. 2B).
All data were collected from adults, no studies measured FEV1
change or other lung function measurements in children.
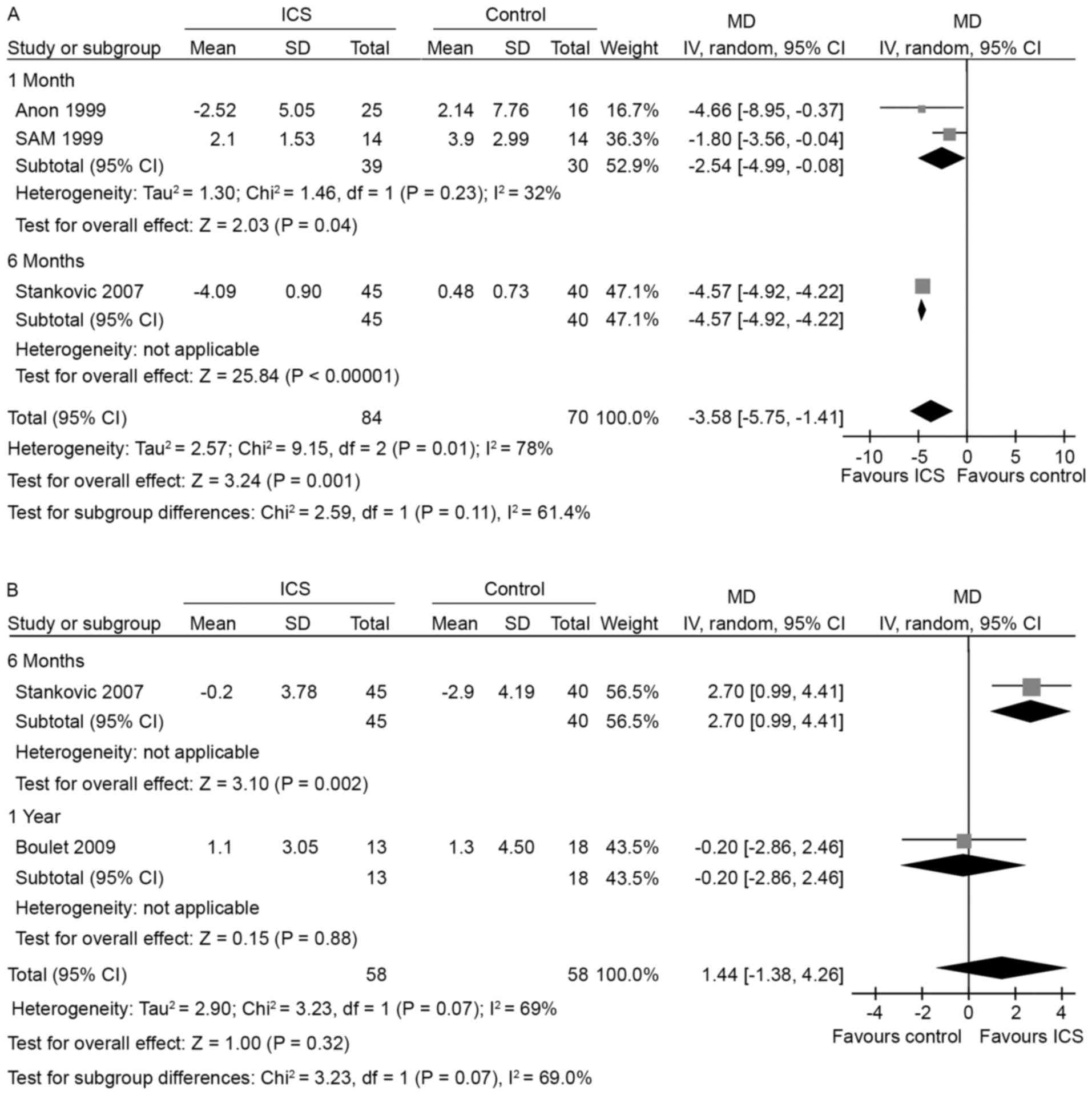
PEF variability
A decrease of PEF variability was observed after 1
month of treatment with ICS compared with placebo (10,21) (2
studies; WMD, −2.54%; 95% CI −4.99 to −0.08%; I2=32%;
Fig. 3A). After 6 months of
treatment, a further reduction of PEF variability was noted
(22) (1 study; WMD, −4.57%; 95% CI,
−4.92 to −4.22%). The overall effect of ICS treatment vs. placebo
was also significant in PEF variability (10,21,22) (3
studies; WMD, −3.58%; 95% CI, −5.75 to −1.41%; I2=78%;
Fig. 3A). Substantial heterogeneity
(I2=78%) in this meta-analysis may be explained by the
small sample size of all 3 studies and the lower methodological
quality of the study conducted by Stanković et al (22).
FEV1/FVC
Apparent change of FEV1/FVC could be seen after 6
months of treatment, while 1 year of treatment made no further
difference (6 months, 1 study; WMD, 2.7%; 95% CI, 0.99 to 4.41% vs.
1 year, 1 study; WMD, −0.2%; 95% CI, −2.86 to 2.46%; Fig. 3B) (11,22). The
overall effect was not significant (2 studies; WMD, 1.44%; 95% CI,
−1.38 to 4.26; I2=69%; Fig.
3B). The heterogeneity (I2=69%) of the meta-analysis
may derive from the inappropriate trial design of the study by
Stanković et al (22), and
the different population of patients may also have caused
heterogeneity.
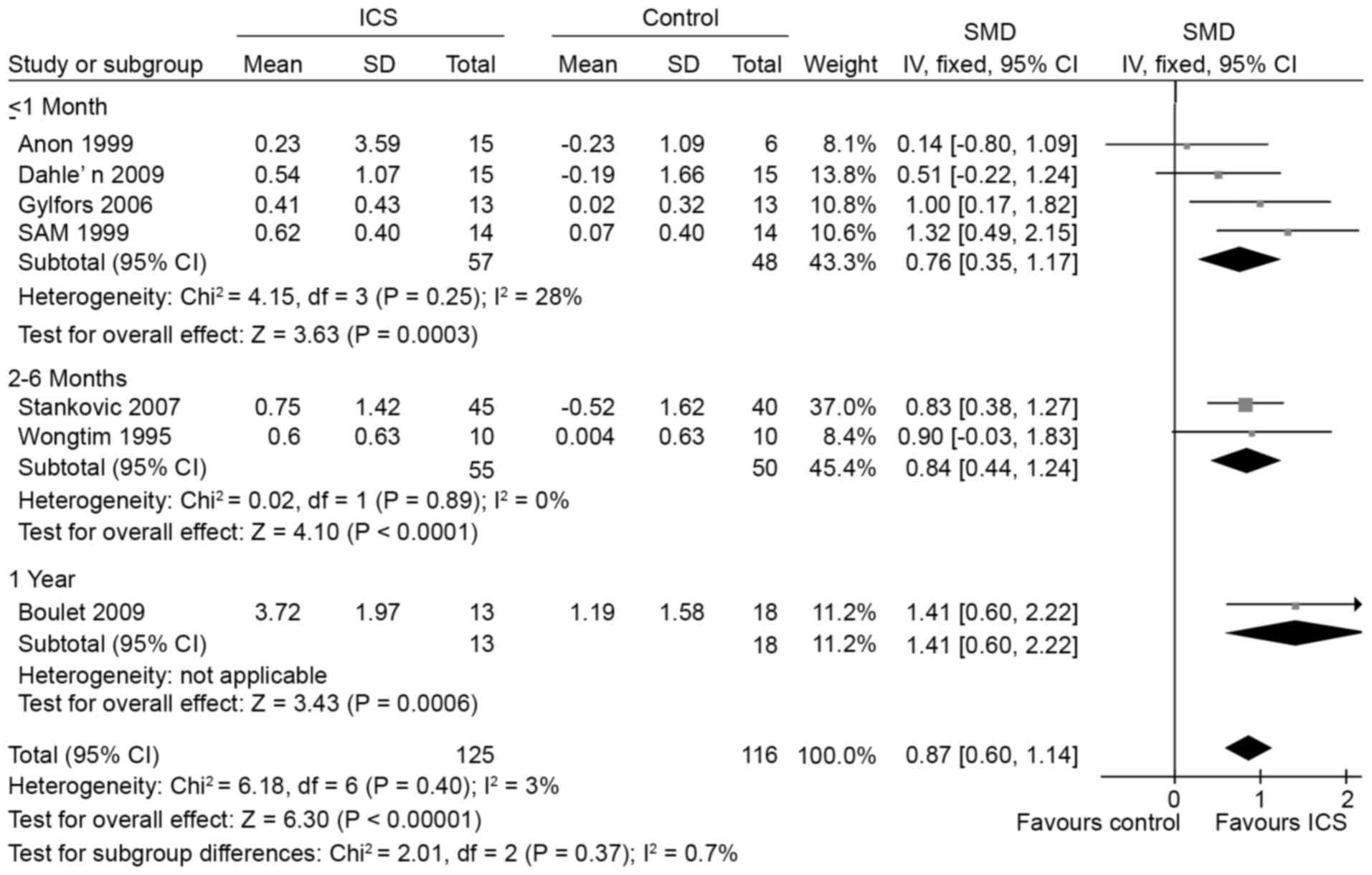
AHR
With treatment of ICS for 1 month, 2–6 months or 1
year, the AHR (indicated as log transformed PC20FEV1) was
attenuated compared with placebo (10,11,13,15,21,22,24) (≤1
month, 4 studies; SMD, 0.76; 95% CI, 0.35 to 1.17;
I2=28% vs. 2–6 months, 2 studies; SMD, 0.84; 95% CI,
0.44 to 1.24; I2=0% vs. 1 year, 1 study; SMD, 1.41; 95%
CI, 0.6 to 2.22; Fig. 4), and the
overall improvement effect of ICS on AHR was also significant when
compared with the placebo (7 studies; SMD, 0.87; 95% CI, 0.60 to
1.14; I2=3%; Fig. 4). All
results were from adults as there was no AHR outcome assessed in
the study investigating children.
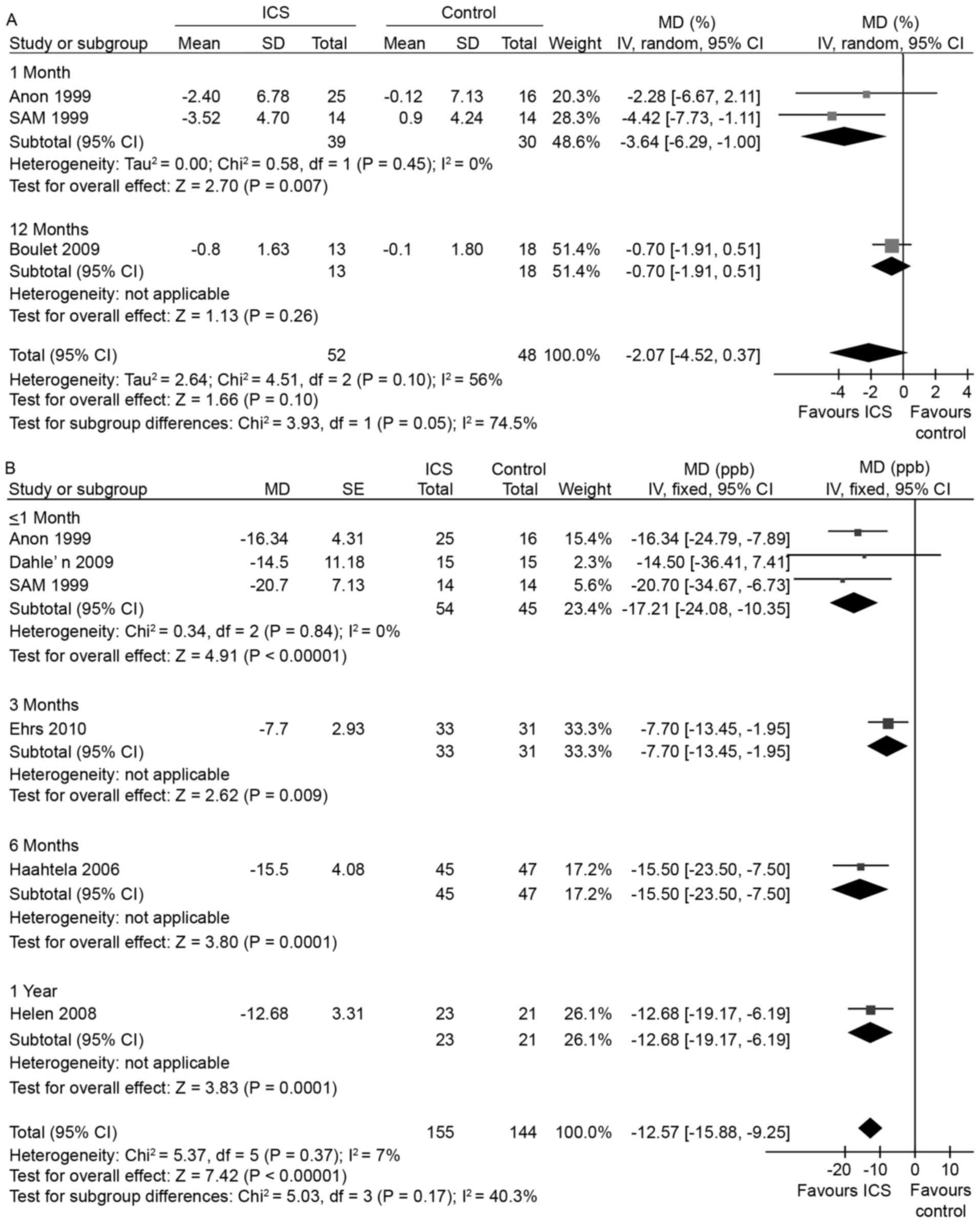
Airway inflammation
Sputum eosinophils
Notably, 1 month of ICS treatment reduced the sputum
eosinophil percentage compared with placebo, whereas 1-year
treatment could not (10,11,21) (1
month, 2 studies; WMD, −3.64%; 95% CI, −6.29 to −1.00%,
I2=0% vs. 1 year, 1 study; WMD, −0.7%; 95% CI, −1.91 to
0.51%; Fig. 5A). It was shown in one
study that single dose ICS could not change it (20). Overall analysis showed no significant
sputum eosinophil percentage change with ICS treatment vs. placebo
(3 studies; WMD, −2.07%; 95% CI, −4.52 to 0.37%; I2=56%;
Fig. 5A). The heterogeneity
(I2=56%) of this meta-analysis may be associated with
the distinct treatment duration of the 3 studies and the small
sample size of these studies.
Only one study compared the influence of ICS on
sputum eosinophil percentage with LTRA, and showed that ICS
decreased sputum eosinophil percentage with no statistical
significance (23) (WMD, −6%; 95%
CI, −12.38 to 0.38%). All results of airway inflammation were from
adults, and there was no related outcomes in the study evaluating
children.
FeNO
ICS treatment within 1 month reduced FeNO levels
compared with placebo (10,13,21) (3
studies; WMD, −17.21 ppb; 95% CI, −24.08 to −10.35 ppb;
I2=0%; Fig. 5B), and
after 3, 6 months or 1 year of treatment, similar results were
found [3 months, one study (14);
WMD, −7.7 ppb; 95% CI, −13.45 to −1.95 ppb; vs. 6 months, one study
(16); WMD, −15.5 ppb; 95% CI, −23.5
to −7.5 ppb vs. 1 year, one study (17); WMD, −12.68 ppb; 95% CI, −19.17 to
−6.19 ppb]. Overall analysis showed an apparent reduced FeNO level
(6 studies; WMD, −12.57 ppb; 95% CI, −15.88 to −9.25 ppb;
I2=7%; Fig. 5B).
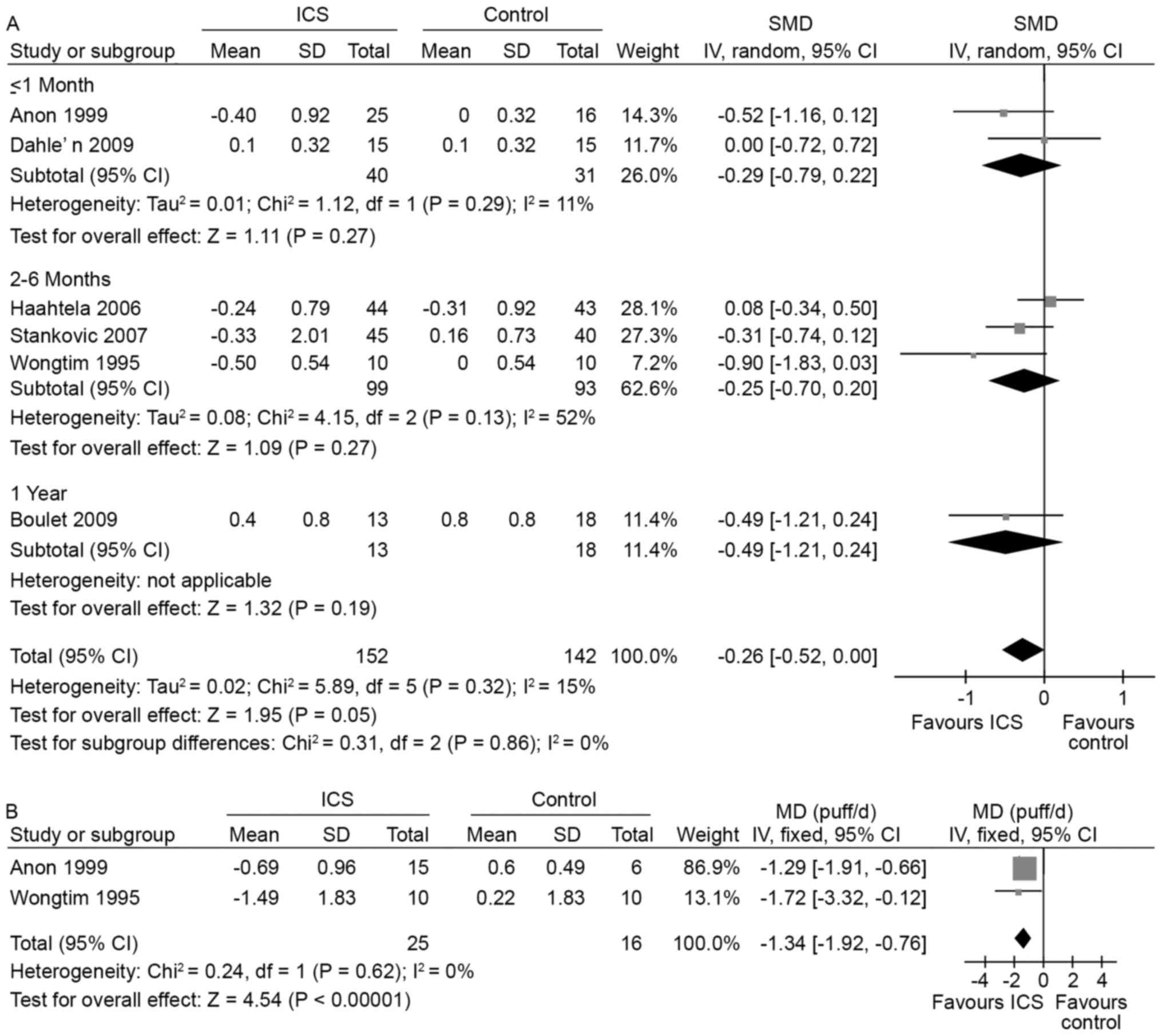
Symptom control
When the duration of ICS treatment was no more than
1 month, the effect of ICS on symptom control (indicated as symptom
score change) was not significant compared with placebo (10,13) (2
studies; SMD, −0.29; 95% CI, −0.79 to 0.22; I2=11%;
Fig. 6A). Similarly, after 2–6
months or 1 year of treatment the effect of ICS on symptom control
was not significant [2-6 months, 3 studies (16,22,24);
SMD, −0.25; 95% CI, −0.7 to 0.2; I2=52%; and 1 year, one
study (11) SMD, −0.49; 95% CI,
−1.21 to 0.24; Fig. 6A]. The overall
effect of ICS on symptom score change was not significant (6
studies; SMD, −0.26; 95% CI, −0.52 to 0; I2=15%;
Fig. 6A). However, ICS was able to
reduce the frequency of rescue inhaler use after 1–2 months of
treatment when compared with placebo (10,24) (2
studies; SMD, −1.34; 95% CI, −1.92 to −0.76; I2=0%;
Fig. 6B).
There was only one study (9) concerned with the symptom control of
children with mild intermittent asthma, which indicated that 3
months of treatment with ICS significantly increased the number of
children without asthma symptoms (RR, 8; 95% CI, 1.04 to 61.52)
compared with placebo. When compared with LTRA, low dose ICS (3
months) was not found to significantly influence symptom control
(23) (SMD, 0.44; 95% CI, −0.02 to
0.9) in adult patients; however, the number of children without
asthma symptoms significantly increased over the same period of low
dose ICS (9) (RR, 2.67; 95% CI, 0.39
to 18.42).
Other parameters
Some studies also assessed the safety of ICS in
addition to its effectiveness. However, there was an insufficient
number of related. Only one study assessed the effect of ICS on the
hypothamo-pituitary-adrenocortical axis, in which Rüdiger et
al (18) found that single low
dose ICS did not influence this endocrine axis. Bousquet et
al (12) also claimed that 3
weeks of high dose ICS did not increase the number of patients
experiencing adverse events (RR, 1.00; 95% CI, 0.42 to 2.4). These
studies indicate that ICS treatment may be safe over a short
period, whereas the safety of long-term use in patients with mild
intermittent asthma remains unclear.
Discussion
The present systemic review attempted to assess the
effects of ICS compared with placebo or LTRA on lung function, AHR,
airway inflammation, symptom control and its adverse effects in
patients with mild intermittent asthma. The findings demonstrated
that, compared with a placebo, ICS improved lung function and
reduced AHR and airway inflammation in adult patients. However,
symptom control was unchanged, and ICS had no advantage over LTRA
for improving lung function and attenuating airway inflammation. In
children with mild intermittent asthma, ICS had a positive effect
on symptom control and was superior to LTRA in terms of symptom
control.
Previous findings have revealed that ICS treatment
results in improved lung function, diminished AHR, fewer symptoms
of asthma and fewer episodes of uncontrolled asthma compared with
as needed SABA alone (25), and
studies involving mild persistent asthma have indicated the
necessity of ICS therapy in these patients (4). However, studies associated with mild
intermittent asthma are lacking, and, due to the potential
long-term side effects of ICS (such as accelerated bone loss),
experts still regard SABA as the first-line treatment for patients
with intermittent asthma (2,26). A recent study focused on airway
inflammation in mild intermittent steroid-naïve asthmatic patients
found that many patients still exhibited persistent airway
inflammation, which could result in airway remodeling (4,7), and
nearly 6% of these patients required hospitalization or attended
the emergency department annually (27). The effect of ICS on bone mineral
density seemed to be slight and thus remains controversial
(28). Therefore, at least in some
patients with mild intermittent asthma, ICS should be
considered.
The present results showed that a longer duration of
ICS treatment induces a superior improvement in lung function and
the alleviation of AHR; however, the effect of attenuated airway
inflammation reduces as the treatment duration increases. A
previous study focused on patients with mild persistent asthma,
lung function and observed an improvement during the first year
(29), which was consistent with our
study concerning patients with mild intermittent asthma. However,
the improvement was decreased after 1 year in patients with
persistent asthma (30), and AHR was
only found to be increasingly improved during the first 3 months in
patients with mild persistent asthma (31); consistent with our study, AHR was
increasingly improved during the first year, implying the effect of
ICS on improvement of AHR is more durable in patients with
intermittent asthma.
In our study, both sputum eosinophil percentages and
FeNO levels were used as markers for airway inflammation, but the
FeNO change was more obvious. In the majority of asthmatic
patients, the correlation between sputum eosinophil and FeNO is
well established, except in patients with severe asthma (32), and the major site of synthesis of NO
is airway epithelial cells (32).
Based on our results, we conclude that in patients with
intermittent asthma, the airway epithelial cells are more sensitive
to ICS treatment than eosinophils.
Side effects of ICS are always a concern. Short-term
ICS use is believed to be safe (12,18);
however, longer treatment with high dose ICS may decrease bone
mineral density and increase the risk of osteoporosis or fracture
in patients with persistent asthma, but the effect of low dose ICS
on bone mineral density and risk of osteoporosis or fracture was
slight (28). Dysphonia or oral
candidiasis may also develop, but it could almost be prevented by
rinsing the mouth after ICS use (33). Therefore, low dose ICS may be safe
for patients with mild asthma, including those with intermittent
asthma.
There are a number of limitations to the present
systemic review. Firstly, the treatment duration of all the studies
included may not sufficient. This limitation prevents us from
identifying more positive and negative effects of ICS on patients
with mild intermittent and confuses the evaluation of the balance
of ICS benefits and risks. Secondly, the number of included studies
is too small, thus publication bias may exist, and the conclusion
from the review may not be able to applicable to a larger
population. Thirdly, some of the included studies were not high
quality trials, which may result in an increased risk of bias.
In conclusion, the present systemic review
demonstrates that ICS may improve lung function, alleviate airway
inflammation and AHR, but cannot ameliorate symptom control in
adult patients with mild intermittent asthma, and has no advantage
over LTRA on these effects. On the contrary, children with mild
intermittent asthma treated with ICS seemingly have a better
control of asthma symptoms vs. placebo or LTRA treatment. Our
findings indicate that ICS may be an effective and safe therapy for
patients with mild intermittent showing signs of progression or
exacerbation, and LTRA should be an alternate choice for adult
patients to improve lung function and reduce airway inflammation.
As for child patients, ICS seems to be the superior choice to
control symptoms, but should be used with caution, as the evidence
remains insufficient.
References
|
1
|
Feng X and Lin J: An Epidemiology Survey
On The Prevalence And Associated Risk Factors Of Asthma Among
Adults In China. Peking Union Medical College Press; Beijing: pp.
942014
|
|
2
|
Global Initiative for Asthma (GINA), .
From the Global Strategy for Asthma Management and Prevention.
2015.http://www.ginasthma.orgMarch
5–2016
|
|
3
|
Humbert M, Holgate S, Boulet LP and
Bousquet J: Asthma control or severity: That is the question.
Allergy. 62:95–101. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dusser D, Montani D, Chanez P, de Blic J,
Delacourt C, Deschildre A, Devillier P, Didier A, Leroyer C,
Marguet C, et al: Mild asthma: An expert review on epidemiology,
clinical characteristics and treatment recommendations. Allergy.
62:591–604. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Israel E and Drazen JM: Treating mild
asthma-when are inhaled steroids indicated? N Engl J Med.
331:737–739. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Van den Toorn LM: Clinical implications of
airway inflammation in mild intermittent asthma. Ann Allergy Asthma
Immunol. 92:589–594; quiz 595–7, 658. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pedersen F, Holz O, Kanniess F, Zielen S,
Schulze J, Gillissen A, von Berg A, Berdel D, Beier J, Beeh K, et
al: Longitudinal measurement of airway inflammation over one year
in children and adults with intermittent asthma. BMC Res Notes.
7:9252014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Higgins JPT, Deeks JJ and Altman DG:
Analysing data and undertaking meta-analysesCochrane Handbook for
Systematic Reviews of Interventions. Higgins JPT and Green S: John
Wiley & Sons; Chichester, UK: pp. 243–296. 2008
|
|
9
|
Castro H Ponce, Rodríguez Espino S and
Rodríguez Orozco AR: Administration of budesonide (inhaled steroid)
to children to control intermittent asthma. Rev Alerg Mex. 56:9–12.
2009.(In Spanish). PubMed/NCBI
|
|
10
|
Jatakanon A, Kharitonov S, Lim S and
Barnes PJ: Effect of differing doses of inhaled budesonide on
markers of airway inflammation in patients with mild asthma.
Thorax. 54:108–114. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Boulet LP, Turcotte H, Prince P, Lemière
C, Olivenstein R, Laprise C, Larivée P, Bégin P and Laviolette M:
Benefits of low-dose inhaled fluticasone on airway response and
inflammation in mild asthma. Respir Med. 103:1554–1563. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bousquet J, Meziane H, Chanez P, Mueser M
and Umile A: The response of two different dosages of beclometasone
dipropionate suspension for nebulization versus a standard dose of
beclometasone dipropionate via a metered-dose inhaler on
bronchoprovocation testing in adults with asthma. Respir Med. 97
Suppl B:11–14. 2003. View Article : Google Scholar
|
|
13
|
Dahlén B, Lantz AS, Ihre E, Skedinger M,
Henriksson E, Jörgensen L, Ekström T, Dahlén SE and Larsson K:
Effect of formoterol with or without budesonide in repeated
low-dose allergen challenge. Eur Respir J. 33:747–753. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ehrs PO, Sundblad BM and Larsson K: Effect
of fluticasone on markers of inflammation and quality of life in
steroid-naive patients with mild asthma. Clin Respir J. 4:51–58.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gyllfors P, Dahlén SE, Kumlin M, Larsson K
and Dahlén B: Bronchial responsiveness to leukotriene D4 is
resistant to inhaled fluticasone propionate. J Allergy Clin
Immunol. 118:78–83. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Haahtela T, Tamminen K, Malmberg LP,
Zetterström O, Karjalainen J, Ylä-Outinen H, Svahn T, Ekström T and
Selroos O: Formoterol as needed with or without budesonide in
patients with intermittent asthma and raised NO levels in exhaled
air: A SOMA study. Eur Respir J. 28:748–755. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Reddel HK, Belousova EG, Marks GB and
Jenkins CR: Does continuous use of inhaled corticosteroids improve
outcomes in mild asthma? A double-blind randomised controlled
trial. Prim Care Respir J. 17:39–45. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rüdiger JJ, Gencay M, Yang JQ, Bihl M,
Tamm M and Roth M: Fast beneficial systemic anti-inflammatory
effects of inhaled budesonide and formoterol on circulating
lymphocytes in asthma. Respirology. 18:840–847. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mendes ES, Campos MA, Hurtado A and Wanner
A: Effect of montelukast and fluticasone propionate on airway
mucosal blood flow in asthma. Am J Respir Crit Care Med.
169:1131–1134. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pizzichini MM, Kidney JC, Wong BJ, Morris
MM, Efthimiadis A, Dolovich J and Hargreave FE: Effect of
salmeterol compared with beclomethasone on allergen-induced
asthmatic and inflammatory responses. Eur Respir J. 9:449–455.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lim S, Jatakanon A, John M, Gilbey T,
O'connor BJ, Chung KF and Barnes PJ: Effect of inhaled budesonide
on lung function and airway inflammation. Assessment by various
inflammatory markers in mild asthma. Am J Respir Crit Care Med.
159:22–30. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Stanković I, Pejcić T, Milenković B,
Jovanović D and Rancić M: Is there any point in a corticosteroid
treatment of intermittent asthma? Scientific World Journal.
7:1082–1089. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tamaoki J, Isono K, Taira M, Tagaya E,
Nakata J, Kawatani K and Nagai A: Role of regular treatment with
inhaled corticosteroid or leukotriene receptor antagonist in mild
intermittent asthma. Allergy Asthma Proc. 29:pp. 189–196. 2008;
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wongtim S, Mogmued S, Chareonlap P and
Limthongkul S: Effect of inhaled corticosteroids on bronchial
hyperresponsiveness in patients with mild asthma. Asian Pac J
Allergy Immunol. 13:81–85. 1995.PubMed/NCBI
|
|
25
|
Haahtela T, Järvinen M, Kava T, Kiviranta
K, Koskinen S, Lehtonen K, Nikander K, Persson T, Selroos O,
Sovijärvi A, et al: Effects of reducing or discontinuing inhaled
budesonide in patients with mild asthma. N Engl J Med. 331:700–705.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Papi A: Treatment strategies in mild
asthma. Curr Opin Pulm Med. 15:29–34. 2009. View Article : Google Scholar
|
|
27
|
Koh MS and Irving LB: The natural history
of asthma from childhood to adulthood. Int J Clin Pract.
61:1371–1374. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Fuhlbrigge AL and Kelly HW: Inhaled
corticosteroids in children: Effects on bone mineral density and
growth. Lancet Respir Med. 2:487–496. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
O'Byrne PM, Barnes PJ, Rodriguez-Roisin R,
Runnerstrom E, Sandstrom T, Svensson K and Tattersfield A: Low dose
inhaled budesonide and formoterol in mild persistent asthma: The
OPTIMA randomized trial. Am J Respir Crit Care Med. 164:1392–1397.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Busse WW, Pedersen S, Pauwels RA, Tan WC,
Chen YZ, Lamm CJ and O'Byrne PM; START Investigators Group, : The
inhaled steroid treatment as regular therapy in early asthma
(START) study 5-year follow-up: Effectiveness of early intervention
with budesonide in mild persistent asthma. J Allergy Clin Immunol.
121:1167–1174. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Juniper EF, Kline PA, Vanzieleghem MA,
Ramsdale EH, O'Byrne PM and Hargreave FE: Effect of long-term
treatment with an inhaled corticosteroid (budesonide) on airway
hyperresponsiveness and clinical asthma in nonsteroid-dependent
asthmatics. Am Rev Respir Dis. 142:832–836. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lemière C, Ernst P, Olivenstein R,
Yamauchi Y, Govindaraju K, Ludwig MS, Martin JG and Hamid Q: Airway
inflammation assessed by invasive and noninvasive means in severe
asthma: Eosinophilic and noneosinophilic phenotypes. J Allergy Clin
Immunol. 118:1033–1039. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Green RH, Brightling CE, Pavord ID and
Wardlaw AJ: Management of asthma in adults: Current therapy and
future directions. Postgrad Med J. 79:259–267. 2003. View Article : Google Scholar : PubMed/NCBI
|