Introduction
The use of 64-slice spiral computed tomography (CT)
imaging of the urinary tract provides the benefits of fastness, a
wide scan range, high Z-axis resolution and little interference
from the surrounding organs, such as the intestinal tract (1). This imaging technique is unparalleled
for the diagnosis and three-dimensional (3D) display of urinary
tract obstruction (2,3). With a standard CT scan of the urinary
tract, images are captured during the arterial, parenchymal and
excretory phases, and a full-range non-enhanced scan may be
required at times. This not only prolongs the total scan time and
therefore time spent in the CT scanner, but also exposes the
patient to a higher X-ray dose (4).
However, single scan radiation dose is small and imaging time is
short, and is therefore a feasible operation (5). Based on B-mode ultrasound or clinical
manifestations, 46 cases of urinary tract obstruction with unknown
causes were selected for inclusion in the current study. Patients
received CT scans with different delay times during the excretory
phase. The aim of the current study was to assess the single
excretory phase diagnostic value of 64-slice spiral CT for urinary
tract obstruction.
Materials and methods
Clinical data
Between January 2013 and January 2015, urinary tract
obstruction of varying degrees was diagnosed by B-mode ultrasound
imaging and clinical manifestations, including back pain and
hematuria, in 46 cases at Department of CT, the Second Affiliated
Hospital of Harbin Medical University (Harbin, China). Of the 46
patients, 32 were male and 21 were female. The patient's age ranged
from 6 to 71 years old. A total of 43 patients reported lower back
pain and 32 patients exhibited hematuria. The study included
patients who had urinary obstruction, and excluded patients who had
undergone kidney transplantation, dialysis or were allergic to
contrast agents. The present study was approved by the
Institutional Review Board of the Second Affiliated Hospital of
Harbin Medical University (Harbin, China) and written informed
consent was obtained from each patient after the nature of the
procedure had been fully explained.
Examination method and scan
preparation
The patients drank 200 ml of water prior to the CT
scans. Then, using a high-pressure injector, 70–90 ml of non-ionic
contrast agent was injected at a rate of 2–3 ml/sec via the medial
cubital vein. Depending on the severity of the urinary tract
obstruction, as indicated by B-mode ultrasound, the urinary tract
was subjected to a single 64-slice spiral CT urography during the
excretory phase for 20–30, 30–60 or 50–180 min for mild, moderate
and severe conditions, respectively. In combination with
renography, the scan delay time was increased for patients with
poor renal function. According to the extent of the renal index, in
which the damage ranged from 20 to 45%, the scan delay time was
increased by 30–60 min as described previously (2–4).
The severity of hydronephrosis was classified based
on the B-mode ultrasound results according to the following
criteria: Mild hydronephrosis, a dilation of one or more renal
calyces with mild pyelic separation and pyelectasia, but without
parenchymal thinning under compression; moderate hydronephrosis, a
dilation of all renal calyces with parenchymal thinning under
compression, but still maintaining a thickness >5 mm; severe
hydronephrosis, a dilation of all renal calyces with parenchymal
thinning and a thickness <5 mm.
Scanning method
To perform scans on group 1 (n=46), a GE Light Speed
VCT 64-slice CT scanner (GE Healthcare, Chicago, IL, USA) was used
(120 kV, 200–380 mA). Three scan sequences of the standard scan
were obtained for the arterial, parenchymal and excretory phases.
For the first two phases, the scan range only consisted of the
kidneys; for the excretory phase, the scan was performed from the
kidneys to the symphysis pubis. The two sequences obtained during
the arterial and parenchymal phases were deleted after the X-ray
dose administered was measured. Only the excretory phase scan was
used for group 2 (n=46).
Image reconstruction
All original images were uploaded to the workstation
for imaging analysis. The reconstruction method included
volume-rendering (VR), maximum intensity projection (MIP),
multi-planar reformating (MPR), and curved planar reformating (CPR)
using standard procedures (2).
Statistical analysis
Continuous variables were expressed as the mean ±
standard deviation and categorical variables were expressed as
frequency or percentage. P<0.05 was considered to indicate a
statistically significant difference. All statistical analysis was
performed by using commercially available software (SPSS18.0; SPSS,
Inc., Chicago, IL, USA).
Results
Patient diagnosis
The excretory phase scan indicated all the patients
suffered from ureter obstruction, and the diagnosis rate was 100%
compared with clinical outcomes including surgery and ureteroscopy.
Of the 46 patients in the present study, the obstructed ureter was
fully displayed in the first single excretory phase CT urography
with good continuity in 96% of cases. The remaining 4% patients
were successfully confirmed with ureter obstruction after the
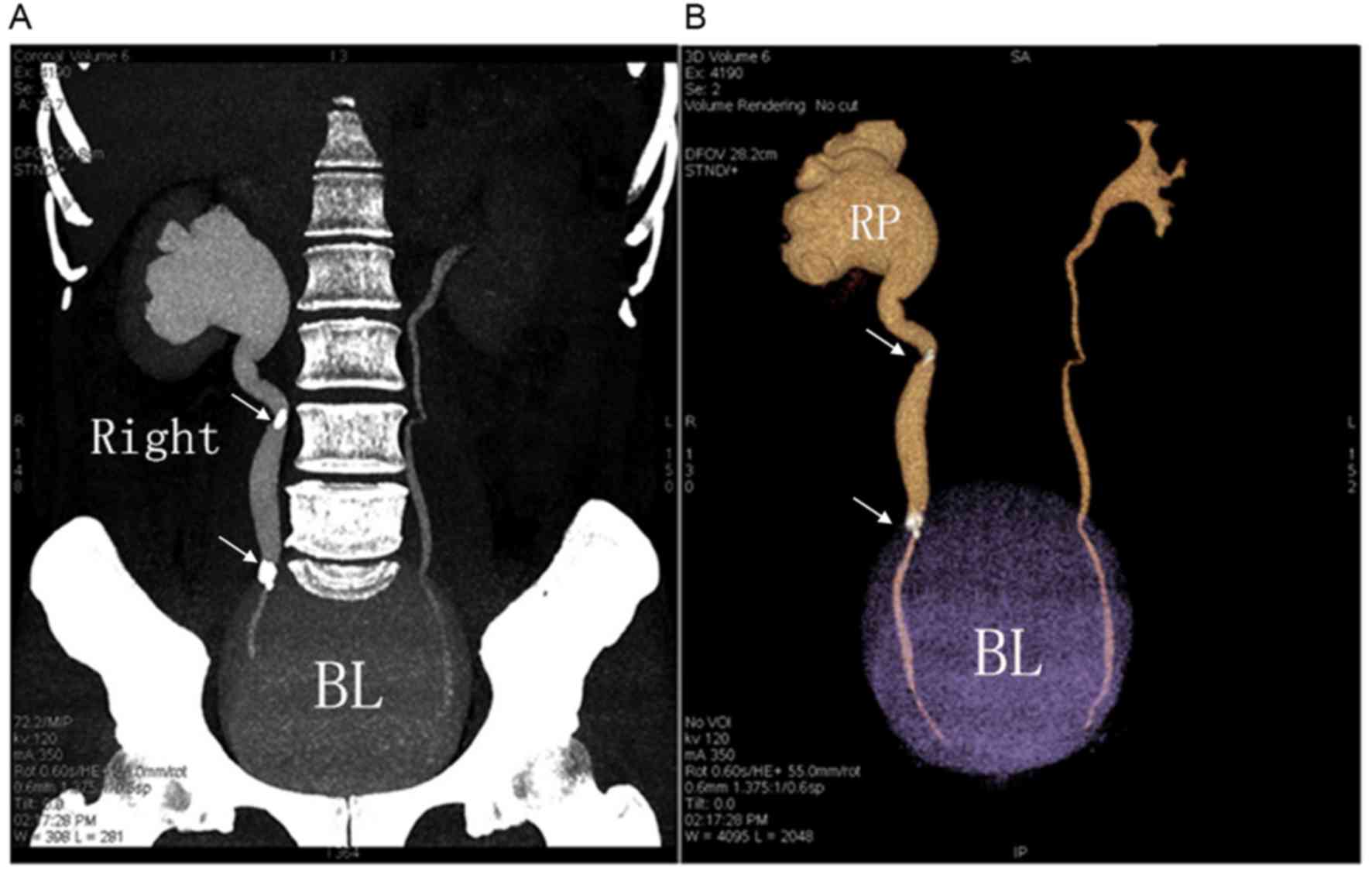
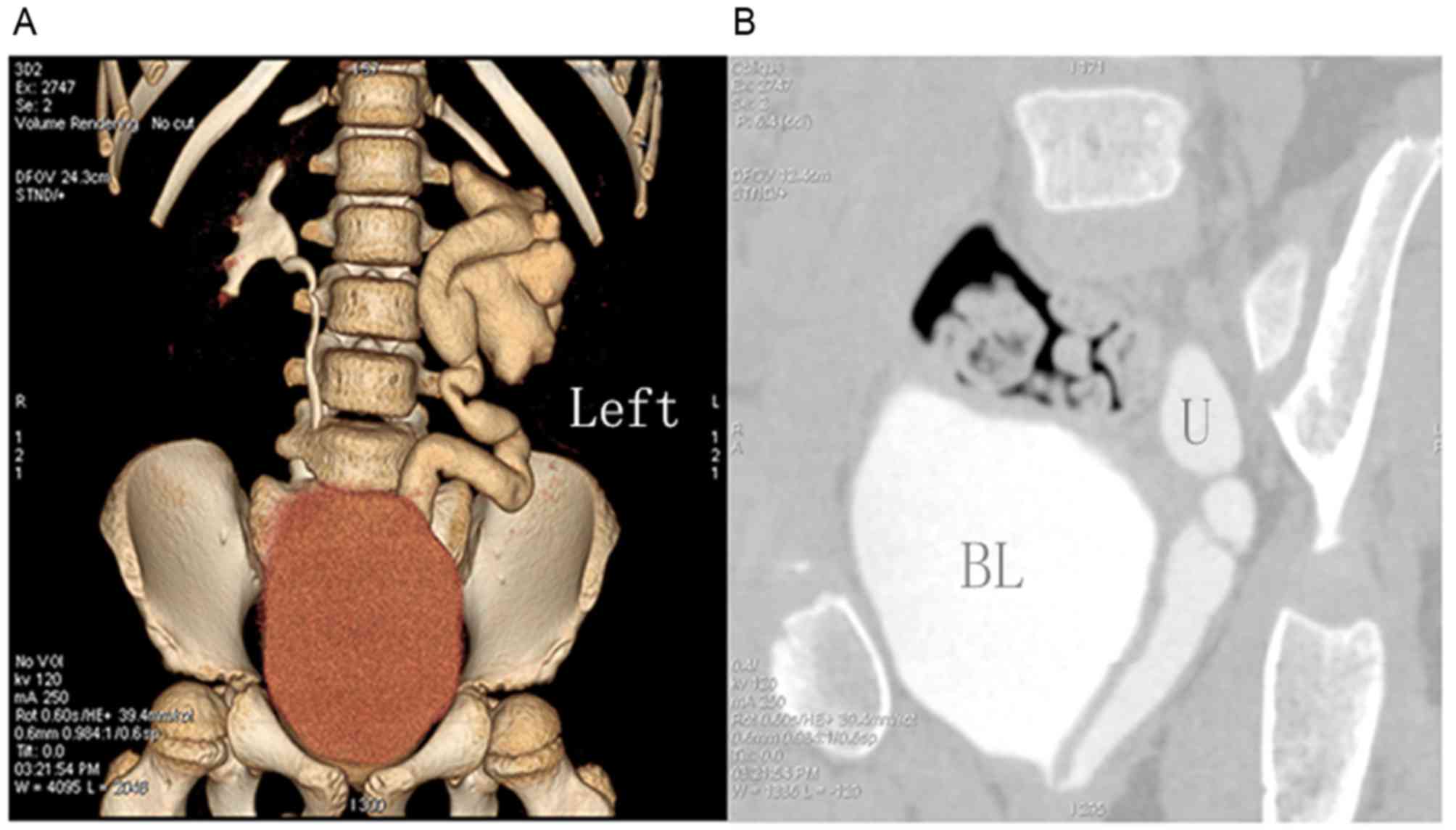
second excretory phase CT scan. Of the 46 patients with pelvic and
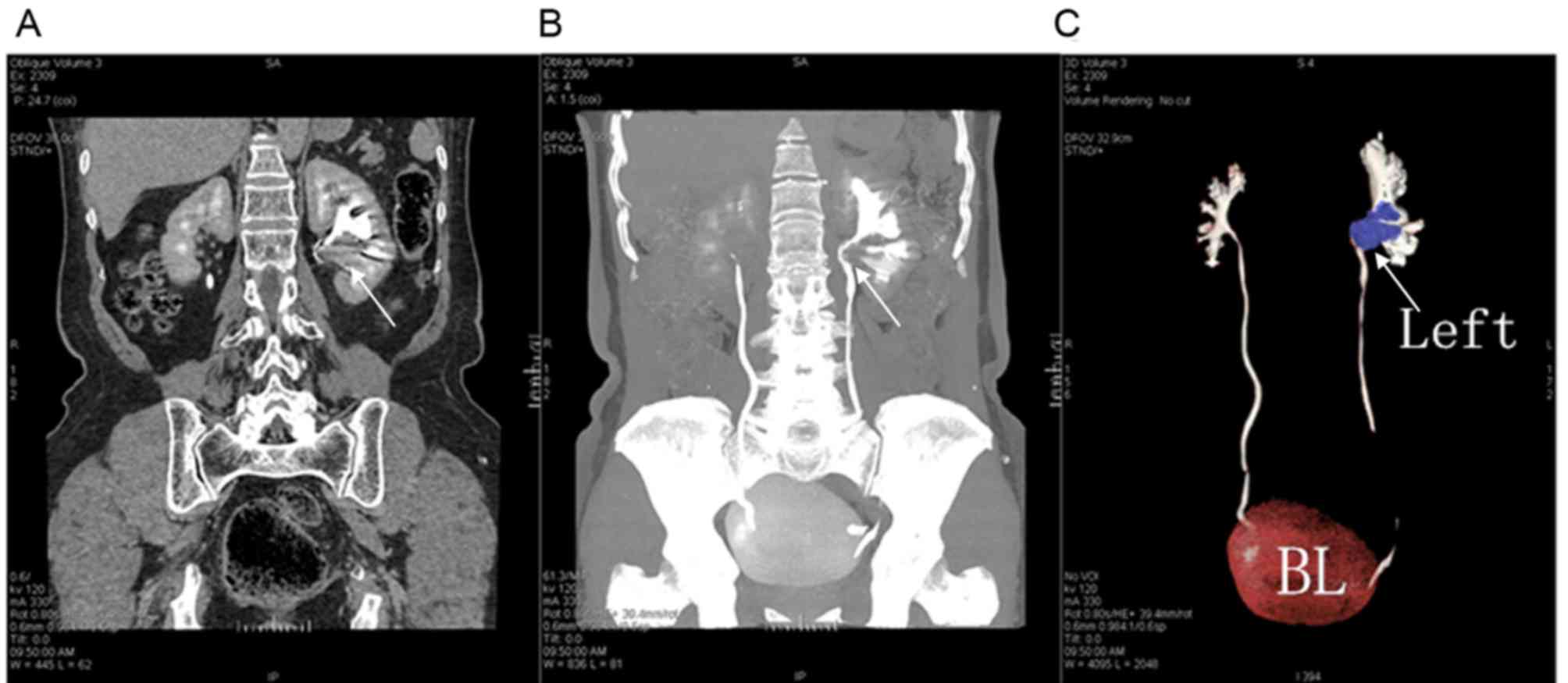
ureteral diseases, 18 had pelvic and ureteral calculi (Fig. 1). In addition, 12 patients had
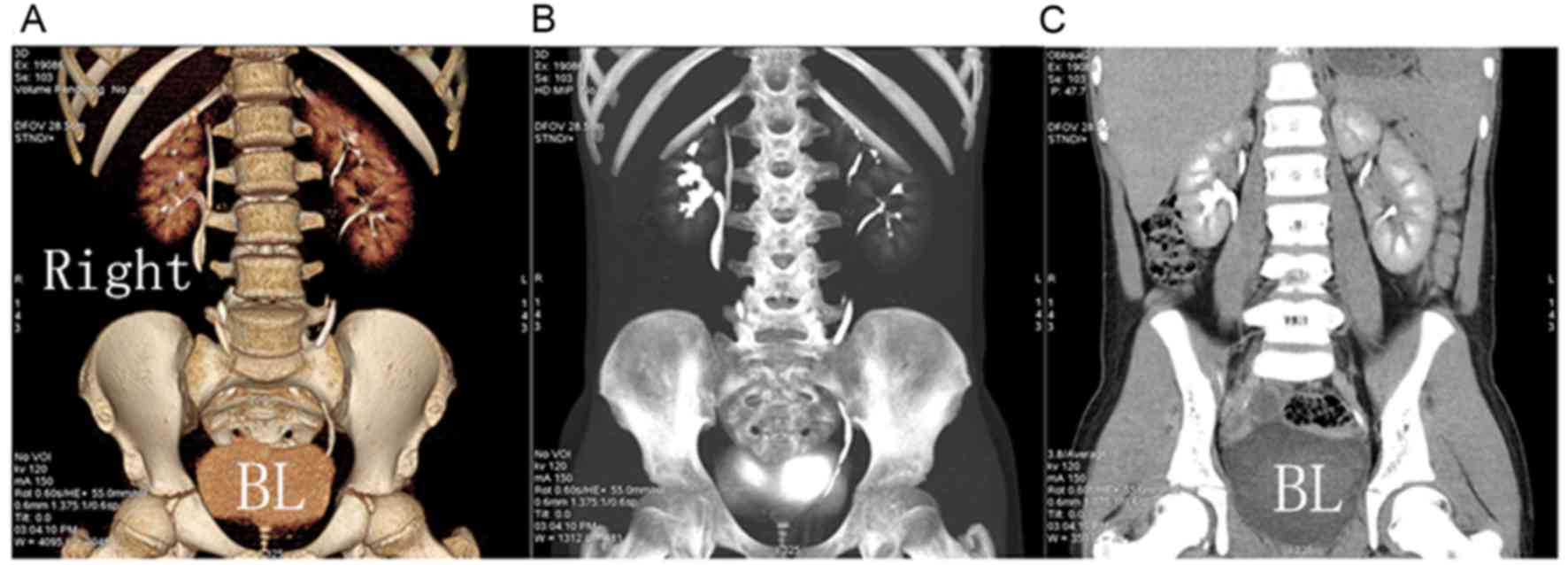
congenital malformations; double pelvis and ureters in 5 cases
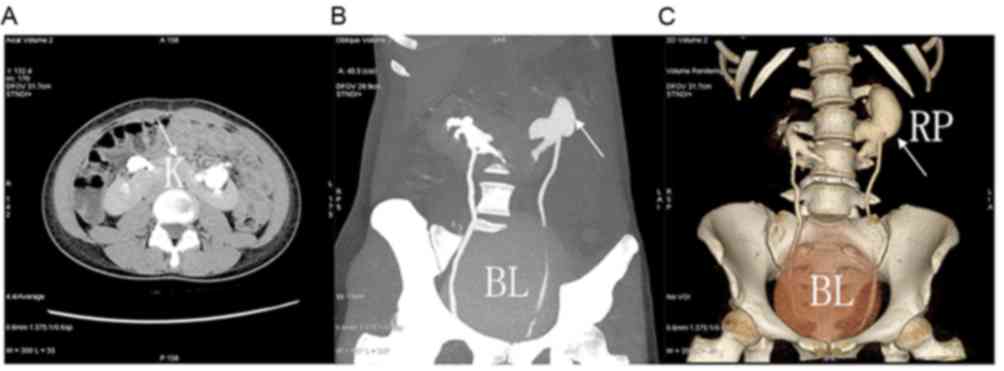
(Fig. 2), horseshoe kidneys in 2
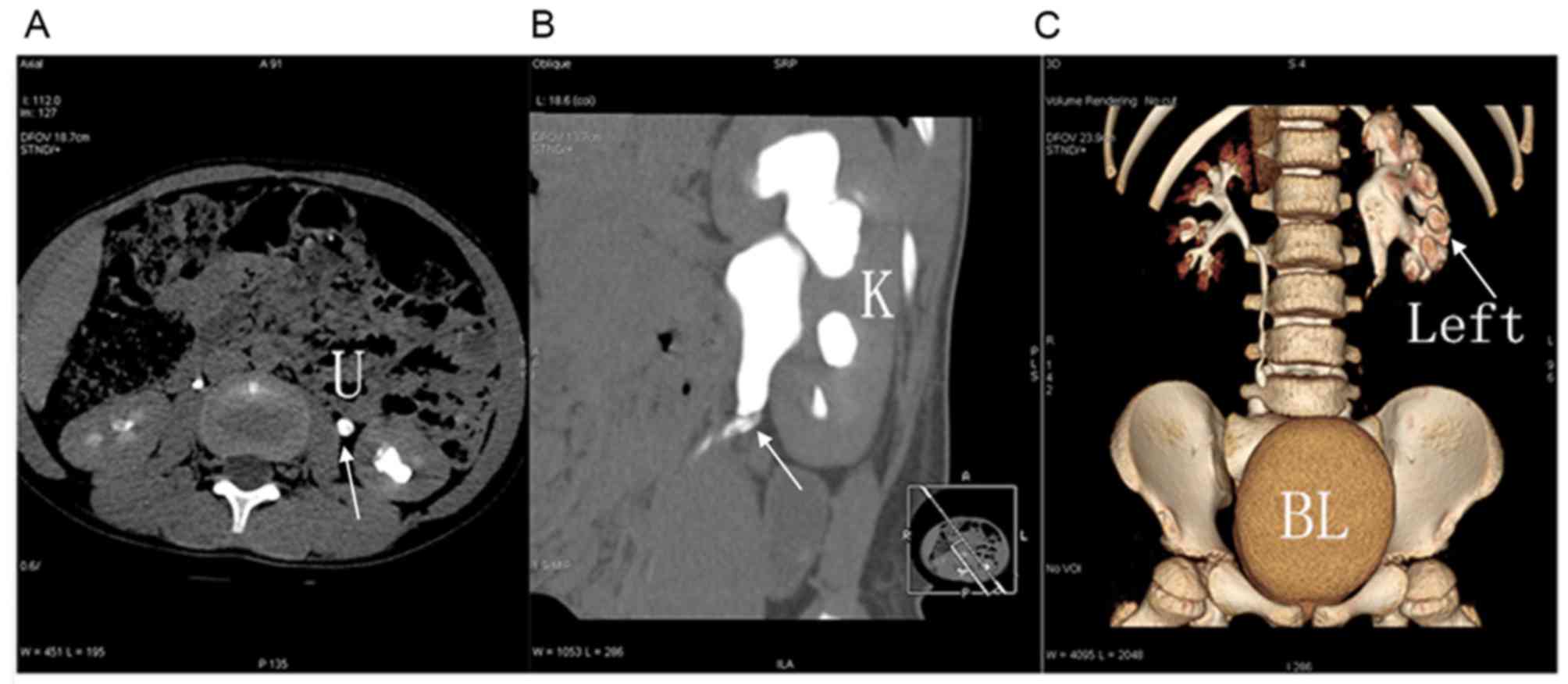
cases (Fig. 3), ureteral valve
disease in 2 cases (Fig. 4),
congenital mega ureter in 2 cases (Fig.
5) and ureteropelvic junction tortuosity and stricture in 1
case. A total of 3 patients exhibited a ureteral stricture caused
by urinary tract infections (urinary tuberculosis in 2 cases and
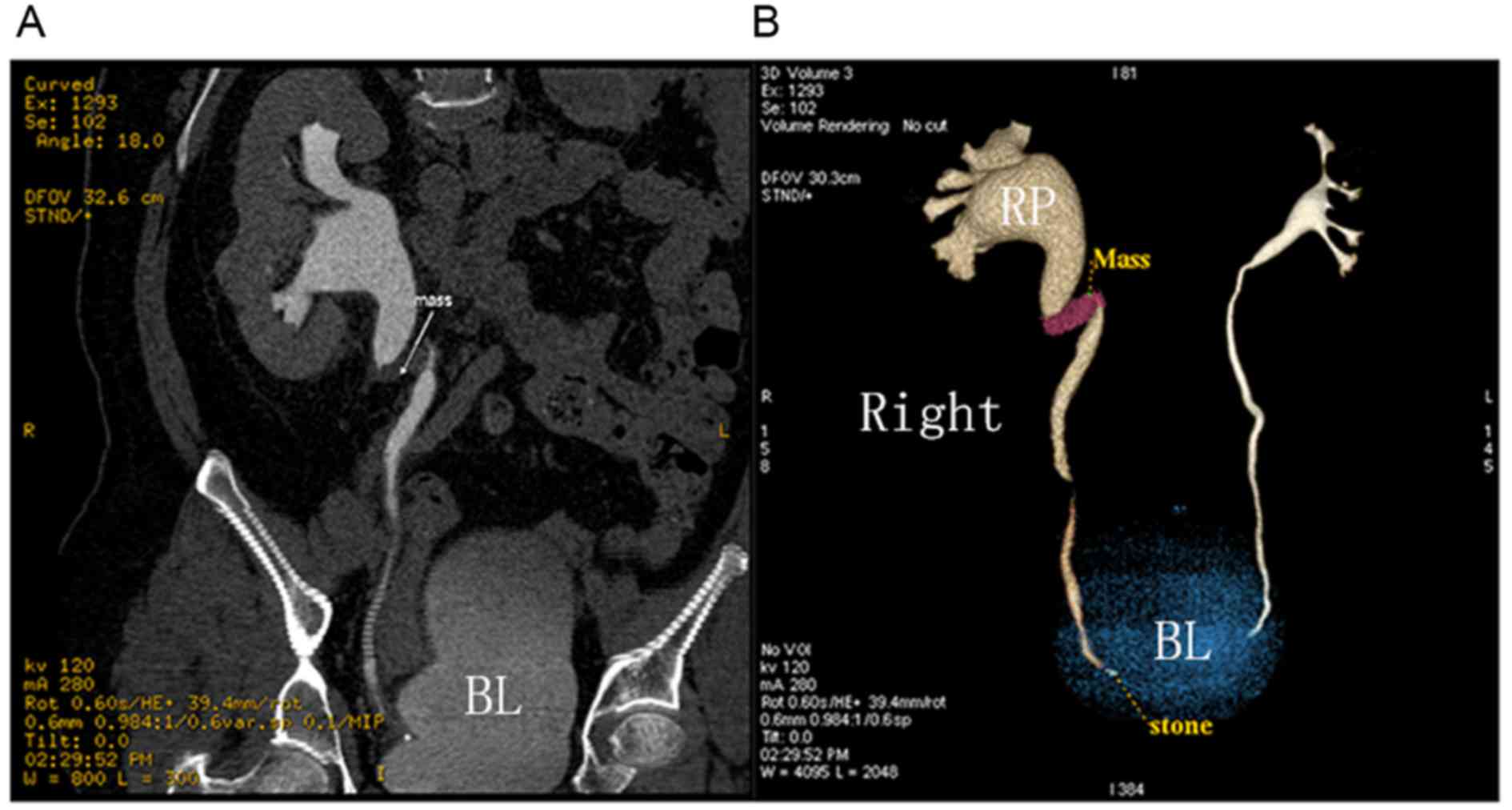
inflammatory stricture in 1 case). Furthermore, 13 patients had
malignant tumors of the urinary tract, including pelvis or ureter
cancer in 9 cases (Figs. 6 and
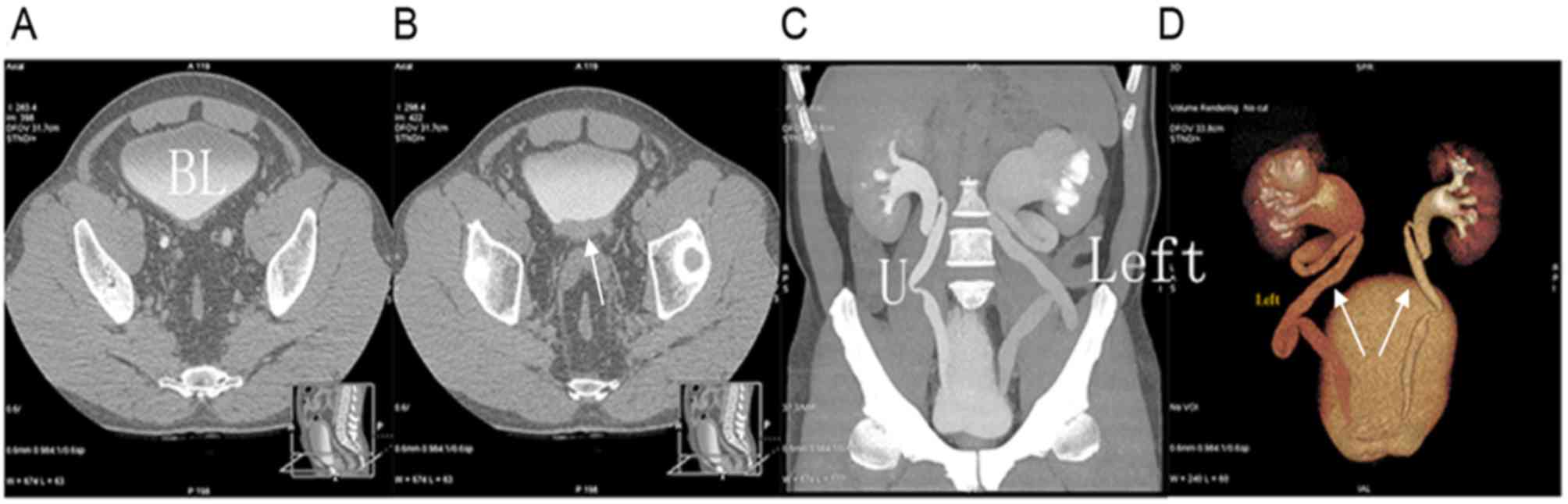
7) and bladder cancer with ureteral
involvement in 4 cases (Fig. 8).
Radiation dosages
The average X-ray dose planned for the standard CT
scan of the urinary tract was 14.11±5.45 mSv, while the actual
X-ray dose administered for CT scan during excretory phase was
9.01±4.56 mSv (data not shown). This difference was of statistical
significance between groups 1 and 2 (t=15.36; P<0.01).
Discussion
Multi-slice spiral CT scanning of the urinary tract
has been identified to have wide applications in the clinics
(6). Conventional procedures require
an extensive scan scope, a considerable number of scan sequences
and a long duration of patient presence in the CT scanner.
Furthermore, patients are exposed to a high X-ray dose using
standard CT imaging. Reducing the duration of scanning and the
X-ray dose that the patient is exposed to during CT imaging of the
urinary tract are research topics that are increasingly drawing
attention (7–9).
CT imaging of the urinary tract can be applied to
diagnose lesions in any part of the urinary system, including the
kidneys, ureter and bladder. Of the various benefits displayed by
multi-slice CT technique for the diagnosis of urinary tract
obstruction, 3D display of the excretory phase is of particular
benefit (6). However, single scan
radiation doses are small and the imaging time is short; therefore,
this technique is feasible (6). By
allocating a different scanning time (30–60 min) for different
severities of urinary tract obstruction, the delay time is
prolonged for those with poor renal function based on renography
results. Of the 46 patients with pelvic and ureteral diseases, CT
scanning during the excretory phase diagnosed 18 cases of pelvic
and ureteral calculi, 12 cases of congenital malformations (double
pelvis and ureters in 5 cases, horseshoe kidneys in 2 cases,
Ureteral valve diseasein 2 cases, congenital megaureter in 2 cases
and ureteropelvic junction tortuosity and stricture in 1 case). In
addition, 3 patients exhibited ureteral stricture caused by urinary
tract infections (urinary tuberculosis in 2 cases and inflammatory
stricture in 1 case), 13 patients had malignant tumors of the
urinary tract (pelvis or ureter cancer in 9 cases and bladder
cancer with ureteral involvement in 4 cases). The diagnosis rate of
urinary tract obstruction was 100% for all patients at the
obstruction sites, diseased sites and the full length of ureter on
the affected side. The average X-ray dose planned for the standard
CT scan of the urinary tract was 14.11±5.45 mSv, and the actual
X-ray dose administered for CT scan during excretory phase was
9.01±4.56 mSv. CT scanning was performed at a standard voltage of
120 kV for all patients. Compared with conventional imaging
procedures, CT scanning during the excretory phase alone reduces
the scanning time and X-ray dose by >30% (6). However, this reduction would be
increased at a lower kV value, as indicated by a previous report
(2).
B-mode ultrasound and intravenous pyelogram (IVP)
imaging are common tools for diagnosing urinary tract obstruction,
with the benefits of being simple procedures that are widely
available (10). However, because of
the inherent physical properties of these two techniques, their
detection rate of urinary tract obstruction remains low (10). Certain researchers advocate the use
of abdominal compression during CT scanning of the urinary tract
(11,12). However, abdominal compression is
unfavorable for maintaining the integrity of the urinary system
(12), particularly in patients with
urinary tract obstruction, where the retention of the contrast
agent in the ureter requires a lack of compression. Of the 46
patients with urinary tract obstruction included in the present
study, the obstructed ureter was fully displayed in the first CT
scan during excretory phase with good continuity in 96% of cases.
In the remaining 4% patients with ureter obstruction, obstruction
was successfully indicated after the second excretory phase CT
scan.
The present study was limited by a small sample size
and the absence of an objective estimate of the scan start time for
excretory phase. For 2 patients with severe hydronephrosis, the
scan of the excretory phase started too early and satisfactory
excretory phase images were only obtained at the correct time
during the second scan. Furthermore, tumors were scanned during the
excretory phase without staging or blood supply assessment. For 1
patient with a pelvis tumor leading to hydronephrosis, scanning
during the excretory phase failed to detect the presence of tumor
thrombi in the renal vein. The tumor staging was performed through
multi-phase scanning.
In conclusion, the results of the present study
indicate that CT scanning of the urinary tract during the excretory
phase is easy to implement, Single scan radiation dose is small and
imaging time is short. The excretory phase CT scanning can assess
the obstruction site and nature of obstruction, and has diagnostic
value for urinary tract obstruction.
Acknowledgements
The present study was supported by the Young and
Middle-aged Scientific Research Innovation Fund of the Second
Affiliated Hospital of Harbin Medical University (grant no.
CX2016-01).
References
|
1
|
Stacul F, Rossi A and Cova MA: CT
urography: The end of IVU? Radiol Med. 113:658–669. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Van Der Molen AJ, Cowan NC, Mueller-Lisse
UG, Nolte-Ernsting CC, Takahashi S and Cohan RH: CT urography:
Definition, indications and techniques. A guideline for clinical
practice. Eur Radiol. 18:4–17. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kemper J, Regier M, Stork A, Adam G and
Nolte-Ernsting C: Improved visualization of the urinary tract in
multi detector CT urography (MDCTU): Analysis of individual
acquisition delay and opacification using furosemide and low-dose
test images. J Comput Assist Tomogr. 30:751–757. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Palma L Dalla, Morra A and Grotto M:
CT-urography. Radiol Med. 110:170–178. 2005.(In Italian).
PubMed/NCBI
|
|
5
|
Yang Q, Zhang ZR, Liu BL, Wang SH and Sui
BB: Clinical evaluation of MSCTU in the diagnosis of upper urinary
tract obstruction. J Clin Radiol. 25:256–259. 2006.
|
|
6
|
Nawfel RD, Judy PF, Schleipman AR and
Silverman SG: Patient radiation dose at CT urography and
conventional urography. Radiology. 232:126–132. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
He YQ, Tang BH, Li LC, Wu RG, Huang DC,
Liang JX and Dong CL: Multi-slice spiral CT urography in the
diagnosis of urinary congenital abnormities. Chin J Radiol.
40:853–856. 2006.
|
|
8
|
Pan WL and Wang XT: Clinical evaluation of
Multi-slice spiral CT urography in the diagnosis of Pyelic and
Uretal disease. J Pract Radiol. 12:1655–1658. 2007.
|
|
9
|
Ma ZL, He LY, Yan YC, Lv XH, Liu SY and
Cao BX: Application of low-dose excretory CT urography. J China
Clin Med. 6:484–496. 2009.
|
|
10
|
EI-Ghar ME, Shokeir AA, EI-Diasty TA,
Refaie HF, Gad HM and EI-Dein AB: Contrast enhanced spiral
computerized tomography in patients with chronic obstructive
uropathy and normal serum creatinine: A single session for
anatomical and functional assessment. J Urol. 172:985–988. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kong WF, Liu RB, Xing Y, Wang N and Shang
L: Optimization of 64-detecter CT urography of normal upper urinary
tract: Effect of compression, prolongation of acquisition delay,
and oral water on images. J Med Imaging. 4:443–446. 2009.
|
|
12
|
Chow LC and Sommer FG: Multi detector CT
urography with abdominal compression and three-dimensional
reconstruction. AJR Am J Roentgenol. 177:849–855. 2001. View Article : Google Scholar : PubMed/NCBI
|