Introduction
Postoperative cognitive dysfunction is defined as
postoperative consciousness, cognitive function, memory and
orientation disorders, complicated with mental and sleep disorders
in patients without mental illness before operation. Postoperative
cognitive dysfunction is caused by postoperative neurological
disorders due to various factors including brain disorders
(1). Strong surgical stimulation
caused by cardiac surgery may lead to significant body stress
response, leading to increased level of catecholamines secreted by
sympathetic nervous system (2). In
particular, bypass coronary artery bypass grafting is considered to
be one of the most common predisposing factors for postoperative
cognitive impairment during cardiopulmonary bypass (3).
In recent years, with the development of anesthesia
and cardiopulmonary bypass technology, incidence of postoperative
cognitive dysfunction was significantly decreased, but still cannot
be eradicated (4). Dexmedetomidine,
as a new and efficient adrenergic receptor agonist α2, can induce
physiological sleep (5).
Dexmedetomidine can also effectively inhibit the body's
inflammatory response and thus improve the protection of the
nervous system (6). This study
mainly explores the impact of dexmedetomidine on postoperative
cognitive function in patients with coronary artery bypass
grafting.
Patients and methods
General information
A total of 80 patients undergoing systemic
anesthesia and extracorporeal coronary artery bypass surgery in the
People's Hospital of Guangxi Zhuang Autonomous Region (Nanning,
China) from January 2015 to August 2017 were selected. Patients
were diagnosed by preoperative imaging, clinical manifestations,
and direct observations during surgery. Patients with cognitive
impairment, mental and psychological illness and chronic
alcoholics, drug addicts, abuse of psychotropic substances,
illiterate education, intraoperative use of epinephrine and
norepinephrine, or allergy to drugs used in this study were
excluded. This study was approved by the Ethics Committee of the
People's Hospital of Guangxi Zhuang Autonomous Region, and all
patients signed informed consent. Patients were randomly divided
into two groups, 40 cases in each group. No significant differences
in sex, average age, body mass index (BMI), left ventricular
ejection fraction, intraoperative cardiopulmonary bypass time and
total operation time were found between the groups (P>0.05).
Preoperative mini-mental state examination (MMSE) and Montreal
Cognitive Assessment (MoCA, Beijing version) were performed and no
significant differences in MMSE and MoCA scores were found between
the groups (Table I).
 | Table I.Comparison of general information
between the two groups. |
Table I.
Comparison of general information
between the two groups.
| Groups | Sex
(male/female) | Age (years) | Body mass index
(kg/m2) | Left ventricular
ejection fraction (%) | Intraoperative
cardiopulmonary bypass time (min) | Total operation time
(min) | MMSE | MoCA |
|---|
| Observation
(n=40) | 28/12 | 42.3±1.6 | 23.5±1.1 | 53.1±2.1 | 113.0±5.1 | 206.5±15.3 | 28.5±0.2 | 28.1±0.5 |
| Control (n=40) | 27/13 | 42.4±1.5 | 23.6±1.0 | 53.0±2.0 | 113.1±5.0 | 206.4±15.2 | 28.6±0.3 | 28.2±0.6 |
| t or χ2
value | 0.001 | 0.288 | 0.425 | 0.218 | 0.089 | 0.029 | 1.754 | 0.810 |
| p-value | 0.999 | 0.774 | 0.672 | 0.828 | 0.930 | 0.977 | 0.083 | 0.421 |
Method
All patients underwent surgical treatment under
general anesthesia with endotracheal intubation. Patients were
fasted and not allowed to drink water before operation. Peripheral
vein was opened and connected to the monitor, and patient's
noninvasive blood pressure, electrocardiogram, heart rate and
oxygen saturation were monitored continuously. Anesthesia machine
was used to detect the changes of respiratory function in patients.
Anesthesia was induced by intravenous infusion of midazolam,
fentanyl, cisatracurium and etomidate. Tracheal intubation was
performed under slow induction of anesthesia, and was connected to
anesthesia machine for mechanical ventilation, oxygen flow rate was
set to 50%, respiratory rate was set to 14 times/min, and tidal
volume was set according to patient weight (10 ml/kg). Peripheral
arterial puncture, central venous catheterization and pressure
measurement were performed. Intraoperative anesthesia was performed
by using propofol, remifentanil and cisatracurium. Cardiopulmonary
bypass technology was used. Dexmedetomidine (SFDA approval number:
H20130027, CISEN), solution (4 µg/ml) was prepared and pumped into
patients in the observation group through a vein with a dose of 1
µg/kg during the first 10 min, followed by the dose of 0.2 µg/kg
until the end of surgery. Equal volume of 0.9% saline was used at
the same speed for patients in the control group, and 1 mg of
midazolam was intravenously administered every 30 min. Based on
patient circulatory function, vasoactive drug was given through
extracorporeal circulation machine during surgery, and vasoactive
drugs were intravenously administered after cardiopulmonary bypass.
All patients had the same indications for the use of vasoactive
drugs, and drugs used here included: popamine, metaxylamine,
epinephrine, phenylephrine and norepinephrine.
Observation indexes
Circulatory function-related complications, such as
arrhythmia, hypertension, and hypotension were compared between the
two groups. BIS was recorded at 30 min before induction of
anesthesia (T0), immediately after intubation (T1), when incision
was made (T2), when chest was closed (T3), when operation was
completed (T4) and at 6 h after operation (T5). The levels of
cortisol, epinephrine and norepinephrine at the end of operation
were recorded, and recovery time and mechanical ventilation time of
the two groups were compared. MMSE and MoCA were performed at 1, 3
and 7 days after operation. The incidence rates of intraoperative
awareness and postoperative cognitive dysfunction in the two groups
were compared.
Assessment criteria
BIS value was measured by using A-3000 BIS monitor
(Aspect Medical System, Covidien, MA, USA) and its ancillary
equipment. BIS value fluctuated between 1 and 100. The higher the
BIS value is, the higher the sober level is. BIS higher than 95%
indicated completely awaken state, and BIS lower than 70% indicated
disorder of consciousness. Stress factors, including cortisol
(80–550 nmol/l), epinephrine (<480 pmol/l) and norepinephrine
(615–3240 pmol/l), were measured by Bio-Rad 450 automatic
biochemical analyzer (Bio-Rad Laboratories, Inc., Hercules, CA,
USA). MMSE contains seven aspects and 30 questions with a score of
0 to 30, and 27 points was the threshold for cognitive impairment.
Lower MMSE score indicated more severe cognitive impairment. MoCA:
Test was completed within 10 min, and the highest score was 30
points, and the lowest score was 0. A score over 26 points
indicated normal conditions. Lower MoCA score indicated more severe
cognitive impairment. MoCA was not performed within 60 min after
MMSE, and MMSE was not performed within 24 h after MoCA.
Arrhythmias are indicated by electrocardiogram. Hypertension in
anesthesia means: blood pressure is greater than 140/95 mmHg or
elevated blood pressure is greater than 20%. Hypotension in
anesthesia was defined as: blood pressure is less than 90/60 mmHg
or decreased blood pressure is greater than 30%.
Statistical analysis
SPSS13.0 (SPSS, Inc., Chicago, IL, USA) was used.
Measurement data are expressed as mean ± standard deviation.
Comparisons of mean values between the two groups were performed by
using t-test, and intragroup comparisons were performed by
χ2 test. P<0.05 was considered to indicate a
statistically significant difference.
Results
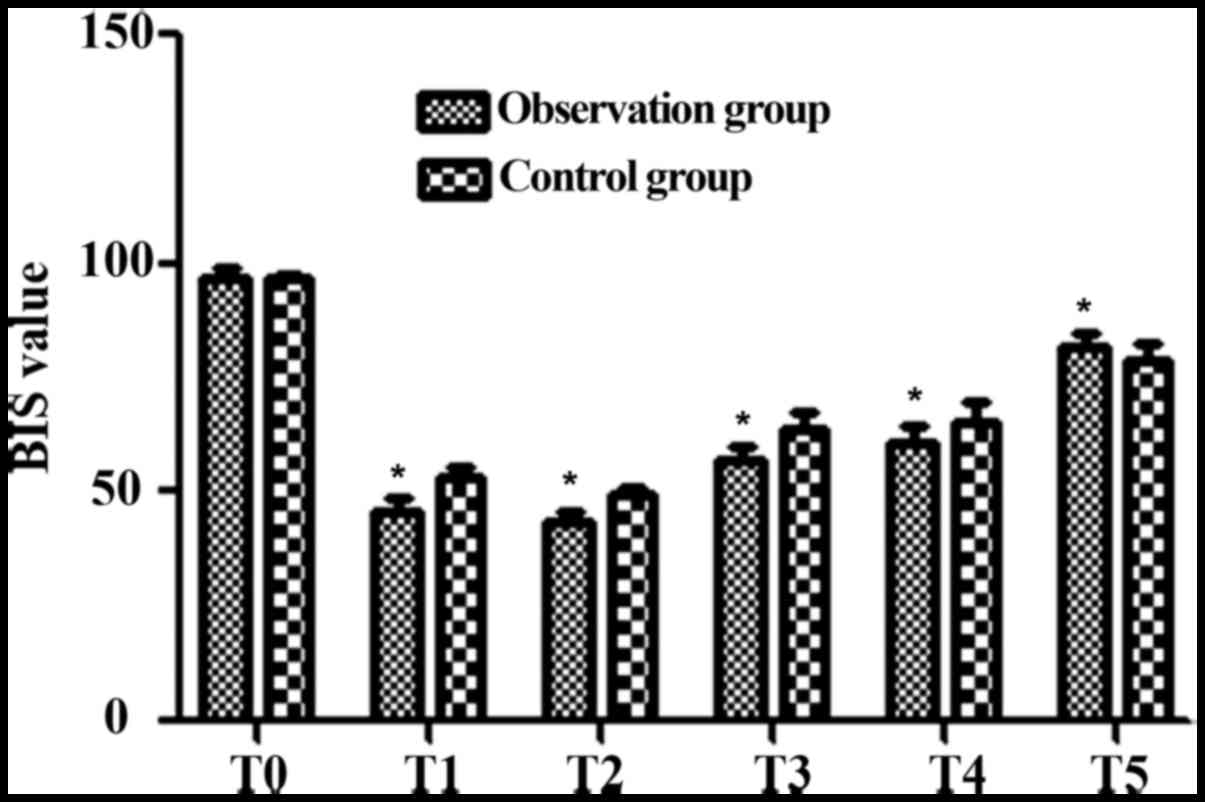
Comparison of BIS values between the
two groups at different time-points
BIS values in the observation group at T0-T5 were
96.8±2.0, 45.8±2.9, 43.3±2.3, 56.9±3.1, 60.9±3.5 and 81.9±3.3,
respectively, and BIS values in the control group at T0-T5 were
96.9±1.0, 53.3±2.6, 49.6±1.8, 63.5±3.9, 65.3±4.6 and 78.9±3.6,
respectively. BIS values in the observation group were
significantly lower than those in the control group at T1 to T4
(t=8.931, 4.980, 8.379 and 4.814, P<0.05), while BIS value in
the observation group was significantly higher than that in the
control group at T5 (t=3.885, P<0.05) (Fig. 1).
Comparison of intraoperative
circulatory function-related complications between the two
groups
The incidence rates of intraoperative arrhythmia,
hypertension and hypotension in the observation group were
significantly lower than those in the control group (P<0.05)
(Table II).
| Table II.Comparison of intraoperative
circulatory function-related complications between the two
groups. |
Table II.
Comparison of intraoperative
circulatory function-related complications between the two
groups.
| Groups | Arrhythmia | Hypertension | Hypotension | Total incidence |
|---|
| Observation
(n=40) | 1 | 1 | 1 | 3 (7.5%) |
| Control (n=40) | 3 | 4 | 4 | 11 (27.5%) |
| χ2
value |
| – |
| 4.242 |
| P-value |
| – |
| 0.039 |
Comparison of levels of cortisol,
epinephrine and norepinephrine between the two groups at the end of
operation
At the end of surgery, the levels of cortisol,
epinephrine and norepinephrine in the observation group were
significantly lower than those in the control group (P<0.05)
(Table III).
| Table III.Comparison of levels of cortisol,
epinephrine and norepinephrine at the end of operation between the
two groups (mean ± SD). |
Table III.
Comparison of levels of cortisol,
epinephrine and norepinephrine at the end of operation between the
two groups (mean ± SD).
| Groups | Cortisol
(nmol/l) | Epinephrine
(pmol/l) | Norepinephrine
(pmol/l) |
|---|
| Observation
(n=40) | 10.1±0.7 |
50.3±2.3 | 58.5±5.0 |
| Control (n=40) | 23.2±1.9 | 100.1±6.5 | 179.6±11.7 |
| t value | 40.918 | 45.680 | 60.196 |
| P-value | <0.001 | <0.001 | <0.001 |
Comparison of anesthesia recovery time
and mechanical ventilation time between the two groups
Anesthesia recovery time in the observation group
was significantly shorter than that in the control group
(P<0.05), and postoperative mechanical ventilation time in the
observation group was also significantly shorter than that in the
control group (P<0.05) (Table
IV).
| Table IV.Comparison of anesthesia recovery time
and mechanical ventilation time between the two groups (h, mean ±
SD). |
Table IV.
Comparison of anesthesia recovery time
and mechanical ventilation time between the two groups (h, mean ±
SD).
| Groups | Anesthesia recovery
time | Mechanical
ventilation time |
|---|
| Observation
(n=40) | 6.2±0.8 | 13.8±2.1 |
| Control (n=40) | 9.9±1.3 | 18.6±2.6 |
| t value | 15.330 | 9.083 |
| P-value | <0.001 | <0.001 |
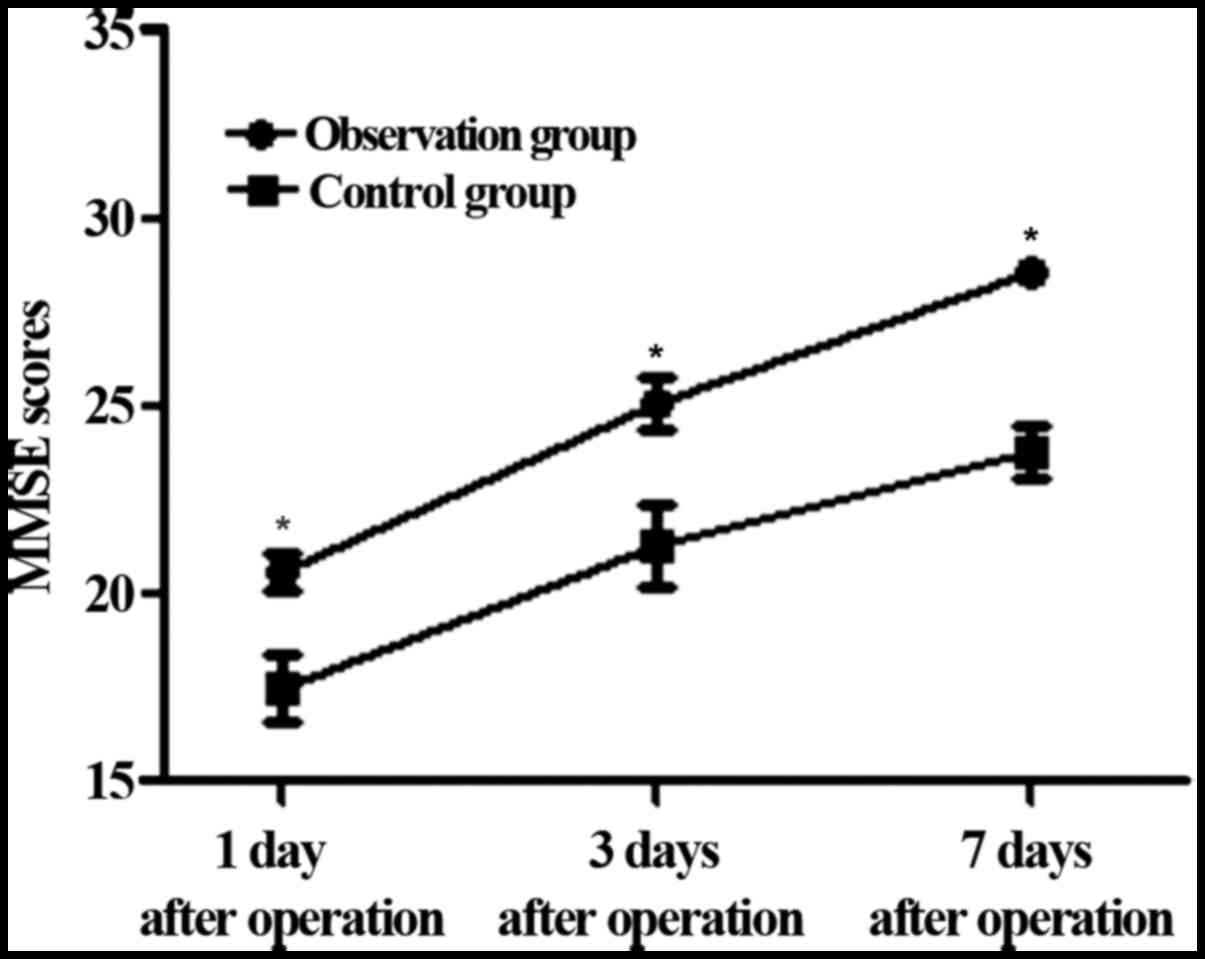
Changes in MMSE during follow-up
MMSE scores in the observation group were 20.6±0.5
points, 25.1±0.7 points and 28.6±0.3 points at 1 day, 3 days and 7
days after operation, respectively. MMSE scores in the control
group were 17.5±0.9 points, 21.3±1.1 points and 23.8±0.7 points at
1 day, 3 days and 7 days after operation, respectively. MMSE scores
in the observation group were significantly higher than those in
the control group at the three time points (t=19.043, 18.433 and
39.862, P<0.001) (Fig. 2).
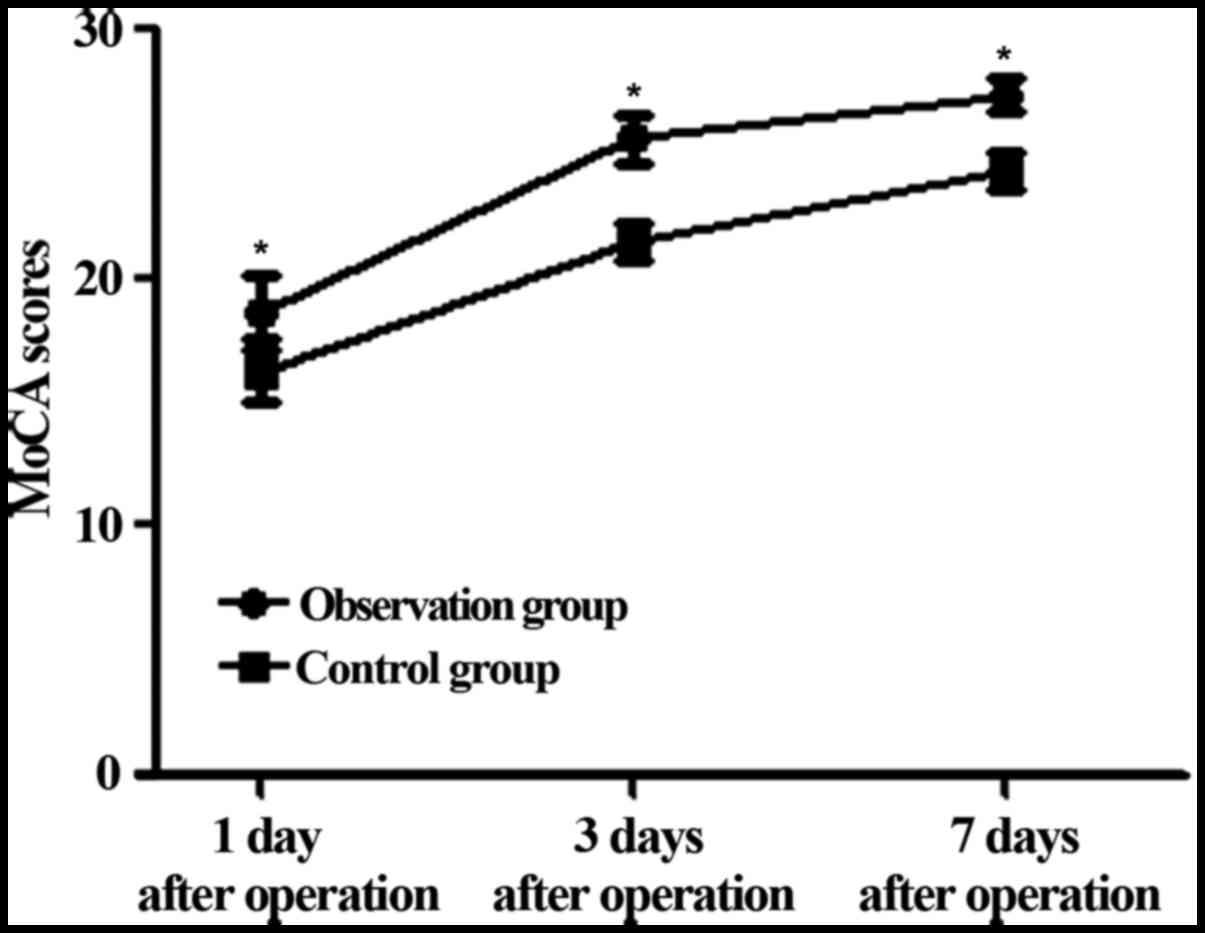
Changes in MoCA during follow-up
MoCA scores were 18.6±1.5 points, 25.6±1.0 points
and 27.4±0.6 points in the observation group at 1 day, 3 days and 7
days after operation, respectively, and MoCA scores in the control
group were 16.3±1.3 points, 21.5±0.8 points and 24.3±0.8 points at
1 day, 3 days and 7 days after operation, respectively. MoCA scores
in the observation group were significantly higher than those in
the control group (t=7.328, 20.248 and 19.606, P<0.001 <0.05)
(Fig. 3).
Comparison of intraoperative awareness
and postoperative cognitive impairment between the two groups
The incidence rates of intraoperative awareness and
postoperative cognitive impairment in the observation group were
significantly lower than those in the control group (Table V).
| Table V.Comparison of intraoperative awareness
and postoperative cognitive impairment between the two groups
(cases, %). |
Table V.
Comparison of intraoperative awareness
and postoperative cognitive impairment between the two groups
(cases, %).
| Groups | Intraoperative
awareness | Postoperative
cognitive impairment |
|---|
| Observation
(n=40) | 1 (2.5) | 1 (2.5) |
| Control (n=40) | 9 (22.5) | 10 (25) |
| χ2
value | 5.600 | 6.746 |
| P-value | 0.018 | 0.009 |
Discussion
Postoperative cognitive impairment is a relatively
mild clinical cognitive disorder, but it may cause decreased social
activities for a few weeks or months, leading to decreased
self-care ability (7). Incidence of
postoperative cognitive impairment in patients with coronary artery
surgery was significantly higher than that in patients without the
surgery (8). Studies have shown that
>40% patients will develop cognitive dysfunction within 7 days
after coronary artery-related surgery (9), and the incidence in elderly patients is
even higher. Dexmedetomidine is currently the most widely used α2
adrenergic receptor agonist in the clinical treatment (10). Dexmedetomidine can induce
physiological sleep, achieve certain synergistic analgesic and
sympathetic inhibitory effects (11). Previous studies (12) have shown that dexmedetomidine can
reduce body stress, inflammation, and inhibit oxidation reaction.
Application of dexmedetomidine in anesthesia can maintain sedation,
accelerate recovery and reduce the feeling of being drunk (13).
The patients in the observation group were treated
with dexmedetomidine. It was found that BIS values in the
observation group were lower than those in the control group at T1
to T4 (T1: immediately after intubation, T2: when incision was
made, T3: when chest was closed, T4: when operation was completed),
while BIS value in the observation group was higher than that in
the control group at T5 (6 h after operation, t=3.885, P<0.05).
The sedative effect was significantly better in the observation
group than in the control group, suggesting that intraoperative
sedation effect of dexmedetomidine can accelerate postoperative
recovery. Comparison of cyclic function related complications
showed that the incidence rates of arrhythmia, hypertension and
hypotension were significantly lower in the observation group than
in the control group, indicating that dexmedetomidine is safer than
midazolam for circulatory function. The comparison of levels of
cortisol, epinephrine and norepinephrine at the end of surgery
showed that the levels of cortisol, epinephrine and norepinephrine
in the observation group were significantly lower than those in the
control group, indicating that dexmedetomidine can effectively
inhibit the body's stress response and reduce catecholamine hormone
secretion. The comparison of anesthesia recovery time and
mechanical ventilation time showed that anesthesia recovery time
and mechanical ventilation time were significantly shorter in the
observation group than in the control group, indicating that
dexmedetomidine can effectively shorten the postoperative
mechanical ventilation, and promote postoperative recovery. The
comparison of MMSE and MoCA scores showed that MMSE and MoCA scores
in the observation group were significantly higher than those in
the control group at 1 day, 3 days and 7 days after operation, and
the incidence rates of intraoperative awareness and postoperative
cognitive dysfunction were significantly lower in the observation
group than in the control group, indicating that dexmedetomidine
can effectively improve postoperative cognitive function and reduce
the incidence of intraoperative awareness.
Continuous intravenous infusion of dexmedetomidine
can alleviate the severity of the patient's stress response and
reduce catecholamine hormone secretion (14), thereby reducing the activity of the
sympathetic nervous system, effectively stabilizing patient's
hemodynamics (15), alleviating the
stress reaction, reducing the trauma to the body caused by
operation and anesthesia stimulation and ischemia-reperfusion
injury caused by extracorporeal circulation, and improving the
protection effects on the nervous system (16). Dexmedetomidine can also inhibit
monocyte Toll-like receptor-1 and Toll-like receptor-2 expression
(17), thereby reducing the body's
inflammatory response (18) and
reducing the incidence of postoperative cognitive dysfunction. In
addition, the use of dexmedetomidine can reduce glutamate
neurotoxicity (19) and apoptosis of
neuronal cells (20). Therefore, it
is of great significance to relieve postoperative cognitive
dysfunction in patients.
In conclusion, dexmedetomidine can effectively
reduce the incidence of postoperative cognitive dysfunction in
patients undergoing cardiopulmonary bypass surgery and it is of
high safety for circulatory function.
Acknowledgements
Not applicable.
Funding
This study was supported by the Self-financing
research project of the Health and Family Planning Commission of
Guangxi Zhuang Autonomous Region (nos. Z20180699, Z20170363 and
Z2012259).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZG and LM conceived and designed the study. ZG, JL
and YZ were responsible for the collection and analysis of the
patient data. JL, XG and AH interpreted the data and drafted the
manuscript. JL and LM revised the manuscript critically for
important intellectual content. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
the People's Hospital of Guangxi Zhuang Autonomous Region (Nanning,
China). Signed informed consents were obtained from the patients or
the guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jo YY, Kim JY, Lee JY, Choi CH, Chang YJ
and Kwak HJ: The effect of intraoperative dexmedetomidine on acute
kidney injury after pediatric congenital heart surgery: A
prospective randomized trial. Medicine (Baltimore). 96:e74802017.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Anton-Martin P, Modem V, Taylor D, Potter
D and Darnell-Bowens C: A retrospective study of sedation and
analgesic requirements of pediatric patients on extracorporeal
membrane oxygenation (ECMO) from a single-center experience.
Perfusion. 32:183–191. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bulow NMH, Colpo E, Pereira RP, Correa
EFM, Waczuk EP, Duarte MF and Rocha JBT: Dexmedetomidine decreases
the inflammatory response to myocardial surgery under
mini-cardiopulmonary bypass. Braz J Med Biol Res. 49:e46462016.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cheng X, Zuo Y, Zhao Q, Gu E and Huang Y:
Comparison of the effects of dexmedetomidine and propofol on
hemodynamics and oxygen balance in children with complex congenital
heart disease undergoing cardiac surgery. Congenit Heart Dis.
10:E123–E130. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Klamt JG, Vicente WV, Garcia LV and
Ferreira CA: Hemodynamic effects of the combination of
dexmedetomidine-fentanyl versus midazolam-fentanyl in children
undergoing cardiac surgery with cardiopulmonary bypass. Rev Bras
Anestesiol. 60:350–362. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tang W, Wang J, Fu GQ and Yuan L: Effect
of dexmedetomidine and midazolam on respiration and circulation
functions in patients undergoing open heart surgery under
acupuncture-assisted general anesthesia. Zhen Ci Yan Jiu.
39:216–221. 2014.(In Chinese). PubMed/NCBI
|
|
7
|
Ueki M, Kawasaki T, Habe K, Hamada K,
Kawasaki C and Sata T: The effects of dexmedetomidine on
inflammatory mediators after cardiopulmonary bypass. Anaesthesia.
69:693–700. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ji F, Li Z, Young JN, Yeranossian A and
Liu H: Post-bypass dexmedetomidine use and postoperative acute
kidney injury in patients undergoing cardiac surgery with
cardiopulmonary bypass. PLoS One. 8:e774462013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lu JG, Pensiero A, Aponte-Patel L, de
Villa Velez B, Rusanov A, Cheng B, Cabreriza SE and Spotnitz HM:
Short-term reduction in intrinsic heart rate during biventricular
pacing after cardiac surgery: A substudy of a randomized clinical
trial. J Thorac Cardiovasc Surg. 146:1494–1500. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Curtis JA, Hollinger MK and Jain HB:
Propofol-based versus dexmedetomidine-based sedation in cardiac
surgery patients. J Cardiothorac Vasc Anesth. 27:1289–1294. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bhaskar P, John J, Sivamurthy SK, Lone RA,
Tysarowski PA, Riyas MK, Syed SA, Bhat AN and Sallehuddin A:
Anesthetic management of an infant with Joubert syndrome for
cardiac surgery. J Clin Anesth. 25:488–490. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Naguib AN, Tobias JD, Hall MW, Cismowski
MJ, Miao Y, Barry N, Preston T, Galantowicz M and Hoffman TM: The
role of different anesthetic techniques in altering the stress
response during cardiac surgery in children: A prospective,
double-blinded, and randomized study. Pediatr Crit Care Med.
14:481–490. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wagner D, Pasko D, Phillips K, Waldvogel J
and Annich G: In vitro clearance of dexmedetomidine in
extracorporeal membrane oxygenation. Perfusion. 28:40–46. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Neema PK: Dexmedetomidine in pediatric
cardiac anesthesia. Ann Card Anaesth. 15:177–179. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yoshitomi O, Cho S, Hara T, Shibata I,
Maekawa T, Ureshino H and Sumikawa K: Direct protective effects of
dexmedetomidine against myocardial ischemia-reperfusion injury in
anesthetized pigs. Shock. 38:92–97. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kunisawa T, Ueno M, Kurosawa A, Nagashima
M, Hayashi D, Sasakawa T, Suzuki A, Takahata O and Iwasaki H:
Dexmedeto-midine can stabilize hemodynamics and spare anesthetics
before cardiopulmonary bypass. J Anesth. 25:818–822. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Huang J, Dinh M, Kuchle N and Zhou J:
Anesthetic management for combined mitral valve replacement and
aortic valve repair in a patient with osteogenesis imperfecta. Ann
Card Anaesth. 14:115–118. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Leino K, Hynynen M, Jalonen J, Salmenperä
M, Scheinin H and Aantaa R; Dexmedetomidine in Cardiac Surgery
Study Group, : Renal effects of dexmedetomidine during coronary
artery bypass surgery: A randomized placebo-controlled study. BMC
Anesthesiol. 11:92011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Butt WW: Minimize stress and maximize
clinical outcome! Pediatr Crit Care Med. 14:1–548. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Maldonado JR, Wysong A, van der Starre PJ,
Block T, Miller C and Reitz BA: Dexmedetomidine and the reduction
of postoperative delirium after cardiac surgery. Psychosomatics.
50:206–217. 2009. View Article : Google Scholar : PubMed/NCBI
|