Introduction
Skin is the largest organ in the human body, as well
as an important tissue covering the body surface and protecting the
internal organs. Inflammation, trauma, ulcers, and resection of
large tumor on the body surface often lead to huge skin defects
that are difficult to repair by themselves. The traditional repair
method of large-area skin defects is autologous skin grafting;
however, the autologous skin source of patients is often
inadequate, there will be new incisions and scars will be left in
the operative area, thus limiting its wide application in clinical
practice. The construction and clinical application of
tissue-engineered skin provide a new way and method for the repair
of large-area skin defects. The seed cell and scaffold material are
major factors in tissue engineering technique (1), the latter of which, as the transport
carrier of seed cells, carries sufficient number of seed cells
required for wound repair, ensuring the effective concentration of
stem cells in wound repair process. A variety of scaffold materials
have been widely used clinically, but no ideal scaffold materials
have obtained satisfactory basic or clinical experimental results
so far. At present, scaffold materials generally have such problems
as low porosity, small cavity diameter, poor mechanical strength,
high immunogenicity and too early degradation time or no
degradation (2); therefore, many
scholars have been exploring an ideal scaffold material that is
safe, non-toxic, low in immunogenicity, moderate in degradation
time, low in price and convenient in application (3,4) for a
long time. The new collagen sponge scaffold (NCSS) was successfully
prepared via experimental research, and it was confirmed that NCSS
had no obvious cytotoxicity, but a larger pore size and higher
porosity, so it was suitable for cell adhesion and growth.
In this study, we tried to construct the
tissue-engineered skin substitute using adipose-derived stem cells
(ADSCs) combined with NCSS to repair the full-thickness skin
defects in nude mice, and observe the effect of ADSCs-NCSS in wound
repair.
Materials and methods
Materials
Main reagents
Low-glucose Dulbecco's modified Eagle's medium
(DMEM-L) (Gibco; Thermo Fisher Scientific, Inc., Waltham, MA, USA);
fetal bovine serum (FBS; Gibco, Melbourne, Australia); type I
collagenase (Sigma-Aldirch; Merck KGaA, Darmstadt, Germany).
A total of 24 specific pathogen-free (SPF) nude mice
(BALB/c-nunu type) with simple T cell deficiency, aged 3–5 weeks
and weighing 18.2–21.1 g, were purchased from Laboratory Animal
Center of Xuzhou Medical College (Xuzhou, China) and Shanghai SLAC
Laboratory Animal Co., Ltd. (Shanghai, China) and qualified in
animal quarantine.
Skin and adipose sources
Specimens were taken from surgical patients in the
Department of Plastic Surgery and Thyroid and Breast Surgery of the
Affiliated Hospital of Xuzhou Medical University. Patients aged
23–45 years signed the informed consent, those with infectious or
skin lesions were excluded, and this study was approved by the
Ethics Committee of the Drum Tower Clinical College of Nanjing
Medical University (Nanjing, China).
Methods
Separation, acquisition and culture of
human ADSCs
Human ADSCs were extracted according to the study of
Zuk et al (5) and previous
research (6,7): Under aseptic conditions, adipose
tissues were taken, repeatedly washed with phosphate-buffered
saline (PBS) containing the double antibody, cut into 1
mm3 pieces, followed by centrifugation at 960 × g at 4°C
in a 50 ml centrifuge tube for 5 min twice. The upper-layer adipose
tissues were retained, and incubated with 0.01% type I collagenase
on a shaker at 37°C for 60 min, followed by centrifugation at 2,010
× g at 4°C for 10 min. The sediment was retained, resuspended using
the double antibody-contained medium, and repeatedly filtered
through a 200-mesh sieve, followed by centrifugation at 1,050 × g
at 4°C for 5 min. After the supernatant was discarded, cells were
resuspended using the medium, and inoculated into a 25
cm2 perforated culture flask in an incubator with 5%
CO2 at 37°C; after 48 h, the solution was replaced. When
80% cells were fused, they were digested using 0.25% trypsin,
followed by passage as the P1 generation. P3-P5-generation ADSCs
were used for experiments.
Preparation of two kinds of dermal
scaffolds
Preparation of acellular dermal matrix
(ADM)
ADM was prepared using the traditional method
(6,7). Under aseptic conditions, the
subcutaneous adipose tissues were cut off, placed into 1 mol/l NaCl
solution for thermostatic water bath at 37°C for 24 h, repeatedly
washed with PBS to remove the epidermal cells, placed into 2% NaOH
solution for thermostatic water bath at 37°C for 16 h, and washed
again with PBS repeatedly until the solution became neutral. Then
tissues were placed at −80°C for 4 h, thawed in a thermostatic
water bath box at 37°C for 4 h; the freezing-thawing process was
repeated 4 times. Finally, tissues were washed with PBS repeatedly,
and stored at 4°C for standby application after frozen drying.
Preparation of NCSS
Under aseptic conditions, the subcutaneous adipose
tissues were cut off, placed into 1 mol/l NaCl solution for
thermostatic water bath at 37°C for 24 h, repeatedly washed with
PBS to remove the epidermal cells, treated with 2% NaOH solution on
a shaker at 45°C for 4 h, and washed again with PBS repeatedly
until the solution became neutral. Then tissues were placed at
−80°C for 4 h, thawed in a thermostatic water bath box at 37°C for
4 h; the freezing-thawing process was repeated for 4 times.
Finally, tissues were washed with PBS repeatedly, and stored at 4°C
for standby application after frozen drying.
ADM and NCSS were hematoxylin and eosin (H&E)
stained and observed under a scanning electron microscope
(SEM).
Construction and cytocompatibility of
tissue-engineered skin
P3-generation ADSCs were inoculated into a 24-well
plate (2×105/well), placed on NCSS soaked in complete
medium in advance for 48 h, and incubated under saturated humidity
with 5% CO2 at 37°C for 3 and 7 days, followed by
fixation via formalin and H&E staining.
Wound model establishment and grouping
of nude mice
After 24 nude mice were weighed and anesthetized
intraperitoneally with 10% chloral hydrate (300 mg/kg), two 10
mm2 round full-thickness skin defects were designed on
both sides of the back reaching the subcutaneous fascia; the defect
borders were fixed with 6-0 suture. Mice were randomly divided into
4 groups: ADSCs-NCSS (group A, cultured for 7 days), simple NCSS
(group B), simple ADSCs (group C) and blank control (group D,
simply covered with oil gauze). After operation, all wounds were
treated with pressure dressing, and mice were fed in separate
cages.
Specimen collection and detection
At 3, 7, 10 and 14 days, the wounds were opened,
photographed and re-bandaged, and the wound healing rate was
calculated (Image-Pro Plus software; Media Cybernetics, Inc.,
Rockville, MD, USA). At 7 and 14 days after operation, 12 nude mice
were sacrificed by cervical dislocation, and the skin tissues were
cut at 2 mm outside the normal skin along the wound margin reaching
the muscular layer. After fixation via formalin, embedding and
sectioning, skin tissues received H&E and immunohistochemical
assay to detect the regenerated tissue thickness and vascular
density (Image-Pro Plus software). Wound healing rate = (original
wound area - residual wound area)/original wound area × 100%.
Regenerated tissue thickness: H&E-stained sections were taken
to detect the regenerated tissue thickness in each group under a
microscope (×200), excluding the regenerated epidermal cells; five
points were selected from each section at the same interval of
distance for measurement. Vascular density detection:
Immunohistochemical sections were taken to count the cluster of
differentiation 31 (CD31)-positive blood vessels under a microscope
(×200). Deep brown-stained cells, instead of the formation of lumen
or the presence or absence of red blood cells in the lumen, could
be regarded as one counting unit. Four different fields of view
were selected from each section to calculate the average number of
blood vessels per unit field of view, namely the interstitial
microvessel density.
Statistical processing
Experimental data were analyzed and processed using
Statistical Product and Service Solutions (SPSS) 12.0 software.
Data were presented as mean ± SD. One-way analysis of variance was
used for the pairwise comparison among groups and the post hoc test
was Least Significant Difference test. The results are presented as
P-value (α=0.05). P<0.05 was considered to indicate a
statistically significant difference.
Results
Detection of scaffold material
characteristics
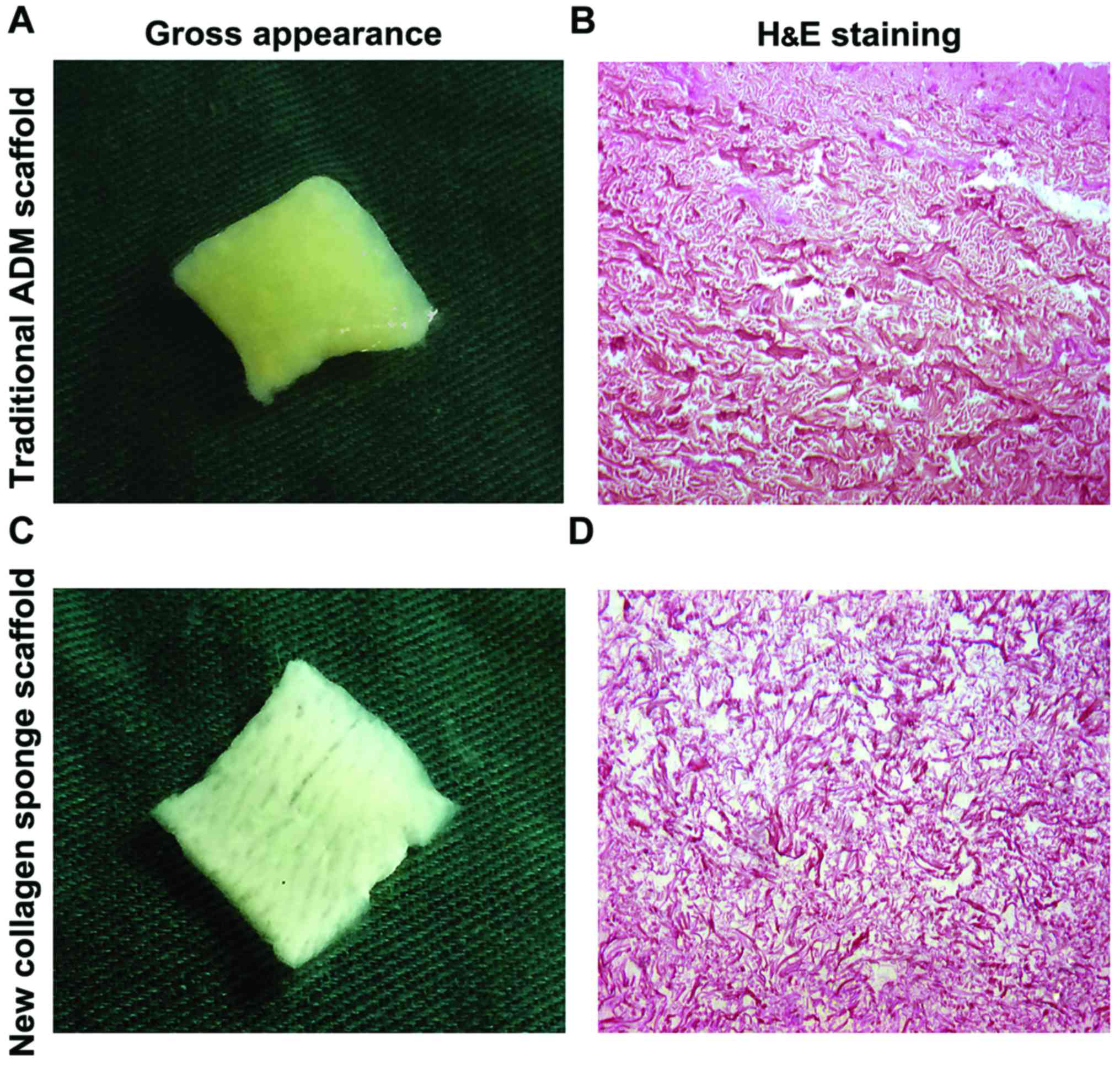
Morphological observation of two kinds of scaffold
materials. By naked eye, traditional ADM scaffold was milky white
or light yellow, tough texture, the surface was flat, smooth and
flexible, and the dense hair follicle holes could be observed
(Fig. 1A); NCSS was milky white or
light yellow, showing soft, loose porous homogeneous shape, and the
surface loose pores could be clearly observed (Fig. 1C).
Histological observation (H&E
staining) of two kinds of scaffold materials
After H&E staining, traditional ADM scaffold
showed red-stained coarse collagen, orderly arrangement of collagen
fibers, complete fibers and uniform pores (Fig. 1B); NCSS showed loose collagen fibers,
slender fibers, complete structure of collagen fibers and uniform
pore distribution (Fig. 1D).
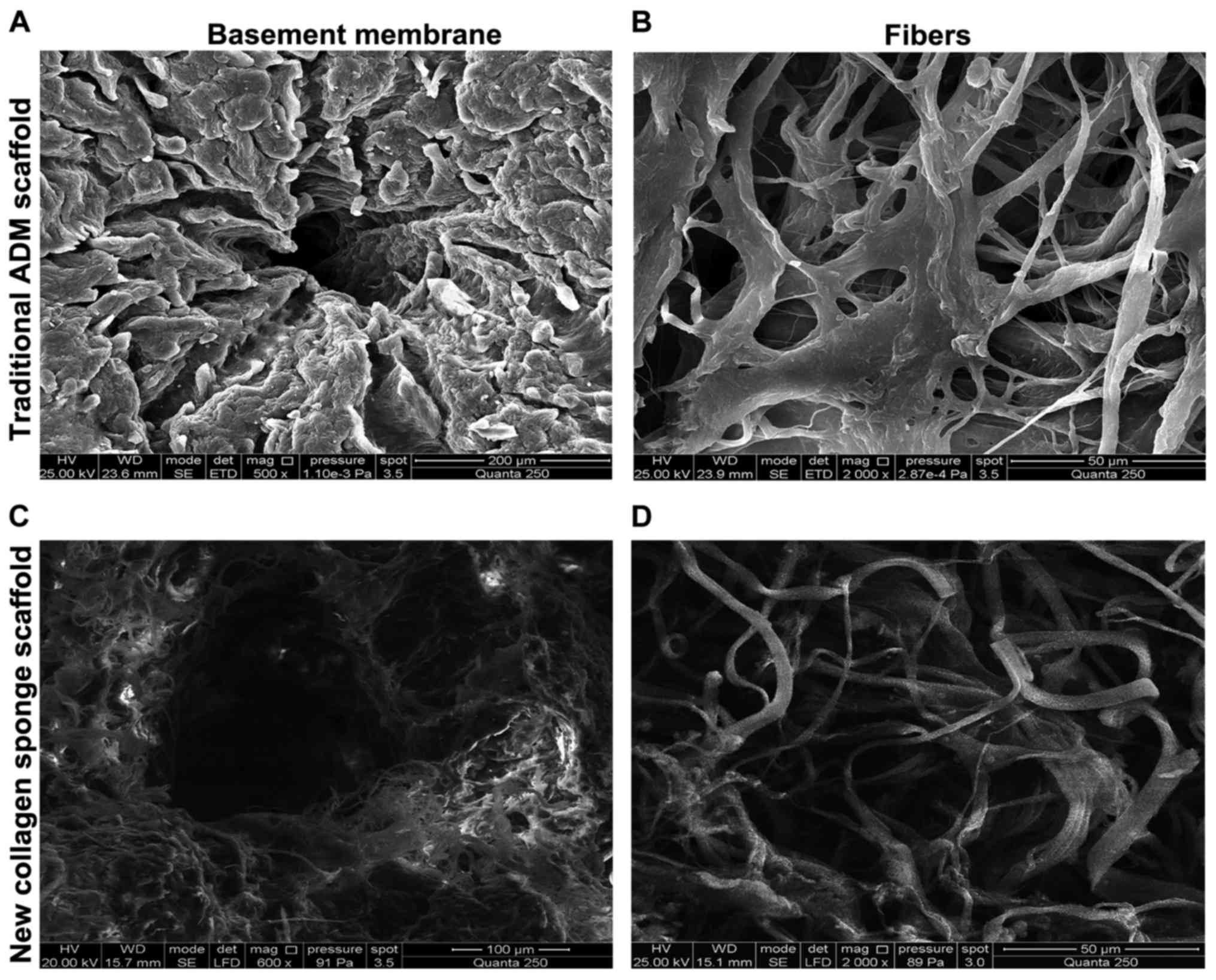
Comparison of pore size of two kinds
of scaffold materials under SEM
No cellular composition could be seen on the surface
of two kinds of scaffold materials under SEM, and the collagen
fibers were arranged neatly and distributed evenly. The fibers were
more slender in NCSS than those in traditional ADM scaffold, and
the porosity was also higher than that in traditional ADM scaffold
by naked eye (Fig. 2).
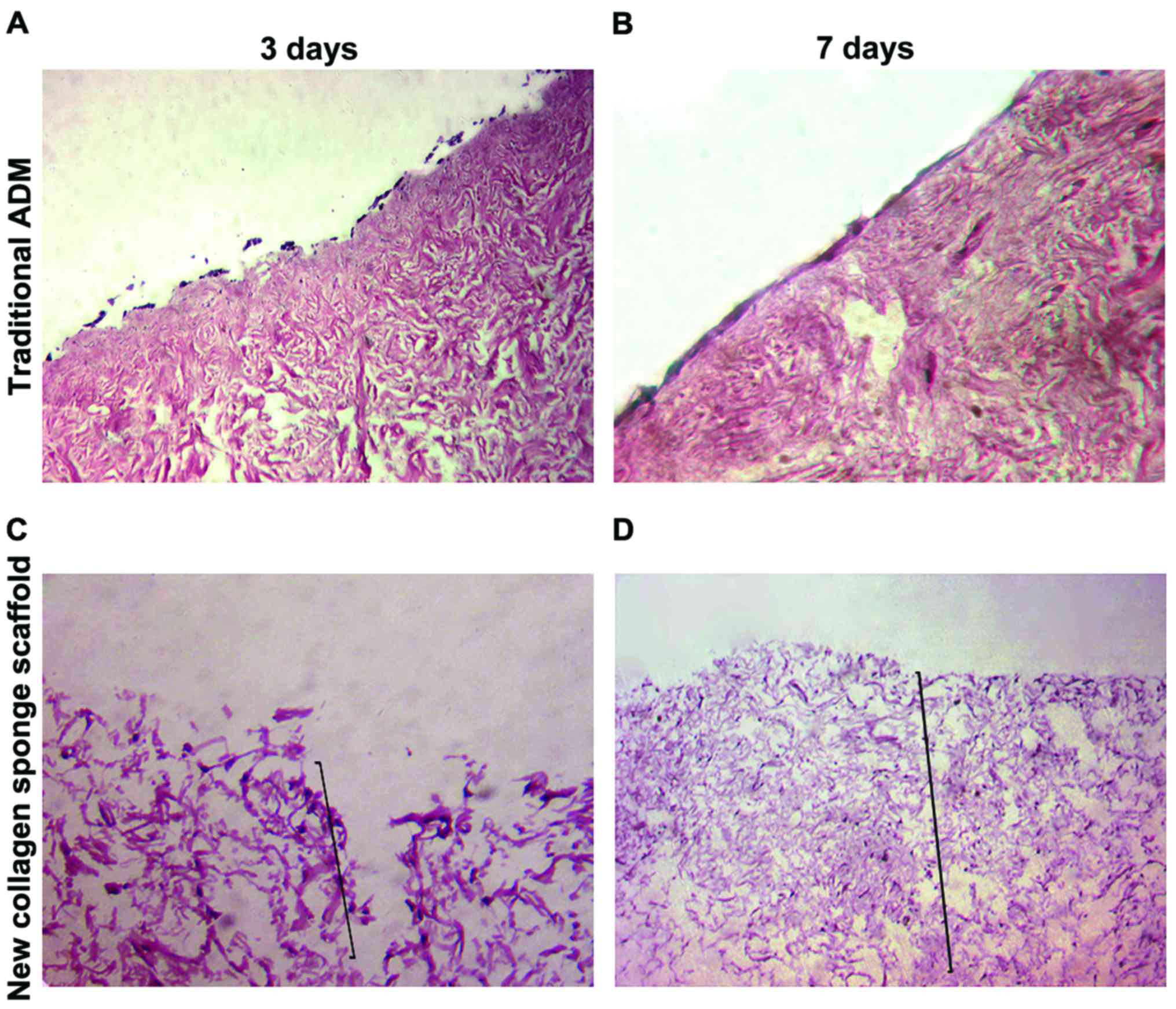
Cytocompatibility and permeability of
two kinds of scaffold materials
At 3 and 7 days after P4-generation ADSCs were
inoculated onto the traditional ADM scaffold material, H&E
staining showed that cells grew in the form of single layer on the
surface of scaffold basement membrane, the number of cells was
increased significantly with the passage of time, and there was no
significant intradermal infiltration (Fig. 3A and B). At 3 and 7 days after ADSCs
were inoculated onto NCSS, H&E staining showed that stem cells
could break through the basal layer for infiltrative growth; the
cell infiltration depth at 7 days was significantly increased
compared with that at 3 days, and the number of cells was also
obviously increased (Fig. 3C and
D).
Skin defect repair via ADSCs combined
with NCSS
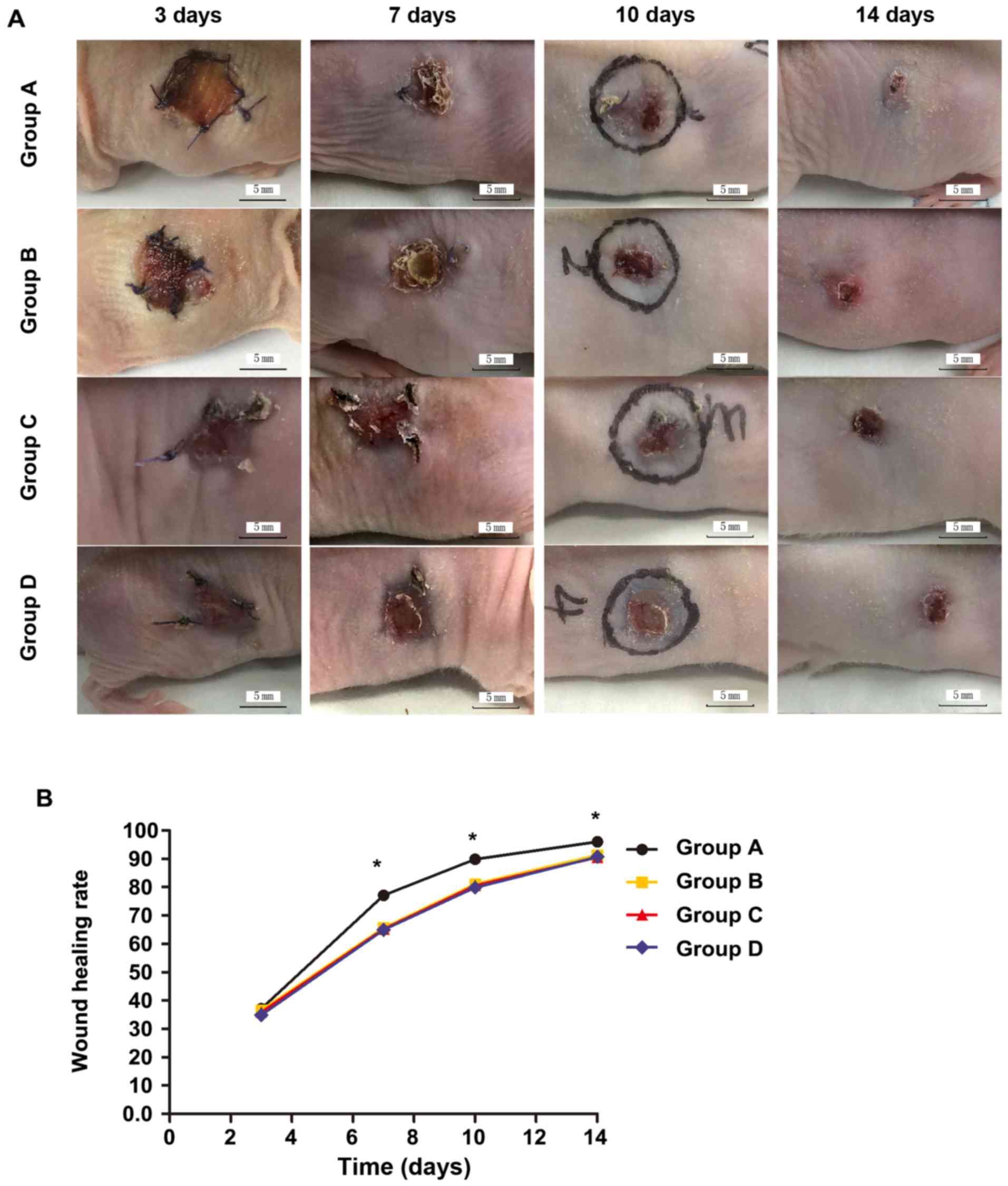
Wound changes and wound healing
rate
At 3 days after operation, the wound was opened; the
grafted skin in groups A and B was ruddy with fine blood supply;
the wounds in groups C and D were clean and moist with fresh
granulation tissues. At 7 days after operation, the wounds in
groups A and B were significantly reduced, and the grafted skin
surfaces were partially desquamated, which was more obvious in
group B than group A; the wounds in groups C and D were further
reduced, and there were no necrosis or infection in either group.
At 10 days after operation, the wound in group A was mostly healed,
and the wound areas in other groups were significantly reduced. At
14 days after operation, the wound in group A was basically healed,
and the residual areas were larger in other groups (Fig. 4). There were no significant
differences in the wound healing rate among groups A-D at 3 days
(p>0.05). At 7, 10 and 14 days, the wound healing rates in group
A were significantly better than those in groups B-D, and the
differences were statistically significant (p<0.05); the
differences among groups B-D were not statistically significant
(p>0.05; Table I).
 | Table I.Wound healing rate at each time-point
after operation. |
Table I.
Wound healing rate at each time-point
after operation.
|
| Wound healing rate
(%) |
|---|
|
|
|
|---|
| Groups | 3 days | 7 days | 10 days | 14 days |
|---|
| A | 37.16±0.78 | 77.13±1.25 | 89.90±1.08 | 96.08±0.6 |
| B | 36.64±1.02 | 65.74±1.31 | 81.09±0.83 | 91.39±0.92 |
| C | 35.96±1.78 | 65.26±0.84 | 80.59±0.94 | 90.55±0.78 |
| D | 34.91±1.58 | 64.96±1.21 | 79.86±1.42 | 90.68±0.53 |
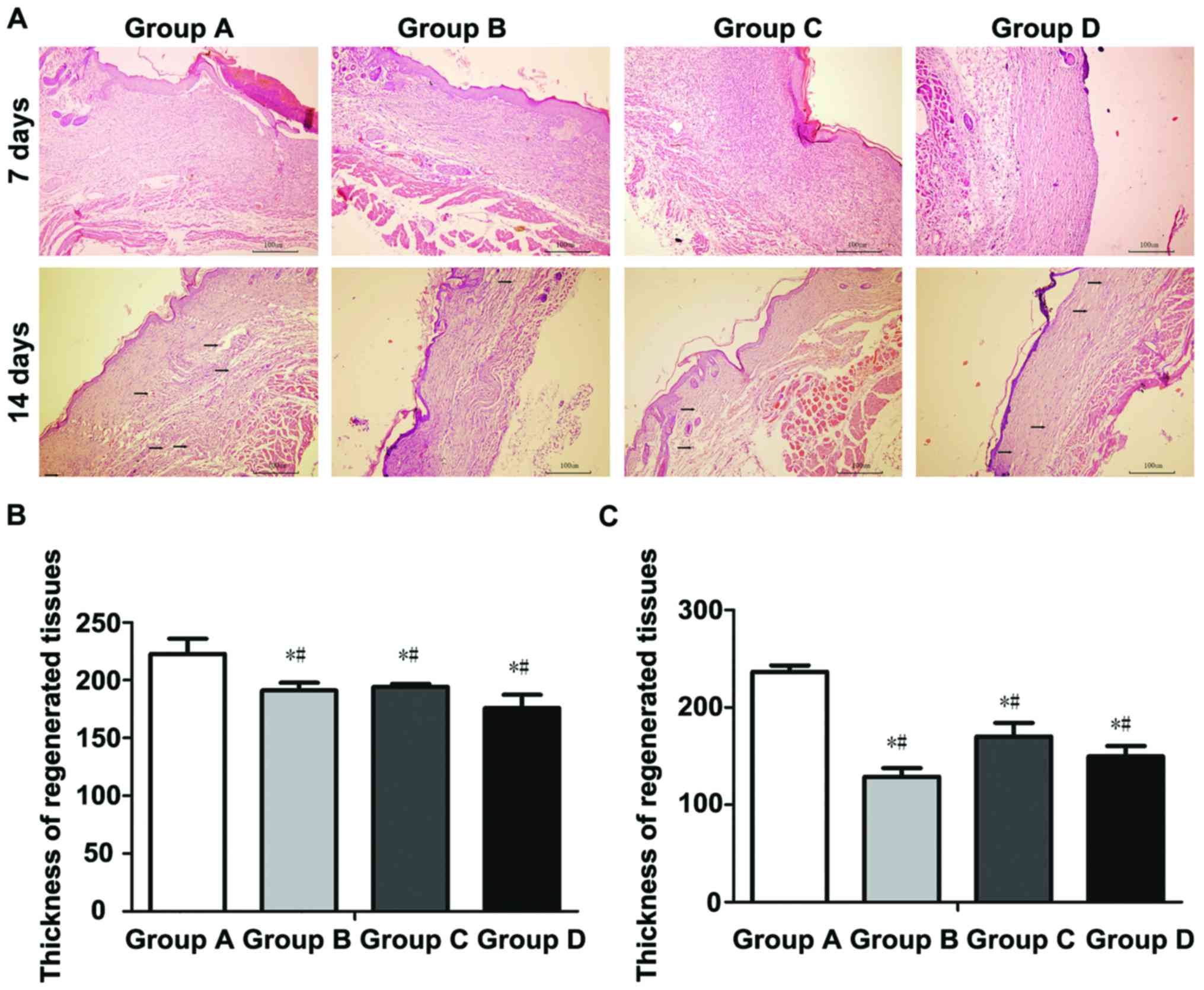
Histological observation of
regenerated skin
At 7 days after operation, the wound tissues were
treated with H&E staining, and observed under an inverted phase
contrast microscope. Results showed the granulation tissue
proliferation in wounds in groups A-D, accompanied by a large
number of microvessels, and varying degrees of inflammatory cell
infiltration in regenerated tissues, accompanied by epidermal cell
regeneration in different degrees (Fig.
5). The thickness of regenerated tissues was (222.72±29.37 µm)
in group A, (180.80±10.32 µm) in group B, (194.18±5.85 µm) in group
C and (175.94±25.79 µm) in group D. The thickness of regenerated
tissues in group A was significantly larger than those in groups
B-D, and the differences were statistically significant
(p<0.05); there were no statistically significant differences
among groups B-D (p>0.05).
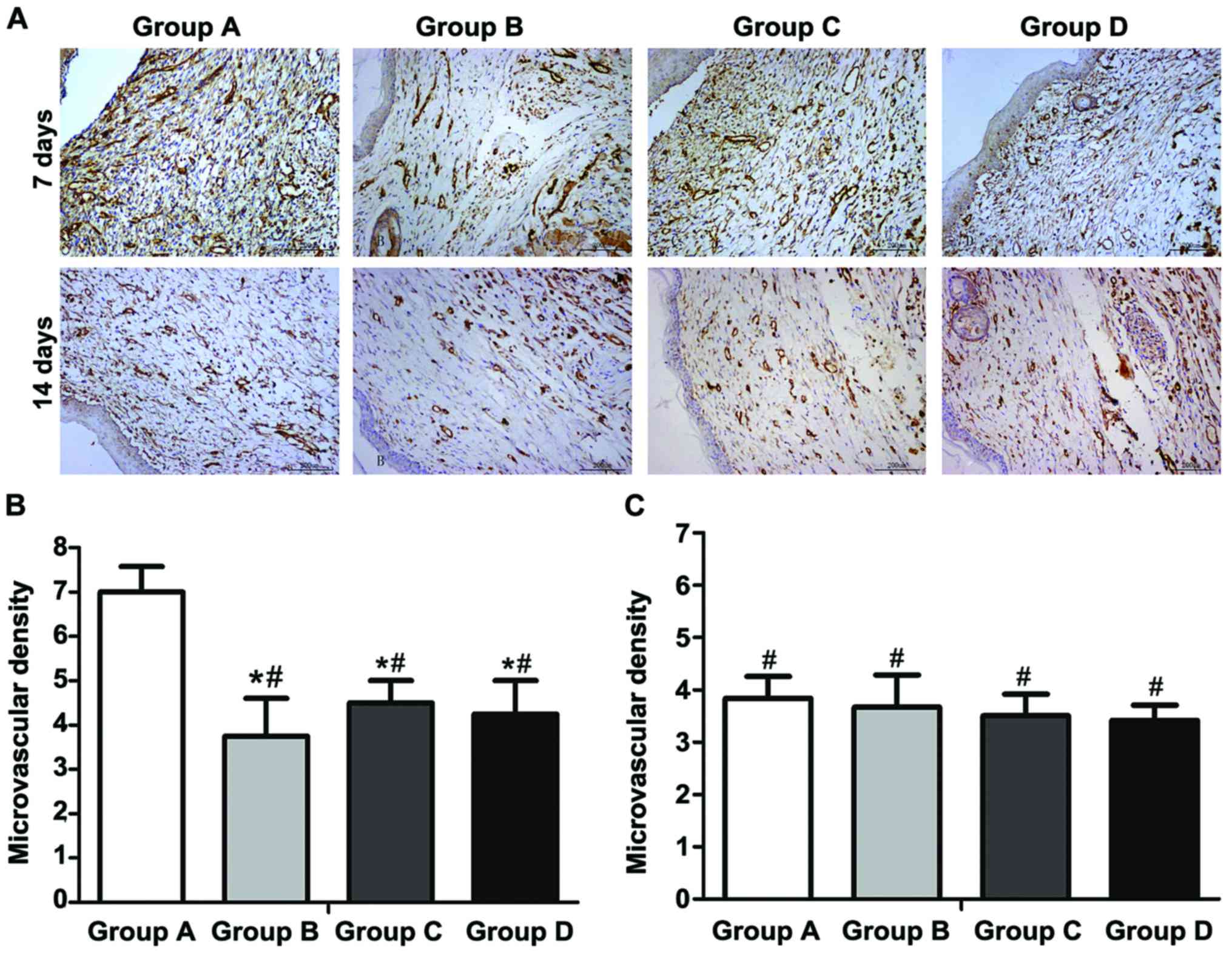
Immunohistochemical detection
At 7 days after operation, the wound tissues were
taken, fixed and sectioned. The immunohistochemical detection
showed that the number of new vessels (deep brown-stained) in the
wound in each group was larger than that at 14 days. At 14 days
after operation, most vessels were occluded, and the number of
vessels was decreased. At 7 days after operation, the average
vascular densities in groups A-D were 7.0±1.2, 3.8±1.7, 4.5±1.0 and
4.3±1.5, respectively. The vascular density in group A was
obviously larger than those in groups B-D, and the difference was
statistically significant (p<0.01); there were no statistically
significant differences among groups B-D (p>0.05). At 14 days
after operation, immunohistochemical detection showed that the
average vascular densities in groups A-D were 3.8±1.5, 3.6±2.1,
3.5±1.4 and 3.4±0.9, respectively; there were no statistically
significant differences in the comparison of vascular density among
groups (p>0.05) (Fig. 6A-C).
Discussion
The large-area wounds left after severe burn,
chronic ulcer and resection of huge superficial tumor often have
significant impact on the patient's physiology and psychology.
Currently, the ideal treatment method is the autologous
split-thickness and full-thickness skin grafting; however, patients
with large-area skin defects often have problems such as
insufficient autologous skin source, new auxiliary incision left
during operation, increase of several surgical scars (8), seriously affecting the clinical
treatment and prognosis of patients. The development of tissue
engineering technique provides a promising treatment means for
wound repair. Moreover, the selection of seed cells and scaffold
materials is crucial in the construction of tissue-engineered
skin.
Experimental studies have shown that ADSCs can
regulate the regenerative microenvironment, and secrete the wound
healing factors during wound repair process (8–10); at
the same time, they also have anti-inflammatory and
immunosuppressive effects (11,12),
with the advantages of promoting cell proliferation, migration,
angiogenesis, anti-apoptosis, improving scar healing (13–16).
ADSCs, therefore, have become a hot topic in the tissue engineering
research.
It was found in the study on stem cells in wound
repair that how to effectively transport stem cells, making them
further differentiate and proliferate in the target area and exert
the repairing effect, is also a difficulty (17,18).
Simple injection of stem cell suspension easily leads to the
‘island’-like deposition of wound cells, local wound ischemia and
hypoxia-induced cell necrosis; besides, the injection scope of stem
cell suspension cannot be precisely controlled, wounds are unevenly
distributed, and a large number of cells are lost (19), affecting the stem cell suspension
injection effect in wound repair. Thus, it can be seen that
reducing the cell loss and death during the migration process and
increasing the effective survival rate in transplantation process
are extremely important for wound repair. Therefore, a suitable
stem cell transfer vector will play an important role in wound
repair.
Scaffold materials can provide stem cells with
adhesion, growth and proliferation sites, and carry sufficient
number of seed cells required for wound repair as stem cell
transport vectors. The collagen scaffold provides the cell adhesion
site for stem cells during wound repair, which facilitates the cell
adhesion, proliferation and migration and provides a good
microenvironment for cell growth; moreover, it can completely cover
and protect the wounds, and prevent the exogenous bacterial
infection. It was found in previous studies that ADM prepared using
the traditional method has problems of low porosity,
non-penetrating pore and poor cell permeability, resulting in low
cell utilization rate and few adherent cells. It is currently
believed that the ideal dermal scaffold material should possess
higher porosity, larger pore size, good cell and tissue
compatibility, and biodegradability. High porosity and larger pore
size are the prerequisites for rapid vascularization in the wound,
while the early rapid vascularization is the key to good wound
healing.
During the preparation of dermal scaffolds, it was
found that temperature has a significant effect on collagen
structure. When heated, collagen fibers will have irreversible
shrinkage; when the temperature rises to 63–65°C, the fiber length
will become 1/9 of the original one; if heated continuously, the
triple-helical structure of collagen molecules will be destroyed,
denatured and decomposed into gelatin, thus losing the natural
pores among collagen fibers and its scaffold effect. Sun et
al (20) found through the
second-harmonic microscope that thermal denaturation may occur in
collagen at 54°C. After repeated experiments, 45°C was selected as
a controllable condition for the preparation of scaffold materials,
which can shorten the length of collagen and loosen the pore
structure of collagen without changing the three-dimensional
structure of collagen and leading to collagen denaturation.
Besides, alkaline process control also has a more obvious impact on
dermal collagen fiber structure; under certain conditions, the
collagen fibers become increasingly looser with the increase of
alkaline solution concentration. Therefore, the temperature and
alkali solution in a certain concentration were used as two
treatment factors, and changing the treatment time as the
experimental condition to successfully prepare NCSS via repeated
experiments. The experimental results showed that the porosity of
NCSS prepared using the modified method (93.1±1.02%) was
significantly higher than that of conventional ADM scaffold
(74.27±2.04%), and the diameter of cavity was (40–247 µm). There
was no statistically significant difference in the in vitro
degradation time between the two kinds of scaffold materials,
basically meeting the requirement for rapid vascularization of
artificial dermis.
The collagen scaffold prepared in this experiment
had obvious three-dimensional structure, which was conducive to the
cell adhesion, growth and proliferation; the diameter of biological
pores was large, benefiting the cell infiltrative growth; the cell
adhesion rate and migration efficiency were high without obvious
cytotoxicity, but a certain mechanical strength and good
plasticity; it could also completely cover the wound and prevent
cell infection. After the repair of full-thickness skin defect on
the back of nude mice via ADSCs combined with NCSS, the wound
healing rate was significantly higher than those in other groups,
indicating that the new tissue-engineered skin substitute
constructed can significantly promote wound healing. Results of
H&E staining showed that the regenerated tissues of wound were
atrophic and thinner at 14 days compared with those at 7 days, the
vascular lumen was occluded and the number of vessels was also
decreased. At 7 and 14 days, the thickness of regenerated tissues
in group A was significantly larger than those in groups B-D. The
number of immunohistochemical CD31-positive vessels in group A at 7
days after operation was significantly larger than those in groups
B-D, suggesting that ADSCs combined with NCSS can significantly
promote wound repair and angiogenesis, and increase the vascular
density in the early stage of wound repair.
ADSCs combined with NCSS and the specific mechanism
of ADSCs in wound healing were not studied in this experiment, but
the animal experimental results showed that the wound healing rate,
regenerated tissue thickness and vascular density in group A were
higher than those in other experimental control and blank control
groups, which was consistent with the results of literature
(7,10,15,21,22); at
the same time, the initial purpose of this experimental research
was achieved.
The key to wound healing is the early
vascularization (23). In this
study, the tissue-engineered skin substitute was constructed using
ADSCs combined with NCSS. After operation, the wound was
photographed and taken for histological detection and
immunohistochemical CD31 vascular density detection. Results showed
that the new tissue-engineered skin substitute could increase the
vascular density in the wound, and improve the wound healing
rate.
NCSS prepared during the experiment met the basic
requirements of scaffold materials in tissue-engineered skin
construction to a certain extent. The tissue-engineered skin
substitute constructed also met the basic conditions of wound
repair, and its biological property, mechanical strength and other
aspects remain to be studied in subsequent experiments.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
AJZ contributed to specimen collection and
detection. TJ and QL helped with preparation of two kinds of dermal
scaffolds. PSJ and QT were responsible for wound model
establishment of mice. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Patients aged 23–45 years signed the informed
consent, those with infectious or skin lesions were excluded, and
this study was approved by the Ethics Committee of the Drum Tower
Clinical College of Nanjing Medical University (Nanjing,
China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Shingyochi Y, Orbay H and Mizuno H:
Adipose-derived stem cells for wound repair and regeneration.
Expert Opin Biol Ther. 15:1285–1292. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ozpur MA, Guneren E, Canter HI, Karaaltin
MV, Ovali E, Yogun FN, Baygol EG and Kaplan S: Generation of skin
tissue using adipose tissue-derived stem cells. Plast Reconstr
Surg. 137:134–143. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Orbay H, Takami Y, Hyakusoku H and Mizuno
H: Acellular dermal matrix seeded with adipose-derived stem cells
as a subcutaneous implant. Aesthetic Plast Surg. 35:756–763. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kim HJ, Park SS, Oh SY, Kim H, Kweon OK,
Woo HM and Kim WH: Effect of acellular dermal matrix as a delivery
carrier of adipose-derived mesenchymal stem cells on bone
regeneration. J Biomed Mater Res B Appl Biomater. 100:1645–1653.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zuk PA, Zhu M, Ashjian P, De Ugarte DA,
Huang JI, Mizuno H, Alfonso ZC, Fraser JK, Benhaim P and Hedrick
MH: Human adipose tissue is a source of multipotent stem cells. Mol
Biol Cell. 13:4279–4295. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhang X, Deng Z, Wang H, Yang Z, Guo W, Li
Y, Ma D, Yu C, Zhang Y and Jin Y: Expansion and delivery of human
fibroblasts on micronized acellular dermal matrix for skin
regeneration. Biomaterials. 30:2666–2674. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Huang SP, Hsu CC, Chang SC, Wang CH, Deng
SC, Dai NT, Chen TM, Chan JY, Chen SG and Huang SM: Adipose-derived
stem cells seeded on acellular dermal matrix grafts enhance wound
healing in a murine model of a full-thickness defect. Ann Plast
Surg. 69:656–662. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wendt H, Hillmer A, Reimers K, Kuhbier JW,
Schäfer-Nolte F, Allmeling C, Kasper C and Vogt PM: Artificial skin
- culturing of different skin cell lines for generating an
artificial skin substitute on cross-weaved spider silk fibres. PLoS
One. 6:e218332011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Reagan MR and Kaplan DL: Concise review:
Mesenchymal stem cell tumor-homing: Detection methods in disease
model systems. Stem Cells. 29:920–927. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Anthony DF and Shiels PG: Exploiting
paracrine mechanisms of tissue regeneration to repair damaged
organs. Transplant Res. 2:102013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Singer NG and Caplan AI: Mesenchymal stem
cells: Mechanisms of inflammation. Annu Rev Pathol. 6:457–478.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liu L, Chiu PW, Lam PK, Poon CC, Lam CC,
Ng EK and Lai PB: Effect of local injection of mesenchymal stem
cells on healing of sutured gastric perforation in an experimental
model. Br J Surg. 102:e158–e168. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Maxson S, Lopez EA, Yoo D,
Danilkovitch-Miagkova A and Leroux MA: Concise review: Role of
mesenchymal stem cells in wound repair. Stem Cells Transl Med.
1:142–149. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Liu YL, Liu WH, Sun J, Hou TJ, Liu YM, Liu
HR, Luo YH, Zhao NN, Tang Y and Deng FM: Mesenchymal stem
cell-mediated suppression of hypertrophic scarring is p53 dependent
in a rabbit ear model. Stem Cell Res Ther. 5:1362014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wahl EA, Fierro FA, Peavy TR, Hopfner U,
Dye JF, Machens HG, Egaña JT and Schenck TL: In vitro evaluation of
scaffolds for the delivery of mesenchymal stem cells to wounds.
BioMed Res Int. 2015:1085712015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Harasymiak-Krzyżanowska I, Niedojadło A,
Karwat J, Kotuła L, Gil-Kulik P, Sawiuk M and Kocki J: Adipose
tissue-derived stem cells show considerable promise for
regenerative medicine applications. Cell Mol Biol Lett. 18:479–493.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kuo YR, Wang CT, Cheng JT, Kao GS, Chiang
YC and Wang CJ: Adipose-derived stem cells accelerate diabetic
wound healing through the induction of autocrine and paracrine
effects. Cell Transplant. 25:71–81. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hiwatashi N, Hirano S, Mizuta M, Tateya I,
Kanemaru S, Nakamura T and Ito J: Adipose-derived stem cells versus
bone marrow-derived stem cells for vocal fold regeneration.
Laryngoscope. 124:E461–E469. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yang J, Yamato M, Kohno C, Nishimoto A,
Sekine H, Fukai F and Okano T: Cell sheet engineering: Recreating
tissues without biodegradable scaffolds. Biomaterials.
26:6415–6422. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sun Y, Chen WL, Lin SJ, Jee SH, Chen YF,
Lin LC, So PT and Dong CY: Investigating mechanisms of collagen
thermal denaturation by high resolution second-harmonic generation
imaging. Biophys J. 91:2620–2625. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Leonardi D, Oberdoerfer D, Fernandes MC,
Meurer RT, Pereira-Filho GA, Cruz P, Vargas M, Chem RC, Camassola
M, Nardi NB, et al: Mesenchymal stem cells combined with an
artificial dermal substitute improve repair in full-thickness skin
wounds. Burns. 38:1143–1150. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Iyyanki TS, Dunne LW, Zhang Q, Hubenak J,
Turza KC and Butler CE: Adipose-derived stem-cell-seeded
non-cross-linked porcine acellular dermal matrix increases cellular
infiltration, vascular infiltration, and mechanical strength of
ventral hernia repairs. Tissue Eng Part A. 21:475–485. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
King A, Balaji S, Keswani SG and
Crombleholme TM: The role of stem cells in wound angiogenesis. Adv
Wound Care (New Rochelle). 3:614–625. 2014. View Article : Google Scholar : PubMed/NCBI
|