Introduction
Down syndrome (DS), also known as trisomy 21
syndrome, is the most common human chromosomal condition (1). Its incidence in newborns ranges from
1/800 to 1/1000 (2). The incidences
of trisomy 18 and trisomy 13 syndromes were next only to that of
trisomy 21 syndrome (3). The major
characteristics of clinical manifestations are severe congenital
mental retardation and unique facial features, which are often
accompanied by a variety of congenital malformations or other
abnormalities (4). These syndromes
cannot be cured. Prenatal diagnosis is the only way to prevent
birth of children with defects (5).
Therefore, early screening, early diagnosis, and timely termination
of pregnancy are important measures to reduce birth defects
(6).
Traditional prenatal diagnosis is actually
conventional karyotype analysis of fetal chromosomes, which detects
limited types of chromosomal abnormalities, and takes longer to
obtain results (7). Prenatal
BACs-on-Beads (BoBs) is a newly-developed and efficient molecular
diagnostic technique. This new technology can quickly detect 5
common aneuploidy abnormalities (21, 18, 13, X, Y), and 9 common
microdeletion syndromes as well (8).
In order to improve the prenatal diagnostic rate and
reduce the incidence of birth defects, in this study, prenatal BoBs
assay was performed together with the traditional karyotype
analysis, aiming to explore potential benefits of combination of
the two testing methods in prenatal diagnosis.
Subjects and methods
Subjects
A total of 558 pregnant women who were admitted to
Xuzhou Maternity and Child Health Care Hospital from July 2015 to
June 2017 were enrolled in this study. All the subjects gave their
informed consent for the study. At 19–24 weeks of pregnancy, the
subjects underwent amniocentesis for karyotype analysis combined
with BoBs assay of amniotic fluid. Prenatal conditions of pregnant
women included: Advanced maternal age, high-risk with prenatal
screening, abnormal findings with non-invasive prenatal testing
(NIPT), fetal ultrasound abnormalities, chromosomal abnormalities
in pregnant women or their husbands, and previous birth of child
with chromosomal abnormalities. The study was approved by the
Ethics Committee of Xuzhou Maternity and Child Health Care
Hospital.
Methods
Amniocentesis
Subjects signed the informed consent form before
undergoing the procedure. Amniocentesis was performed under
ultrasound guidance. Amniotic fluid (25 ml) was withdrawn, of which
20 ml was cultured to allow for karyotype analysis of chromosomes,
and the remaining 5 ml was used for BoBs assay.
Chromosome karyotype analysis
Approximately 20 ml of amniotic fluid was
centrifuged at 2,500 × g for 10 min at 4°C to separate amniotic
cells. The cells were cultured, harvested and mounted on glass
slides after routine treatments for chromosome G-banded analysis.
On each slide, 30 stained metaphases were examined, and 5
karyograms were created for chromosome analysis. If a suspicious
chromosomal abnormality or chromosomal polymorphism was found, the
count number of metaphases was then increased to 50, and the number
of karyograms was increased to ≥20 for a more reliable result.
BoBs assay
Genomic DNA was extracted from approximatley 5 ml of
amniotic fluid using DNA extraction reagents according to
manufacturer's instructions. BoBs kit (Perkin Elmer, Waltham, MA,
USA) was used for BoBs assay. The beads were analyzed using a
Luminex 200 cytometric acquisition system (Austin, TX, USA) for
data collection. Data were analyzed using BoBsoft 2.0 software.
Indicators observed
The subjects were divided into the observation and
control groups. Karyotype analysis was performed on the control
group, and BoBs assay was performed on the observation group. The
major technical indicators were summarized, and cases of
chromosomal abnormalities were further evaluated.
Statistical analysis
Statistical analysis was performed using the SPSS
19.0 software (IBM SPSS, Armonk, NY, USA). Comparison between
multiple groups was done using one-way ANOVA test followed by post
hoc test (Least Significant Difference). P<0.05 was considered
to indicate a statistically significant difference.
Results
Comparsion of karyotype analysis
(control group) and BoBs assay (observation group)
Detection time was shorter in the observation group
(BoBs technique) than in the control group, and the number of
chromosomal loci detected was less than that of the control group.
However, 9 more microdeletions were added to the detection range
(Table I).
 | Table I.Karyotype analysis (control group) and
BACs-on-Beads assay (observation group). |
Table I.
Karyotype analysis (control group) and
BACs-on-Beads assay (observation group).
| Groups | Test time | Items tested |
|---|
| Observation | 24 h | 21, 18, 13, X, Y
chromosomes and 9 microdeletions |
| Control | 3 weeks | 46 chromosomes |
Number of amniocentesis performed for
high-risk pregnant women with different prenatal conditions
Amniocentesis was mainly performed for pregnant
women with high-risk with prenatal screening (non-invasive positive
was not included), advanced maternal age pregnant women
(non-invasive positive was not included) and pregnant women with
sex chromosomal abnormalities with NIPT (Tables II and III).
| Table II.Prenatal conditions of high-risk
pregnant women that underwent amniocentesis. |
Table II.
Prenatal conditions of high-risk
pregnant women that underwent amniocentesis.
| Prenatal
conditions | Cases |
|---|
| Trisomy 21 with
non-invasive prenatal testing | 60 |
| Trisomy 18 with
non-invasive prenatal testing | 16 |
| Trisomy 13 with
non-invasive prenatal testing | 1 |
| Sex chromosomal
abnormalities with non-invasive prenatal testing | 61 |
| High-risk with
prenatal screening (not including positive findings with
non-invasive prenatal testing) | 195 |
| Advanced maternal age
(not including positive findings with non-invasive prenatal
testing) | 128 |
| Abnormal findings
with color Doppler ultrasound (not including positive findings with
non-invasive prenatal testing) | 56 |
| Chromosomal
abnormalities in pregnant women or their husbands | 17 |
| Previous birth of
child with chromosomal abnormalities | 54 |
| Total | 588 |
| Table III.Prenatal diagnostic outcomes of
pregnant women with different prenatal conditions. |
Table III.
Prenatal diagnostic outcomes of
pregnant women with different prenatal conditions.
|
| Diagnostic
outcome |
|---|
|
|
|
|---|
| Prenatal
conditions | Trisomy 21 | Trisomy 18 | Trisomy 13 | Sex chromosomal
abnormalities | Balanced chromosome
translocation | Chromosome
microdeletion |
|---|
| Positive findings
with non-invasive prenatal testing (T21, T18 and T13) | 60 | 16 | 1 | 24 | 0 | 0 |
| High-risk with
prenatal screening (not including positive findings with
non-invasive prenatal testing) | 2 | 0 | 0 | 2 | 0 | 0 |
| Advanced maternal age
(not including positive findings with non-invasive prenatal
testing) | 3 | 0 | 0 | 1 | 0 | 0 |
| Abnormal findings
with color Doppler ultrasound (not including positive findings with
non-invasive prenatal testing) | 9 | 4 | 0 | 0 | 1 | 1 |
| Chromosomal
abnormalities in pregnant women or their husbands | 1 | 0 | 0 | 0 | 11 | 0 |
| Previous birth of
child with chromosomal abnormalities | 0 | 0 | 0 | 0 | 0 | 0 |
| Total cases | 75 | 20 | 1 | 27 | 12 | 1 |
Diagnostic outcomes of pregnant women
in the observation group and the control group
Test results of chromosomal abnormalities showed
that the diagnostic outcomes of two groups were similar in trisomy
21, trisomy 18, trisomy 13 and sex chromosomal abnormalities.
Balanced chromosome translocation were detected in the control
group but not in the observation group. Chromosome microdeletion
were detected in the observation group but not in the control
group. The two tests complement each other, and the difference was
statistically significant (p<0.05) (Table IV).
| Table IV.Comparison of diagnostic outcomes
between observation group and control group. |
Table IV.
Comparison of diagnostic outcomes
between observation group and control group.
| Groups | Trisomy 21 | Trisomy 18 | Trisomy 13 | Sex chromosomal
abnormalities | Balanced chromosome
translocation | Chromosome
microdeletion |
|---|
| Observation | 75 | 20 | 1 | 27 | 0 | 1 |
| Control | 75 | 20 | 1 | 27 | 12 | 0 |
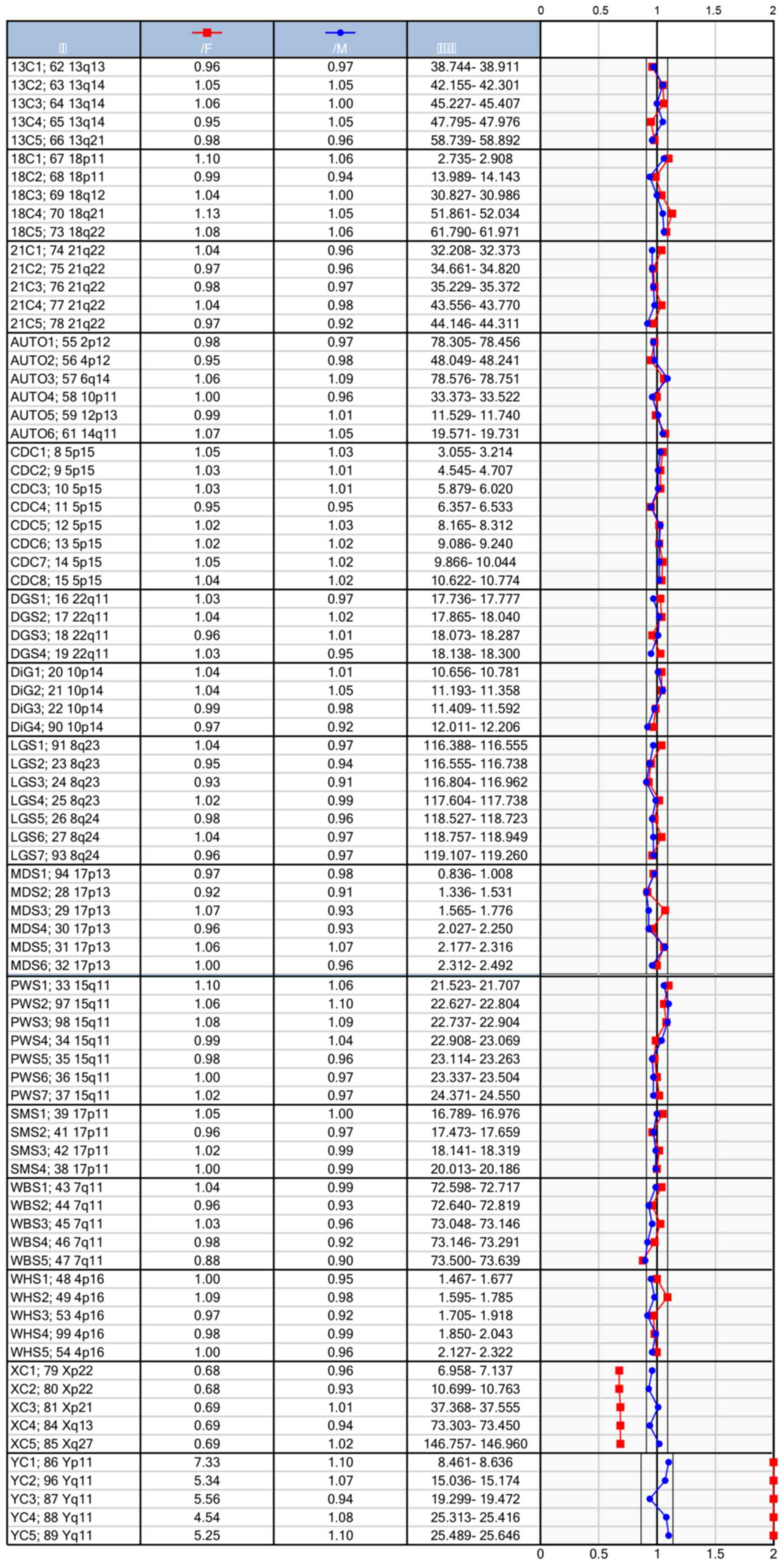
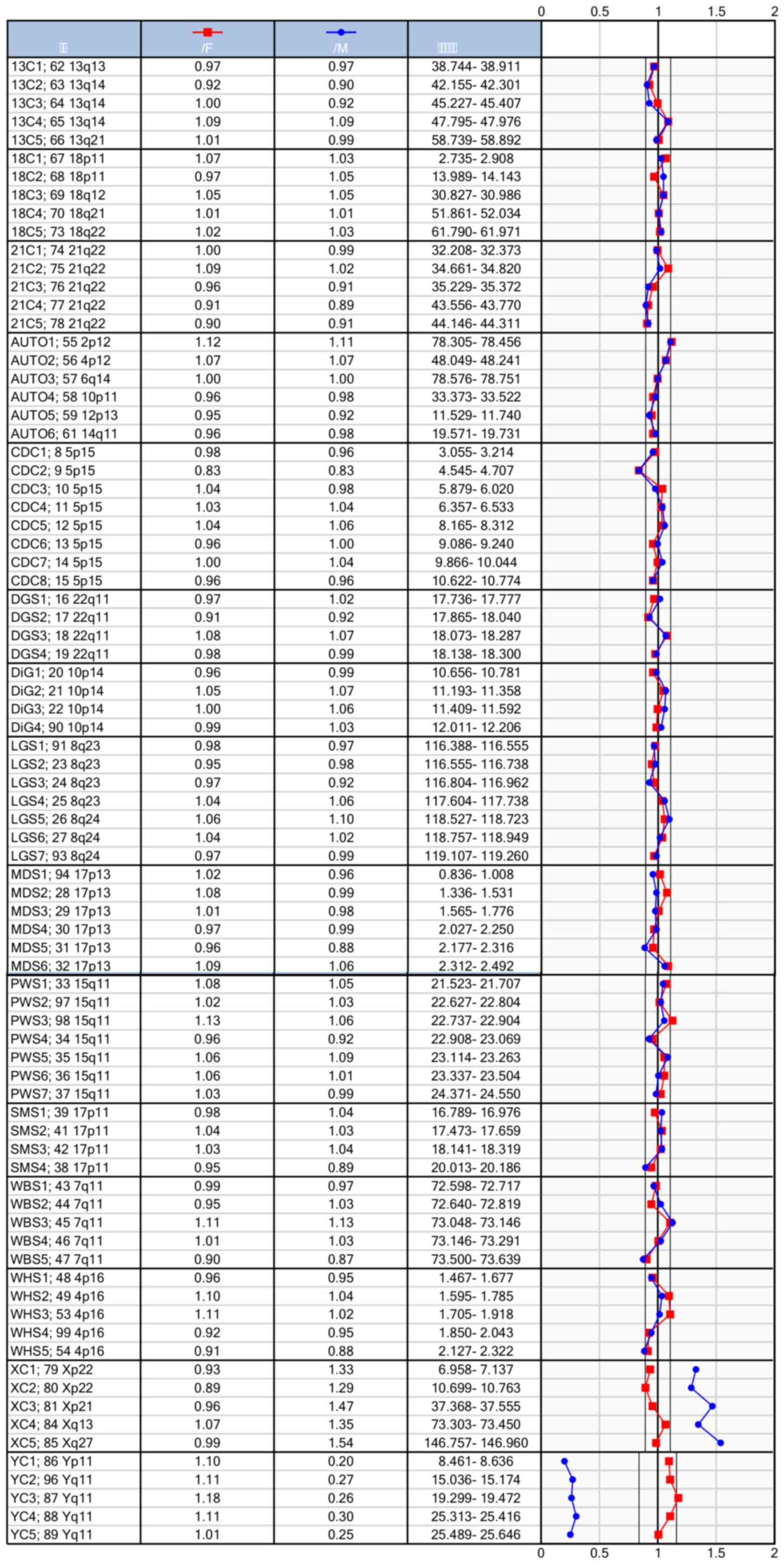
Reports of normal findings with BoBs
assay
DNA probes were added to the fluorescently-labeled
(red) microspheres. After amplification by PCR and fluorescent
labeling (blue), the genotypes of the samples were determined.
Figs. 1 and 2 show the genomic sequence of normal males
and females.
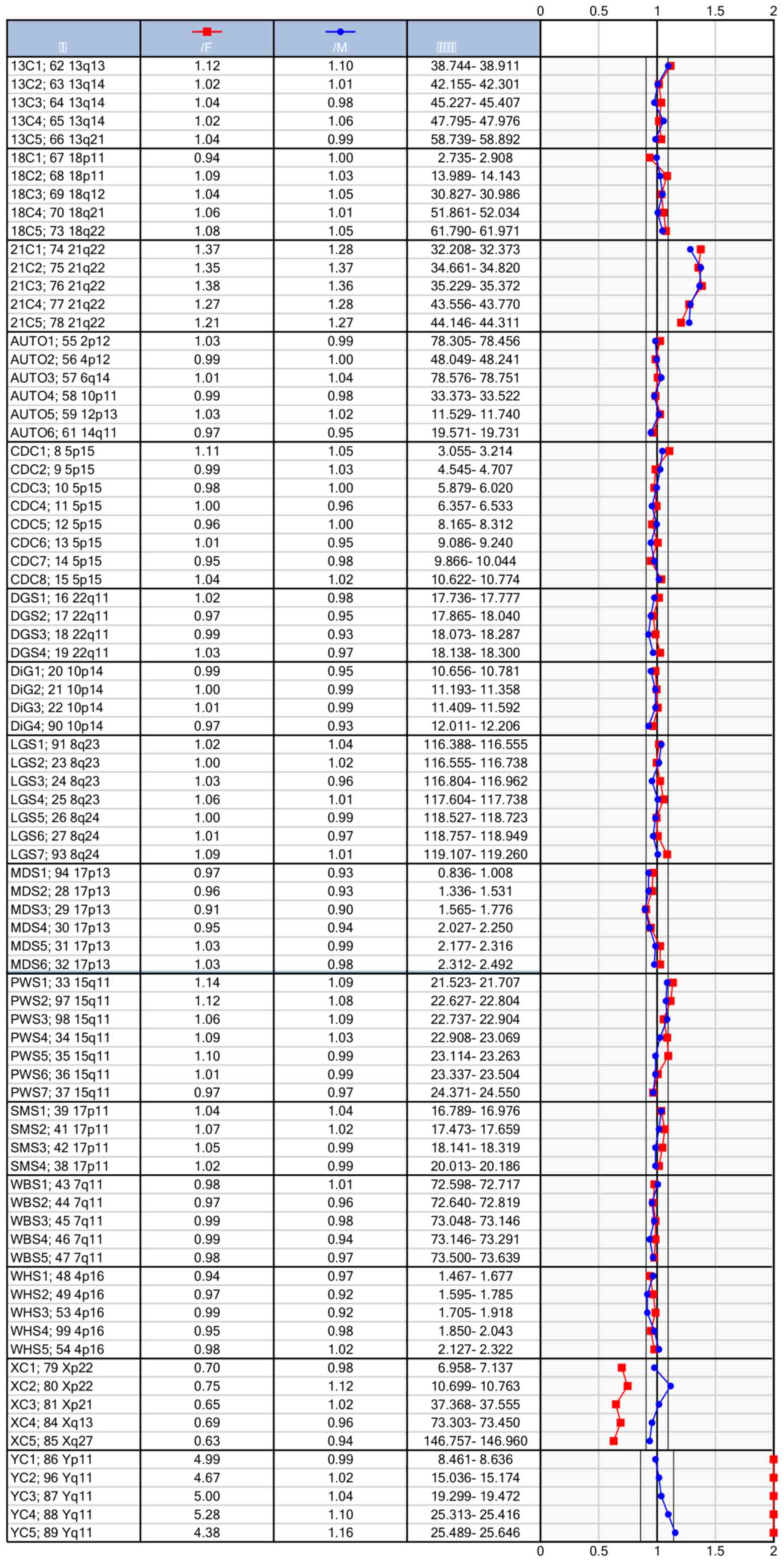
Abnormal findings with BoBs assay
Targets selection is highly specific. Menu-based
detection can quickly detect 21-trisomy aneuploidy, which can
compensate the limitations of karyotype analysis. Fig. 3 shows the detection results of BoBs
for prenatal 21-trisomy.
Discussion
China currently has a population of 1.4 billion, and
is the first most populous country in the world. Not only is the
birth rate the highest in the world, but the total number of birth
defects also rank first in the world (9). Previous studies have confirmed that
trisomy 21 is the most common type of neonatal birth defects,
followed by trisomy 18, trisomy 13, and aneuploidy of sex
chromosomes X and Y (10). The
present strategy of managing birth defects due to chromosomal
abnormalities is implementation of secondary prevention, i.e.,
intervention through prenatal screening and diagnosis (11). Karyotype analysis following
amniocentesis was the gold standard of prenatal diagnosis in
previous studies (12), which was
highly sensitive and specific, and had an almost 100% prenatal
diagnostic rate for fetal chromosomal abnormalities. However, the
technology requires a longer period of time to obtain results and
has low resolution, thus only detection of larger mutations is
allowed. Moreover, karyotype analysis requires high skill level to
process the chromosome samples, and results were interpreted with
high subjectivity and in the case of an unsuccessful amniotic fluid
cell culture, the whole experiment is in vain (13,14).
Prenatal BoBs technology is a cytogenetic assay for
rapid prenatal diagnosis. Results obtained from the chromosome
analysis are characteristic for both normal male and normal female.
In this assay, a small amount of DNA sample was required to perform
analysis of multiple chromosomes and find abnormalities. Trisomy 21
served as an example of an abnormal result. In addition, BoBs assay
takes less time to obtain results than traditional karyotype
analysis. In a typical assay, the results can be obtained within 24
h, which greatly reduces anxiety and relieves psychological stress
in high-risk pregnant women. Except for fast results, this
technology also enables high throughput by analysis of more than 92
samples at the same time (15).
Through molecular karyotyping, genomic DNA in identified target
region is amplified, and target deletion is detected (16). In addition to detecting aneuploidy of
chromosomes 13, 18, 21, and sex chromosomes X and Y (17), BoBs technology enables aberration
detection in 9 additional meticulously chosen microdeletion regions
(18). Thereby diagnostic accuracy
can be improved, and shortcomings in abnormal cell culture for
karyotype analysis can be offset to some extent (19,20).
In this study, in order to explore the clinical
application of BoBs assay combined with karyotype analysis, results
obtained by BoBs assay were compared with results obtained by
traditional karyotype analysis of the same enrolled pregnant women.
The two testing methods yielded exactly the same diagnostic
outcomes in the detection of trisomy 21, trisomy 18, trisomy 13,
and sex chromosomal abnormalities. Balanced chromosome
translocation was detected only by karyotype analysis (control
group), whereas chromosome microdeletion was detected only by BoBs
assay (observation group). Thus, the two testing methods were
complementary to each other.
In conclusion, karyotype analysis combined with BoBs
technology for prenatal diagnosis was easy to perform, and provided
quick results with high accuracy. Combined use of the two testing
methods significantly improved the diagnostic rate of chromosomal
abnormalities thus reducing birth defects and guiding continued
pregnancy of high-risk pregnant women.
Acknowledgements
Not applicable.
Funding
This study was funded by The First Batch of Training
Project for reserve medical youth in Xuzhou (no. 2014011).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
YF and GW contributed significantly to writing the
manuscript and conducted amniocentesis. LG helped with karyotype
analysis of chromosomes. JW and FS performed BoBs assay. MG and LG
interpreted statistical analysis. All authors read and approved the
final study.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Xuzhou Maternity and Child Health Care Hospital.
Signed informed consents were obtained from the patients or the
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bianca I, Geraci G, Gulizia MM, Assenza
Egidy G, Barone C, Campisi M, Alaimo A, Adorisio R, Comoglio F,
Favilli S, et al: Consensus Document of the Italian Association of
Hospital Cardiologists (ANMCO), Italian Society of Pediatric
Cardiology (SICP), and Italian Society of Gynaecologists and
Obstetrics (SIGO): Pregnancy and congenital heart diseases. Eur
Heart J Suppl. 19 Suppl D:D256–292. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pandya VK and Sutariya HC: Unilateral
multicystic renal dysplasia: Prenatal diagnosis on ultrasound.
Saudi J Kidney Dis Transpl. 28:916–920. 2017.PubMed/NCBI
|
|
3
|
Choy KW, Kwok YK, Cheng YK, Wong KM, Wong
HK, Leung KO, Suen KW, Adler K, Wang CC, Lau TK, et al: Diagnostic
accuracy of the BACs-on-Beads™ assay versus karyotyping for
prenatal detection of chromosomal abnormalities: A retrospective
consecutive case series. BJOG. 121:1245–1252. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Grati FR, Gomes Molina D, Ferreira JC,
Dupont C, Alesi V, Gouas L, Horelli-Kuitunen N, Choy KW,
García-Herrero S, de la Vega AG, et al: Prevalence of recurrent
pathogenic microdeletions and microduplications in over 9500
pregnancies. Prenat Diagn. 35:801–809. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Marcato L, Turolla L, Pompilii E, Dupont
C, Gruchy N, De Toffol S, Bracalente G, Bacrot S, Troilo E, Tabet
AC, et al: Prenatal phenotype of Williams-Beuren syndrome and of
the reciprocal duplication syndrome. Clin Case Rep. 2:25–32. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rosenfeld JA, Morton SA, Hummel C,
Sulpizio SG, McDaniel LD, Schultz RA, Torchia BS, Ravnan JB,
Ellison JW and Fisher AJ: Experience using a rapid assay for
aneuploidy and microdeletion/microduplication detection in over
2,900 prenatal specimens. Fetal Diagn Ther. 36:231–241. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mei J, Wang H and Zhan L: 10p15.3p13
duplication inherited from paternal balance translocation
(46,XY,t(5;10)(q35.1;p13)) identified on non-invasive prenatal
testing. J Obstet Gynaecol Res. 43:1076–1079. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
García-Herrero S, Campos-Galindo I,
Martínez-Conejero JA, Serra V, Olmo I, Lara C, Simón C and Rubio C:
BACs-on-Beads technology: A reliable test for rapid detection of
aneuploidies and microdeletions in prenatal diagnosis. BioMed Res
Int. 2014:5902982014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Choy RK, Chen Y, Sun XF, Kwok YK and Leung
TY: BACs-on-beads: A new robust and rapid detection method for
prenatal diagnosis. Expert Rev Mol Diagn. 14:273–280. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Piotrowski K, Halec W, Wegrzynowski J,
Pietrzyk A, Henkelman M and Zajaczek S: Prenatal diagnosis of
Langer-Giedion Syndrome confirmed by BACs-on-Beads technique.
Ginekol Pol. 85:66–69. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ragni MV: Prenatal diagnosis by droplet
digital PCR. Blood. 130:240–241. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Łaczmańska I and Stembalska A: New
molecular methods in prenatal invasive diagnostics. Ginekol Pol.
84:871–876. 2013.(In Polish). View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Baxter L and Adayapalam N: A comparative
study of standard cytogenetic evaluation and molecular karyotyping
for products of conception. Diagn Mol Pathol. 22:228–235. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kiiski K, Roovere T, Zordania R, von
Koskull H and Horelli-Kuitunen N: Prenatal diagnosis of
17p13.1p13.3 duplication. Case Rep Med. 2012:8405382012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Piotrowski K, Henkelman M and Zajaczek S:
Will the new molecular karyotyping BACs-on-Beads technique replace
the traditional cytogenetic prenatal diagnostics? Preliminary
reports. Ginekol Pol. 83:284–290. 2012.(In Polish). PubMed/NCBI
|
|
16
|
Vialard F, Simoni G, Gomes DM, Abourra A,
De Toffol S, Bru F, Romero Martinez MC, Nitsch L, Bouhanna P,
Marcato L, et al: Prenatal BACs-on-Beads™: The prospective
experience of five prenatal diagnosis laboratories. Prenat Diagn.
32:329–335. 2012. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Popowski T, Vialard F, Leroy B, Bault JP
and Molina-Gomes D: Williams-Beuren syndrome: The prenatal
phenotype. Am J Obstet Gynecol. 205:e6–e8. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shaffer LG, Coppinger J, Morton SA,
Alliman S, Burleson J, Traylor R, Walker C, Byerly S, Lamb AN,
Schultz R, et al: The development of a rapid assay for prenatal
testing of common aneuploidies and microdeletion syndromes. Prenat
Diagn. 31:778–787. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fox KA and Lee W: Prenatal diagnosis and
evaluation of abnormal placentation. Clin Obstet Gynecol.
60:596–607. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Salvador Llorens R, Sainz Viegas A,
Filardi Montoya A, Fornas Montoliu G and Serrano Menor F:
Evaluation of the fetal cerebellum by magnetic resonance imaging.
Radiologia. 59:380–390. 2017.(In English, and Spanish). PubMed/NCBI
|