Introduction
Toxic epidermal necrolysis (TEN) and Stevens-Johnson
syndrome (SJS) are severe drug-induced diseases characterized by
the detachment of large areas of the epidermis and mucous membranes
(1,2). According to the area of epidermal
detaching in affected patients, disease severity ranges from SJS
(<10% of the body surface area) to TEN/SJS overlap (10–30% of
the body surface area) to TEN (>30% of the body surface area)
(1–3). SJS and TEN are rare, but potentially
life-threatening, disorders. It is reported that the mortality
rates at 6 weeks for SJS, TEN/SJS overlap, and SJS are 12, 29 and
46%, respectively (4). The
well-known chronic symptoms of TEN/SJS include ocular and cutaneous
sequelae and mucosal involvement (5). In clinical practice, acute pulmonary
complications are frequently observed in association with TEN/SJS.
However, chronic forms of pulmonary complications are rare, and
little is known regarding the prognosis, incidence and clinical
manifestations of patients with chronic complications.
The present study reports the case of a patient with
TEN who subsequently developed chronic bronchitis with severe
obstructive ventilatory impairment and bronchiectasis. In addition,
a review of the relevant literature is presented.
Case report
A 29-year-old Chinese woman with a chronic cough,
sputum production and a large number of red papules and erythemas
was referred to the Department of Dermatology, Ruijin Hospital
(Shanghai, China) for evaluation and treatment in April 2009. The
patient presented with a sore throat for 2 days and had
self-administered azithromycin (0.25 g) before being admitted to
hospital. However, several h after taking azithromycin, the patient
had rapidly developed a high fever (40°C) and facial erythema. By
the following day, the rash had spread to the trunk, back, upper
arms and thighs; this was immediately followed by the development
of large flaccid bullae, erythema and vesicular lesions of the
mouth, eyes and vulva. The erosion involved 60–70% of the patient's
body in a short period of time. Subsequently, a diagnosis of TEN
was established. Physical examination revealed that the lungs were
clear, without any expiratory rhonchi. Clubbing was absent, heart
sounds were normal, and Nikolsky's sign was positive. A chest X-ray
scan was taken once the patient was administered to hospital and
demonstrated no abnormalities. Following the diagnosis of TEN,
administration of methylprednisolone was given to the patient
immediately and initiated at 1 mg/kg per day. After 3 days, the
symptoms deteriorated and the bullae ruptured, producing large
areas of detached skin on the face, trunk and upper arms.
Therefore, the methylprednisolone dose was increased to 2 mg/kg per
day, and the patient began to improve at ~10 days after initiation
of the treatment. At 11 days after the onset of TEN, the patient
began to cough, producing scant mucus-like sputum. Pathological
examination of the lung tissue was not performed due to hypoxia.
Re-epithelialization was evident and complete on day 37 after
administration and the patient was then asymptomatic and discharged
from hospital. After intensive therapy, the patient recovered from
TEN, but scars remained and the patient suffered from severe
symblepharon.
However, 1 month after the release from hospital the
patient developed dyspnea and a productive cough. The patient was
then presented to Zhongshan Hospital, Fudan University (Shanghai,
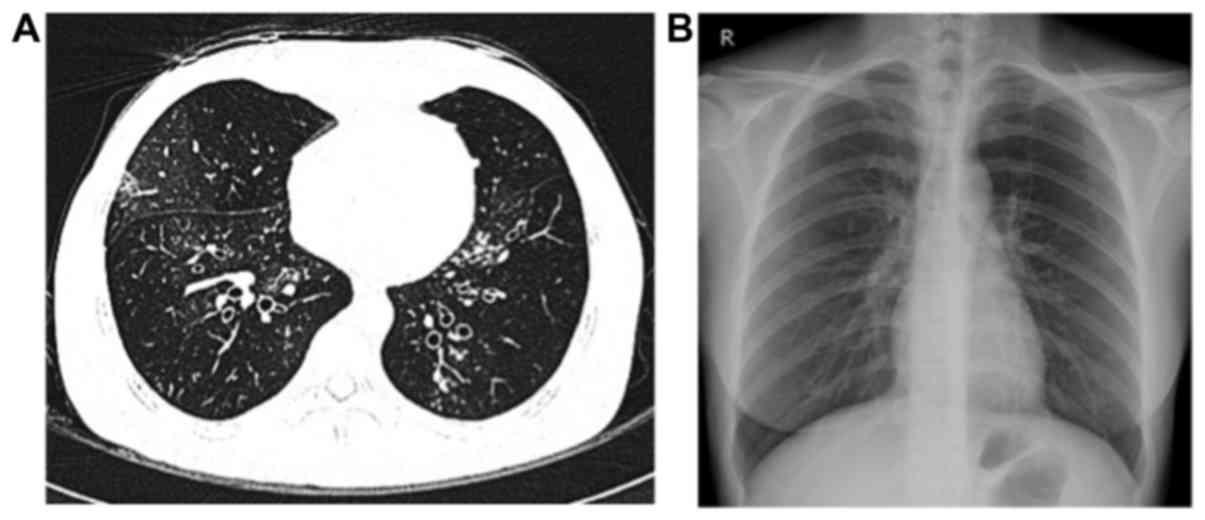
China). Blood gas examination revealed hypoxemia [partial pressure
of O2, 73 mmHg (normal range, 80–100 mmHg); partial
pressure of CO2, 39 mmHg (normal range, 35–45 mmHg)],
and pulmonary function tests demonstrated severe obstruction, with
a forced expiratory volume in 1 sec (FEV1) of 21.5%, FEV1/forced
vital capacity (FVC) of 46.6%, and a mild diffusion defect [FEV1,
0.45 liters (15% of predicted value); FVC, 42% of predicted value].
The single-breath diffusing capacity of the lungs for
CO2CO (DLCO) was 12.5 ml/mmHg/min (68% of the predicted
value), while the DLCO divided by the alveolar volume was 5.67
ml/mmHg/min (123% of the predicted value). Furthermore,
bronchodilation examination indicated non-reversible obstruction. A
chest high-resolution computed tomography (HRCT) scan demonstrated
central bronchiectasis (Fig. 1).
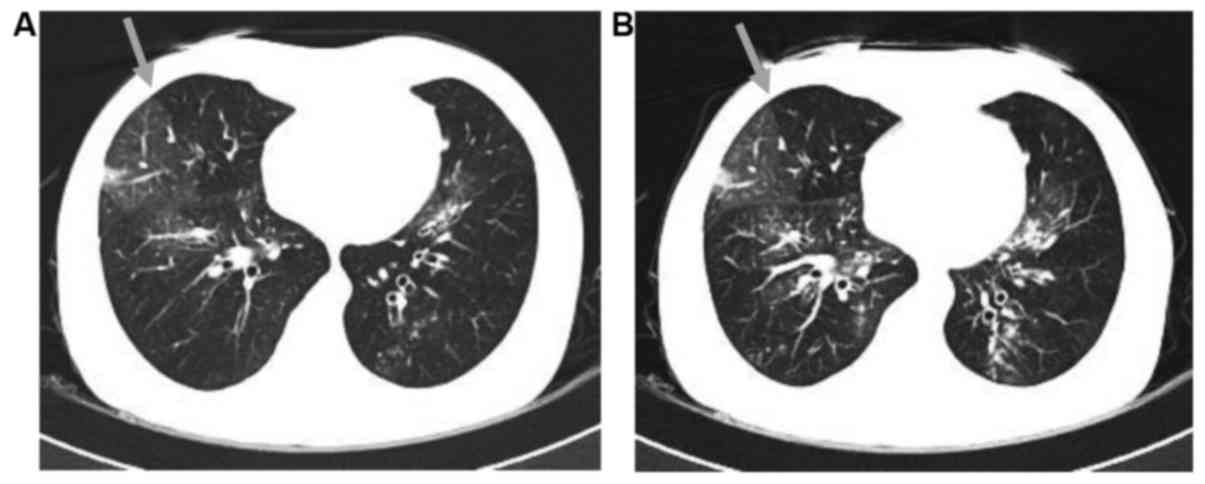
Subsequently, a chest CT with inspiratory and expiratory images was
further conducted to evaluate these findings. In the inspiratory
image (Fig. 2A), a heterogeneous
opacity was visible in a mosaic or patchy pattern. The expiratory
image (Fig. 2B) revealed an area of
trapped air in the lung, showing an attenuated intensity compared
with the adjacent normal lung. These results, including a
respiratory function test and radiological examination, were highly
suggestive of bronchiolitis obliterans (BO).
Therefore, the diagnosis of BO was established, and
tiotropium bromide powder (18 µg, inhalation) and salmeterol
xinafoate and fluticasone propionate powder (50/250 µg, inhalation)
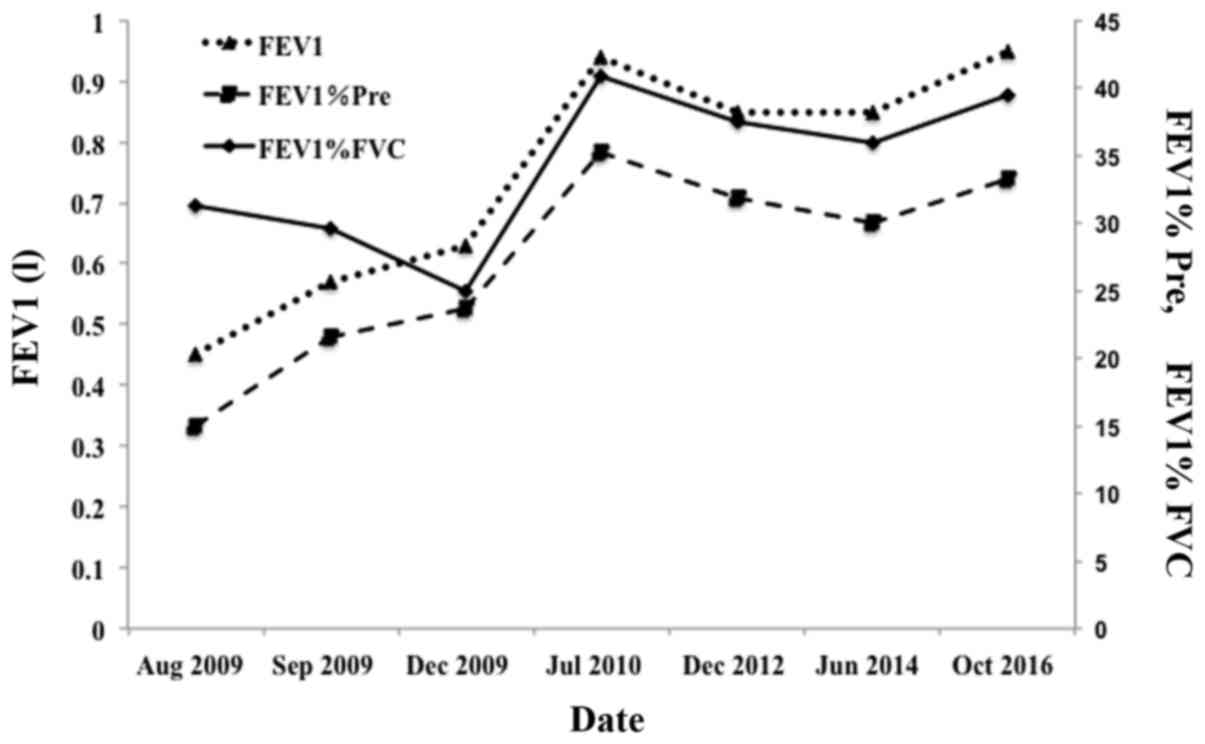
were administered. After 1 month, the FEV1 increased to 0.57 liters
(21.5% of predicted), and the FVC was 64.8% of the predicted value.
Furthermore, after 1 year, the FEV1 increased to 0.94 liters (35.3%
of predicted), the FEV1/FVC was 40.81% and the FVC was 76.1% of the
predicted value. At June 2017, 8 years after the onset of the
disease, the patient was alive. Pulmonary function examinations
demonstrated stability with the long-term use of long-acting
β2-agonists and inhaled corticosteroids (Fig. 3). However, the patient did not
recover completely and suffered from a chronic cough,
hypersecretion of sputum (with occasional blood) and exertional
dyspnea at the latest follow-up.
Discussion
Chronic pulmonary complications resulting from TEN
and SJS are rare. According to previous studies published in
English, 22 patients who suffered from chronic pulmonary diseases
following TEN/SJS were identified, including the present case
(6–24). The age of patients ranged between 2
and 52 years, and there were 10 male and 12 female patients
(Table I). Therefore, it appears
that chronic pulmonary diseases induced by TEN/SJS are likely to
occur at a younger age, and that there is no significant prevalence
associated with the patients' sex.
 | Table I.Chronic pulmonary complications
resulting from toxic epidermal necrolysis/Stevens-Johnson syndrome
in cases described in the present and previous studies. |
Table I.
Chronic pulmonary complications
resulting from toxic epidermal necrolysis/Stevens-Johnson syndrome
in cases described in the present and previous studies.
| First author | Age (years/sex) | Early pulmonary
symptoms | Chronic pulmonary
complication | Treatments | Outcome/time after
onset | (Refs.) |
|---|
| Taguchi et al | 53/M | − | BO | Steroid, antibiotics,
bronchodilator | Alive/26 months | (6) |
| Date et al | 13/M | + | BO | Living-donor lobar
lung transplantation | Alive/11 months | (7) |
| Minamihaba et al | 24/F | + | Bronchial
obstruction | Steroid,
bronchodilator, reopen by balloon catheter | Succumbed/1.3
years | (8) |
| Kim and Lee | 10/M | N/A | BO,
bronchiectasis | Steroid, antibiotics,
bronchodilator | Alive/1.8 years | (9) |
| Kim and Lee | 6/F | + | BO,
bronchiectasis | Steroid, antibiotics,
bronchodilator | Alive/2 years | (9) |
| Yatsunami et al | 25/M | + | BO,
bronchiectasis | Steroid, antibiotics,
bronchodilator | Alive/1 year | (10) |
| Edell et al | 8/F | − | Bronchial
obliteration | Steroid,
bronchodilator | Alive/7 months | (11) |
| Martín Mateos et
al | 5/F | N/A | Chronic bronchitis,
pneumopathy with deficit pulmonary perfusion | N/A | Alive/3 years | (12) |
| Tsunoda et al | 41/F | + | BO | Steroid,
bronchodilator | Succumbed/2
months | (13) |
| Reyes de la Rocha et
al | 15/F | + | Obstructive pulmonary
disease | Steroid,
bronchodilator | Alive/1.1 years | (14) |
| Virant et al | 2/F | + | Interstitial lung
disease | Antibiotics,
bronchodilator | Alive/1.5 months | (15) |
| Edwards et al | 8/M | + | Chronic obliterative
bronchitis | Steroid,
bronchodilator | Succumbed/9
months | (16) |
| Schønheyder | 8/M | + | Bronchiolar
obstruction | Steroid,
bronchodilator | Succumbed/3.5
months | (17) |
| McIvor et al | 40/F | + | BOOP | N/A | Succumbed/3
months | (18) |
| Kamada et al | 33/M | + | Chronic bronchitis,
bronchiectasis | Steroid, antibiotics,
bronchodilator | Succumbed/1.5
years | (19) |
| Bakirtas et al | 8/M | − | BO | Steroid, antibiotics,
bronchodilator | Alive/15 months | (20) |
| Bakirtas et al | 13/M | − | BO | Steroid, antibiotics,
bronchodilator | Alive/3 months | (20) |
| Thimmesch et al | 3/F | N/A | BO | Steroid, antibiotics,
bronchodilator | Alive/7 years | (21) |
| Yang et al | N/A | + | Interstitial lung
disease | Steroid | Alive/1 year | (22) |
| Shah et al | 13/F | + | Constrictive
bronchiolitis | Steroid,
antibiotics, bronchodilator | Alive/2 years | (23) |
| Woo et al | 29/F | − | Obliterative
bronchitis | Steroid,
immunosuppressants (cyclosporine), antibiotics | Succumbed/1.7
years | (24) |
| Present case | 29/F | + | BO | Steroid,
antibiotics, bronchodilator | Alive/8 years | N/A |
In the published literature, the precise interval
between the onset of TEN/SJS and the development of complications
was unknown. Certain patients developed chronic respiratory
symptoms after 1 month, while other patients developed these
symptoms after 1 week. However, the majority (13 out of 22
patients) demonstrated early pulmonary symptoms, including
wheezing, dyspnea, hypoxia or bloody sputum. In the present case,
the patient experienced dyspnea and hypoxia soon after the onset of
TEN. Following treatment with short-term, high-dose corticosteroid
therapy, the patient became asymptomatic, but then began to suffer
from severe respiratory obstruction 1 month later. On the basis of
these observations, it is suggested that the presence of early
pulmonary symptoms should prompt close monitoring for possible
delayed complications in these patients. However, the severity of
the chronic pulmonary symptoms does not appear to be correlated
with the severity of early pulmonary symptoms.
TEN and SJS are reported to be causes of several
types of chronic pulmonary complications (6–24). In
the current literature review, BO was observed in 10 cases,
respiratory tract obliteration/obstruction was present in 5 cases,
bronchiectasis in 4 cases, chronic (obliterative) bronchitis in 4
cases, interstitial lung disease in 2 cases, while BO organizing
pneumonia (BOOP), obstructive pulmonary disease and pneumopathy
with pulmonary perfusion deficit were each observed in 1 case.
These cases demonstrated that the most common manifestations of
chronic pulmonary complications associated with SJS or TEN are
chronic bronchitis/bronchiolitis with obstructive impairment
(including BO and BOOP), bronchiectasis and respiratory tract
obstruction. In the present case, the patient presented BO with a
severe obstructive ventilatory impairment. Several diseases can
cause BO, and the known causes include connective tissue disorders
(the most common factor), infections, inhalational injury, drugs
and organ transplantation among others (25). In the current case, the patient did
not have any rheumatologic manifestations. Upon referral to
Zhongshan Hospital, the patient's lungs were clear, viral antibody
tests were negative, while no abnormalities were identified on the
chest X-ray scans. The patient had not previously suffered from
chronic cough, and had no history of asthma, chronic obstructive
pulmonary disease, bronchiectasis or organ transplantation.
Therefore, it is suggested that TEN was responsible for the
development of BO in the present case.
In previous studies (13,17,18), the
prognoses of chronic pulmonary complications resulting from TEN/SJS
were considered to be poor. Considering all the relevant studies
published to date that were identified by the present study, 4
patients who suffered from chronic pulmonary complications from
TEN/SJS succumbed to the disease within 1 year, and a further 3
patients succumbed within 2 years, whereas 4 patients survived for
>2 years and 1 patient survived for >7 years. In the present
case, the patient survived for >8 years. Although the patient
suffered from chronic severe obstruction, the lung function (FEV1
and FEV1% predicted) was slightly improved, which may be due to the
alleviation of the inflammatory response by long-term use of
inhalation of corticosteroid and long-acting β2-agonist.
Thus, it appears that it is possible for such patients to survive
for a long time, and the prognosis of patients with chronic
pulmonary complications is not necessarily poor.
Treatment of chronic pulmonary complications mainly
includes the administration of antibiotics, bronchodilators and
steroids; however, these treatments do not reverse the
deterioration of the pulmonary function (6). A living-donor lobar lung
transplantation was performed in 1 previous case and presented good
results (7). Reopening of the
obstructed bronchi using a balloon catheter under the guidance of
fiber-optic bronchoscopy was also applied in 1 patient who
developed BO following TEN (8).
However, rapid restenosis of the bronchi occurred, leading to the
hypothesis that inflammatory responses may persist for a prolonged
period subsequent to the onset of TEN/SJS. However, in the present
case, the results of follow-up pulmonary function examinations
following the development of chronic pulmonary complications
suggested that inflammatory responses are likely to generally
improve during the chronic phase of pulmonary complications
(Fig. 3).
In conclusion, not only skin, but also respiratory
tract is simultaneously injured in TEN. Therefore, physicians
should be alert not only of acute symptoms but also the chronic
pulmonary complications. The majority of patients with TEN/SJS
generally experience deteriorating pulmonary function, rather than
improvement. Therefore, when patients begin to present persistent
pulmonary difficulties, early, intense and sustained treatment
should be administered. This may maintain or even slightly improve
the patient's pulmonary function. Therefore, close monitoring,
including pulmonary function examinations and HRCT, is advised for
patients with TEN/SJS.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant no. 81401877), the
Program for Young Talents of Zhongshan Hospital, Fudan University
(grant no. 2015ZSYXQN18) and the Shanghai Three-Year Plan of the
Key Subjects Construction in Public Health-Infectious Diseases and
Pathogenic Microorganism (grant no. 15GWZK0102).
References
|
1
|
Mawson AR, Eriator I and Karre S:
Stevens-Johnson syndrome and toxic epidermal necrolysis (SJS/TEN):
Could retinoids play a causative role? Med Sci Monit. 21:133–143.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Letko E, Papaliodis DN, Papaliodis GN,
Daoud YJ, Ahmed AR and Foster CS: Stevens-Johnson syndrome and
toxic epidermal necrolysis: A review of the literature. Ann Allergy
Asthma Immunol. 94(419–438): 4562005.
|
|
3
|
Bastuji-Garin S, Rzany B, Stern RS, Shear
NH, Naldi L and Roujeau JC: Clinical classification of cases of
toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema
multiforme. Arch Dermatol. 129:92–96. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sekula P, Dunant A, Mockenhaupt M, Naldi
L, Bavinck Bouwes JN, Halevy S, Kardaun S, Sidoroff A, Liss Y,
Schumacher M, et al: Comprehensive survival analysis of a cohort of
patients with Stevens-Johnson syndrome and toxic epidermal
necrolysis. J Invest Dermatol. 133:1197–1204. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Roujeau JC and Stern RS: Severe adverse
cutaneous reactions to drugs. N Engl J Med. 331:1272–1285. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Taguchi S, Furuta J, Ohara G, Kagohashi K
and Satoh H: Severe airflow obstruction in a patient with
ulcerative colitis and toxic epidermal necrolysis: A case report.
Exp Ther Med. 9:1944–1946. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Date H, Sano Y, Aoe M, Goto K, Tedoriya T,
Sano S, Andou A and Shimizu N: Living-donor lobar lung
transplantation for bronchiolitis obliterans after Stevens-Johnson
syndrome. J Thorac Cardiovasc Surg. 123:389–391. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Minamihaba O, Nakamura H, Sata M, Inage M,
Shirakabe M, Tanida H, Osada Y, Kondo S and Tomoike H: Progressive
bronchial obstruction associated with toxic epidermal necrolysis.
Respirology. 4:93–95. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim MJ and Lee KY: Bronchiolitis
obliterans in children with Stevens-Johnson syndrome: Follow-up
with high resolution CT. Pediatr Radiol. 26:22–25. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yatsunami J, Nakanishi Y, Matsuki H,
Wakamatsu K, Takayama K, Kawasaki M, Ogino H, Hashimoto S and Hara
N: Chronic bronchobronchiolitis obliterans associated with
Stevens-Johnson syndrome. Intern Med. 34:772–775. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Edell DS, Davidson JJ, Muelenaer AA and
Majure M: Unusual manifestation of Stevens-Johnson syndrome
involving the respiratory and gastrointestinal tract. Pediatrics.
89:429–432. 1992.PubMed/NCBI
|
|
12
|
Mateos Martín MA, Polemeque A, Pastor X
and Muñoz López F: Uncommon serious complications in
Stevens-Johnson syndrome: A clinical case. J Investig Allergol Clin
Immunol. 2:278–283. 1992.PubMed/NCBI
|
|
13
|
Tsunoda N, Iwanaga T, Saito T, Kitamura S
and Saito K: Rapidly progressive bronchiolitis obliterans
associated with Stevens-Johnson syndrome. Chest. 98:243–245. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
de la Rocha Reyes S, Leonard JC and
Demetriou E: Potential permanent respiratory sequela of
Stevens-Johnson syndrome in an adolescent. J Adolesc Health Care.
6:220–223. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Virant FS, Redding GJ and Novack AH:
Multiple pulmonary complications in a patient with Stevens-Johnson
syndrome. Clin Pediatr (Phila). 23:412–414. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Edwards C, Penny M and Newman J:
Mycoplasma pneumonia, Stevens-Johnson syndrome, and chronic
obliterative bronchitis. Thorax. 38:867–869. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Schønheyder H: Stevens-Johnson syndrome
associated with intrahepatic cholestasis and respiratory disease: A
case report. Acta Derm Venereol. 61:171–173. 1981.PubMed/NCBI
|
|
18
|
McIvor RA, Zaidi J, Peters WJ and Hyland
RH: Acute and chronic respiratory complications of toxic epidermal
necrolysis. J Burn Care Rehabil. 17:237–240. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kamada N, Kinoshita K, Togawa Y, Kobayashi
T, Matsubara H, Kohno M, Igari H, Kuriyama T, Nakamura M, Hirasawa
H and Shinkai H: Chronic pulmonary complications associated with
toxic epidermal necrolysis: Report of a severe case with
anti-Ro/SS-A and a review of the published work. J Dermatol.
33:616–622. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bakirtas A, Harmanci K, Toyran M, Razi CH
and Turktas I: Bronchiolitis obliterans: A rare chronic pulmonary
complication associated with Stevens-Johnson syndrome. Pediatr
Dermatol. 24:E22–E25. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Thimmesch M, Gilbert A, Tuerlinckx D and
Bodart E: Chronic respiratory failure due to toxic epidermal
necrosis in a 10 year old girl. Acta Clin Belg. 70:69–71. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yang CW, Cho YT, Chen KL, Chen YC, Song HL
and Chu CY: Long-term sequelae of Stevens-Johnson syndrome/toxic
epidermal necrolysis. Acta Derm Venereol. 96:525–529. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shah AP, Xu H, Sime PJ and Trawick DR:
Severe airflow obstruction and eosinophilic lung disease after
Stevens-Johnson syndrome. Eur Respir J. 28:1276–1279. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Woo T, Saito H, Yamakawa Y, Komatsu S,
Onuma S, Okudela K, Nozawa A, Aihara M, Ikezawa Z and Ishigatsubo
Y: Severe obliterative bronchitis associated with Stevens-Johnson
syndrome. Intern Med. 50:2823–2827. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ryu JH, Myers JL and Swensen SJ:
Bronchiolar disorders. Am J Respir Crit Care Med. 168:1277–1292.
2003. View Article : Google Scholar : PubMed/NCBI
|