Introduction
Upper ureteral calculi are a common ailment
encountered at urology departments, and they have a long embedding
time and easily induce secondary conditions, including oedema in
the ureteric wall, chronic inflammatory diseases and inflammatory
polyps (1). These diseases develop
and involve the tissues around the ureter, resulting in serious
ureteral obstruction (1).
Surgery is the most efficient treatment for upper
ureteral calculi (2). However, in
specific cases, the embedded stones have large volumes and adhere
to the ureteric wall, thus increasing the difficulty of the
operation for upper ureteral calculi and resulting in limitations
(2). Furthermore, the therapeutic
methods for upper ureteral calculi are complicated as the
ureteroscope, soft lenses and percutaneous nephrolithotripsy (PCN)
have advantages and disadvantages (2). Upper segment stones are easily washed
into the pelvis during ureteroscopy, increasing the surgical
difficulty of this procedure. The soft lens can be utilized to
treat upper ureteral calculi; however, due to its fragile nature,
it is easily damaged and therefore often associated with increased
surgical costs. PCN exhibits high lithotripsy efficiency coupled
with various risk factors. Rigid ureteroscopy exhibited poor
outcomes for the treatment of upper ureteral calculi. Due to the
stone obstructing the ureteral cavity, drainage of the fluids used
for flushing is hindered and a larger pressure is required for the
process, which has the potential of moving the stone into the wrong
direction (3,4). PCN suggested better curative effects
with 90.09% success rate of lithotripsy (5), but causes a larger surgical wound and
bears risks of hemorrhoea, hemopneumothorax, sepsis and peripheral
tissue injury during or following surgery. Soft ureteroscopy
treatment has improved safety and effects to the upper ureteral
calculi, but requires highly trained surgeons to treat ureteral
incarcerated stones. Complications, including bleeding, may occur
during surgery by damaging the ureteral wall. A combination of hard
and soft lens may combine advantages to reduce surgical
complications and significantly improve the surgical
efficiency.
In the present study, ureteroscope lithotripsy
assisted by a guide sheath was used to treat upper ureteral calculi
in order to improve the vision, to increase the efficiency of
lithotripsy and to decrease the difficulty of the operation and the
occurrence of complications.
Patients and methods
Patients
A total of 81 patients with upper ureteral calculi
who were treated at Ningbo First Hospital (Ningbo, China) between
January 2012 and June 2014 were included in the present
observational study. The data collected included patient age, sex
and body mass index as well as medical history, including diabetes
mellitus, vascular disease and pelvic radiation. Patients with
pelvic radiation history were excluded. The cohort was comprised of
57 males and 24 females aged 25–71 years, with an average age of
43.4±12.9 years.
The inclusion criteria were as follows: i) The
embedding time in the same region was >2 months (6); ii) the calculi caused serious kidney
hydronephrosis, which was confirmed according to the standard
clinical criteria (7); and iii)
extracorporeal shock wave lithotripsy (ESWL) therapy failed. The
exclusion criteria were as follows: Patients who had undergone
local radiotherapy or who had a history of retroperitoneal surgery,
which may lead to ureterostenosis. Overall, 46 patients had left
ureteral calculi, while 35 patients had right ureteral calculi,
which is presented in Table I. The
diameters of the stones were 7–25 mm. Stones from 57 patients were
≥1.5 cm in diameter, while 24 patients had stones <1.5 cm.
 | Table I.Clinical data for all patients (n=81)
and safety and outcome measures. |
Table I.
Clinical data for all patients (n=81)
and safety and outcome measures.
| Parameter | Value |
|---|
| Sex |
|
| Male | 57 (70.4%) |
|
Female | 24 (29.3%) |
| Age (years) | 43.4±12.9
(25–71) |
| Body mass index
mg/m2 | 21.0±2.0 |
| Diabetes | 7 (8.6%) |
| Hypertension | 9 (11.1%) |
| Pelvic radiation
(Gy) | 30±5 |
| Left ureteral
calculi | 46 |
| Right ureteral
calculi | 35 |
| Diameter of calculi
(mm) | 7–25 |
| Mode of surgery |
|
| Simply
rigid ureteroscope lithotripsy assisted with ureteral access
sheath | 63a |
| Rigid and
flexible ureteroscope lithotripsy assisted with guide sheath | 18 |
| Operation time
(min) | 56.0±4.8
(30–115) |
| Complications |
|
|
Post-operative fever
37.4–39.1°C (mean, 37.7±0.3°C) | 7 |
| Ureteral
perforation | 0 |
|
Conversion to PCNL or open
surgery | 0 |
|
Peripheral organ injury | 0 |
| Ureteral
avulsion | 0 |
| Residual stone
diameter in the renal pelvis after surgery |
|
| <2
mm | 69b |
| 2-4
mm | 12 |
| Stone-free rate at 1
month after surgery | 81 (100%) |
Treatments
All procedures were performed with the patient under
general intravertebral anesthesia in a standard lithotomy position.
A rigid ureteroscope (hard lens type, F8/8.9; Richard Wolf GmbH,
Knittlingen, Germany) was inserted into the ureter by using a Zebra
urological guide-wire (Zibo Qianyan Medical Instrument Co., Ltd.,
Zibo, China). The ureteroscope and the guide-wire were placed at
the lower end of the stones. The rigid ureteroscope was placed
outside and the guide sheath (type, F12/14; length, 35 cm) (Cook
Medical, Bloomington, IN, USA) was placed along the guide-wire.
According to body surface measurement and judgment
of the distance between the stones and the ureter, the guide sheath
was placed to avoid one step. The length of the sheath placed into
the ureter was adjusted according to the method described in a
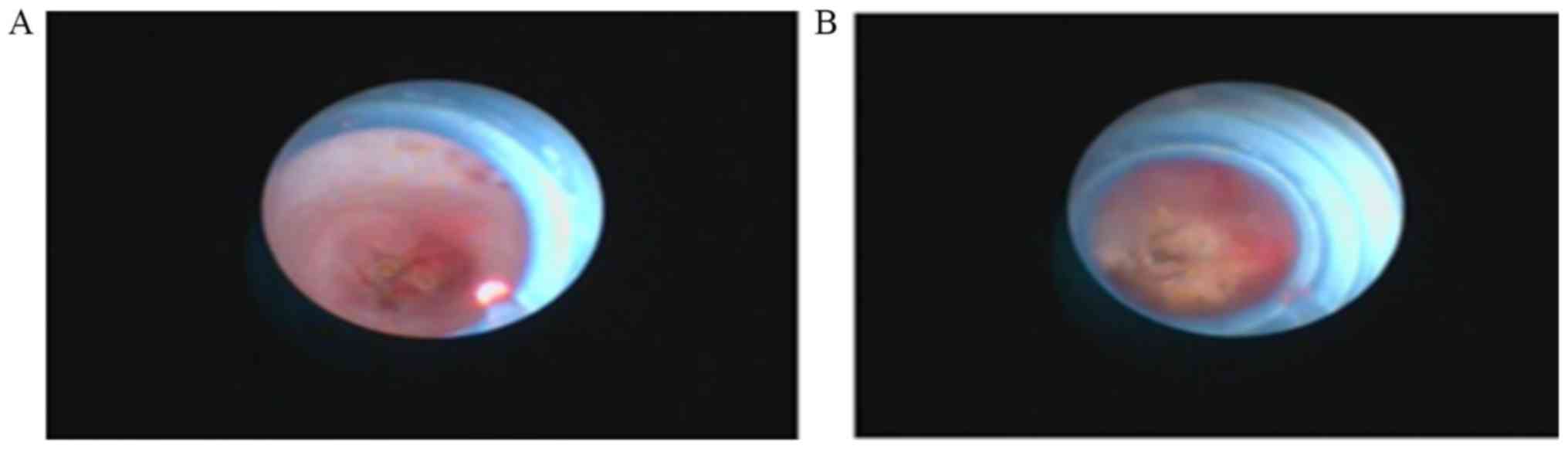
previous study (8). When the sheath
was in direct proximity to the stones, the inner core was removed,
and the small ureteroscope (Richard Wolf GmbH, Knittlingen,
Germany) was placed (hard lens type, F/6.5/7; Fig. 1)
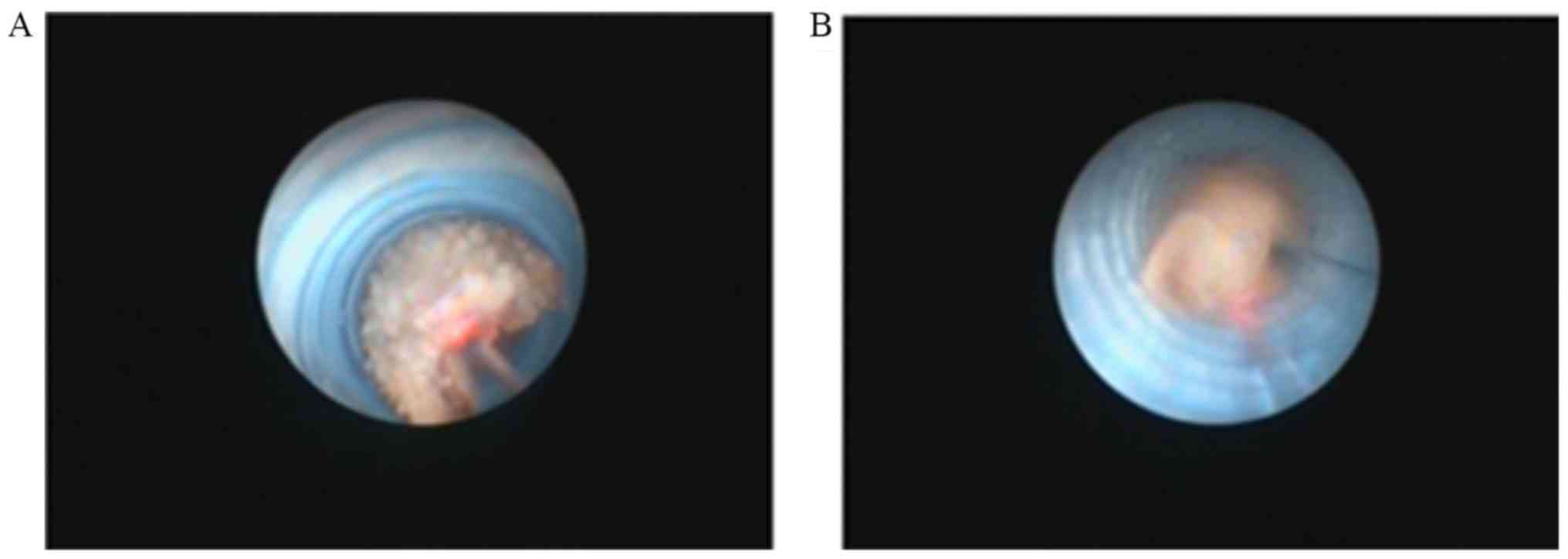
The placement of the guide sheath and the condition
of the upper ureter were observed along the guide sheath. The guide
sheath was placed close to the lower part of the stones.
Subsequently, holmium laser lithotripsy was performed (Fig. 2).
During the holmium laser lithotripsy, the placements
and methods were determined according to methods described in a
previous study (9). Gradual
lithotripsy was performed with high frequency and low power (20 W,
1.0 J × 20 Hz). The frequency and power were adjusted according to
stone hardness. For larger stones refluxing to the renal pelvis, a
soft ureteroscope was used with methods similar to those for the
rigid ureteroscope. During lithotripsy, part of the stone was
treated using an ureteroscopic basket. The soft ureteroscope was
used with a distorted or thin ureter. The stones were directly
fragmented by lithotripsy. Double J-tube stenting was performed
subsequent to surgery. Ultrasound examination of kidneys, ureters
and bladder (KUB) or urinary system computed tomography (CT) was
re-performed after one month in order to confirm the absence of any
residual stones and to withdraw the D-J tube. All patients were
followed up for 3–12 months.
Statistical analysis
All data are expressed as the mean ± standard
deviation. Statistical analysis was performed with SPSS 20.0
software (IBM Corp., Armonk, NY, USA) and Student's t-test was used
to compare the proportion of patients treated by simple rigid
ureteroscope lithotripsy assisted with ureteral access sheath and
those treated with rigid and flexible ureteroscope lithotripsy
assisted with guide sheath.
Results
Surgery effects
A total of 63 patients were successfully treated
with rigid ureteroscope lithotripsy assisted by a ureteral access
sheath, while 18 patients were successfully treated with rigid and
flexible ureteroscope lithotripsy assisted by a guide sheath
(Table I).
A number of broken stones were washed out the
ureteral dilated sheath (Fig. 3).
The majority of patients 77.8% (63/81) with incarcerated calculi of
the upper ureter were treated with hard lens accompanied with
ureteral dilated sheath. If treatment by hard lens only was not
advisable, it was combined with the soft lens to improve the
surgical success rate. During surgery, changing the flushing
pressure aided removing partial stones from the ureteral dilated
sheath and furthered the overall decrease of stones.
At 1 day after surgery, KUB and urinary system CT
scans were performed. The D-J tubes were well-placed in all cases.
A total of 69 patients had residual calculi in the renal pelvis
that were <2 mm, while the residual calculi were 2–4 mm in 12
patients. In all of the patients, the calculi were completely
discharged after 1 month, with a stone clearance rate of 100%
(Table I). Patients exhibited a
better response to lithotripsy and shattered residual stones (<4
mm) were discharged following surgery.
Complications
The proportion of patients treated by simple rigid
ureteroscope lithotripsy assisted with ureteral access sheath
(63/81) was significantly higher than that of patients treated by
rigid and flexible ureteroscope lithotripsy assisted with a guide
sheath (18/81; P<0.01). The operation time ranged between 30 and
115 min (average, 56±4.8 min; Table
I). A total of 7 patients had an elevated body temperature
37.4–39.1°C (mean temperature, 37.7±0.3°C) after surgery (Table I), which may indicate poor infection
control prior to surgery, but no other complications were
encountered. During or after surgery, no obvious bleeding occurred,
conversion to percutaneous nephrolithotomy (PCNL) or open surgery
was not required in any of the cases and no inter-operative
complications, including urethral perforation or visceral injury,
occurred. The 7 patients who developed an elevated temperature
after the operation were treated by anti-infective therapy and they
recovered without any other complications. All patients were
followed up for 3–12 months and no associated complications,
including ureterostenosis or atresia of the ureter, occurred
(Table I).
Discussion
Due to the long course of embedding and the
irritation by the upper ureteral calculi, a series of immune
reactions in the body may easily lead to inflammatory polyps or
stricture in the ureter around the stones (10). Surgery is the major therapy for upper
ureteral calculi, with techniques including rigid ureteroscope
lithotripsy, open surgery under retroperitoneal laparoscopy and
soft ureteroscope lithotripsy.
Rigid ureteroscope lithotripsy used on upper
ureteral calculi may lead to complications, including stones
blocking the ureter, non-smooth drainage of flushing liquid
requiring enhanced power and stones moving up, and its application
is limited (3,4). Multiple turnovers are required to
withdraw stones, which is associated with a risk of serious
complications, including mucous membrane injury and avulsion
(11,12). Post-processing of the retained renal
calculi is also challenging (13).
Gdor et al (14) reported a
success rate of endoscopic treatment of upper ureteral calculi of
only 56%. The minimally invasive nephroscope treatment had a higher
efficiency for upper ureteral calculi, with a success rate of 90.9%
(5). However, injury to kidney
tissue resulted in larger trauma and even serious injury, including
bleeding, hemopneumothorax, hematosepsis and tissue injury. Lin
et al (15) analyzed 528
patients who received PCNL treatment for upper ureteral calculi, of
which 17 patients experienced bleeding during surgery, 2 patients
had pleural effusion, 1 patient had colon perforation, 8 patients
had an elevated temperature and 3 patients had seroperitoneum. The
rate of complications was 5.8%. During open surgery with
retroperitoneal laparoscopy, the stones were completely withdrawn,
but retroperitoneal laparoscopic surgery is performed in a narrow
space and the incidence of complications, including urinous
infiltration and ureterostenosis. Due to the surgical incision into
the ureteral cavity, there was a risk of urine leakage.
Compared with the hard lens, the soft ureteroscope
has a better safety and efficiency in treating upper ureteral
calculi. As the calculi was located in the ureter and the soft lens
allowed surgery in narrow space, a more advanced technique was
required. The use of soft lenses usually causes inflammatory polyps
and poses a limitation during the operation. It easily causes
bleeding and ureteral wall injury, leading to fail of
operation.
In the present study, ureteroscope lithotripsy
assisted by a guide sheath was used for treating upper ureteral
calculi. During the surgery, injection and refluxing of liquid was
facilitated due to improved vision. For the placement of the guide
sheath, a larger space between the ureteroscope and the guide
sheath was available, which was beneficial for the flow of the
flushing liquid. Auge et al (16) reported that the guide sheath in the
ureter was helpful for reducing the pressure in the renal pelvis by
57–75%, as well as decreasing stone refluxing. The assistance of
the ureteric guide sheath had certain advantages leading to an
improved success rate and efficiency of the operation. According to
Breda et al (17), the
ureteral access sheath is highly recommended for the treatment of
upper urinary tract disease by means of retrograde intrarenal
surgery, during which the lower part of the calculus usually causes
distortion or partial stricture, resulting in difficulty in using
the rigid ureteroscope. In the present study, the placement of the
guide sheath straightened the ureteral lumen to a certain extent,
which was convenient during surgery, as the ureteral sheath tightly
connected to ureteral wall and stretching of the sheath aided to
straighten the ureteral cavity during surgery.
The increasing pressure of the flushing liquid
facilitated the passing of the ureteroscope. It was possible to
remove most of the stones by expanding the sheath from the PCN.
This method increased the efficiency of lithotripsy and withdrawal
of the stones. The ureteroscopic basket was also convenient,
eliminating the requirement for open surgery and avoiding multiple
turnovers, which reduced injury to the ureteral lumen and
mucosa.
The guide sheath was safe and efficient, but
problems still existed with the calculi or remnants refluxing to
the renal pelvis (18). Particularly
during or at the end of the lithotripsy, the lumen was gradually
opened as the distal calculi broke. The fluxing liquid caused a
high pressure, and parts of the stones were easily refluxed to the
renal pelvis, which required a change to the soft ureteroscope. Due
to the low capacity of the calculi to reflux to the renal pelvis,
the use of a basket is suggested for withdrawing the stones. For
removing the residual stones, it was attempted to fragment them
into particles of <2 mm in size (9).
With the assistance of a guide sheath, a change to
the soft ureteroscope was also require for patients with distorted
or structured ureters and difficulty in passing. The soft
ureteroscope had a thinner tube than the ureter and a more flexible
head-end, which was helpful for passing through the distorted or
restricted ureters. Lithotripsy with a soft ureteroscope was
performed on calculi. Polyps occurred, usually in the narrow space.
By applying a skilled technique, bleeding and injury of the
ureteral lumen were avoided, after soft ureteroscopy, a change from
the soft to the rigid ureteroscope was required. In addition, the
soft ureteroscope expanded the lumen, which resulted in
straightening of the restricted ureter by flushing liquid with
increasing power after clearing the polyps and stones.
Subsequently, the thin ureteroscope was successfully passed through
the ureter. Rigid ureteroscope lithotripsy was efficient in surgery
assisted by a guide sheath.
In conclusion, ureteroscope lithotripsy was
successful with a rigid or soft ureteroscope assisted by a guide
sheath for upper ureteral calculi. The technique is helpful for the
surgery due to factors including the abundant refluxing of liquid,
enhancing the vision, decreasing pressure in the renal pelvis,
increasing the efficiency of withdrawing stones and reducing
refluxing of stones in the renal pelvis. Due to further advantages,
including the protection of the ureteral lumen and decreased
complications during or after surgery, particularly for larger
stones in the upper ureter, it is suggested that guide
sheath-assisted rigid ureteroscope lithotripsy is an efficient
treatment for upper ureteral calculi. However, further studies
using larger samples are required to confirm these results.
Acknowledgements
Not applicable.
Funding
No funding received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
J-SH performed the surgical procedures. G-HX and
H-SY collected the images. G-LL, X-LJ and ZZ collected and analyzed
data. YC analyzed the data and supervised this study. All authors
read and approved the final version of the manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from all
patients and the present study was approved by the Ethics Committee
of Ningbo First Hospital.
Patient consent for publication
Written informed consent was obtained from all
patients.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Mugiya S, Ito T, Maruyama S, Hadano S and
Nagae H: Endoscopic features of impacted ureteral stones. J Urol.
171:89–91. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Manohar T, Ganpule A and Desai M:
Comparative evaluation of Swiss LithoClast 2 versus Holmum: YAG
laser lithotripsy for impacted upper-ureteral stones. J Endourol.
22:443–446. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ma L, Yu DM, Zhang ZG, Li GH, Ding GQ,
Chen YB, Xu LW, Wu HY and Cai XJ: Transperitoneal laparoscopic
ureterolithotomy for upper ureteral calculi: A report of 1171
cases. Zhonghua Yi Xue Za Zhi. 93:1577–1579. 2013.(In Chinese).
PubMed/NCBI
|
|
4
|
Martov AG, Teodorovich OV, Galliamov EA,
Lutsevich OÉ, Zabrodina NB, Gordienko AIu and Parkhonin DI:
Endoscopic ureterolithotomy in large concrements of the upper third
of the ureter. Urologiia. 5:50–55. 2011.(In Russian).
|
|
5
|
Cengiz K, Berkan R, Mirze B and Ünsal A:
Efficacy of a percutaneous antegrade approach for the treatment of
large upper ureteral stonse: Single-center experience. Turkish J
Urol. 37:210–216. 2011. View Article : Google Scholar
|
|
6
|
Roberts WW, Cadeddu JA, Micali S, Kavoussi
LR and Moore RG: Ureteral stricture formation after removal of
impacted calculi. J Urol. 159:723–726. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Morgentaler A, Bridge SS and Dretler SP:
Management of the impacted ureteral calculus. J Urol. 143:263–266.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cheng Y and Liu GL: The flexible
ureteroscope treatment of urinary tract calculi surgical skills to
share. Xiandaiminiaowaikezazhi. 19:281–284. 2014.(In Chinese).
|
|
9
|
Cheng Y, Yan ZJ, Xie GH, Yuan HS and Liu
G: Powdered gravel Application of flexible ureteroscope in the
treatment of kidney stones. Weichuangweikeminiaozazhi. 2:210–212.
2013.(In Chinese).
|
|
10
|
Zhong W, Zeng G, Wu W, Chen W and Wu K:
Minimally invasive percutaneous nephrolithotomy with multiple mini
tracts in a single session in treating staghorn calculi. Urol Res.
39:117–122. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Alapont JM, Broseta E, Oliver F, Pontones
JL, Boronat F and Jiménez-Cruz JF: Ureteral avulsion as a
complication of ureteroscopy. Int Braz J Urol. 29:18–23. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jiang YM, Li JM, Xu HY, Liu JH, Yan YJ,
Zhang JS, Chen J and Jia WJ: Ureteral avulsion long segment.
Zhonghuaminiaowaikezazhi. 29:408–410. 2008.
|
|
13
|
Dong ZQ, Li KJ, Xu XM, Zhang P, Zhang LS
and Mao Z: Different ways to comparative efficacy of lithotripsy
treatment of ureteral calculi incarcerated on segment.
Zhongguoneijingzazhi. 13:163–165. 2007.
|
|
14
|
Gdor Y, Gabr AH, Faerber GJ, Roberts WW
and Wolf JS Jr: Success of endoureterotomy of ureteral strictures
associated with ureteral stones is related to stone impaction. J
Endourol. 22:2507–2511. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lin W, Li Y, Huang HP, Meng DL, Wang JG
and He JQ: Comparison of two minimally invasive methods of
treatment failure after treatment of upper ureteral calculi ESWL.
Shiyongyixuelinchuang. 10:49–53. 2009.(In Chinese).
|
|
16
|
Auge BK, Pietrow PK, Lallas CD, Raj GV,
Santa-Cruz RW and Preminger GM: Ureteral access sheath provides
protection against elevated renal pressures during routine flexible
ureteroseopic stone manipulation. J Endourol. 18:33–36. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Breda A, Territo A and Lópezmartínez JM:
Benefits and risks of ureteral access sheaths for retrograde renal
access. Curr Opin Urol. 26:70–75. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liu DY, He HC, Wang J, Tang Q, Zhou YF,
Wang MW, Chu CL, Zhang CY, Zhu Y, Zhou WL and Shen ZJ:
Ureteroseopic lithotripsy using holmium laser for 1 87 patients
with proximal ureteral stones. Chin Med J (Eng1). 125:1542–1546.
2012.
|