Introduction
With the increase in the success rate of liver
transplantation, giving rise to overall 1- and 5-year patient
survival rates of 90 and 75%, respectively (1), more and more patients are developing
late complications, such as renal dysfunction. Liver transplant
patients have the second highest incidence of chronic kidney
disease (CKD) post-surgery, after heart and lung transplant
patients (2). Some studies have
reported the incidence of CKD is 4.0–27.5% within 1 year after
liver transplantation (3). CKD is a
major contributor to post-transplant mortality. The relative risk
is 3.32 (2.96–3.71) (2). Therefore,
it is necessary to identify the causes of new-onset CKD after liver
transplantation. Some studies have reported that the causes are
complex and may include the preoperative glomerular filtration
rate, a history of hypertension, diabetes, the degree of
proteinuria, hemoglobin level and the duration of renal impairment
(4–6). Calcineurin inhibitor (CNI)-related
nephrotoxicity and chronic CNI nephrotoxicity are often observed in
liver transplant patients. One study indicated that low-dose
tacrolimus combined with everolimus 1 month after liver
transplantation could help preserve renal function at 1 year
post-liver transplantation (7).
However, few studies have been published regarding the
intraoperative risk factors for new-onset CKD. The goal of the
current study was to analyze the risk factors for new-onset CKD
occurring in patients receiving liver transplantation, and to
assess how the quality of life and long-term survival of these
patients may be improved.
Patients and methods
Patients
Forty patients with new-onset CKD were analyzed
retrospectively among 190 patients who underwent liver
transplantation between March 2001 and January 2015 at Beijing
Tsinghua Changgung Hospital (Beijing, China) or People's Hospital,
Peking University (Beijing, 100044); the remaining 150 patients did
not develop CKD, and 40 of them were selected randomly, using a
random number chart, to serve as the control group. The risk
factors for new-onset CKD occurrence were analyzed in patients who
received liver transplantation.
Methods
Demographic details, relevant preoperative and
postoperative laboratory tests, and average levels of CNIs (during
liver transplantation to the onset of CKD) were recorded. All
patients were followed up every 3 months after liver
transplantation, and urinalysis and kidney function were examined.
None of the patients required hemodialysis. Kidney function was
assessed by estimated glomerular filtration rate (eGFR), which was
calculated with the CKD-EPI equation according to the 2002 KDOQI
guidelines (3). CKD is defined as
renal impairment (kidney morphology, pathology, imaging, blood or
urine composition abnormalities) persisting for >3 months with
or without eGFR decrease, and/or eGFR<60 ml/min·1.73
m2 for >3 months with or without renal impairment.
New-onset CKD is defined as CKD that occurs after liver
transplantation. In patients with hepatitis B virus (HBV), HBsAg,
HBsAb, HBeAg, HBeAb, HBcAb and HBV-DNA were tested regularly.
Antiviral drugs included entecavir, adefovir dipivoxil and
tenofovir. In patients with hepatitis C virus (HCV), hepatitis C
antibody and HCV-RNA were examined regularly. The routine
treatments included interferon, lamivudine and ribavirin.
Prednisone, tacrolimus and mycophenolate mofetil were selected as
anti-rejection drugs after liver transplantation.
Statistical analysis
Statistical analyses were performed with SPSS
version 17.0, with P<0.05 considered to indicate a statistically
significant difference. Measurement data are expressed as the mean
± standard deviation (SD). Data were estimated by
Kolmogorov-Smirnov test for normal distribute test, unpaired
Student's t-test was used to compare between groups if the data
were estimated to be normally-distributed, and the Mann Whitney U
test was used if the data had a non-normal distribution. Count data
are expressed as a percentage, and a χ2 test was used to
compare between two groups. Logistic regression analysis was used
to analyze the contributing factors to new-onset CKD in patients
receiving liver transplantation.
Results
Comparison of preoperative clinical
data between the new-onset CKD group and the non-CKD group in
patients who received liver transplantation
The new-onset CKD patients were followed up for
63±45 months (4–156 months) vs. 42±21 months (6–84 months) in the
non-CKD group. The average age in the new-onset CKD group was
51.5±8.8 (28–70) years, compared with 47.4±11.2 (10–60) years in
the non-CKD group. Of the 40 patients in the new-onset CKD group,
35 (87.5%) were male.
Primary diseases of the liver included HBV-related
cirrhosis, alcoholic cirrhosis, liver cancer, HBV-related cirrhosis
with hepatocellular carcinoma, primary biliary cirrhosis,
cryptogenic cirrhosis and drug-induced hepatitis. There were no
statistically significant differences in primary liver diseases
between the two groups (P=0.054), as shown in Table I. Preoperative biochemical tests
included hemoglobin level, liver function, renal function, and
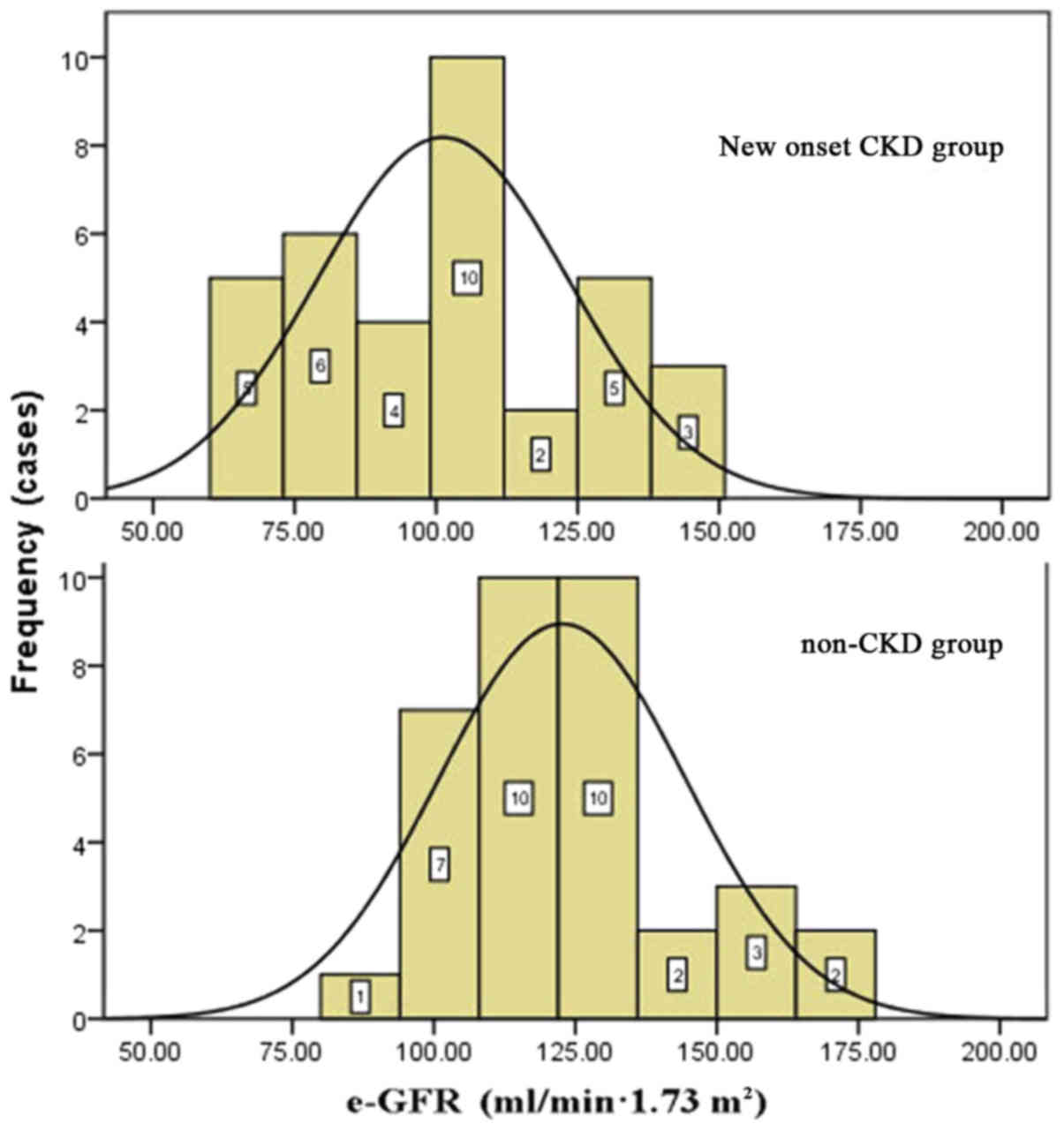
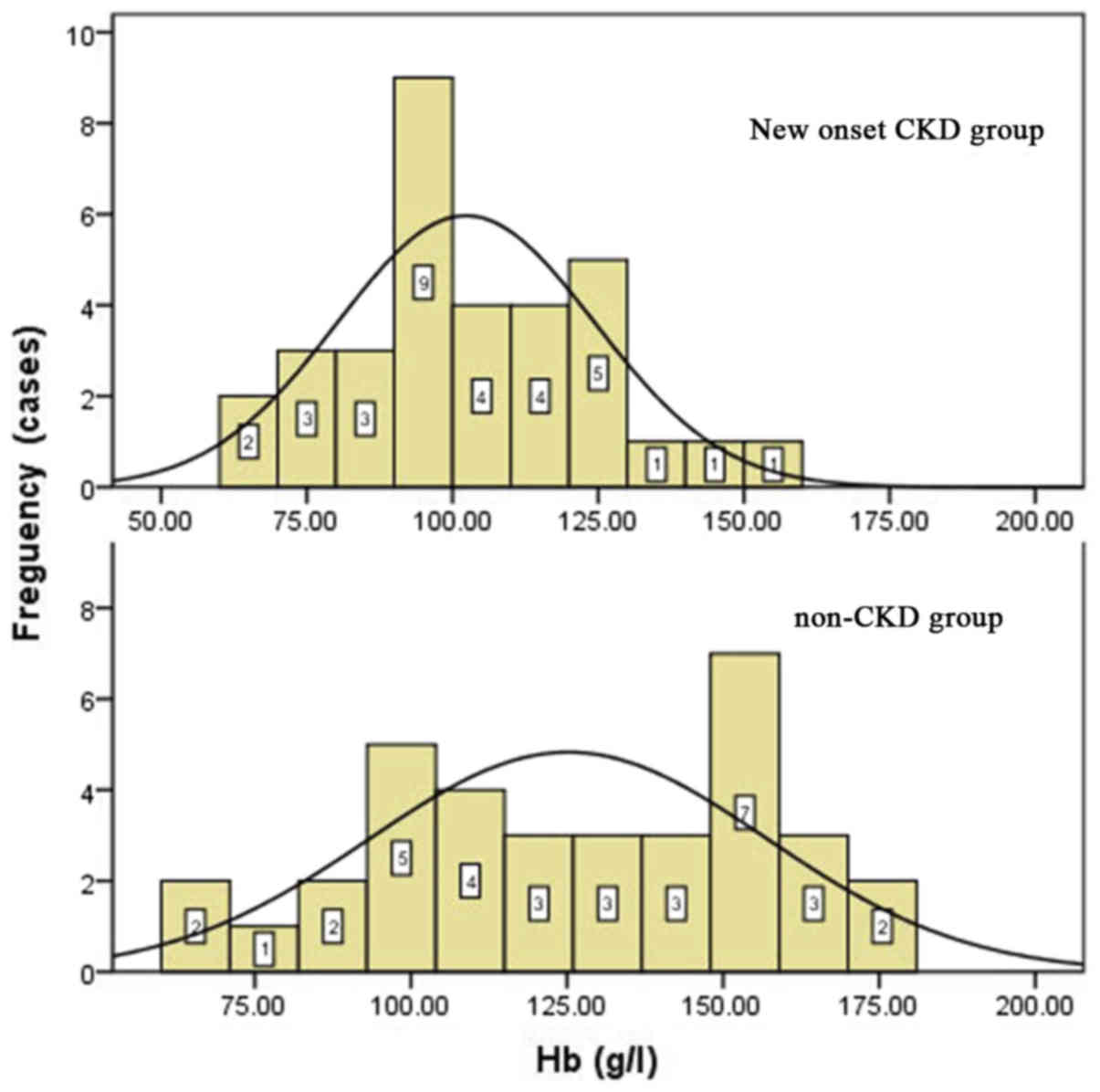
albumin and lipid levels. The preoperative eGFRs and hemoglobin
levels of the new-onset CKD group were significantly lower than
those in the control group (P<0.05): The mean hemoglobin level
was 102.6±21.7 g/l in the new-onset CKD group vs. 121.3±28.7 g/l in
non-CKD patients; and the mean eGFR was 105.6±37.1 ml/min·1.73
m2 in the new-onset CKD group vs. 131.6±44.1 ml/min·1.73
m2 in the non-CKD group (Table II; Figs.
1 and 2). None of the patients
in the new-onset CKD and non-CKD groups were diagnosed with CKD
prior to the liver transplant. Some of the patients in new-onset
CKD group seems have lower eGFR but the data were all in normal
range.
 | Table I.Primary liver diseases in new onset
CKD and non-CKD groups. |
Table I.
Primary liver diseases in new onset
CKD and non-CKD groups.
| Factors | New-onset CKD, n (%)
(n=40) | Non-CKD, n (n=40)
(%) | χ2 | P-value |
|---|
| Hepatitis B liver
cirrhosis | 16 (40.0) | 9 (22.5) |
|
|
| Hepatitis C liver
cirrhosis | 2 (5.0) | 2 (5.0) |
|
|
| Alcoholic
cirrhosis | 4 (10.0) | 3 (7.5) |
|
|
| Liver cancer | 3 (7.5) | 4 (10.0) | 16.70 | 0.06 |
| Hepatitis B liver
cirrhosis and liver cancer | 12 (30.0) | 20 (50.0) |
|
|
| Hepatitis C liver
cirrhosis and liver cancer | 0 (0) | 1 (2.5) |
|
|
| Alcoholic cirrhosis
and liver cancer | 1 (2.5) | 0 (0) |
|
|
| Hepatitis B and C
liver cirrhosis | 2 (5.0) | 1 (2.5) |
|
|
| Table II.Preoperative clinical data in
new-onset CKD and non-CKD groups. |
Table II.
Preoperative clinical data in
new-onset CKD and non-CKD groups.
| Factors | New-onset CKD
(n=40) | Non-CKD (n=40) | Z/t | P-value |
|---|
| HB (g/l) | 102.6±21.7 | 121.3±28.7 | −3.039 | 0.003a |
| Scr (umol/l) | 77.7±26.1 | 61.4±16.3 | 3.125 | 0.003a |
| eGFR (ml/min·1.73
m2) | 105.6±37.1 | 131.6±44.1 | −2.661 | 0.010a |
| BUN (mmol/l) | 7.9±6.6 | 4.6±1.4 | 1.674b | 0.094 |
| ALT (U/l) | 44.7±48.9 | 41.5±32.0 | 0.135b | 0.893 |
| AST (U/l) | 59.6±35.7 | 53.6±43.3 | 1.355b | 0.175 |
| TBIL (mmol/l) | 136.8±167.4 | 79.4±119.3 | 1.787b | 0.074 |
| TG (mmol/l) | 1.12±0.84 | 0.93±0.44 | 0.270b | 0.787 |
| LDL (mmol/l) | 1.63±1.58 | 1.79±0.71 | −0.503 | 0.619 |
| ALB (g/l) | 35.0±7.1 | 36.6±5.9 | −1.035 | 0.304 |
| Hypertension (%) | 3/40 (7.5) | 3/40 (7.5) |
| N/A |
| Diabeties (%) | 2/40 (5) | 2/40 (5) |
| N/A |
Surgical methods, intraoperative blood
loss, blood transfusion and anhepatic time
13/40 patients (40.6%) in the new-onset CKD group
and 22/40 (55%) in the non-CKD group received orthotropic liver
transplantation. 19/40 (59.4%) patients in the new-onset CKD group
and 18/40 (45%) in the non-CKD group received piggyback orthotropic
liver transplantation. There were no significant differences in
surgical procedures between the two groups (P=0.263).
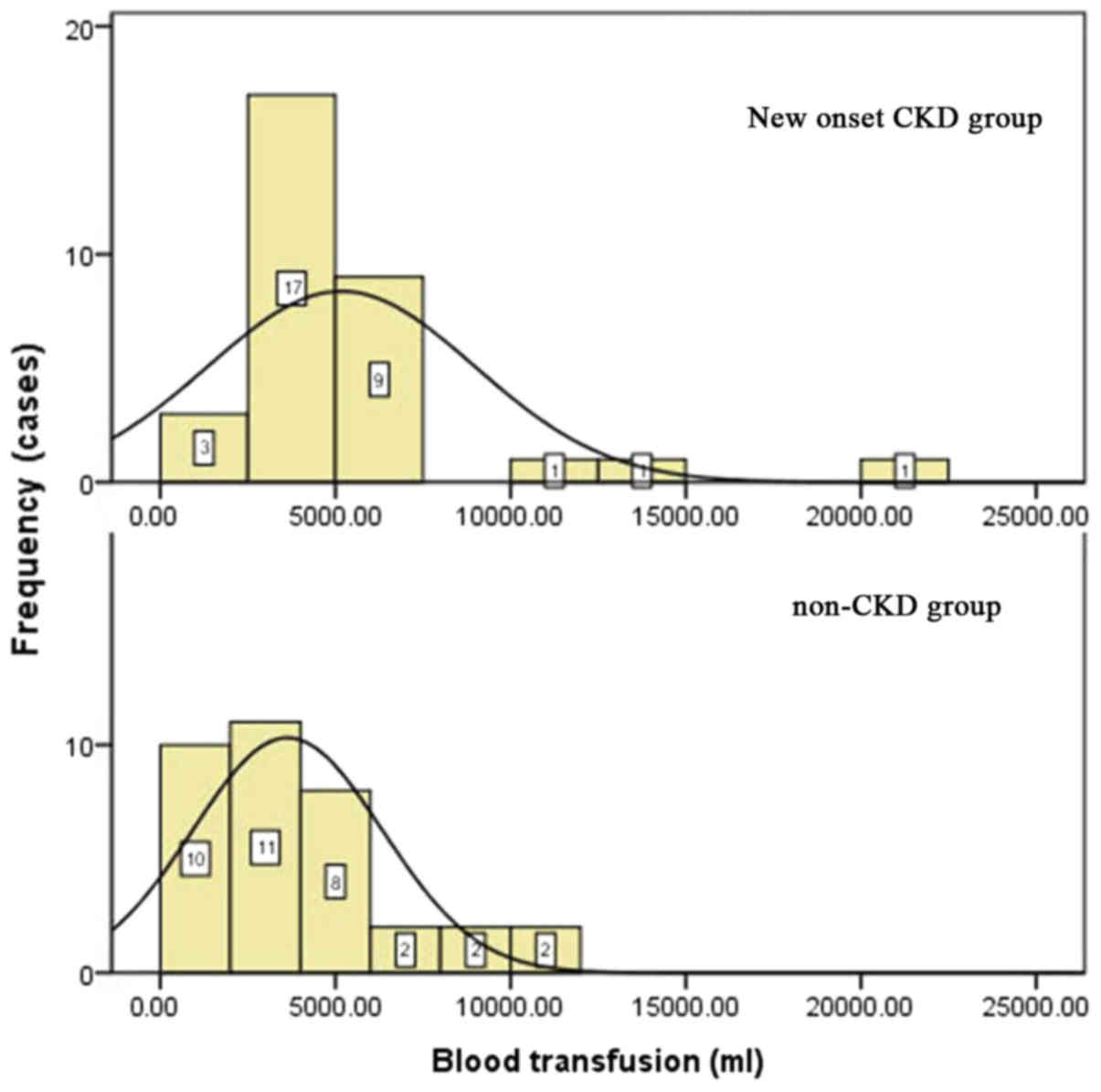
Blood loss in the new-onset CKD group was
5,697±7,749 ml vs. 2,268±2,185 ml in the control group (P=0.000),
and intraoperative blood transfusion in the new-onset CKD group was
5,181±3,780 ml vs. 3,754±2,902 ml in the control group (P=0.031).
Blood loss and intraoperative blood transfusion were different
between the two groups. The anhepatic time was 63.3±15.6 min in the
new-onset CKD group vs. 69.2±18.0 min in the non-CKD group, and
there was no significant difference between the two groups
(P=0.611). The blood transfusion volumes during surgery are shown
in Fig. 3.
Postoperative incidence of acute
kidney injury (AKI)
AKI after liver transplantation was defined as a
serum creatinine level elevated to ≥26.4 µmol/l, or increased to
≥50% of the baseline within one 48 h period during 1 month
following liver transplantation. 16/40 (40%) patients in the
new-onset CKD group developed postoperative AKI vs. no patients in
the non-CKD group, as shown in Table
III.
| Table III.Postoperative clinical data on
new-onset CKD and non-CKD patients who received liver
transplantation. |
Table III.
Postoperative clinical data on
new-onset CKD and non-CKD patients who received liver
transplantation.
| Factors | New-onset CKD | Non-CKD | t/χ2 | P-value |
|---|
| AKI (%) | 16 (40.0) | 0 (0.0) | 17.797 |
<0.001a |
| Tacrolimus
(ng/ml) | 14.0±4.5 | 11.0±2.8 | 3.334b | 0.001a |
| Postoperative
hypertension (%) | 14 (35.0) | 5 (12.5) | 4.234 | 0.040a |
| Postoperative
diabetes (%) | 13 (32.5) | 10 (25.0) | 1.491 | 0.222 |
Average levels of CNIs from liver
transplantation to the onset of CKD
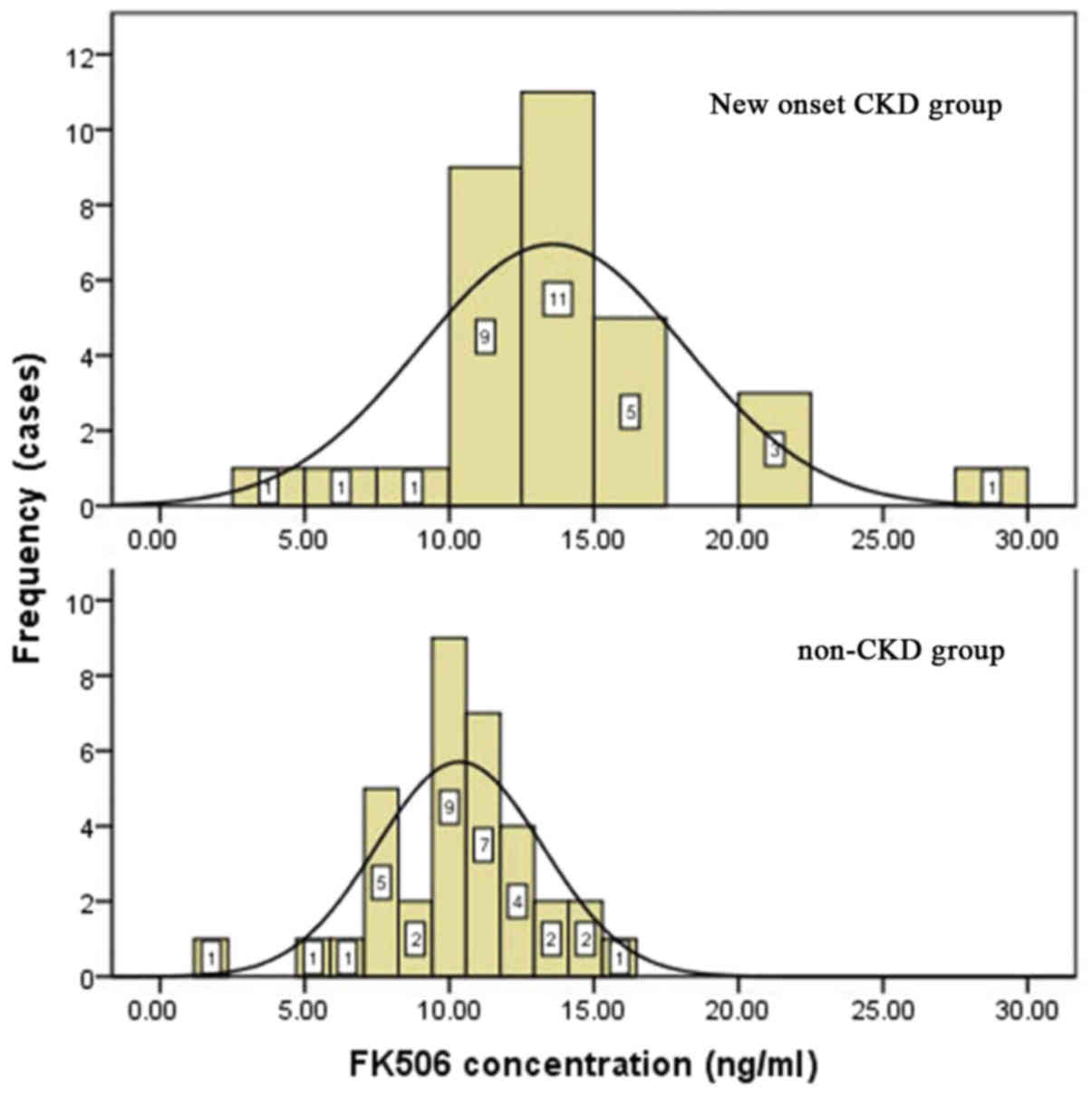
We calculated the average levels of CNIs from liver
transplantation to the onset of CKD. The mean concentration of
tacrolimus in the new-onset CKD group was 14.0±4.5 ng/ml vs.
11.0±2.8 ng/ml in the control group (P=0.001), as shown in Table III and Fig. 4.
Postoperative complications
Postoperative complications included postoperative
hypertension and diabetes. 14/40 (35.0%) patients developed
hypertension in the new-onset CKD group vs. 5/40 (12.5%) patients
in the control group (P=0.040); 13/40 (32.5%) patients developed
diabetes in the new-onset CKD group vs. 9/40 (25.0%) patients in
the control group (P=0.222), as shown in Table III. There was no recurrence of HBV
and HCV post-liver transplantation within the follow-up period,
which was 63±45 months in the new-onset CKD group and 42±21 months
in the control group.
Risk factors for new-onset CKD in
patients receiving liver transplantation, identified by logistic
regression analysis
Our data, analyzed by univariate analysis, indicated
that preoperative eGFR (P=0.010), preoperative hemoglobin
(P=0.003), intraoperative blood loss (P=0.000), intraoperative
blood transfusion (P=0.031), postoperative AKI (P=0.000),
postoperative average levels of CNIs (P=0.001) and postoperative
hypertension (P=0.040) were associated with new-onset CKD
occurrence in patients who had undergone liver transplantation, as
shown in Table IV. By multivariate
logistic regression analysis, we showed that preoperative eGFR,
hemoglobin level, average postoperative levels of CNIs and
postoperative hypertension were independent risk factors for
new-onset CKD occurrence (Table
V).
| Table IV.Risk factors for new onset CKD in
patients that received liver transplantation by univariate logistic
regression analysis. |
Table IV.
Risk factors for new onset CKD in
patients that received liver transplantation by univariate logistic
regression analysis.
| Factors | b | OR | 95% CI | P-value |
|---|
| eGFR | −0.017 | 0.983 | 0.970–0.997 | 0.010 |
| HGB | −0.029 | 0.972 | 0.952–0.992 | 0.003 |
| Intraoperative
blood loss | 0.000 | 1.000 | 1.000–1.001 | <0.001 |
| Intraoperative
blood transfusion | 0.027 | 1.003 | 1.000–1.010 | 0.031 |
| Acute kidney
injury | 0.115 | 1.010 | 1.001–1.021 | <0.001 |
| Calcineurin
concentration | 0.261 | 1.299 | 1.082–1.559 | 0.001 |
| Postoperative
hypertension | 1.212 | 3.360 | 1.063–10.620 | 0.040 |
| Table V.Risk factors for new onset CKD in
patients that received liver transplantation by multivariate
logistic regression analysis. |
Table V.
Risk factors for new onset CKD in
patients that received liver transplantation by multivariate
logistic regression analysis.
| Items | b | OR | 95% CI | P-value |
|---|
| eGFR | −0.020 | 0.980 | 0.962–0.999 | 0.041 |
| HGB | −0.029 | 0.972 | 0.946–0.998 | 0.034 |
| Calcineurin
concentration | 0.311 | 1.364 | 1.063–1.751 | 0.015 |
| Postoperative
Hypertension | 1.575 | 4.833 | 1.014–23.03 | 0.048 |
| Acute kidney
injury | 0.132 | 2.015 | 1.010–12.13 | 0.065 |
| Intraoperative
blood loss | 1.578 | 4.845 | 0.540–43.48 | 0.159 |
| Intraoperative
blood transfusion | 1.748 | 5.741 | 0.643–51.28 | 0.118 |
Renal pathology of patients with
new-onset CKD following liver transplantation
Out of 40 patients in the new-onset CKD group, only
7 patients gave consent for renal biopsy. 6/7 (85.7%) patients had
tubulointerstitial damage, which was associated with CNIs. Some
exhibited glomerular diseases, including IgA nephropathy,
HBV-associated nephropathy, membranous proliferative
glomerulonephritis, focal segmental glomerulosclerosis (FSGS) and
cryoglobulinemia-associated kidney damage, as shown in Table VI.
| Table VI.Clinical and pathological data of 7
new onset CKD patients that received liver transplantation. |
Table VI.
Clinical and pathological data of 7
new onset CKD patients that received liver transplantation.
| Item no. | Sex | Age | PLD | P-HB | P-eGFR | IBT | P-FK506 | P-AKI | P-HTN | P-RBT | RP |
|---|
| 1 | Male | 56 | HBC/LC | 93.3 | 100.3 | 3,800 |
4.0 | + | − | 3 months | FSGS/ATI |
| 2 | Male | 62 | HBC | 96.9 | 87.6 | 4,000 | 17.0 | − | + | 4 months | IgA/CFRI |
| 3 | Male | 50 | HBC | 121.2 | 146.2 | 6,500 | 15.9 | − | + | 2 years | STIN/CFRI |
| 4 | Male | 56 | HBC/LC | 112.6 | 137.2 | 2,800 | 17.4 | − | + | 3 years | IgA/CGKD/STIN |
| 5 | Male | 50 | HBC | 89.7 | 80.4 | 3,500 | 14.3 | − | + | 6 years | IgA/CGKD/STIN |
| 6 | Male | 28 | HCC | 114.3 | 171.6 | 3,800 |
9.1 | − | − | 7 years | MPGN/CFRI/STIN |
| 7 | Male | 43 | HBC | 94.8 | 88.1 | 3,600 |
6.0 | − | + | 9 years | MPGH |
Discussion
CKD significantly impacts long-term prognosis and is
a common complication in patients who have received a liver
transplant. Studies (3) have
reported that the incidence rates of CKD are 4.0–27.5% within 1
year and 30–50% within 10 years post-surgery (8). In this study, 190 patients who
underwent liver transplantation were followed up for 4–156 months;
40/190 (21.1%) patients developed new-onset CKD, which was
significantly higher than the general population.
There have been few studies regarding intraoperative
risk factors for new-onset CKD. In the present study, we analyzed
surgical methods (orthotopic liver transplantation or piggyback
orthotopic liver transplantation), anhepatic time, intraoperative
blood loss and blood transfusion, and the results indicates that
the volume of intraoperative blood loss and blood transfusion was a
risk factor for new-onset CKD occurrence. The kidneys are sensitive
to ischemia, especially in patients with impaired renal function,
who are less tolerant of intraoperative hemodynamic instability.
With an increase in intraoperative blood loss and blood transfusion
leading to a decrease in renal perfusion pressure and glomerular
filtration rate, renal ischemia-reperfusion injury is aggravated.
That eventually leads to inflammatory responses, such as leukocyte
infiltration, interstitial edema and a decrease in microvascular
blood flow, which conversely exacerbates ischemic reperfusion
injury (9).
Previous data also indicated that the dose-dependent
nephrotoxicity of CNIs also plays an important role in new-onset
CKD (10). Morard et al
(11) reported that FK506
concentrations of ≥10 and ≥8 ng/ml at 1 and 5 years post-liver
transplantation, respectively, were independent risk factors for
the occurrence of CKD. In this study, we analyzed the average
plasma FK506 concentration between the time of liver
transplantation and the onset of CKD. Our results showed that the
average plasma FK506 concentration was 14.0±4.5 ng/ml in the
new-onset CKD group, in contrast to 11.0±2.8 ng/ml in the control
group (P=0.001). Our multivariate analysis indicated that the
average plasma concentration of FK506 from the time of liver
transplantation to the onset of CKD was an independent risk factor
for new-onset CKD in patients who had received liver
transplantation. Calcineurin stimulates the secretion of endothelin
by vascular endothelial cells, the release of angiotensin II and
the overexpression of transforming growth factor-β. This process is
accompanied by weakening of matrix degradation enzyme activity,
which causes excessive contraction of glomerular arterioles,
hyalinosis, chronic thromboembolism and excessive synthesis of the
extracellular matrix. Finally, it leads to tubular atrophy,
interstitial fibrosis, and a decrease in renal blood flow and
glomerular filtration rate. The severity of nephrotoxicity is
mainly due to the long-term use of calcineurin drugs. In addition,
the side effects of CNIs, such as hypertension, diabetes,
hyperlipidemia and hyperuricemia, also increase renal damage.
Our study also showed that preoperative low
glomerular filtration rate and low hemoglobin are risk factors for
new-onset CKD in patients who have received a liver transplant.
These patients are more prone to ischemia-reperfusion injury during
and after surgery because of the trauma and circulation
instability.
Several studies have analyzed the postoperative risk
factors for CKD in patients who have received liver
transplantation. AKI was associated with the occurrence of CKD
(12–14). The occurrence of CKD in liver
transplant patients who had AKI was several times higher than in
those patients who did not have concomitant AKI (15). Tinti et al (16) retrospectively studied 24 patients who
had received liver transplantation, 9 of which developed
postoperative AKI. The incidence rates of CKD were 44.4 and 6.7% in
the AKI group and the non-AKI group, respectively. Our univariate
analysis showed that postoperative AKI was a risk factor for
new-onset CKD occurrence in patients who had received liver
transplantation. The rate of AKI was 100% in the new-onset CKD
group. In contrast, it was only 40.7% in the non-CKD group
(P=0.000).
In the general population, elevated blood pressure
may cause various injuries, including glomerular endothelial and
epithelial cell injuries, and an increase in the activity of
renin-angiotensin-aldosterone system. This eventually leads to
damage to kidney function and proteinuria. Hypertension is commonly
seen among patients with chronic glomerulonephritis, especially in
FSGS. Some studies have reported that postoperative hypertension
and diabetes are risk factors for CKD among patients who have
received liver transplantation. Shao et al (10) retrospectively analyzed 772 liver
transplant patients, and showed that post-operative hypertension
(OR=2.230, 95% CI: 1.059–4.696, P<0.05) was a risk factor for
CKD, as determined by logistic regression. Our study consistently
showed that postoperative hypertension was an independent risk
factor for new-onset CKD occurrence. However, there was no
statistical difference in the postoperative occurrence of diabetes
between the new-onset CKD group and the non-CKD group, according to
our data. This discrepancy may possibly be attributed to the short
history of diabetes. However, our results will be further confirmed
by future studies with larger number of patients.
In the past, very few CKD patients who received
liver transplantation underwent renal biopsy. Several studies
showed that the renal pathology in CKD patients was complex and
diverse, including CNI-induced renal damage, hypertensive renal
damage, diabetic nephropathy, HBV-associated membranous
nephropathy, IgA nephropathy, thrombotic microangiopathy, FSGS,
membranous proliferative glomerulonephritis,
cryoglobulinemia-associated renal damage, acute tubular necrosis,
acute interstitial nephritis, amyloidosis, anti-glomerular basement
membrane nephropathy, crescent glomerulonephritis and hydroxyethyl
starch-associated tubule and interstitial lesions (11,17,18). In
our study, 7 out of the 40 new-onset CKD patients underwent renal
biopsy, among which 6 patients had acute or chronic tubular and
interstitial damage. On the contrary, glomerular diseases included
IgA nephropathy, membranous proliferative glomerulonephritis
associated with HBV, membranous proliferative glomerulonephritis,
FSGS and cryoglobulinemia associated with renal damage.
In conclusion, CKD is a common complication in
patients who have received liver transplantation, and can affect
the long-term prognosis of these patients. The preoperative
glomerular filtration rate, hemoglobin level, average level of CNIs
and postoperative hypertension are major risk factors for new-onset
CKD following liver transplantation. Considering the severe
shortage of liver donors, it is important to prevent new-onset CKD
and improve survival by more carefully monitoring renal disease and
function. Anemia correction, careful monitoring of CNI
concentration and the prevention of AKI are of great significance
for liver transplant patients with regard to avoiding new-onset
CKD. We will examine more kidney biopsy samples among new-onset CKD
patients post-liver transplant in order to better analyze the
contribution of various risk factors to renal pathology in a future
study. Finally, our study provided evidence to support the
development of a better follow-up system to improve survival and
quality of life for liver transplant patients.
Our sample size was limited, some of the conclusions
were failed to be further discussed, such as the number of patients
in the new-onset CKD groups were not sufficient to assess the
severity of CKD. We will expand the sample size for future
studies.
References
|
1
|
Kim WR, Smith JM, Skeans MA, Schladt DP,
Schnitzler MA, Edwards EB, Harper AM, Wainright JL, Snyder JJ,
Israni AK and Kasiske BL: OPTN/SRTR 2012 annual data report: Liver.
Am J Transplant. 14 Suppl 1:S69–S96. 2014. View Article : Google Scholar
|
|
2
|
Sharma P and Bari K: Chronic kidney
disease and related long-term complications following liver
transplantation. Adv Chronic Kidney Dis. 225:404–411. 2015.
View Article : Google Scholar
|
|
3
|
Weber ML, Ibrahim HN and Lake JR: Renal
dysfunction in liver transplant recipients: Evaluation of the
critical issues. Liver Transpl. 18:1290–1301. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ruebner R, Goldberg D, Abt PL, Bahirwani
R, Levine M, Sawinski D, Bloom RD and Reese PP: Risk of end-stage
renal disease among liver transplant recipients with pretransplant
renal dysfunction. Am J Transplant. 12:2958–2965. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Israni AK, Xiong H, Liu J, Salkowski N,
Trotter JF, Snyder JJ and Kasiske BL: Predicting end-stage renal
disease after liver transplant. Am J Transplant. 13:1782–1792.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sharma P, Goodrich NP, Schaubel DE,
Guidinger MK and Merion RM: Patient-specific prediction of ESRD
after liver transplantation. J Am Soc Nephrol. 24:2045–2052. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fischer L, Klempnauer J, Beckebaum S,
Metselaar HJ, Neuhaus P, Schemmer P, Settmacher U, Heyne N, Clavien
PA, Muehlbacher F, et al: A randomized, controlled study to assess
the conversion from calcineurin-inhibitors to everolimus after
liver transplantation-PROTECT. Am J Transplant. 12:1855–1865. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fabrizi F, Dixit V, Martin P and Messa P:
Chronic kidney disease after liver transplantation: Recent
evidence. Int J Artif Organs. 33:803–811. 2010.PubMed/NCBI
|
|
9
|
Li B, Chen B, Zhang G, Wang K, Zhou L and
Hu S: Cell apoptosis and Fas gene expression in liver and renal
tissues after ischemia-reperfusion injury in liver transplantation.
Transplant Proc. 42:pp. 1550–1556. 2010; View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shao ZY, Yan LN, Wang WT, Li B, Wen TF,
Yang JY, Xu MQ, Zhao JC and Wei YG: Prophylaxis of chronic kidney
disease after liver transplantation - experience from west China.
World J Gastroenterol. 18:991–998. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Morard I, Mentha G, Spahr L, Majno P,
Hadengue A, Huber O, Morel P and Giostra E: Long-term renal
function after liver transplantation is related to calcineurin
inhibitors blood levels. Clin Transplant. 20:96–101. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kubal C, Cockwell P, Gunson B, Jesky M,
Hanvesakul R, Dronavalli V, Bonser RS and Neil D: Chronic kidney
disease after nonrenal solid organ transplantation: A histological
assessment and utility of chronic allograft damage index scoring.
Transplantation. 93:406–411. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cantarovich M, Tchervenkov J, Paraskevas
S, Ghali P, Wong P, Deschênes M, Chaudhury P, Hassanain M,
Vrochides D, Metrakos P and Barkun J: Early changes in kidney
function predict long-term chronic kidney disease and mortality in
patients after liver transplantation. Transplantation.
92:1358–1363. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lee JP, Heo NJ, Joo KW, Yi NJ, Suh KS,
Moon KC, Kim SG and Kim YS: Risk factors for consequent kidney
impairment and differential impact of liver transplantation on
renal function. Nephrol Dial Transplant. 25:2772–2785. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Velidedeoglu E, Bloom RD, Crawford MD,
Desai NM, Campos L, Abt PL, Markmann JW, Mange KC, Olthoff KM,
Shaked A and Markmann JF: Early kidney dysfunction post liver
transplantation predicts late chronic kidney disease.
Transplantation. 77:553–556. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tinti F, Umbro I, Mecule A, Rossi M, Merli
M, Nofroni I, Corradini SG, Poli L, Pugliese F, Ruberto F, et al:
RIFLE criteria and hepatic function in the assessment of acute
renal failure in liver transplantation. Transplant Proc.
42:1233–1236. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kamar N, Guilbeau-Frugier C, Servais A,
Tack I, Thervet E, Cointault O, Esposito L, Guitard J, Lavayssière
L, Muscari F, et al: Kidney histology and function in liver
transplant patients. Nephrol Dial Transplant. 26:2355–2361. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kim JY, Akalin E, Dikman S, Gagliardi R,
Schiano T, Bromberg J, Murphy B and de Boccardo G: The variable
pathology of kidney disease after liver transplantation.
Transplantation. 89:215–221. 2010. View Article : Google Scholar : PubMed/NCBI
|