Introduction
Heparin has been widely used for the maintenance of
intravascular catheters in patients requiring intravenous
medications or arterial hemodynamic monitoring. The beneficial
roles of heparin solution in ameliorating catheter occlusion,
prolonging patency and reducing phlebitis have been investigated in
a number of clinical studies (1,2). As a
classical anticoagulant-medicine, heparin is considered to prevent
the formation of thrombus within the indwelling catheter while
being used as a flushing or locking solution (3–6).
However, other studies have reported no additional benefits from
heparin compared to normal saline in promoting catheter patency
(7–9). A previous systematic review and
meta-analysis of randomized controlled trials (RCTs) indicated that
intermittent flushing with heparin was not superior to normal
saline in reducing catheter occlusion, whereas low dose infusion
with heparin may improve the catheter patency and prevent phlebitis
(4). Furthermore, two Cochrane
systematic reviews were unable to provide conclusive evidence
favoring the application of heparin solution over normal saline in
the maintenance of central venous and arterial catheters (10,11).
Previous studies on the use of heparin solution in
peripheral venous catheters have shown controversial results. One
Cochrane review that included both randomized and quasi-randomized
trials reported significant heterogeneity among studies, which were
not available for a meta-analysis (1). Another systematic review that focused
on pediatric patients reported that continuous heparin infusion
improved catheter patency, decreased infusion failures and lessened
phlebitis. However, the same study showed no significant benefits
of intermittent heparin flushing (3). A recent meta-analysis demonstrated
similar beneficial roles of heparin solution in continuous infusion
rather than intermittent flushing in adults (12).
Despite its wide use in daily practice, there are
some concerns about the safety of heparin. For example, heparin has
been shown to induce thrombocytopenia, and increasing bleeding risk
and allergic reactions may occur following heparin infusion or
flushes (13). Furthermore, a
routine use of heparin for the most extensively placed peripheral
venous catheters may unnecessarily increase the cost of health care
when its cost-effectiveness remains unclear (14). As such, a number of RCTs with
inconsistent or conflicting results have been published, prompting
further debate on the use of heparin solution for peripheral venous
catheter maintenance (15–17). Therefore, this updated systematic
review and meta-analysis of RCTs was conducted to more precisely
evaluate the role of heparin in maintaining peripheral venous
catheters.
Materials and methods
Search strategy
A comprehensive literature search up to February
2016 was performed using PubMed (www.ncbi.nlm.nih.gov/pubmed), Embase (www.embase.com), Web of Science (www.isiknowledge.com) and Cochrane Central Register of
Controlled Trials (www.cochranelibrary.com/about/central-landing-page.html)
without language limitation. Manual searching was also used to
identify eligible studies from key journals, major conference
abstracts, original articles and reference lists. The following
Medical Subject Headings and free text words were used: ‘Heparin’,
‘placebo’, ‘control’ and ‘peripheral’. Furthermore, the search was
restricted to human studies and RCTs.
Study selection
Two investigators independently assessed the
articles, and any disagreements were resolved by consensus with a
third reviewer. Studies were selected if they met the following
criteria: i) RCTs, ii) conducted in subjects with peripheral venous
catheters, iii) compared heparin added to intravenous fluid vs. no
heparin added to the similar fluid and iv) measured catheter
patency, occlusion, infusion failure or phlebitis. Furthermore,
studies in which the subjects received systemic anticoagulation
with heparin from any other access were excluded.
Data extraction
Abstracts and full texts of the studies included
were retrieved by two reviewers independently and managed in
Endnote X7 (Clarivate Analytics, Philadelphia, PA, USA). Data were
extracted by two reviewers and further verified by a third
reviewer, who then resolved the disagreements. The following data
were extracted and stored in standardized forms: First author,
publication year, country, study type, population and protocol,
patient and catheter numbers, catheter material and size, heparin
dosage and frequency of administration, outcomes and results.
Assessment of bias
The quality of the studies were evaluated using the
Cochrane risk of bias tool (18),
comprising of random sequence generation, allocation concealment,
blinding, incomplete outcome data, selective reporting, and other
bias. Any discrepancies were resolved by consensus with a third
reviewer.
Outcomes
In the majority of the studies included, the primary
outcomes of interest reported were catheter occlusion and patency
duration. Secondary outcomes were infusion failure caused by any
reasons, phlebitis and other major adverse events associated with
the use of heparin. Phlebitis was determined when pain, induration,
tenderness, erythema or palpable cord was recorded. Furthermore,
major adverse events included heparin induced thrombocytopenia,
allergy and major bleeding.
Data analysis
The effects of heparin solution from either
continuous infusion or intermittent flushing studies were analyzed
for subgroups. The total effects of dichotomous data using risk
ratios (RRs) were pooled. Continuous outcomes were expressed as the
mean ± standard deviation (SD) and analyzed using standard mean
differences (SMDs). Furthermore, the I2 test was
conducted to assess the heterogeneity among the studies. Once
significant heterogeneity was found (I2>50%), the
random effects models (Inversed-Variance) were used and a
sensitivity analysis was performed to verify the consistency of the
results. Alternatively, the fixed model (Mantel-Haenszel for
dichotomous data and Inverse-Variance for continuous data) was
selected for the analysis. The Egger's and Begg's tests, and funnel
plots were used to assess the publication bias, and subgroup
analysis and meta-regression were used to identify potential
sources for heterogeneity between studies. Statistical analysis was
performed with Stata (version 12; StataCorp LLC, College Station,
TX, USA), using the metan, metareg and metainf commands amongst
others. A two-sided P≤0.05 was considered statistically
significant.
Results
Study selection and
characteristics
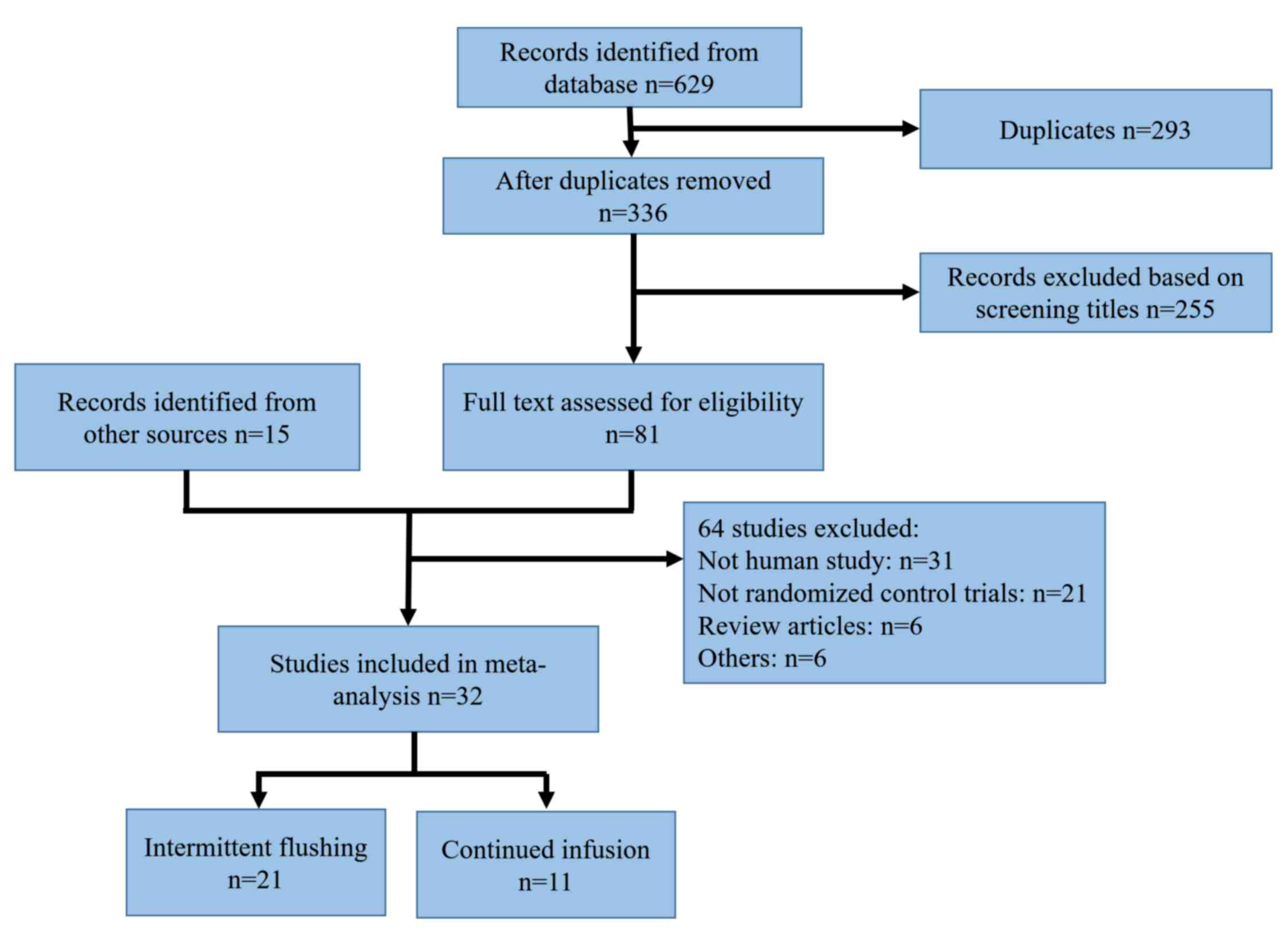
A standard workflow of searching and selection of
eligible studies according to the PRISMA statement (19) is presented in Fig. 1. In total, 629 references from
electronic databases were revealed by the literature search, of
which, 293 were identified as duplicates due to the overlap of the
databases. The remaining 336 citations were screened for
eligibility, yielding 81 studies for full-text review. Further
examination of the relevant reference lists of published reviews
and meta-analyses identified 15 additional citations. Finally, 32
studies were found to comply with the predefined inclusion
criteria. The characteristics of the final 32 studies included in
the present review are displayed in Table I, among which, there are 21 reported
results for intermittent flushing (7–9,14–17,20–33) and
11 evaluated heparin for continuous infusion (34–44).
 | Table I.Characteristics of the 32 studies
included in the present meta-analysis. |
Table I.
Characteristics of the 32 studies
included in the present meta-analysis.
| First author | Year | Country and
scale | Population | Heparin group,
patient/catheter (dosage) | Control group,
patient/catheter (treatment) | Catheter material
(size, G) | Outcomes | (Refs.) |
|---|
| Niesen | 2003 | USA, single
center | Adults, pregnant
women | 38/38 (10 U/ml/24
h)a | 35/35 (saline
placebo) | (16,18)d | Patency, phlebitis,
occlusion |
(7) |
| Hamilton | 1988 | USA, single
center | Adults,
surgical | 80/170 (100 U/ml/8
h)a | 80/137 (saline
placebo) | Teflon (18–22) | Patency, phlebitis,
occlusion |
(8) |
| Shoaf | 1992 | Country not
mentioned, single center | Adults, cardiac
surgery | 132/132 (10 U/ml/8
h)a | 128/128 (saline
placebo) | Teflone | Patency, phlebitis,
infusion failure, occlusion |
(9) |
| Kleiber | 1993 | USA, single
center | Children, medical
wards | 56/56 (10 U/ml/6
h)a | 68/68 (saline
placebo) | Teflon (18–24) | Patency, infusion
failure | (14) |
| Upadhyay | 2015 | India, single
center | Neonates, NICU | 60/96 (10 U/ml/12
h)a | 60/100 (saline
placebo) | (24)d | Patency | (15) |
| Wang | 2015 | China, single
center | Adults, liver
cirrhosis | 36/65 (50 U/ml/12
h)a | 32/125 (saline
placebo) | (22,
24)d | Patency, phlebitis,
occlusion | (16) |
|
Bertolino3 | 2014 | Italy, single
center | Adults, medical
wards | 107/285 (100
U/ml/12 h)a | 107/363 (saline
placebo) | Polyurethane, (18,
20, 22) | Patency, phlebitis,
occlusion | (17) |
| Meyer | 1995 | USA, single
center | Adults, pregnant
women | 31/31 (100 U/ml/6
h)a | 33/33 (saline
placebo) | (18)d | Patency, phlebitis,
infusion failure, occlusion | (20) |
| Mok | 2007 | China, single
center | Children, Medical
Wards | 82/82 (1–10
U/ml/6–8 h)a | 74/74 (saline
placebo) | (22,
24)d | Patency,
occlusion | (21) |
| Arnts | 2011 | The Netherlands,
single center | Neonates, NICU | 42/42 (10 U/ml/8
h)a | 46/46 (saline
placebo) | Neoflon (24) | Patency, phlebitis,
infusion failure | (22) |
| Kotter | 1996 | Country not
mentioned, single center | Neonates, NICU | 24/43 (10 U/ml/4
ha | 27/75 (saline
placebo) | Teflon (24) | Patency, phlebitis,
infusion failure | (23) |
| Beecroft | 1997 | Country not
mentioned, single center | Children, medical
wards | 238/238 (10 U/ml/8
h)a | 213/213 (saline
placebo) | Teflon (22,
24) | Patency, infusion
failure | (24) |
| Brown | 1999 | Canada, single
center | Neonates, NICU | 93/181 (5 U/ml/6
h)a | 93/150 (saline
placebo) | Teflon (24) | Patency, infusion
failure, phlebitis, occlusion | (25) |
| Heilskov | 1998 | USA, single
center | Neonates, NICU | 63/63 (2 U/ml/6 h
and 10 U/ml/6 h)a | 27/27 (saline
placebo) | Teflone | Patency, infusion
failure | (26) |
| Nelson | 1998 | USA, single
center | Neonates, NICU | 26/28 (10 U/ml/8
h)a | 32/46 (saline
placebo) | Teflon (24) | Patency, infusion
failure, phlebitis, occlusion | (27) |
| Schultz | 2002 | USA, single
center | Neonates, NICU | 20/20 (2 U/ml/3
h)a | 29/29 (saline
placebo) | Teflon (24) | Patency, infusion
failure, occlusion | (28) |
| Golberg | 1999 | Country not
mentioned, single center | Neonates, NICU | 23/23 (4 U/ml/6
h)a | 24/24 (saline
placebo) | (24)d | Patency,
phlebitis | (29) |
| Ashton | 1990 | USA, single
center | Adults, ICU | 16/16 (10 U/ml/12
h)a | 16/16 (saline
placebo) | (8–22)d | Phlebitis | (30) |
| Patidar | 2014 | India, single
center | Adults,
volunteer | 25/25 (10 U/ml/8
h)a | 25/25 (saline
placebo) | (22)d | Patency, phlebitis,
occlusion | (31) |
| LeDuc | 1997 | USA, single
center | Children, Emergency
Dept. | 77/77 (10
U/ml)b | 73/73 (saline
placebo) | (22,
24)d | Phlebitis,
occlusion | (32) |
| McMullen | 1993 | USA, single
center | Children, medical
wards | 68/68 (10
U/ml)a,b | 74/74 (saline
placebo) | (18–24)d | Patency, infusion
failure | (33) |
| Tanner | 1980 | Ireland, single
center | Adults,
surgical | 36/36 (1 U/ml
infusion) | 36/36 (saline
placebo) | –d,e | Phlebitis | (34) |
| Daniell | 1973 | USA, single
center | Adults, CCU | 88/88 (1 U/ml
infusion) | 86/86 (saline
placebo) | (18)d | Phlebitis,
occlusion | (35) |
| Messing | 1986 | France, single
center | Adults,
medical-surgical | 32/32 (1 U/ml
infusion) | 33/33 (without
heparin) | Teflone | Patency, phlebitis,
infusion failure, occlusion | (36) |
| Alpan | 1984 | Country not
mentioned, single center | Neonates, NICU | 13/105 (1 U/ml
infusion) | 13/122 (saline
placebo) | Teflon (22) | Patency, phlebitis,
infusion failure | (37) |
| Klenner | 2003 | Germany, single
center | Neonates, NICU | 145/565 (0.5 U/ml
infusion) | 151/692 (saline
placebo) | Teflon (26); Polyurethane (24) | Patency, phlebitis,
infusion failure, occlusion | (38) |
| Moclair | 1995 | UK, single
center | Neonates, NICU | 15/35 (0.1 U/ml
infusion) 16/47 (0.25 U/ml infusion) 23/61 (0.5 U/ml infusion)
16/30 (1 U/ml infusion) | 20/72 (without
heparin) | Teflon (24) | Patency, infusion
failure | (39) |
| Moclair | 1991 | UK, single
center | Adults,
surgical | 9/9 (0.1 U/ml
infusion) | 7/7 (without
heparin) | (18)d | Patency, infusion
failure, phlebitis | (40) |
| Reid | 1990 | USA, single
center | Adults,
surgical | 20/?c (1 U/ml infusion) | 20/?c (without
heparin) | Teflon (18) | Patency, phlebitis
score | (41) |
| Bassan | 1983 | Country not
mentioned, single center | Adults, MI
suspect | 25/25 (2 U/ml
infusion) | 25/25 (saline
placebo) | –d,e | Phlebitis | (42) |
| Sketch | 1972 | USA, single
center | Adults, CCU | 126/168 (1 U/ml
infusion) | 65/71 (without
heparin) | Polyethylenee | Patency, phlebitis,
occlusion | (43) |
| Wright | 1995 | Australia, single
center | Children, medical
wards | 36/36 (1 U/ml
infusion) | 44/44 (without
heparin) | (22–24)d | Patency, phlebitis,
infusion failure, occlusion | (44) |
Baseline characteristics
Among the 32 studies included in the present review,
the scale ranged from 16 patients/16 catheters to 451
patients/1,257 catheters. In total, 10 studies reported multiple
catheters per patient (15–17,23,25,27,37–39,43),
with the rest of the studies reported a single catheter per
patient. The study populations included pediatric patients
(14,15,21–24,
26–29,32,33,37–39,44),
healthy volunteers and adults (7–9,16,17,
20,30,31,34–36,40–43), and
the administered treatments in all studies primarily consisted of
antibiotics and parenteral nutrition. Furthermore, the origin of
countries reported included the USA (7,8,14,20,26–28,30,32,33,35,43), the
UK (39,40), Germany (38), France (36), the Netherlands (22), Australia (44), Italy (17), Canada (25), Ireland (34), India (15,31) and
China (16). In the infusion
studies, the concentration of heparin varied between 0.1 and 2
U/ml, whereas in the intermittent flush studies the concentration
used varied between 2 and 100 U/ml. Finally, the material of
catheters included Teflon, polyurethane, Neoflon and polyethylene,
and the size of catheters varied between 16 and 26 gauge.
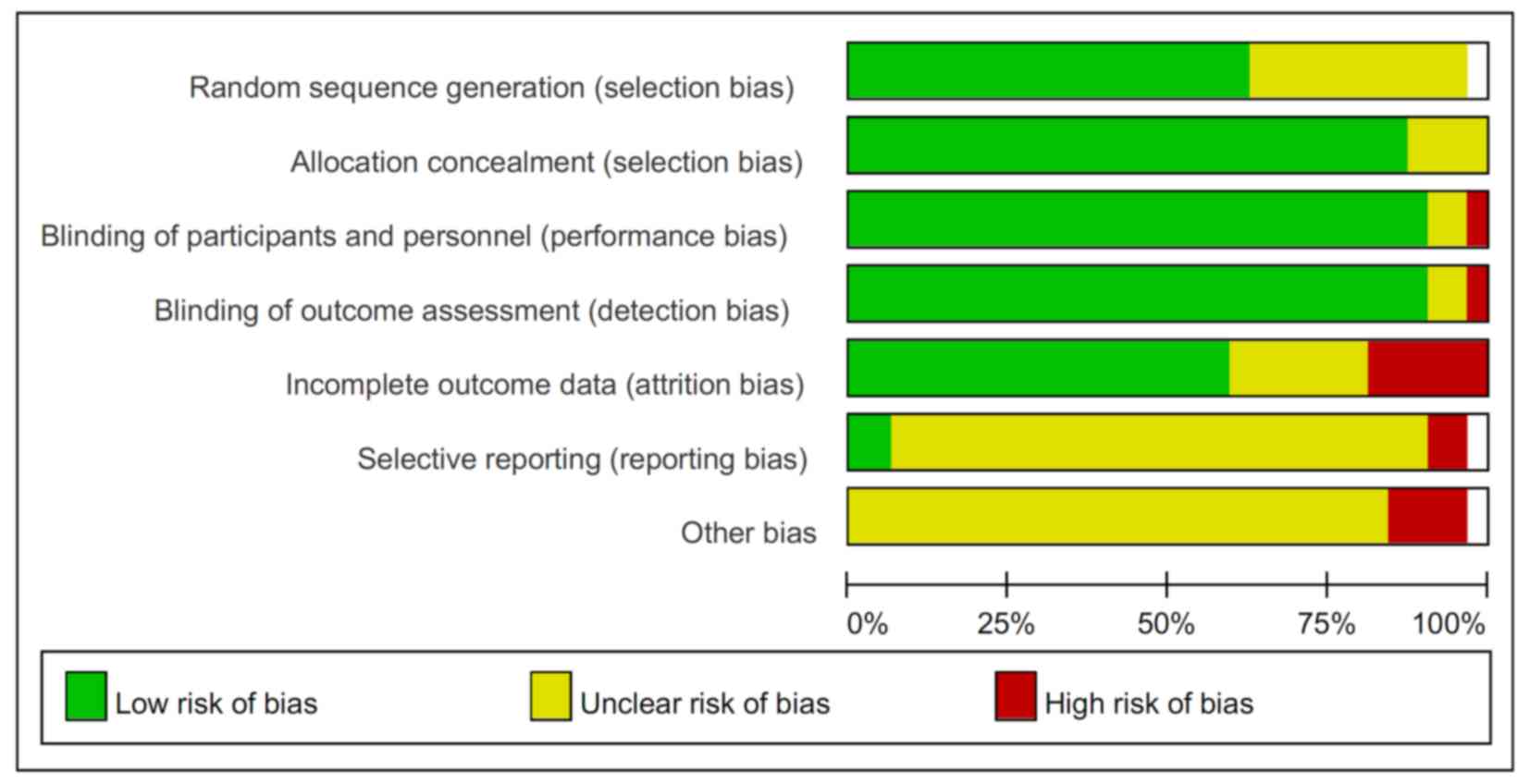
Methodological quality
The majority of the studies demonstrated a low to
unclear level of risk of bias, as shown in Fig. 2. In total, 10 studies did not
properly address the methods for the generation of random sequence
(14,21,28,29,33,36,
38,40–42). The
majority of studies described an adequate method of allocation
concealment, with 5 reported unclear results (8,22,31,40,43).
Furthermore, all studies reported well-defined methods of blinding
except for 2 studies (31,34). In terms of selective reporting and
bias, however, the majority of studies did not provide a clear
description. Although incomplete data were included in 5 studies,
only small portions of subjects were removed following
randomization. In addition, 7 studies did not provide drop-out
details (28,34,40–44).
Meta-analysis
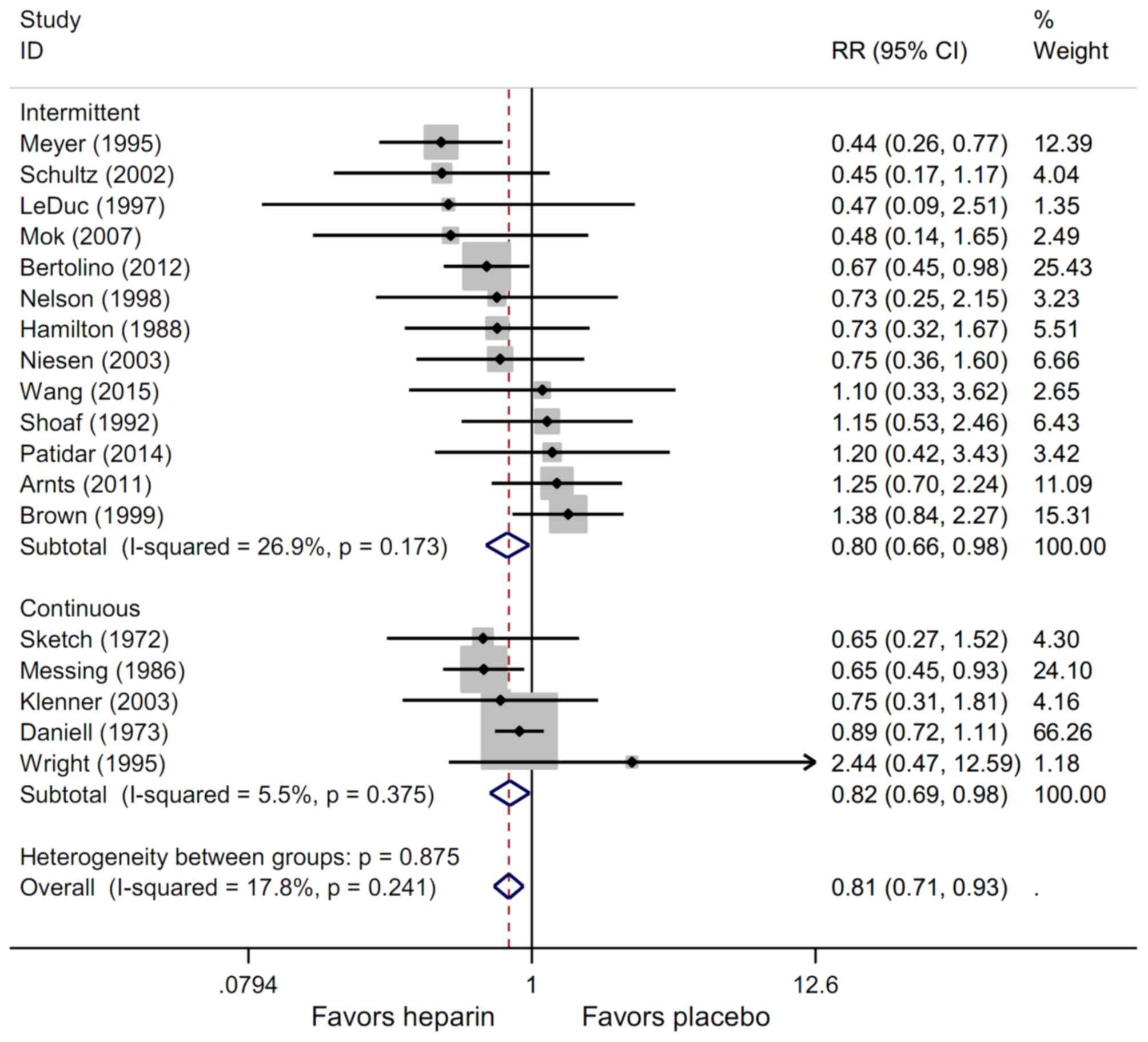
Occlusion
Of the included studies, 21 reported the rates of
occlusion per catheter, whereas 11 studies presented the occlusion
rates per patient. The use of heparin in intermittent flushing lead
to a 20% reduced risk in catheter occlusion [RR, 0.80; 95%
confidence interval (CI), 0.66–0.98; P<0.05], and a similar
reduction of the occlusion rate was exhibited in continuous heparin
infusion studies (RR, 0.82; 95% CI, 0.69–0.98; P<0.05). In
addition, the use of heparin also significantly decreased the
overall risk of occlusion (RR, 0.81; 95% CI, 0.71–0.93; P<0.01).
Finally, no significant heterogeneity was observed among the
studies (intermittent, I2=26.9%; continuous,
I2=5.5%; overall, I2=17.8%; Fig. 3) and no publication bias was noticed
among the studies as indicated by Egger's (continuous, P=0.962;
intermittent, P=0.801; overall, P=0.560) and Begg's (continuous,
P=0.624; intermittent, P=0.464; overall, P=0.554) tests.
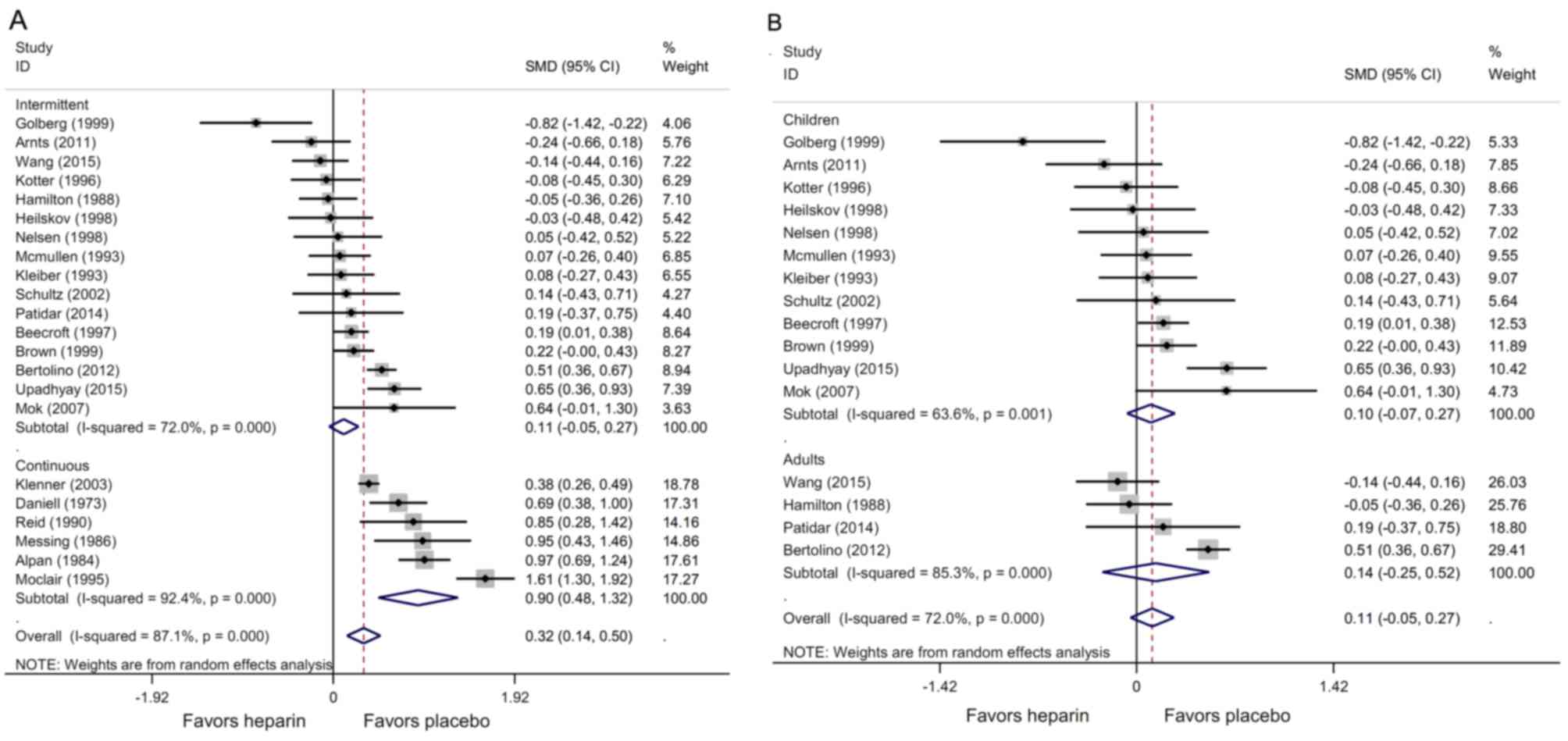
Duration of catheter patency
The duration of catheter patency was reported in 22
studies, including 6 of continuous infusion and 16 of intermittent
flushing. These studies described the duration in h (mean ± SD),
which were summarized in Table I. In
some studies, elective removal was issued for a quantity of
catheters, which were separately recorded in the results. Other
studies directly combined results from both elective and
non-elective catheter removals. As shown in Fig. 4, continuous infusion of heparin
solution in peripheral intravenous catheters significantly
increased the duration of catheter patency (SMD, 0.90; 95% CI,
0.48–1.32; P<0.001) whereas intermittent flushing with heparin
did not display significant differences compared with placebo (SMD,
0.11; 95% CI, −0.05–1.27; P=0.165; Fig.
4A). Furthermore, between-sample heterogeneities were
significant in both groups (continuous, I2=92.4%;
intermittent, I2=72.0%), therefore potential sources of
these observations were sought. The continuous infusion studies
demonstrated no publication bias, as assessed by Egger's (P=0.11)
and Begg's (P=0.57) tests. However, in the intermittent flushing
studies, the Egger's test showed significant publication bias
(P<0.05) whereas the Begg's test did not display any significant
difference. Notably, subgroup analysis revealed that both the
duration of catheter patency (SMD, 0.30; 95% CI, 0.17–0.42;
P<0.01) and occlusion profile (RR, 0.64; 95% CI, 0.48–0.86;
P<0.01) were significantly improved when a higher concentration
of heparin (100 U/ml) was used as an intermittent flushing
solution.
Furthermore, a population-based subgroup analysis
was conducted in the intermittent flushing studies and no
significant changes of catheter patency by heparin were detected in
children (SMD, 0.10; 95% CI, −0.07–0.27; P=0.25) or adult
population (SMD, 0.14; 95% CI, −0.25–0.52; P=0.49). Homogeneity
tests showed persistent between-study heterogeneity in both
children (I2=63.6%) and adults (continuous,
I2=85.3%; Fig. 4B).
Additionally, a univariate meta-regression test showed that the
publication year, generation of random sequence, censor of elective
catheter removal as well as catheter/patient ratio did not
contribute significantly to the heterogeneity observed in the
duration of patency.
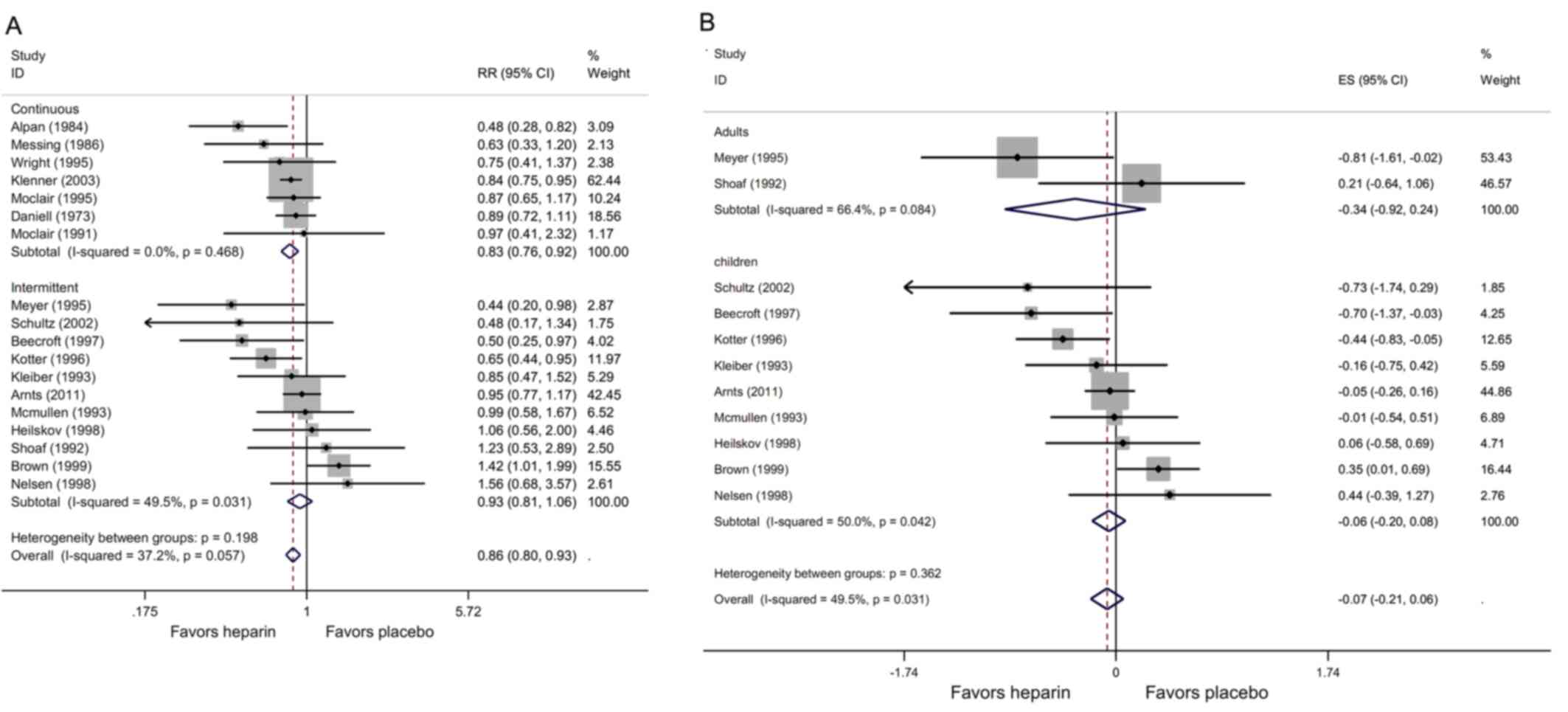
Infusion failure
A total of 7 studies utilizing continuous infusion
of heparin solution and 11 studies testing intermittent flushing
with heparin presented this outcome as dichotomous data. A
usage-based subgroup meta-analysis was performed for each group.
Accordingly, only continuous application of heparin significantly
reduced the risk of infusion failure in peripheral intravenous
catheters (RR, 0.83; 95% CI, 0.76–0.92; P<0.001), whereas
intermittent flushing with heparin failed to show a statistical
difference (RR, 0.93; 95% CI, 0.81–1.06; P=0.28). Nevertheless,
heparin demonstrated a significant overall effect on decreasing
infusion failure in peripheral intravenous catheters (RR, 0.86; 95%
CI, 0.80–0.93; P<0.001). Further analysis showed no significant
between-study heterogeneities (continuous, I2=0%;
intermittent, I2=49.5%; overall, I2=37.2%;
Fig. 5A). There was also no evidence
of potential publication bias among the studies included as
assessed by Begg's (continuous, P=0.453; intermittent, P=0.938;
overall, P=0.678) and Egger's tests (continuous, P=0.261;
intermittent, P=0.425; overall, P=0.935).
When heparin was used as intermittent flushing, no
significant difference of infusion failure was noted in either
children (RR, −0.06; 95% CI, −0.20–0.08; P=0.40) or adult (RR,
−0.34; 95% CI, −0.92–0.24; P=0.26) populations, as indicated by
population-based subgroup tests (Fig.
5B). Further analysis of meta-regression indicated no
significant association between the years of publication,
catheter/patient ratios, censoring for catheter removal, generation
of random sequence and the heterogeneity noticed in infusion
failure.
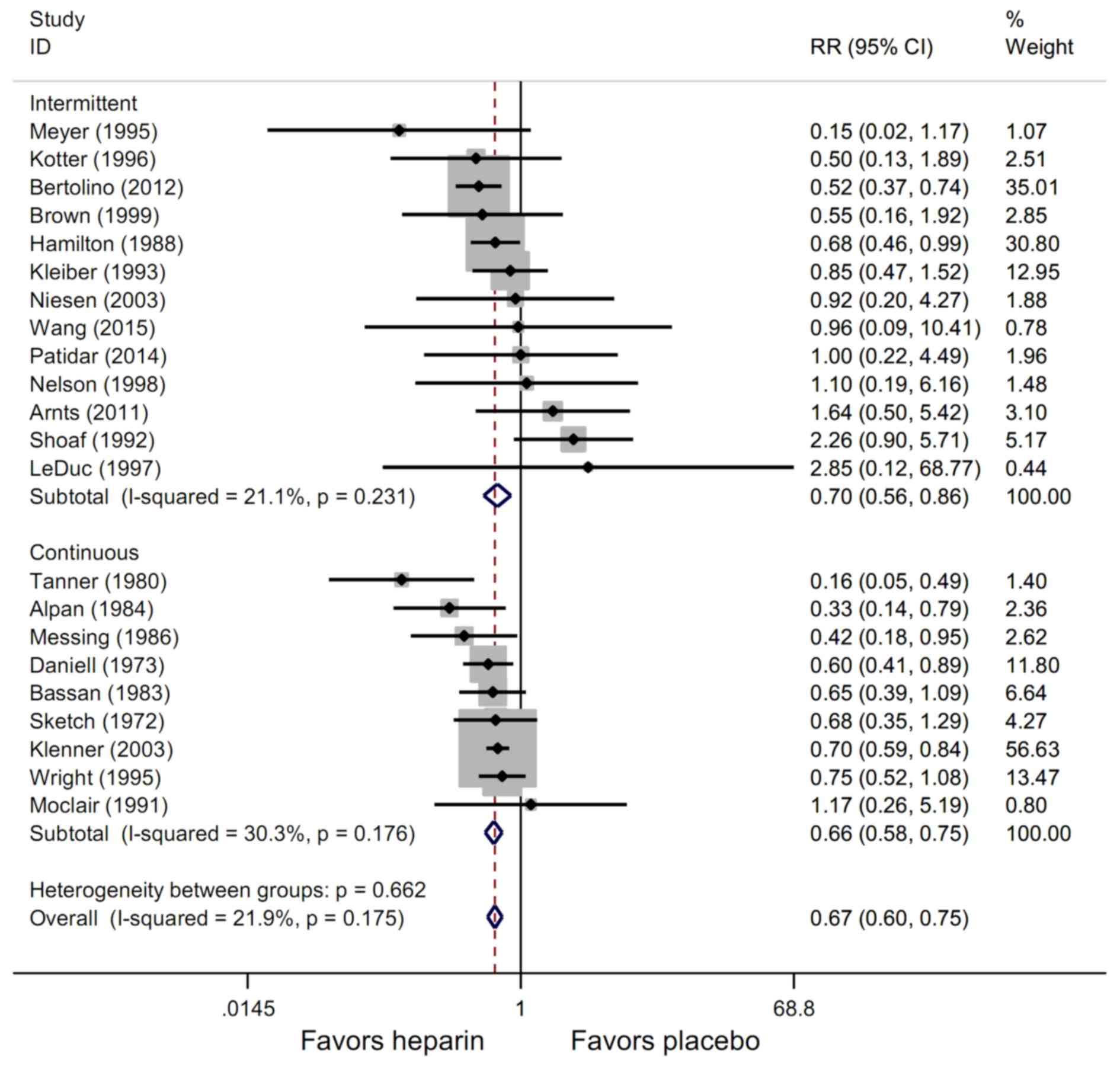
Phlebitis
The majority of included studies reported phlebitis
as an outcome in binary format. According to the meta-analysis, the
use of heparin significantly lowered the rates of phlebitis in both
intermittent flushing (RR, 0.70; 95% CI, 0.56–0.86; P<0.01) and
continuous infusion (RR, 0.66; 95% CI, 0.58–0.75; P<0.001) as
compared with the placebo. The overall effect of heparin on
reducing phlebitis was also statistically significant (RR, 0.67;
95% CI, 0.60–0.75; P<0.001). Furthermore, the tests for
homogeneity revealed a low level of heterogeneity among studies
(continuous, I2=21.1%; intermittent,
I2=30.3%; overall, I2=21.9%; Fig. 6), and no significant publication bias
was indicated by Egger's (continuous, P=0.105; intermittent,
P=0.230; overall, P=0.589) and Begg's (continuous, P=0.095;
intermittent, P=0.807; overall, P=0.527) tests.
Major adverse events
One study reported adverse events, one of which
reported 10 intracranial bleeding events, and 23 episodes of
heparin-induced thrombocytopenia in neonates (38). Other studies only reported
mild-bleedings, and no onset of sepsis or allergic reaction was
noted (17,25,38).
Discussion
Heparin has been utilized as an antithrombotic agent
for maintaining catheters for four decades. Anticoagulation by
heparin is predominantly mediated through antithrombin III in
plasma (45). Due to rapid
pharmacokinetics and a relatively lower cost, heparin is widely and
routinely used in clinical practice. In some countries and medical
facilities, flushing and locking catheters with heparin solutions
are becoming standard procedures. However, a number of clinical
trials studying heparin in catheter maintenance failed to find
significance of its efficacy (8,9,14,23,26).
Therefore, several systematic reviews and meta-analyses are
conducted but their results remain controversial (3,4,11). Whereas many studies focus on central
venous catheters, only a few have investigated the role of heparin
in peripheral catheters. The present study performed an updated
systematic review and meta-analysis of the efficacy of heparin
solution used as both continuous infusion and intermittent flushing
in peripheral venous catheters.
The results of the current meta-analysis
demonstrated that the addition of heparin significantly reduced the
rate of catheter occlusion, infusion failure and prolonged the
duration of catheter patency in continuous infusion of a peripheral
venous catheter. Conversely, heparin also showed a border effect on
reducing occlusion and failed to display improvements in the
duration of patency as well as infusion failure as an intermittent
flushing solution. Nevertheless, a significant decrease was
observed in the rate of phlebitis in both intermittent and
continuous use of heparin.
The majority of infusion studies used low
concentrations of heparin (1 U/ml) (34–39,41–44),
whereas the majority of intermittent flushing studies used higher
concentrations (10–100 U/ml). It is speculated that the difference
of effects between these two distinctive modes of heparin usage may
be due to discrepancies of concentrations. Notably, it was revealed
that there were significant benefits in catheter patency when
heparin was used for intermittent flushing at the highest
concentration of 100 U/ml. In addition, the pooled effect
demonstrated that a higher frequency of flushing with heparin did
not bring any further advantages in catheter patency. Additionally,
one study of intermittent flushing with heparin showed no
significant difference in catheter patency between concentrations
of 1 and 10 U/ml (21). Conversely,
an intergroup difference corresponding to concentration gradients
of heparin was reported in one study using heparin as a continuous
infusion (39).
In 1991, two meta-analyses including randomized and
quasi-randomized studies were published, which reported that
heparin solution was not superior to normal saline in maintaining
patency of vascular catheters (46,47).
Another meta-analysis from 1998, which included only RCTs,
demonstrated different results, in which heparin improved catheter
patency during continuous infusion rather than intermittent
flushing (4). However, in subgroup
analysis, the authors revealed that a higher concentration of
heparin exerted substantial benefits in catheter patency compared
with the placebo. This result is in accordance with the present
findings that a higher concentration of heparin was beneficial in
intermittent flushing. More recently, two updated meta-analyses
reported the efficacy of heparin on catheter patency in adults and
children, respectively. In the first study, which focused on
pediatric patients, heparin was shown to improve catheter patency
while being continuously infused (3). In the second study, which focused on
adult patients, inclusion of heparin in continuous infusion
solutions resulted in improved patency outcomes and less phlebitis
(12). Nonetheless, neither study
reported significant benefits of heparin in intermittent
application. Another systemic review by Shah and Shah (1) focused in neonates but did not conduct a
meta-analysis due to high heterogeneity among the studies included,
in which both semi-randomized and randomized trials were
included.
Besides similar observations of phlebitis in the use
of heparin as a continuous infusion, the present study demonstrated
significant beneficial effects of heparin on preventing phlebitis
as an intermittent flushing solution. Considering a similar
duration of patency and occlusion profiles in the intermittent use
of heparin compared with placebo was demonstrated in the present
results, this improvement in phlebitis by heparin may be
independent of catheter patency. Traditionally, phlebitis is
considered to be caused by thrombosis and is usually called
‘thrombophlebitis’ (48). The
observations of the present study that heparin showed additional
benefits in preventing phlebitis besides anticoagulation may be
explained by its anti-inflammatory role, which has been reported in
sports injuries and inflammatory bowel disease (49,50).
Notwithstanding these benefits, administration of heparin may
result in potential complications such as bleeding,
thrombocytopenia and allergy (51–53).
These drawbacks may discourage the clinical use of heparin at
higher concentrations, although the morbidity of the complications
has been low in previous observations (7,13,16,51,53).
The meta-analysis of the present study showed
improved outcomes of patency in the continuous infusion; however,
the results must be interpreted with caution due to a series of
limitations. First of all, high heterogeneity was observed in the
analysis of duration of catheter patency. Furthermore, a subsequent
meta-regression of the catheter/patient ratio, proper generation of
randomization, year of publication and censoring for elective
withdrawal failed to identify significant sources of heterogeneity.
Additionally, since SMD was used as pooled effects for the
continuous data as h, the discrepancies in the acquisition of
outcomes among different studies may compromise the homogeneity of
the results. Also, it is not possible to delineate the effects of
the catheter material on the current observations in the present
meta-analysis due to insufficient catheter information. The lack of
sub-group studies with concentration gradients made it difficult to
pool a concentration-dependent outcome. Additionally, there are
other causes of bias in this review. For instance, a few studies
included multiple groups that used other agents in combination with
heparin (36,42,43), and
some other studies reported a considerable drop-out rate of the
subjects (9,35,42).
Furthermore, one study reported the median rather than the mean and
SD, and only effect size can be obtained from another (39,44). It
is noteworthy that one study with a large number of patients used
cluster randomization instead of the classical randomization method
(17). In addition, multi-center or
large-scale RCTs were not identified for inclusion in the current
meta-analysis. All of these factors may contribute to the
heterogeneity and bias among the studies and affect the quality of
the meta-analysis.
In conclusion, this updated systematic review and
meta-analysis demonstrated that the use of heparin as a continuous
infusion may significantly improve the patency of peripheral
intravenous catheters, whereas intermittent flushing with heparin
only reduces the rate of occlusion but shows no significant benefit
on the duration of patency and infusion failure. Furthermore, the
present findings suggest that both intermittent and continuous uses
of heparin in peripheral intravenous catheters ameliorate
phlebitis.
Acknowledgements
The authors are grateful to Dr Li Zhu (Soochow
University; Suzhou, China) for his contributions to the search
updates and manuscript preparation.
References
|
1
|
Shah PS and Shah VS: Continuous heparin
infusion to prevent thrombosis and catheter occlusion in neonates
with peripherally placed percutaneous central venous catheters.
Cochrane Database Syst Rev: CD002772. 2008. View Article : Google Scholar
|
|
2
|
Unal S, Ekici F, Cetin II and Bilgin L:
Heparin infusion to prevent umbilical venous catheter related
thrombosis in neonates. Thromb Res. 130:725–728. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kumar M, Vandermeer B, Bassler D and
Mansoor N: Low-dose heparin use and the patency of peripheral IV
catheters in children: A systematic review. Pediatrics.
131:e864–e872. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Randolph AG, Cook DJ, Gonzales CA and
Andrew M: Benefit of heparin in peripheral venous and arterial
catheters: Systematic review and meta-analysis of randomised
controlled trials. BMJ. 316:969–975. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yau JW, Stafford AR, Liao P, Fredenburgh
JC, Roberts R and Weitz JI: Mechanism of catheter thrombosis:
Comparison of the antithrombotic activities of fondaparinux,
enoxaparin, and heparin in vitro and in vivo. Blood. 118:6667–6674.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Daniell HW: Heparin prevention of catheter
thrombosis. JAMA. 216:12001971. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Niesen KM, Harris DY, Parkin LS and Henn
LT: The effects of heparin versus normal saline for maintenance of
peripheral intravenous locks in pregnant women. J Obstet Gynecol
Neonatal Nurs. 32:503–508. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hamilton RA, Plis JM, Clay C and Sylvan L:
Heparin sodium versus 0.9% sodium chloride injection for
maintaining patency of indwelling intermittent infusion devices.
Clin Pharm. 7:439–443. 1988.PubMed/NCBI
|
|
9
|
Shoaf J and Oliver S: Efficacy of normal
saline injection with and without heparin for maintaining
intermittent intravenous site. Appl Nurs Res. 5:9–12. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Robertson-Malt S, Malt GN, Farquhar V and
Greer W: Heparin versus normal saline for patency of arterial
lines. Cochrane Database Syst Rev: CD007364. 2014. View Article : Google Scholar
|
|
11
|
Lopez-Briz E, Garcia V Ruiz, Cabello JB,
Bort-Marti S, Sanchis R Carbonell and Burls A: Heparin versus 0.9%
sodium chloride intermittent flushing for prevention of occlusion
in central venous catheters in adults. Cochrane Database Syst Rev:
CD008462. 2014. View Article : Google Scholar
|
|
12
|
Kumar M, Vandermeer B, Bassler D and
Mansoor N: Low-dose heparin for prolonging the patency of
peripheral intravenous catheters in adults - a systematic review
and meta-analysis. Int J Med. 2:13–21. 2014. View Article : Google Scholar
|
|
13
|
Ahmed I, Majeed A and Powell R: Heparin
induced thrombocytopenia: Diagnosis and management update. Postgrad
Med J. 83:575–582. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kleiber C, Hanrahan K, Fagan CL and
Zittergruen MA: Heparin vs. saline for peripheral i.v. locks in
children. Pediatr Nurs. 19:405–409, 376. 1993.PubMed/NCBI
|
|
15
|
Upadhyay A, Verma KK, Lal P, Chawla D and
Sreenivas V: Heparin for prolonging peripheral intravenous catheter
use in neonates: A randomized controlled trial. J Perinatol.
35:274–277. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wang R, Zhang MG, Luo O, He L, Li JX, Tang
YJ, Luo YL, Zhou M, Tang L, Zhang ZX, et al: Heparin saline versus
normal saline for flushing and locking peripheral venous catheters
in decompensated liver cirrhosis patients: A randomized controlled
trial. Medicine (Baltimore). 94:e12922015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bertolino G, Pitassi A, Tinelli C,
Staniscia A, Guglielmana B, Scudeller L and Balduini C Luigi:
Intermittent flushing with heparin versus saline for maintenance of
peripheral intravenous catheters in a medical department: A
pragmatic cluster-randomized controlled study. Worldviews Evid
Based Nurs. 9:221–226. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Higgins JP, Altman DG, Gøtzsche PC, Jüni
P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA, et
al: The Cochrane Collaboration's tool for assessing risk of bias in
randomised trials. BMJ. 343:d59282011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Moher D, Liberati A, Tetzlaff J and Altman
DG; PRISMA Group, : Preferred reporting items for systematic
reviews and meta-analyses: The PRISMA statement. PLoS Med.
6:e10000972009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Meyer BA, Little CJ, Thorp JA, Cohen GR
and Yeast JD: Heparin versus normal saline as a peripheral line
flush in maintenance of intermittent intravenous lines in obstetric
patients. Obstet Gynecol. 85:433–436. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mok E, Kwong TK and Chan MF: A randomized
controlled trial for maintaining peripheral intravenous lock in
children. Int J Nurs Pract. 13:33–45. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Arnts IJ, Heijnen JA, Wilbers HT, van der
Wilt GJ, Groenewoud JM and Liem KD: Effectiveness of heparin
solution versus normal saline in maintaining patency of intravenous
locks in neonates: A double blind randomized controlled study. J
Adv Nurs. 67:2677–2685. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kotter RW: Heparin vs saline for
intermittent intravenous device maintenance in neonates. Neonatal
Netw. 15:43–47. 1996.PubMed/NCBI
|
|
24
|
Beecroft PC, Bossert E, Chung K, Greene
CV, Johnson LC, Jury D, Kent Y, O'Byrne C, Powell SL and Sperhac
AM: Intravenous lock patency in children: dilute heparin versus
saline. J Pediatr Pharm Pract. 2:211–223. 1997.
|
|
25
|
Brown K, Tay-Uyboco JS and McMillan DD:
Heparin is not required for peripheral intravenous locks in
neonates. Paediatr Child Health. 4:39–42. 1999.PubMed/NCBI
|
|
26
|
Heilskov J, Kleiber C, Johnson K and
Miller J: A randomized trial of heparin and saline for maintaining
intravenous locks in neonates. J Soc Pediatr Nurs. 3:111–116. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nelson TJ and Graves SM: 0.9% sodium
chloride injection with and without heparin for maintaining
peripheral indwelling intermittent-infusion devices in infants. Am
J Health Syst Pharm. 55:570–573. 1998.PubMed/NCBI
|
|
28
|
Schultz AA, Drew D and Hewitt H:
Comparison of normal saline and heparinized saline for patency of
IV locks in neonates. Appl Nurs Res. 15:28–34. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Golberg M, Sankaran R, Givelichan L and
Sankaran K: Maintaining patency of peripheral intermittent infusion
devices with heparinized saline and saline. Neonatal Intensive
Care. 12:18–22. 1999.
|
|
30
|
Ashton J, Gibson V and Summers S: Effects
of heparin versus saline solution on intermittent infusion device
irrigation. Heart Lung. 19:608–612. 1990.PubMed/NCBI
|
|
31
|
Patidar AB, Choudhary M, Bindu K and Midha
V: Comparative efficacy of heparin saline and normal saline flush
for maintaining patency of peripheral intravenous lines: A
randomized control trial. IJHSR. 4:159–166. 2014.
|
|
32
|
LeDuc K: Efficacy of normal saline
solution versus heparin solution for maintaining patency of
peripheral intravenous catheters in children. J Emerg Nurs.
23:306–309. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
McMullen A, Fioravanti ID, Pollack V,
Rideout K and Sciera M: Heparinized saline or normal saline as a
flush solution in intermittent intravenous lines in infants and
children. MCN Am J Matern Child Nurs. 18:78–85. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Tanner WA, Delaney PV and Hennessy TP: The
influence of heparin on intravenous infusions: A prospective study.
Br J Surg. 67:311–312. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Daniell HW: Heparin in the prevention of
infusion phlebitis. A double-blind controlled study. JAMA.
226:1317–1321. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Messing B, Leverve X, Rigaud D, Krummel Y,
Botta D, Latarget J, Mudry P and Guignier M: Peripheral venous
complications of a hyperosmolar (960 mOsm) nutritive mixture: The
effect of heparin and hydrocortisone. A multicenter double-blinded
random study in 98 patients. Clin Nutr. 5:57–61. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Alpan G, Eyal F, Springer C, Glick B,
Goder K and Armon J: Heparinization of alimentation solutions
administered through peripheral veins in premature infants: A
controlled study. Pediatrics. 74:375–378. 1984.PubMed/NCBI
|
|
38
|
Klenner AF, Fusch C, Rakow A, Kadow I,
Beyersdorff E, Eichler P, Wander K, Lietz T and Greinacher A:
Benefit and risk of heparin for maintaining peripheral venous
catheters in neonates: A placebo-controlled trial. J Pediatr.
143:741–745. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Moclair A and Bates I: The efficacy of
heparin in maintaining peripheral infusions in neonates. Eur J
Pediatr. 154:567–570. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Moclair AE, Moselhi M, Benjamin IS and
Hecker JF: Total parenteral nutrition via a peripheral vein: A
comparison of heparinised and non-heparinised regimens. Int J Pharm
Pract. 1:38–40. 1991. View Article : Google Scholar
|
|
41
|
Reid I, Keane FBV, Monson JRT and Tanner
WA: Thrombophlebitis following peripherally administered parenteral
nutrition-A randomized clinical study of the effect of infusion
additives. Surg Res Commun. 9:69–77. 1990.
|
|
42
|
Bassan MM and Sheikh-Hamad D: Prevention
of lidocaine-infusion phlebitis by heparin and hydrocortisone.
Chest. 84:439–441. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Sketch MH, Cale M, Mohiuddin SM and Booth
RW: Use of percutaneously inserted venous catheters in coronary
care units. Chest. 62:684–689. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Wright A, Hecker J and McDonald G: Effects
of low-dose heparin on failure of intravenous infusions in
children. Heart Lung. 24:79–82. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Anderson AJ, Krasnow SH, Boyer MW,
Raucheisen ML, Grant CE, Gasper OR, Hoffmann JK and Cohen MH:
Hickman catheter clots: A common occurrence despite daily heparin
flushing. Cancer Treat Rep. 71:651–653. 1987.PubMed/NCBI
|
|
46
|
Goode CJ, Titler M, Rakel B, Ones DS,
Kleiber C, Small S and Triolo PK: A meta-analysis of effects of
heparin flush and saline flush: Quality and cost implications. Nurs
Res. 40:324–330. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Peterson FY and Kirchhoff KT: Analysis of
the research about heparinized versus nonheparinized intravascular
lines. Heart Lung. 20:631–640. 1991.PubMed/NCBI
|
|
48
|
Brodin-Sartorius A, Martinez F and
Legendre C: Treatment of superficial thrombophlebitis. N Engl J
Med. 364:380–381. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Tyrrell DJ, Horne AP, Holme KR, Preuss JM
and Page CP: Heparin in inflammation: Potential therapeutic
applications beyond anticoagulation. Adv Pharmacol. 46:151–208.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Folwaczny C, Wiebecke B and Loeschke K:
Unfractioned heparin in the therapy of patients with highly active
inflammatory bowel disease. Am J Gastroenterol. 94:1551–1555. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Pföhler C, Müller CS, Pindur G, Eichler H,
Schäfers HJ, Grundmann U and Tilgen W: Delayed-type heparin
allergy: Diagnostic procedures and treatment alternatives-a case
series including 15 patients. World Allergy Organ J. 1:194–199.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Karaaslan H, Peyronnet P, Benevent D,
Lagarde C, Rince M and Leroux-Robert C: Risk of heparin
lock-related bleeding when using indwelling venous catheter in
haemodialysis. Nephrol Dial Transplant. 16:2072–2074. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Mohamed M, Hayes R and Mosetlhi T: A man
with acute venous thromboembolism and thrombocytopenia. Heparin
induced thrombocytopenia. BMJ. 348:g11642014. View Article : Google Scholar : PubMed/NCBI
|