Introduction
Ewing sarcoma is a very rare malignant tumor usually
associated with femur, pelvis, ribs, and scapula (1). Ewing sarcoma originating from the
uterus is very rare. According to Loverro et al (2), only 48 cases of Ewing sarcoma have been
found in female genitalia until 2015. It is more common in men than
in women (55:45). Ewing sarcoma in young females is associated with
worse prognosis. It is predominantly seen in Caucasians rather than
in Asians or Black teenagers and young adults (3). Ewing sarcoma is associated with primary
site pelvic lengthening from the first sign until diagnosis
(4). Diagnosis of Ewing sarcoma
lesions is made through histological and physical examination, as
well as radiologically via X-ray, CT, bone scan, and magnetic
resonance imaging (MRI). A screening antibody is used to
characterize Ewing sarcoma cells immunohistochemically. Cytogenetic
and reverse transcription polymerase chain reaction (PCR) assays
are used to determine the presence of characteristic genetic
alterations in Ewing sarcoma cells. Molecular genetic testing has
revealed that most Ewing sarcoma cases have chromosomes 11 and 22
dislocations involving fusion of EWS gene on chromosome 22
and FLI1 gene on 11 (5).
Transmission of Ewing sarcoma is confirmed by standard imaging
technique or bone marrow aspirate/biopsy. Metastasis occurs in
about 25% of cases diagnosed with Ewing sarcoma (6).
Blood contains intact circulating tumor cells (CTCs)
and cell-free circulating tumor DNA (cfDNA), which facilitate
precise molecular diagnosis. In addition, blood sampling is
relatively noninvasive and easy. CTC and cfDNA carry mutations in
tissues of primary carcinomas. Clinical studies are investigating
the role of CTC and cfDNA in early diagnosis of cancer, monitoring
effects of anticancer therapy, and in prognosis. Liquid biopsy of
cancer is expected to become a new paradigm for ultra-precise
medicine (7,8). Centrifugal microfluidic system based on
a new fluid-assisted separation technology (FAST) has been
developed to detect CTCs in the blood based on their size and can
be used in a ‘Lab-on-a-disc’ to isolate CTCs in a few ml of blood
within a minute at high efficiency (more than 95%). The role of
blood CTCs has been investigated in cancer diagnosis based on
representative markers (9). Among
malignant neoplasms of hepatocellular origin, distant metastasis
occurs in half of sarcoma patients with primary lesions with
primary metastasis (10). Most
sarcomas spread through the vascular system following infiltration
of cells from primary carcinoma into blood vessels. These blood
CTCs float through the lymphatic system and cause metastasis
(11). To investigate the metastatic
process in rare cancers such as Ewing sarcoma and identify new
therapeutic targets, blood CTCs have been characterized using
biomarkers to predict prognosis of patients (12). In the present study, we found Ewing
sarcoma as primary carcinoma and blood CTCs of uterine origin in a
pediatric patient. Following liquid biopsy, molecular tests
including personalized genetic variation analysis were conducted.
Cancer mutations were monitored using CTC and cfDNA for
comprehensive insight into cancer progress and prognosis.
Case report
Ethics statements and informed
consent
The present study was approved by the Institutional
Review Board of Chonbuk National University Hospital (Jeonju,
Republic of Korea). It was conducted according to the Declaration
of Helsinki for biomedical research involving human subjects and
Guidelines for Good Clinical Practice. A detailed explanation of
this study was provided to all subjects. Written informed consent
was obtained from each participant prior to screening.
A 16-year-old female patient visited the hospital
with complaints of pain and a feeling of stabbing injury to the
underbelly. Abdominal distension occurred starting two weeks ago.
No specific personal or family history was detected. Abdominal
ultrasonography showed multiple diaphragmatic cysts on a thick wall
measuring about 12 cm in size. In addition to a hemoglobin level of
9.6 g/dl (normal range, 12 to 16 g/dl), LFT, BUN, creatinine, and
coagulation profiles were within normal range. No tumor markers
such as CA125, CA19-9, CEA, AFP, and hCG were detected either
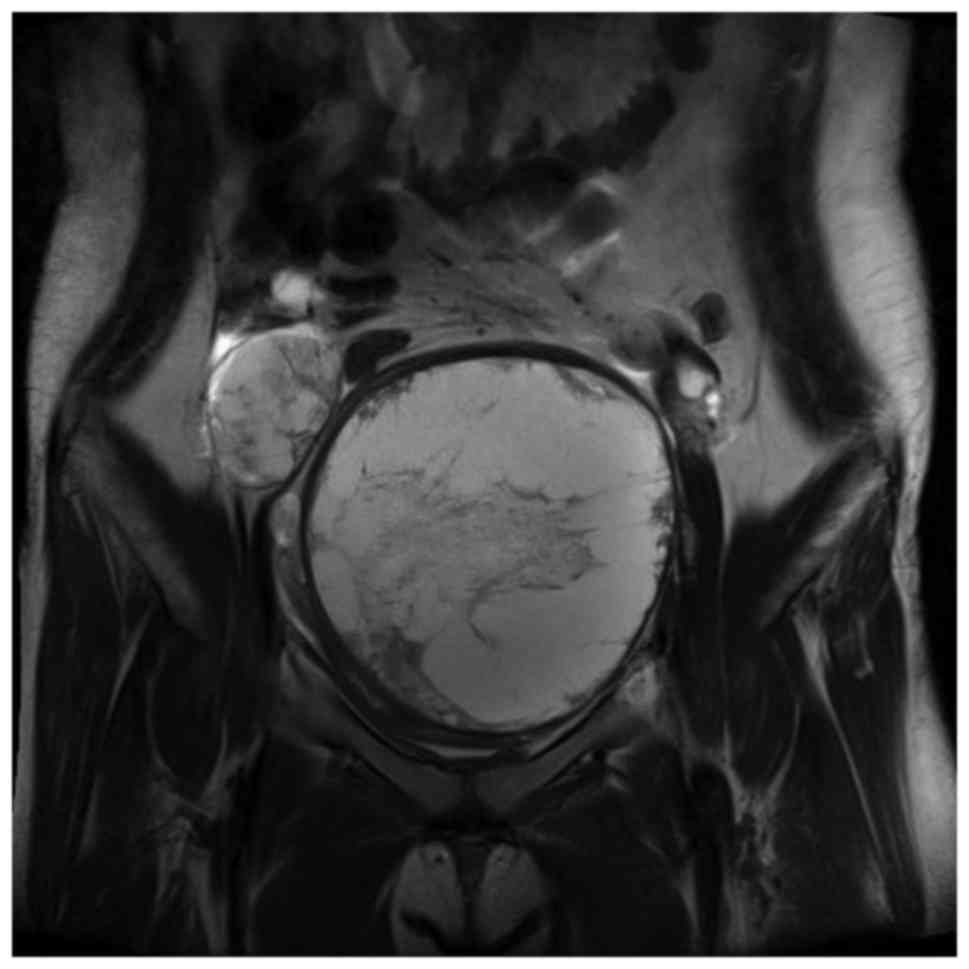
(Table I). This is a MRI image taken
at the first hospital visit. Pelvic MRI revealed a round mass
measuring 12.3×11.6×13.0 cm in size and located in the left pelvic
cavity. Multi-septate and focal wall thickening was also detected
(Fig. 1). Preoperative laparotomy
was performed under general anesthesia to investigate suspected
left ovarian tumor, which originated in the posterior wall of the
uterus. Complete excision of the mass was done followed by
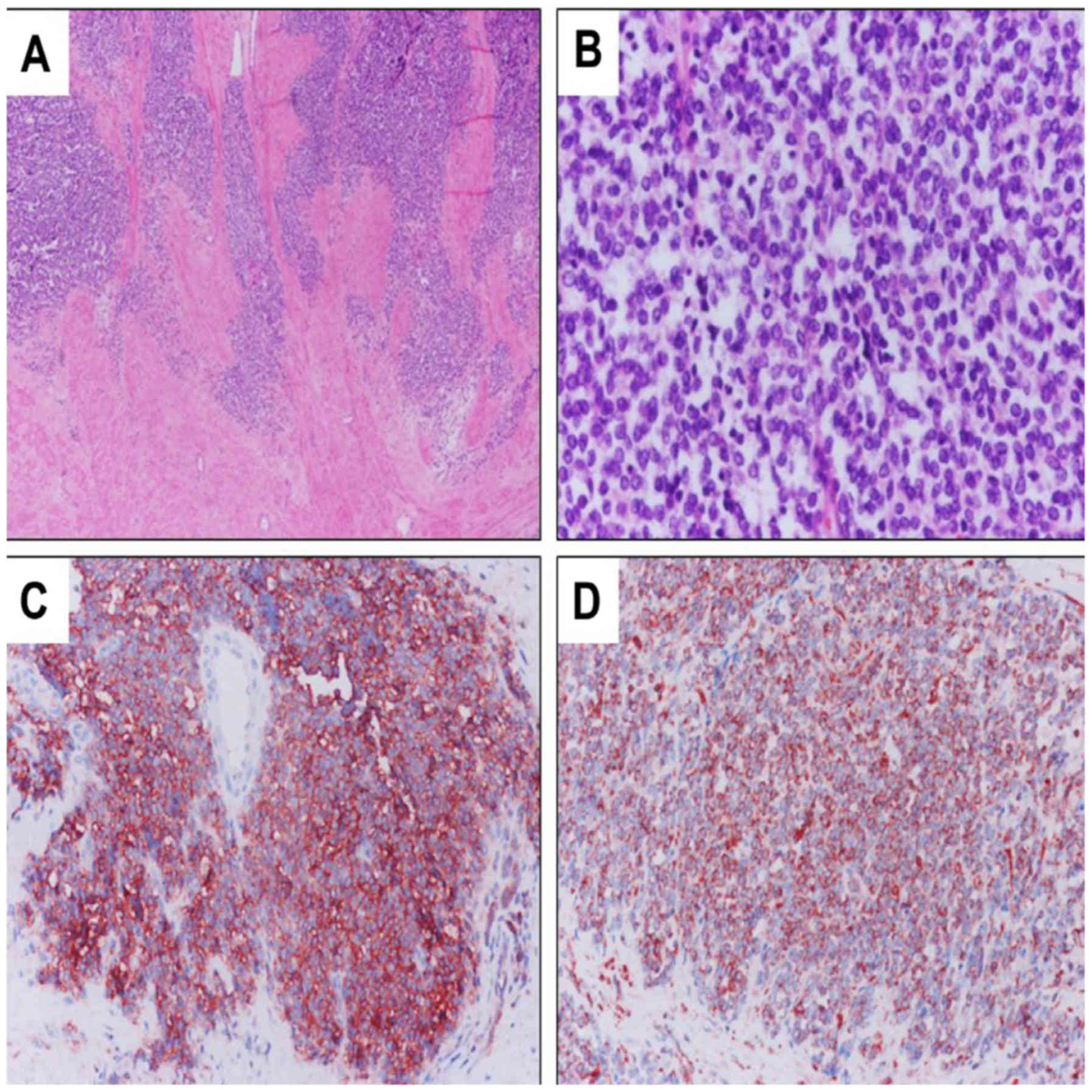
reconstruction of the uterus via myomectomy. Immunohistochemical
analysis of the patient's tissues confirmed positive results for
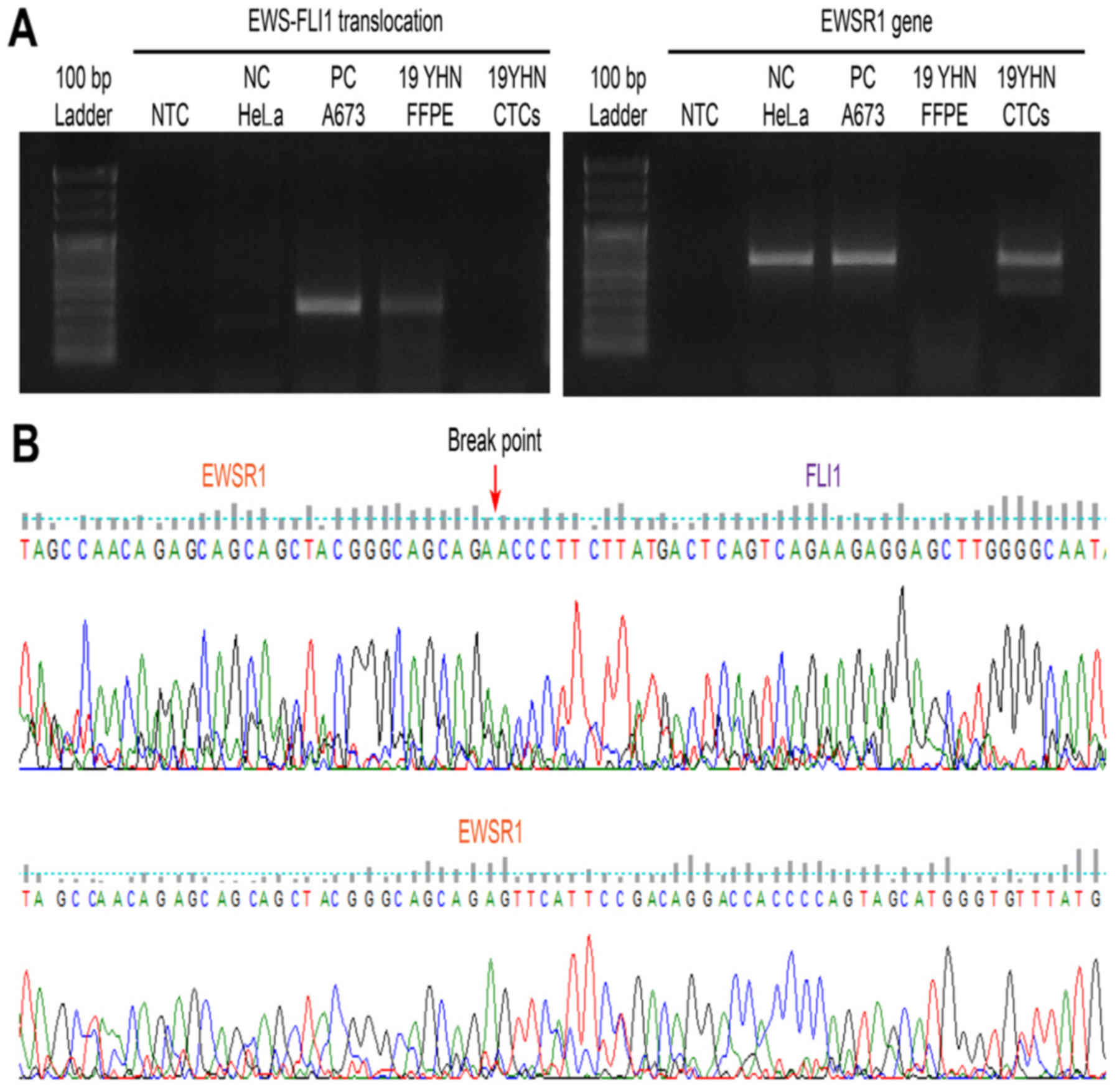
CD99, vimentin, S-100, EMA, and PAS (Fig. 2). Molecular genetic testing confirmed
the fusion of EWS gene on chromosome 22 and FLI1 gene on chromosome
11, a EWS-FLI1 translocation (Fig.
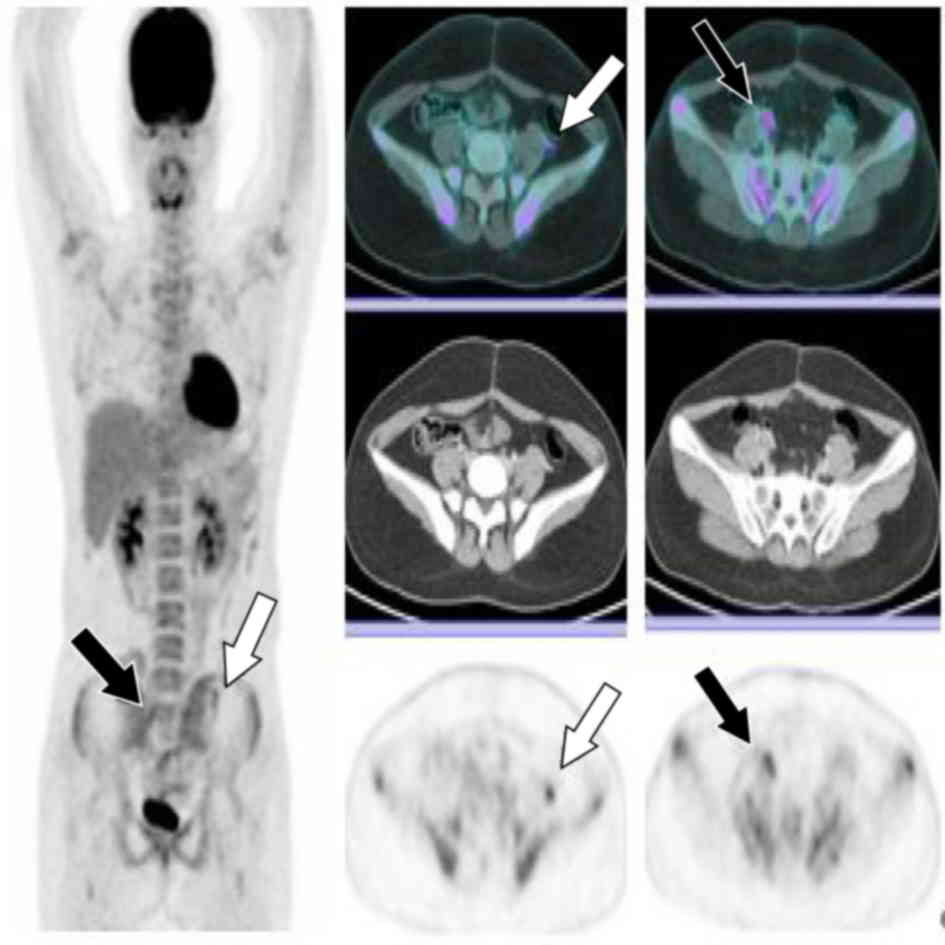
3). Bone scan and PET were performed preceded by postoperative
pelvic MRI, revealing no evidence of metastasis. Patients and
caregivers rejected reoperation and radiotherapy. Combination
chemotherapy regimens comprising VaC (vincristine, adriamycin,
cyclophosphamide) and IE (ifosfamide, etoposide) were administered.
Pelvic (lymph node) metastasis was confirmed in the eighth month
after complete remission (Fig. 4).
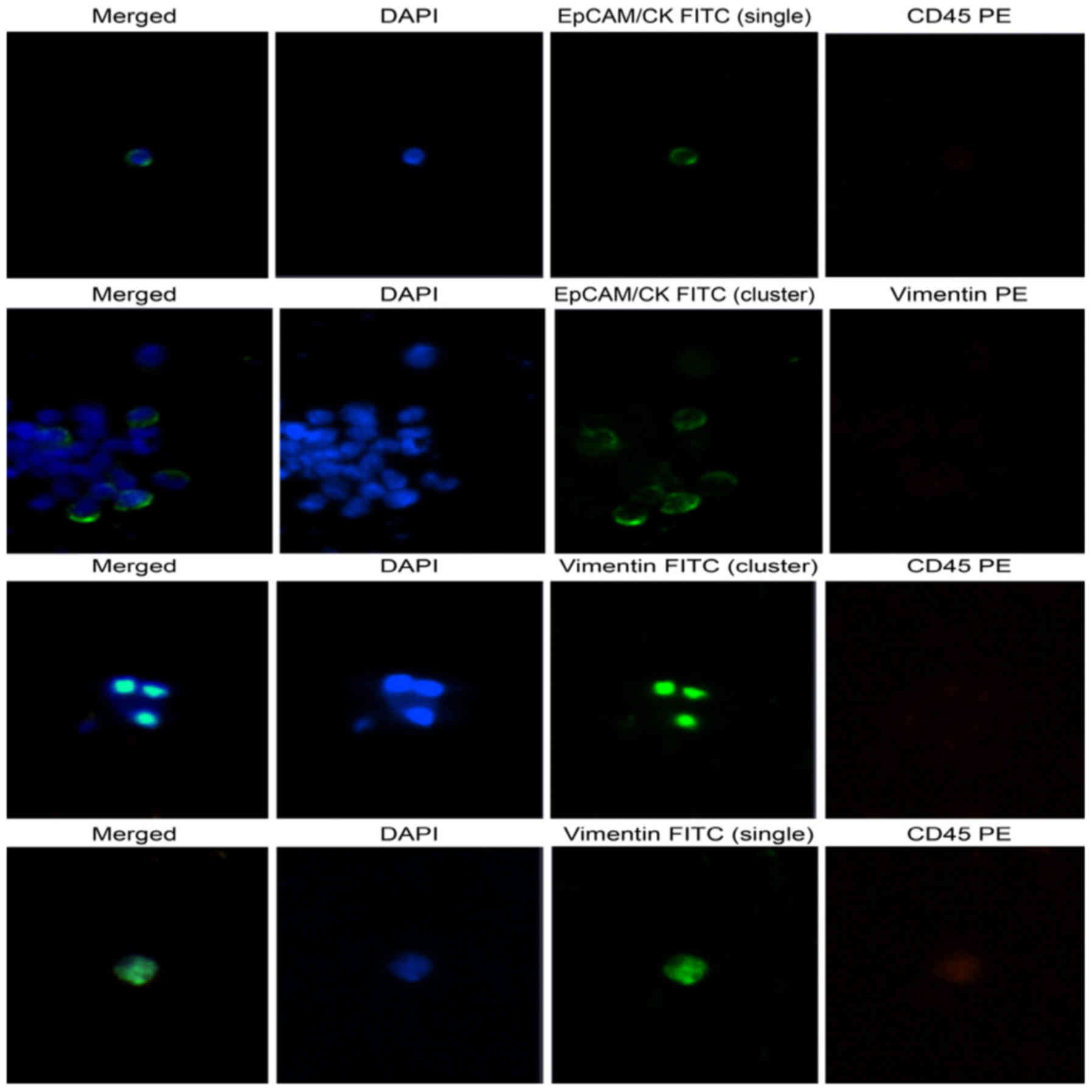
Using high-efficiency blood-CTC isolation technique, EpCAM-positive
CTCs and vimentin-positive CTCs were detected in the patient's
biopsy specimens (Fig. 5). The
patient underwent cervical lymph node metastasis five months after
transplantation, when EpCAM-positive CTCs and vimentin-positive
CTCs were confirmed by liquid phase biopsy (Table II).
 | Table I.Clinicopathological features of Ewing
sarcoma. |
Table I.
Clinicopathological features of Ewing
sarcoma.
| Characteristics | Feature |
|---|
| Sex | Female |
| Age | 16 |
| Primary site | Uterus
(extraosseous) |
| Initial symptom | Stabbing pain in
lower abdomen |
| Diagnostic
evaluation | MRI |
|
| PET/CT scan |
|
| Bone scan |
|
| X-ray |
| Blood chemistry
study |
|
| Hemoglobin | 9.6 g/dl |
| Liver function
test | Normal range |
| BUN | Normal range |
| Creatinine | Normal range |
| Coagulation
profile | Normal range |
| CA125 | 25.5 U/ml |
| CA19-9 | 4.16 U/ml |
| CEA | 1.66 ng/ml |
| AFP | 1.1 ng/ml |
| hCG | 0 mIU/m |
| IHC |
|
| CD99 | Positive, membranous
and cytoplasmic |
| Vimentin | Diffuse, 3+ |
| S-100 | Focal positive |
| EMA | Focal positive |
| PAS | Positive |
| Table II.Identification of EWS-FLI1 fusion in
FFPE and CTCs in Ewing sarcoma patients. |
Table II.
Identification of EWS-FLI1 fusion in
FFPE and CTCs in Ewing sarcoma patients.
| A673 spiking (no. of
cells) | NTC | 0.15 | 0.5 | 1.5 | 5 | 15 | 50 | 150 | 500 | Patient CTCs |
|---|
| PBMC (no. of
cells) | 2,000 |
|
|
|
|
|
|
|
|
|
|---|
| ∆∆Ct-1st | ND | 33.821 | 33.224 | 30.651 | 30.364 | 28.16 | 26.707 | 24.18 | 22.884 | ND |
| ∆∆Ct-2nd | ND | 34.292 | 33.346 | 30.531 | 30.276 |
28.058 | 26.454 |
24.206 | 22.937 | ND |
Chromosomal translocation analysis
using RT-PCR
Ewing sarcoma cell line A673 was used as a negative
control and a positive control. RNAs were extracted from CTCs
captured from membranes of Ewing sarcoma patients using RNeasy mini
kit (Qiagen GmbH, Hilden, Germany) following successful therapy.
RNA extraction from formalin-fixed paraffin-embedded (FFPE) slide
was performed using RNease FFPE kit (Qiagen GmbH) at the time of
Ewing sarcoma diagnosis. SuperScript VILO cDNA Synthesis Kit
(Invitrogen; Thermo Fisher Scientific, Inc., Waltham, MA, USA) was
used for cDNA synthesis, under the following reaction conditions:
25°C for 10 min, 42°C for 120 min, and 85°C for 5 min. To confirm
chromosomal translocation, RT-PCR was performed using specific
primers and Platinum PCR SuperMix High Fidelity (Invitrogen; Thermo
Fisher Scientific, Inc.). RT-PCR was performed under the following
conditions: 94°C for 10 min, 45 cycles of 94°C for 1 min, 68°C for
1 min, 72°C for 1 min 30 sec, and 72°C for 5 min (13). The following Ewing sarcoma-specific
fusion primers were used for RT-PCR: Forward primer,
5′-TCCTACAGCCAAGCTCCAAGTC-3′; Reverse primer,
5′-ACTCCCCGTTGGTTCCCCTCC-3′. PCR products were subjected to 1.5%
agarose gel electrophoresis at 50 volts for 15 min. The breakpoint
of EWS-FLI1 translocation was confirmed by RT-PCR and direct
sequencing using DNA from FFPE slide of Ewing sarcoma patient.
However, EWSR1 gene was sequenced (Cosmogenetech Inc., Seoul,
Republic of Korea) and detected in the patient's CTCs, confirming
the absence of gene arrangement (Fig.
3).
Immunohistochemical analysis
Enrichment and enumeration of
CTCs
A 21G needle was used to collect blood from the
patient into a K2 EDTA vacuum tube coated with anticoagulant (BD
Biosciences, Franklin Lakes, NJ, USA). The blood was mixed with
Ficoll-paque reagent in a 1:1 ratio. After separating mononuclear
cells, the CD-OPR-1000 driver and CD-PRIME systems of CD-CTC solo
disposable disk were used to isolate CTCs with high efficiency. The
CD-CTC Enrichment kit was used for cell enrichment. The membrane on
which CTCs were captured was placed on a glass slide (Clinomics,
Inc., Ulsan, Republic of Korea) and stained with EpCAM/CK, Pan-CK,
CD45, DAPI, vimentin-FITC, and vimentin-PE antibodies using CD-CTC
Enumeration kit. Stained CTCs were observed using a Bioview CCBS
system (BioView, Ltd., Nes Ziona, Israel). Of a total of 7,440
cells captured on the membrane, 175 (2.73%) tumor cells stained
positive for EpCAM/CK and pan-CK. Clustering of CTCs was observed
in 11 (6.28%) of these 175 DAPI-stained nuclei (Fig. 5).
Chromosomal translocation analysis
using RT-qPCR
CTCs were membrane-captured using CD-PRIME
(Clinomics, Inc.). RNAs were extracted from CTCs using QIAamp RNA
Blood Mini Kit (Qiagen GmbH). The quality of extracted RNA was
measured using Agilent RNA 6000 Pico Kit and 2100 Bioanalyzer
(Agilent Technologies, Inc., Santa Clara, CA, USA). However, RNA
integrity number (RIN) value or concentration was not obtained. RNA
concentration was measured using a Qubit RNA HS Assay kit and a
Qubit Fluorometer (Thermo Fisher Scientific, Inc.). However, it
showed a very low concentration. All the extracted RNAs were used
for cDNA synthesis using the same cDNA synthesis kit used for
RT-PCR. EWS-FLI1 primers (forward primer,
5′-CCAAGTCAATATAGCCAACAG-3′; reverse primer,
5′-GGCCAGAATTCATGTTATTGC-3′) were designed using the EWS-FLI1
fusion primer designed by Lewis et al (14), Power SYBR-Green PCR Master Mix and
ABI ViiA 7 Real-Time PCR system (Applied Biosystems; Thermo Fisher
Scientific, Inc.) were used for RT-qPCR. The following PCR program
parameters were used: Hold stage at 50°C for 2 min, 95°C for 10
min, and 40 cycles of 95°C for 15 sec and 60°C for 1 min. For melt
curve analysis, the following parameters were added: 95°C for 15
sec, 60°C for 1 min, and 95°C for 15 sec. After spiking A673 cells
to normal PBMC, the LOD value confirming EWS-FLI1 translocation
based on ΔΔCt value in RT-qPCR was found to be a mixing ratio of
one A673 cell to 2,000 normal PBMC cells. Using CTCs isolated from
patients, the ΔΔCt value was undetermined, indicating the absence
of EWS-FLI1 translocation (Table
II).
Personal genomic mutation profiling
using targeted massively parallel sequencing
DNA was extracted from FFPE slide prepared at the
time of laparotomy for the diagnosis of patient's Ewing sarcoma
using QIAamp DNA FFPE Tissue kit (Qiagen GmbH). Using CD-PRIME,
CTCs were captured from patient's blood when pelvic (lymph node)
metastasis occurred at eight months after the diagnosis. DNA was
extracted from CTCs using QIAamp DNA Micro kit (Qiagen GmbH). The
cfDNA was extracted from the patient's plasma using QIAamp
Circulating Nucleic Acid kit (Qiagen GmbH). Using Cancer-PRIME
(Clinomics, Inc.), a comprehensive cancer panel, sequencing was
performed on an Ion S5 platform (Thermo Fisher Scientific, Inc.)
according to the application guide. Mutations of FGFR4 (c.1162G>
a; p.G388A) and HRAS (c.182A> G; p.Q61R) were detected in DNA
extracted from FFPE. In DNA extracted from CTC, FGFR3 (c.1948A>
G; p.K650E) and the same FGFR4 (c.1162G> A; p.G388A) mutation
were detected in FFPE DNA. Therefore, the FGFR4 genetic mutation
was identified as a germ line mutation. In addition, FGFR3
(c.1948A> G; p.K650E), FGFR4 (c.1162G> A; p.G388A) and HRAS
(c.182A> G; p.Q61R) mutations in FFPE DNA and CTC DNA, were also
detected in cfDNA (Table III). On
the other hand, BRAF (c.1799T> A; p.V600E), CDKN2A
(c.1_471del471), or TP53 (c.354_355insCA) mutations were not
identified in Ewing sarcoma A673 cells. The CTNNB1
(c.133_135delTCT; p.S45del) or NRAS (c.181C> A; p.Q61K) mutation
identified in oncogene mutation profiling of Ewing sarcoma patients
reported by Shukla et al (15), was not identified in Ewing sarcoma
A673 cells either.
| Table III.Molecular genetics and mutational
analysis of Ewing sarcoma. |
Table III.
Molecular genetics and mutational
analysis of Ewing sarcoma.
|
|
|
|
|
| Patient |
|---|
|
|
|
|
|
|
|
|---|
| Gene | Mutation | Mutation type | CosmicID | Positive control
A673 | FFPE | CTCs | cfDNA |
|---|
| FGFR3 | c.1948A>G
(p.K650E) | Somatic | COSM719 |
|
| √ | √ |
| FGFR4 | c.1162G>A
(p.G388A) | Germline | – |
| √ | √ | √ |
| HRAS | c.182A>G
(p.Q61R) | Somatic | COSM499 |
| √ |
| √ |
| BRAF | c.1799T>A
(p.V600E) | Somatic | COSM476 | √ |
|
|
|
| CDKN2A | c.1_471del471
(p.0?) | Somatic | COSM12526 | √ |
|
|
|
| TP53 | c.354_355insCA
(p.A119fs*5) | Not confirmed | COSM26839 | √ |
|
|
|
Discussion
Ewing sarcoma is a very rare cancer. Skeletal Ewing
sarcoma is the most common (40%), followed by trunk (32%),
extremity limb (26%), head and neck (18%), retroperitoneum (16%),
and other sites (9%) (16). Ewing
sarcoma of the skeleton originating in the uterus is very rare.
Early symptoms of Ewing sarcoma include hemorrhage, pelvic mass,
uterine hypertrophy, abdominal pain, tibial pain, and metastasis of
the pelvis and lungs (17–19). Diagnosis of Ewing sarcoma is
confirmed via histopathological examination, blood tests, MRI,
PET/CT, bone scan, bone marrow aspiration, biopsy, and X-ray. Ewing
sarcoma cells are small and round in shape and blue in color.
Immunohistochemical analysis of the cells reveals positive staining
for CD99, Vimentin, and S-100 (20).
In the present study, early symptoms of Ewing sarcoma and
pathological findings were similar to those of previous reports.
Chromosomal translocation has been observed in about 90% of Ewing
sarcoma cases (21,22). The EWS-FLI1 fusion gene was also
observed in primary cancer tissues in this study. Although not
investigated in this study, EWS-FLI1 fusion gene can be observed
cytogenetically using FISH for diagnosis (19). EWS is known to play an
important role in the molecular diagnosis of sarcoma. Fusion of
EWS with chromosome 11q24 FLI1 gene, resulted in EWS gene
translocation (23). When EWS-FLI1
fusion gene was observed in primary cancer of the present study,
pelvic lymph node metastasis was confirmed radiologically at eight
months after complete remission. In this study, CTCs in the blood
were used for non-invasive diagnosis of Ewing sarcoma. The
detection of CTCs in the blood indicates pelvic lymph node
metastasis. EpCAM-positive CTCs are markers of circulating
epithelial tumor cells and sarcoma. In the present case, at the
time of pelvic lymph node metastasis, EpCAM and vimentin positive
CTCs were detected in mesenchymal cancer cell line. EWS-FLI1 fusion
did not occur in the patient's CTCs. However, the EWSR1 gene
sequence was confirmed in CTC suggesting that Ewing
sarcoma-specific fusion gene was no longer expressed following
treatment. Therefore, CTCs may be used as a noninvasive method to
predict prognosis following biopsy. However, despite the absence of
Ewing sarcoma-specific fusion gene in CTCs and detection of primary
cancer-derived cells with similar mutational features as the
primary cancer in the patient's blood, continuous invasive
monitoring of CTCs is needed. This study elucidates the role of
blood CTCs derived from primary cancer in diagnostic methods to
indicate the prognosis of cancer. Since Ewing sarcoma in the uterus
is rare, studies profiling its specific genetic mutations are very
limited. Shukla et al (15),
studied the profile of oncogene mutations in pediatric solid tumors
and found that Ewing sarcoma represented the smallest proportion
(19.73%, 75/380) of pediatric solid tumors. Based on sequence
analysis, genetic variation was found only in 4% (3/75) of these
subjects with Ewing sarcoma (15).
The mechanism involved in the release of CTCs and cf DNA into the
blood from primary cancers has yet to be elucidated. However, we
identified a pathogenic somatic mutation in the patient's blood
that closely resembled the genetic variation of CTC and cfDNA in
primary cancers because CTCs occur in the pathway of tumor cells
(originating from primary cancer tissues into the blood). However,
Ewing sarcoma-specific EWS-FLI1 translocation might be associated
with a favorable prognosis following treatment. Further studies are
needed to validate the role of CTCs and molecular pathologic
changes in cfDNA as indicators of cellular metastasis and
progression or treatment. In the present study, we used various
methods for the diagnosis of Ewing sarcoma, especially skeletal
Ewing sarcoma. In particular, liquid biopsy was performed using
CTCs and the DNA of circulating free cells in blood. Liquid biopsy
represents a relatively noninvasive and clinically significant
modality facilitating the monitoring of therapeutic effect and
prognosis in cancer, and therefore, is expected to play a pivotal
role in ultra-precise medicine.
Acknowledgements
Not applicable.
Funding
The present study was supported by a grant from the
Basic Research Program through the National Research Foundation
funded by the Ministry of Science, ICT & Future Planning,
Republic of Korea (grant no. 2017R1A2B4012353).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
SYL and DHC designed the study. SL performed the
experiment. SYL, SL and DHC analyzed the data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board of Chonbuk National University Hospital (Jeonju,
Republic of Korea). Written informed consent was obtained from the
participant.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of their data and associated
images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
FLI1
|
friend leukemia integration 1
transcription factor
|
|
CTCs
|
circulating tumor cells
|
|
LFT
|
liver function test
|
|
BUN
|
blood urea nitrogen
|
|
CA125
|
cancer antigen 125
|
|
CA19-9
|
cancer antigen 19-9
|
|
CEA
|
carcinoembryonic antigen
|
|
AFP
|
alpha-fetoprotein
|
|
hCG
|
human chorionic gonadotropin
|
|
LOD
|
limit of detection
|
|
EpCAM
|
epithelial cell adhesion molecule
|
|
FFPE
|
formalin-fixed paraffin-embedded
|
|
EDTA
|
ethylenediaminetetraacetic acid
|
|
PET/CT
|
positron emission tomography-computed
tomography
|
|
CK
|
cytokeratin
|
|
PBMC
|
peripheral blood mononuclear cell
|
|
TP53
|
tumor protein p53
|
|
FGFR3
|
fibroblast growth factor receptor
3
|
|
FGFR4
|
fibroblast growth factor receptor
4
|
|
HRAS
|
HRas proto-oncogene
|
|
CDKN2A
|
cyclin-dependent kinase inhibitor
2A
|
|
CTNNB1
|
catenin beta 1
|
|
NRAS
|
NRAS proto-oncogene
|
|
FISH
|
fluorescence in situ
hybridization
|
References
|
1
|
Burt M, Karpeh M, Ukoha O, Bains MS,
Martini N, McCormack PM, Rusch VW and Ginsberg RJ: Medical tumors
of the chest wall. Solitary plasmacytoma and Ewing's sarcoma. J
Thorac Cardiovasc Surg. 105:89–96. 1993.
|
|
2
|
Loverro G, Resta L, Di Naro E, Caringella
AM, Mastrolia SA, Vicino M, Tartagni M and Schonauer LM:
Conservative treatment of Ewing's sarcoma of the uterus in young
women. Case Rep Obstet Gynecol. 2015:8718212015.PubMed/NCBI
|
|
3
|
Jawad MU, Cheung MC, Min ES,
Schneiderbauer MM, Koniaris LG and Scully SP: Ewing sarcoma
demonstrates racial disparities in incidence-related and
sex-related differences in outcome: An analysis of 1631 cases from
the SEER database, 1973-2005. Cancer. 115:3526–3536. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Brasme JF, Chalumeau M, Oberlin O,
Valteau-Couanet D and Gaspar N: Time to diagnosis of Ewing tumors
in children and adolescents is not associated with metastasis or
survival: A prospective multicenter study of 436 patients. J Clin
Oncol. 32:1935–1940. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Owen LA, Kowalewski AA and Lessnick SL:
EWS/FLI mediates transcriptional repression via NKX2.2 during
oncogenic transformation in Ewing's sarcoma. PLoS One. 3:e19652008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Esiashvili N, Goodman M and Marcus RB Jr:
Changes in incidence and survival of Ewing sarcoma patients over
the past 3 decades: Surveillance epidemiology and end results data.
J Pediatr Hematol Oncol. 30:425–430. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shapiro B, Chakrabarty M, Cohn EM and Leon
SA: Determination of circulating DNA levels in patients with benign
or malignant gastrointestinal disease. Cancer. 51:2116–2120. 1983.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Crowley E, Di Nicolantonio F, Loupakis F
and Bardelli A: Liquid biopsy: Monitoring cancer-genetics in the
blood. Nat Rev Clin Oncol. 10:472–484. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim TH, Lim M, Park J, Oh JM, Kim H, Jeong
H, Lee SJ, Park HC, Jung S, Kim BC, et al: FAST: Size-selective,
clog-free isolation of rare cancer cells from whole blood at a
liquid-liquid interface. Anal Chem. 89:1155–1162. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mackall CL, Meltzer PS and Helman LJ:
Focus on sarcomas. Cancer Cell. 2:175–178. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pennacchioli E, Tosti G, Barberis M, De
Pas TM, Verrecchia F, Menicanti C, Testori A and Mazzarol G:
Sarcoma spreads primarily through the vascular system: Are there
biomarkers associated with vascular spread? Clin Exp Metastasis.
29:757–773. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tellez-Gabriel M, Brown HK, Young R,
Heymann MF and Heymann D: The challenges of detecting circulating
tumor cells in sarcoma. Front Oncol. 6:2022016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Aryee DN, Niedan S, Kauer M, Schwentner R,
Bennani-Baiti IM, Ban J, Muehlbacher K, Kreppel M, Walker RL,
Meltzer P, et al: Hypoxia modulates EWS-FLI1 transcriptional
signature and enhances the malignant properties of Ewing's sarcoma
cells in vitro. Cancer Res. 70:4015–4023. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lewis TB, Coffin CM and Bernard PS:
Differentiating Ewing's sarcoma from other round blue cell tumors
using a RT-PCR translocation panel on formalin-fixed
paraffin-embedded tissues. Mod Pathol. 20:397–404. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Shukla N, Ameur N, Yilmaz I, Nafa K, Lau
CY, Marchetti A, Borsu L, Barr FG and Ladanyi M: Oncogene mutation
profiling of pediatric solid tumors reveals significant subsets of
embryonal rhabdomyosarcoma and neuroblastoma with mutated genes in
growth signaling pathways. Clin Cancer Res. 18:748–757. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cates JM and Coffin CM: Neurogenic tumors
of soft tissue. Pediatr Dev Pathol. 15 1 Suppl:S62–S107. 2012.
View Article : Google Scholar
|
|
17
|
Park JY, Lee S, Kang HJ, Kim HS and Park
SY: Primary Ewing's sarcoma-primitive neuroectodermal tumor of the
uterus: A case report and literature review. Gynecol Oncol.
106:427–432. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fadare O: Uncommon sarcomas of the uterine
cervix: A review of selected entities. Diagn Pathol. 1:302006.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yi T, Wang P, Lin L and Jiang W: Ewing's
sarcoma/peripheral primitive neuroectodermal tumors of the uterus
confirmed with fluorescence in situ hybridization in a 29-year-old
Chinese female: A case report and published work review. J Obstet
Gynaecol Res. 41:478–482. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Iwamoto Y: Diagnosis and treatment of
Ewing's sarcoma. Jpn J Clin Oncol. 37:79–89. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Couturier J: Soft tissue tumors: Ewing's
tumors/Primitive neurectodermal tumors (PNET). Atlas Genet
Cytogenet Oncol Haematol. 2:148–150. 1998.
|
|
22
|
Turc-Carel C, Aurias A, Mugneret F, Lizard
S, Sidaner I, Volk C, Thiery JP, Olschwang S, Philip I, Berger MP,
et al: Chromosomes in Ewing's sarcoma. I. An evaluation of 85 cases
of remarkable consistency of t(11;22)(q24;q12). Cancer Genet
Cytogenet. 32:229–238. 1988.
|
|
23
|
Weiss S and Goldblum J: Extraskeletal
Ewing's sarcoma/primitive neuroectodermal tumor family. In:
Enzinger and Weiss's soft tissue tumors. 5th. Weiss SW and Goldblum
JR: Mosby, St Louis, MO: pp. 963–979. 2007
|