Introduction
Multiple causes lead to impaired glomerular
filtration function, so that a large amount of albumin in plasma
leak into the urine of patients, becoming a disease of albuminuria,
which is called nephrotic syndrome, one of the more common diseases
in the pediatric urinary system (1).
It is clinically believed that the pathogenesis of the disease is
not yet very clear. Most of the views believe that it is related to
the immune system dysfunction (2).
Nephrotic syndrome is often accompanied by various infectious
diseases due to immune dysfunction. A variety of cytokines related
to immune regulation play a role in promoting the glomerular
dysfunction in nephrotic syndrome (3). The overreaction of inflammatory system
and overexpression of serum level of high-sensitivity C-reactive
protein (hs-CRP) in children with nephrotic syndrome accelerates
the inflammatory reaction process and further aggravates vascular
endothelial injury (4). The load
remodeling of renal blood vessels, the increased glomerular
filtration rate and the increased urinary protein in patients
aggravate the severity of nephrotic syndrome (5). In addition, the main treatment of
nephrotic syndrome is to use hormones, but hormones often lead to
varying degrees of obesity in children (6). In the human body, there is a
polypeptide hormone leptin synthesized and secreted by fat cells,
the main role of which is to regulate the body's lipid metabolism
(7). It is closely related to the
body weight of children and the severity of the disease, and it
also affects the 24 h urinary protein quantitative in children
(8). However, at present, the
judgment of the patient's condition is not very clear through the
detection of plasma leptin and serum inflammatory factors hs-CRP
and interleukin-18 (IL-18) in children with nephrotic syndrome, and
more evidence-based bases are needed to support it.
Patients and methods
General data
A total of 28 children diagnosed with nephrotic
syndrome in People's Hospital of Rizhao (Rizhao, China) from
November 2015 to October 2016 were selected as the treatment group,
another 25 healthy children were selected as the control group,
including 30 males and 23 females aged 5–13 years old with an
average age of 8.56±2.72 years old. By collecting the patients'
age, sex, serum albumin and other basic data, all patients included
in the treatment group were diagnosed with nephrotic syndrome
according to the About Clinical Classification, Diagnosis and
Treatment Recommendation of Glomerular Diseases in Children
designated by Chinese Medical Association of Pediatrics in 2000.
Exclusion criteria: child patients aged over 14 years old; child
patients with first-onset nephrotic syndrome; patients with no
history of recurrence and without treatment with glucocorticoids or
drugs related to mediation of immunity prior to treatment; tumor
patients; patients with severe circulatory system, metabolic
system, urinary system, or immune system diseases; patients who
exited midway or had incomplete clinical data. This study was
approved by the Ethics Committee of People's Hospital of Rizhao.
Signed written informed consents were obtained from the
parents/guardians of all patients before the study.
Methods
Children with nephrotic syndrome received routine
treatment after admission, of which the most important was the
treatment with hormones and immunosuppressive agents with the whole
course of treatment of 8–10 weeks, while children in the healthy
control group did not received any treatment. Detection of the
plasma leptin levels, inflammatory factors and renal function: 20
ml of morning fasting peripheral venous blood was collected from
patients in the treatment group on the day before treatment. The
leptin level was measured by radioimmunoassay, the levels of hs-CRP
and IL-18 were measured by immunoturbidimetry, the levels of blood
urea nitrogen (BUN) and serum creatinine (SCr) were measured by
enzyme-linked immunosorbent assay (ELISA). Meanwhile, levels of
serum leptin, hs-CRP, IL-18, BUN and SCr of patients in the control
group were also determined by the same method at the same time.
Moreover, the levels of serum leptin, hs-CRP, IL-18, BUN and SCr of
patients in the treatment group were also determined by the same
method at 2 weeks, 3 months and 6 months after treatment. The kits
were supplied by the Bender (Vienna, Austria).
Detection of urinary protein: 24 h urine specimens
of patients in the treatment group were collected one day before
the treatment, and the 24 h urinary protein quantitative was
calculated. Meanwhile, the 24 h urinary protein quantitative of
patients in the control group was detected by the same method at
the same time. Moreover, the 24 h urinary protein of patients in
the treatment group was quantified by the same method at 2 weeks, 3
months and 6 months after treatment.
Statistical analysis
The data were processed by SPSS 19.0 software (IBM,
Armonk, NY, USA), collection data were expressed by mean ± SD,
enumeration data were compared by χ2 test, correlation
analysis was used for two factors, and P<0.05 suggested that the
difference was statistically significant.
Results
Comparisons of general conditions
between the treatment group and the control group before
treatment
There were no statistically significant differences
in the age, sex, body mass index (BMI) and serum albumin between
the treatment group and the control group before treatment
(P>0.05), and the data were comparable (Table I).
 | Table I.Comparisons of general data between
the treatment group and the control group before treatment. |
Table I.
Comparisons of general data between
the treatment group and the control group before treatment.
| General data | Treatment group
(n=28) | Control group
(n=25) | P-value |
|---|
| Age (years) | 8.38±1.96 | 8.72±2.05 | 0.871 |
| Sex
(male/female) | 16/12 | 14/11 | 0.905 |
| BMI
(kg/m2) | 22.43±5.71 | 20.78±4.93 | 0.059 |
| Serum albumin
(g/l) | 17.72±2.75 | 17.82±3.91 | 0.051 |
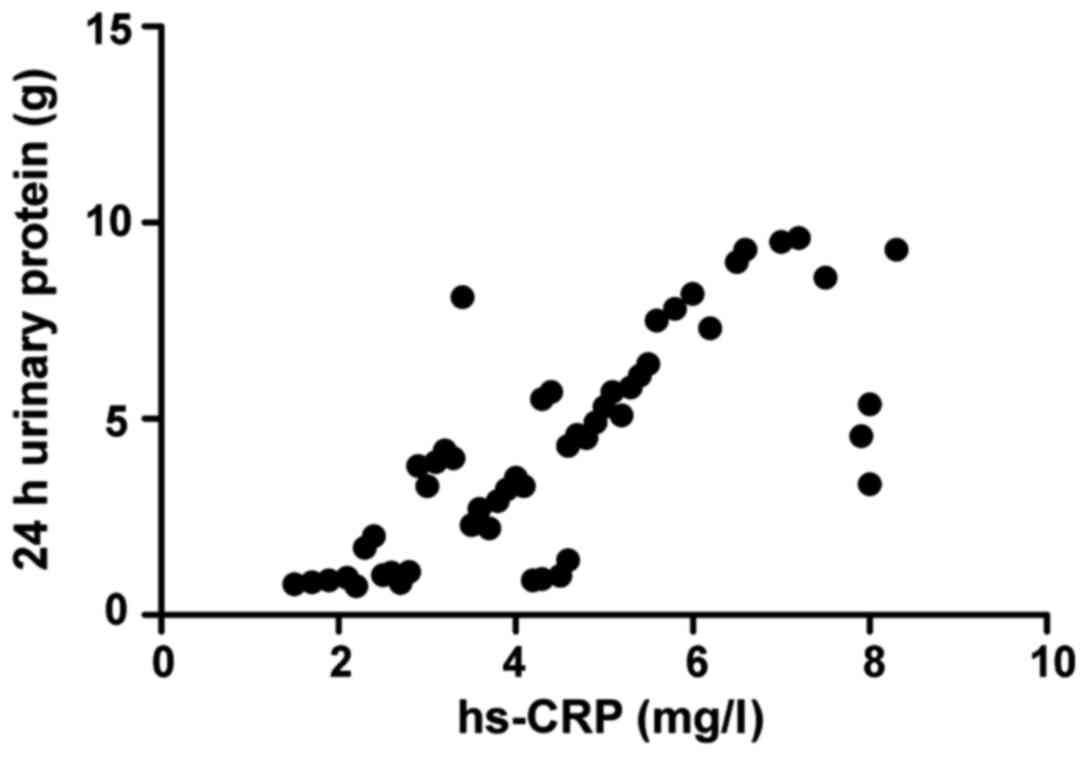
Correlation analysis of inflammatory
factors and 24 h urinary protein in treatment group before
treatment
The serum hs-CRP factor level in the treatment group
before treatment was positively correlated with the 24 h urinary
protein level (r=0.408, P=0.005), with statistical significance
(Fig. 1).
Comparison of peripheral plasma leptin
levels between the treatment group and the control group before
treatment, and at 2 weeks, 3 months and 6 months after
treatment
The plasma leptin level in the treatment group was
significantly higher before treatment than that in the control
group, significantly lower at 2 weeks after treatment than that
before treatment, significantly lower at 3 months after treatment
than that at 2 weeks after treatment, and significantly lower at 6
months after treatment than that at 2 weeks after treatment and
before treatment, and the differences were statistically
significant (P<0.05); there was no significant difference in
plasma leptin level between the treatment group and the healthy
control group at 6 months after treatment (P>0.05) (Table II).
| Table II.Comparison of leptin levels between
the treatment group and the control group before treatment, at 2
weeks, 3 months and 6 months after treatment. |
Table II.
Comparison of leptin levels between
the treatment group and the control group before treatment, at 2
weeks, 3 months and 6 months after treatment.
| Group | Leptin (µg/l) |
|---|
| Control group
(n=25) | 9.26±2.89 |
| Treatment group
(n=28) |
|
| Before
treatment | 29.78±5.95 |
| After
treatment |
|
|
2 weeks | 20.81±3.41 |
|
3 months | 13.17±2.57 |
|
6 months | 10.08±1.26 |
Comparisons of the levels of hs-CRP
and IL-18 in peripheral blood serum between the treatment group and
the control group before treatment, and at 2 weeks, 3 months and 6
months after treatment
The levels of peripheral serum inflammatory factors
hs-CRP and IL-18 in the treatment group were significantly higher
before treatment than those in the control group, significantly
lower at 2 weeks after treatment than those before treatment,
significantly lower at 3 months after treatment than those at 2
weeks after treatment, and significantly lower at 6 months after
treatment than those at 2 weeks after treatment and before
treatment, and the differences were statistically significant
(P<0.05); the levels of inflammatory factors in the treatment
group at 6 months after treatment were not significantly different
from those in the healthy control group (P>0.05) (Table III).
| Table III.Comparison of the levels of hs-CRP and
IL-18 between the treatment group and the control group before
treatment, at 2 weeks, 3 months and 6 months after treatment. |
Table III.
Comparison of the levels of hs-CRP and
IL-18 between the treatment group and the control group before
treatment, at 2 weeks, 3 months and 6 months after treatment.
| Group | hs-CRP (mg/l) | IL-18 (pg/ml) |
|---|
| Control group
(n=25) | 2.05±0.94 | 39.16±0.17 |
| Treatment group
(n=28) |
|
|
| Before
treatment | 5.36±1.54 | 59.63±15.02 |
| After
treatment |
|
|
|
2 weeks | 4.07±1.36 | 52.39±11.22 |
|
3 months | 2.95±0.98 | 43.61±4.16 |
|
6 months | 2.11±0.53 | 39.15±2.79 |
Comparisons of the levels of 24 h
urinary protein, serum BUN and SCr between the treatment group and
the control group before treatment, and at 2 weeks, 3 months and 6
months after treatment
The levels of 24 h urinary protein, BUN and SCr in
the treatment group were significantly higher before treatment than
those in the control group, significantly lower at 2 weeks after
treatment than those before treatment, significantly lower at 3
months after treatment than those at 2 weeks after treatment, and
significantly lower at 6 months after treatment than those at 2
weeks after treatment and before treatment, and the differences
were statistically significant (P<0.05); there were no
significant differences in 24 h urinary protein, BUN and SCr levels
between the treatment group and the healthy control group at 6
months after treatment (P>0.05) (Table IV).
| Table IV.Comparison of 24 h urinary protein,
BUN and SCr between the treatment group and the control group
before treatment, at 2 weeks, 3 months and 6 months after
treatment. |
Table IV.
Comparison of 24 h urinary protein,
BUN and SCr between the treatment group and the control group
before treatment, at 2 weeks, 3 months and 6 months after
treatment.
| Group | 24 h urinary protein
(g) | BUN (mmol/l) | SCr (µmmol/l) |
|---|
| Control group
(n=25) | 1.01±0.23 | 4.32±0.88 | 63.58±14.4 |
| Treatment group
(n=28) |
|
|
|
| Before
treatment | 6.32±2.57 | 7.09±4.14 | 115.76±22.56 |
| After
treatment |
|
|
|
|
2 weeks | 5.08±1.98 | 6.01±3.82 | 90.31±18.25 |
|
3 months | 3.02±1.14 | 4.93±3.61 | 79.54±9.57 |
|
6 months | 1.31±0.98 | 4.34±1.27 | 64.37±10.63 |
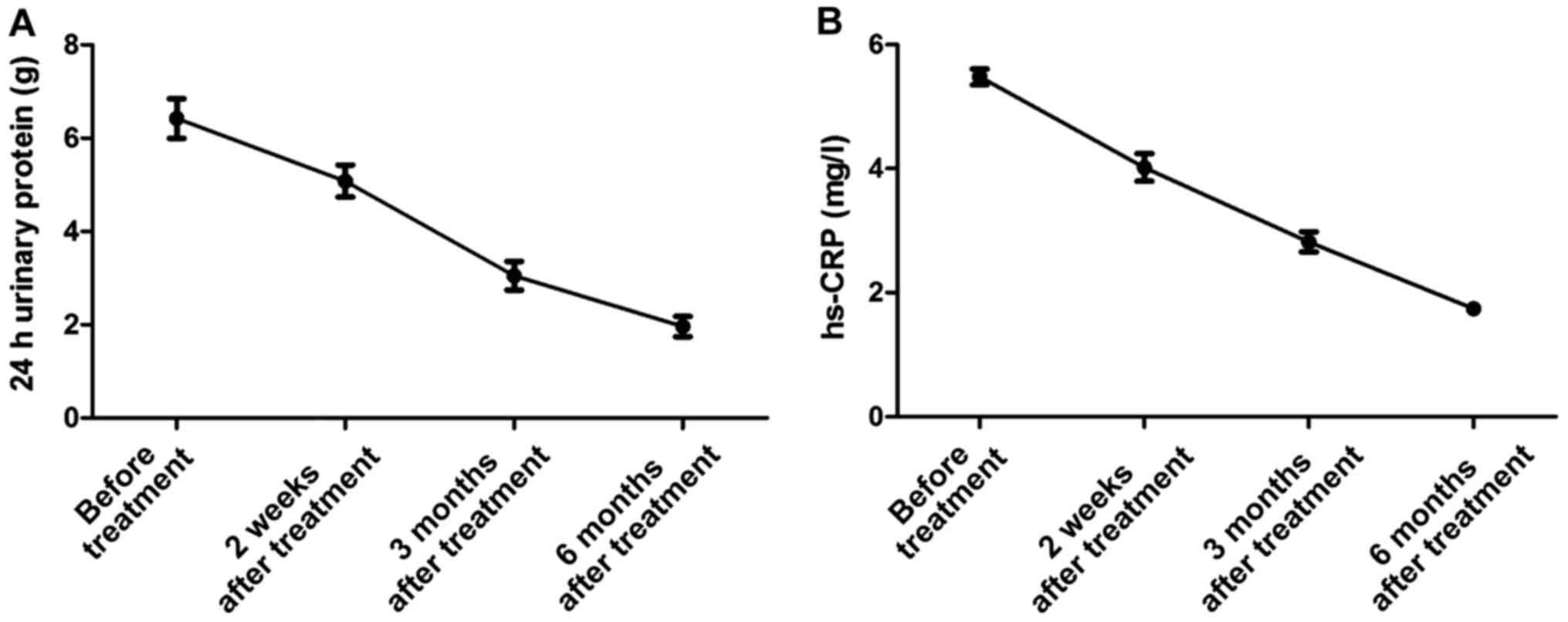
The trends of serum hs-CRP and 24 h
urinary protein in the treatment group before treatment, and at 2
weeks, 3 months and 6 months after treatment
The serum inflammatory factors levels and 24 h
urinary protein in the treatment group before treatment, and at 2
weeks, 3 months and 6 months after treatment showed decreasing
trends (Fig. 2).
Discussion
Glomerular dysfunction caused by different reasons
may lead to nephrotic syndrome. Because the pathological type of
the disease is numerous, and the mechanism is not very clear
(9), it often brings difficulties to
clinicians in the treatment. The most common clinical manifestation
is low serum protein level due to leakage of urinary protein,
generally below 3.5 grams (10). If
the patient is in a low-protein state for a long time, the colloid
osmotic pressure in the human body will decrease, and the patient
will then have symptoms such as edema (11). In pediatric urinary system, nephrotic
syndrome is one of the common diseases, whose main treatment is to
use hormones and immunosuppressive agents (12). Numerous research data have shown that
the plasma leptin level is closely related to the severity of
impaired renal function, and the more serious the renal function
damage is, the higher the plasma leptin level is (13). This study found that the plasma
leptin level in children with nephrotic syndrome was significantly
higher than that in the healthy control group, and significantly
lower after treatment than that before treatment. The leptin level
after 6 months of treatment was not significantly different from
that in the healthy control group, which was consistent with
numerous research data. The main reason for the increased leptin in
nephrotic syndrome is the decreased glomerular filtration rate
(14). Second, impaired immune
function in children, deficiency of complement factors, and low
serum protein malnutrition and many other factors will lead to an
increase in plasma leptin level in children with nephrotic syndrome
(15).
On the other hand, in the immune system, IL-18 plays
an important role in maintaining the balance of the immune system
(16). Mononuclear macrophages, B
cells, killer cells and other factors in the human body can
synthesize and secrete IL-18, and IL-18, in turn, can promote the
macrophage and other response. These immune cells will cause damage
to the immune response of the kidney to some extent (17). At the same time, the overreaction of
inflammatory system and overexpression of hs-CRP in children with
nephrotic syndrome lead to the deformation of vascular endothelial
tissue cells and an increase of resistance (18). hs-CRP can also lead to the production
and secretion of angiotensin receptor and vascular
endothelium-secreting plasminogen activator inhibitor, resulting in
different degrees of hardening of arteries (19), deposited on vascular endothelial
cells in the form of immune complexes, causing the release of
another inflammatory factor in the process of attacking vascular
endothelium, and eventually leading to renal vascular damage,
glomerular filtration dysfunction, impaired renal function and 24 h
urinary protein quantitative increase. This study concluded that
the levels of inflammatory factors in children with nephrotic
syndrome before treatment were significantly higher than those in
children in the healthy control group, and significantly lower
after treatment than those before treatment. From the correlation
analysis, and the change trends of inflammatory factors and 24 h
urinary protein before and after treatment, it can be seen that the
higher levels of inflammatory factors in children with nephrotic
syndrome, the more serious damage to the kidneys.
In conclusion, the detection of plasma leptin, serum
inflammatory factors hs-CRP and IL-18 levels in children with
nephrotic syndrome is crucial for the judgment of the severity of
disease, and it is of important reference value in improving the
treatment and prognosis of children with nephrotic syndrome.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
JZ designed the study and prepared the manuscript.
FS collected the data. WX analysed the data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
People's Hospital of Rizhao (Rizhao, China). Signed written
informed consents were obtained from the parents/guardians of all
patients before the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Landt M, Ludbrook PA and Billadello JJ:
Role of protein binding in renal elimination of leptin. Clin
Endocrinol (Oxf). 59:44–48. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yao H, Cai ZY and Sheng ZX: NAC attenuates
adriamycin-induced nephrotic syndrome in rats through regulating
TLR4 signaling pathway. Eur Rev Med Pharmacol Sci. 21:1938–1943.
2017.PubMed/NCBI
|
|
3
|
Daschner M, Tönshoff B, Blum WF, Englaro
P, Wingen AM, Schaefer F, Wühl E, Rascher W and Mehls O: European
Study Group for Nutritional Treatment of Chronic Renal Failure in
Childhood: Inappropriate elevation of serum leptin levels in
children with chronic renal failure. J Am Soc Nephrol. 9:1074–1079.
1998.PubMed/NCBI
|
|
4
|
Yoshida T, Momotani N, Hayashi M, Monkawa
T, Ito K and Saruta T: Serum leptin concentrations in patients with
thyroid disorders. Clin Endocrinol (Oxf). 48:299–302. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bakr A, Shokeir M, El-Chenawi F,
El-Husseni F, Abdel-Rahman A and El-Ashry R: Tumor necrosis
factor-alpha production from mononuclear cells in nephrotic
syndrome. Pediatr Nephrol. 18:516–520. 2003.PubMed/NCBI
|
|
6
|
Florian M, Florianova L, Hussain S and
Magder S: Interaction of estrogen and tumor necrosis factor alpha
in endothelial cell migration and early stage of angiogenesis.
Endothelium. 15:265–275. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Matsumoto K and Kanmatsuse K: Elevated
interleukin-18 levels in the urine of nephrotic patients. Nephron.
88:334–339. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Drewe E, McDermott EM and Powell RJ:
Treatment of the nephrotic syndrome with etanercept in patients
with the tumor necrosis factor receptor-associated periodic
syndrome. N Engl J Med. 343:1044–1045. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Reinehr T, Kratzsch J, Kiess W and Andler
W: Circulating soluble leptin receptor, leptin, and insulin
resistance before and after weight loss in obese children. Int J
Obes. 29:1230–1235. 2005. View Article : Google Scholar
|
|
10
|
Lányi E, Csernus K, Erhardt E, Tóth K,
Urbán B, Lénárd L and Molnár D: Plasma levels of acylated ghrelin
during an oral glucose tolerance test in obese children. J
Endocrinol Invest. 30:133–137. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Schroth M, Kratzsch J, Gröschl M, Rauh M,
Rascher W and Dötsch J: Increased soluble leptin receptor in
children with nephrotic syndrome. J Clin Endocrinol Metab.
88:5497–5501. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schroth M, Gröschl M, Dörr HG, Blum WF,
Rascher W and Dötsch J: Renal loss of leptin in patients with
nephrotic syndrome. Eur J Endocrinol. 145:463–468. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Garcia GE, Xia Y, Ku G, Johnson RJ, Wilson
CB and Feng L: IL-18 translational inhibition restricts IFN-gamma
expression in crescentic glomerulonephritis. Kidney Int.
64:160–169. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nguyen MT and Devarajan P: Biomarkers for
the early detection of acute kidney injury. Pediatr Nephrol.
23:2151–2157. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Washburn KK, Zappitelli M, Arikan AA,
Loftis L, Yalavarthy R, Parikh CR, Edelstein CL and Goldstein SL:
Urinary interleukin-18 is an acute kidney injury biomarker in
critically ill children. Nephrol Dial Transplant. 23:566–572. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Araya C, Diaz L, Wasserfall C, Atkinson M,
Mu W, Johnson R and Garin E: T regulatory cell function in
idiopathic minimal lesion nephrotic syndrome. Pediatr Nephrol.
24:1691–1698. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wakkach A, Augier S, Breittmayer JP,
Blin-Wakkach C and Carle GF: Characterization of IL-10-secreting T
cells derived from regulatory CD4+CD25+ cells
by the TIRC7 surface marker. J Immunol. 180:6054–6063. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Barrat FJ, Cua DJ, Boonstra A, Richards
DF, Crain C, Savelkoul HF, de Waal-Malefyt R, Coffman RL,
Hawrylowicz CM and O'Garra A: In vitro generation of interleukin
10-producing regulatory CD4(+) T cells is induced by
immunosuppressive drugs and inhibited by T helper type 1 (Th1)- and
Th2-inducing cytokines. J Exp Med. 195:603–616. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kiliś-Pstrusińska K, Medyńska A, Zwolińska
D and Wawro A: Interleukin-18 in urine and serum of children with
idiopathic nephrotic syndrome. Kidney Blood Press Res. 31:122–126.
2008. View Article : Google Scholar : PubMed/NCBI
|