Introduction
Males have a higher incidence of bladder cancer than
females (1). Although cigarette
smoking and occupational exposure to chemicals are the common risk
factors associated with the development of bladder cancer, the
higher incidence in males cannot be fully explained even after
adjustment for these carcinogenic factors (2–4). Recent
findings have suggested that androgen signals could account, in
part, for the gender difference in bladder cancer incidence
(5–7). Androgen receptor (AR) and
dihydrotestosterone (DHT) are the most important factors in
androgen signals. Although in vitro and animal studies have
demonstrated that AR serves an important role in bladder cancer
(6,7), no significant association was observed
between AR expression and pathological stage, grade or outcome of
bladder cancer in a recent multi-institute study (8). DHT has also been demonstrated to
promote the growth of bladder cancer cells both in vitro and
in animals (6,9), but there is no report on the expression
of enzymes involving the formation of DHT in patients with bladder
cancer.
Dehydroepiandrosterone is one of the sources of DHT,
which is converted from dehydroepiandrosterone sulfate by steroid
sulfatase (STS) (10).
Dehydroepiandrosterone, having higher circulating concentration and
longer half-life in blood, acts as a central reservoir for the
formation of biologically active androgens via the action of tissue
STS (10). Inhibition of STS may be
a novel approach to block the formation of steroids with potent
androgenic property; STS has also been suggested to be a
therapeutic target for androgen-dependent cancer, such as prostate
cancer (11,12), in which STS expression was observed
in 85% of cancer tissues, but not in normal tissues (13). To the best of our knowledge the
expression of STS in bladder cancer has not yet been studied. The
purpose of the present study was to determine the clinical and
functional signification of STS in bladder cancer.
Materials and methods
Patients
Immunohistochemical analysis was performed on
samples from 114 patients with urothelial carcinoma, who were
treated for bladder cancer by radical cystectomy at Osaka City
University Hospital between January 1995 to December 2015. The
clinicopathological characteristics of the patients are summarized
in Table I. There were 89 male and
25 female patients, and the median age was 69 years (range, 33–84
years). Patients who were either incompletely resected, or
histologically confirmed as small cell carcinoma of the bladder, or
lost to follow-up, were excluded from the study. Pathologic staging
was performed according to the 2009 Tumor, Node, Metastasis
classification system (14), and
grading was done according to the criteria by the World Health
Organization, 2004 (15). The
Institutional Review Board at Osaka City University Graduate School
of Medicine approved the use of the specimens and clinical data in
accordance with the Declaration of Helsinki and guidelines of Osaka
City University Graduate School of Medicine (study approval no.
1955). All 114 patients included in the present study provided
written informed consent for the collection and use of tissue
samples and for the publication of their results.
 | Table I.Patients' characteristics and steroid
sulfatase expression (n=114). |
Table I.
Patients' characteristics and steroid
sulfatase expression (n=114).
| Characteristic | Steroid
sulfatase-positive tumors, n (%) | P-value |
|---|
| Age, years |
| 0.758 |
| <65
(n=30) | 7 (23.3) |
|
| ≥65
(n=84) | 22 (26.2) |
|
| Sex |
| 0.852 |
| Male
(n=89) | 23 (25.8) |
|
| Female
(n=25) | 6 (24.0) |
|
| Pathological
Stage |
| 0.003 |
| pTa +
pT1 + pTis (n=52) | 6 (11.5) |
|
| pT2 +
pT3 + pT4 (n=62) | 23 (37.1) |
|
| Grade |
| 0.561 |
| Low
(n=11) | 2 (18.2) |
|
| High
(n=103) | 27 (26.2) |
|
| Lymph node
involvement |
| 0.065 |
| Yes
(n=13) | 6 (46.2) |
|
| No
(n=101) | 23 (22.6) |
|
| Neoadjuvant
chemotherapy |
| 0.844 |
| Yes
(n=45) | 11 (24.4) |
|
| No
(n=69) | 18 (26.1) |
|
| Smoking
history |
| 0.648 |
| Yes
(n=47) | 13 (27.7) |
|
| No
(n=67) | 16 (23.9) |
|
Immunohistochemical analysis of STS,
E-cadherin and vimentin in bladder cancer tissues
Tissues obtained by radical cystectomy were fixed
with 10% formalin for 24–48 h at room temperature and
paraffin-embedded. Paraffin embedding was performed as follow: 100%
ethanol (4×1.5 h at 37°C), 100% ethanol (2×2 h at 37°C), 100%
ethanol (3 h at 37°C), 100% xylene (3×30 min at 35°C), paraffin wax
(2×30 min at 58°C), paraffin wax (30 min at 59°C), paraffin wax (30
min at 60°C) and embedding of the tissues into paraffin blocks.
Tissues were cut into 3-µm sections for histological analysis.
Tissues were stained with Mayer's hematoxylin solution for 5 min
and counterstained in eosin Y ethanol solution for 3–5 min both at
room temperature. Formalin-fixed, paraffin-embedded tissues of
bladder cancer were analyzed by immunohistochemical staining as
described previously (4,16). Sections were incubated with rabbit
polyclonal antibody to STS (HPA 002904; 1:100; Sigma-Aldrich; Merck
KGaA, Darmstadt, Germany), rabbit polyclonal antibody to E-cadherin
(sc-7870; 1:100; Santa Cruz Biotechnology, Inc., Dallas, TX, USA)
and rabbit monoclonal antibody to vimentin (D21H3; 1:100; Cell
Signaling Technology, Inc., Danvers, MA, USA) at 4°C overnight.
This was followed by incubation with biotinylated goat anti-rabbit
IgG (BA-4000; 1:200; Vector Laboratories, Inc., Burlingame, CA,
USA) for 30 min at room temperature. Immunoreactivity was detected
using a VECSTAIN Elite ABC kit (PK-6101; Vector Laboratories, Inc.)
and 3,3′-diaminobenzidine hydrochloride (Sigma-Aldrich, St Louis,
MO, USA).
Immunohistochemical analysis was performed by three
pathologists. Immunoreactivity of STS was observed in the cytoplasm
of bladder cancer cells, but not in normal urothelium. A benign
prostate tissue, which was simultaneously removed at the time of
radical cystectomy, was used as a positive control. Tissues with
>5% cancer cells immunoreactive for STS were defined as positive
(17). Evaluation of staining for
E-cadherin and vimentin were performed based on a staining index
(18,19).
Cell lines
The human bladder cancer cell lines (5637, HT1376,
UMUC3, TCCSUP and T24) and prostate cancer cell lines (LNCaP and
PC-3) were purchased from the American Tissue Culture Collection
(Manassas, VA, USA). Cells were authenticated by short tandem
repeat analysis performed by Takara Bio, Inc. (Otsu, Japan) and
tested to ensure that they were mycoplasma-free by DDC Medical
(Thermo Fisher Scientific, Inc., Waltham, MA, USA) in November
2017. Cells were maintained as monolayer cultures at 37°C and 5%
CO2. The 5637 cell line was grown in RPMI-1640
(Sigma-Aldrich; Merck KGaA) supplemented with 10% fetal bovine
serum (FBS) (Sigma-Aldrich; Merck KGaA), 1% HEPES, and 1%
D-Glucose. HT-1376 was grown in Eagle's minimal essential medium
(EMEM; Wako Pure Chemical Industries, Ltd., Osaka, Japan)
supplemented with 10% FBS, 1% sodium pyruvate solution
(Sigma-Aldrich; Merck KGaA) and 1% MEM non-essential amino acid
solution (Thermo Fisher Scientific, Inc.). UMUC3 and TCCSUP were
grown in EMEM, LNCaP and PC-3 in RPMI 1640, and T24 in McCoy's 5A
medium (Thermo Fisher Scientific, Inc.), supplemented with 10%
FBS.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Total RNA was extracted from cell lines using RNeasy
Mini kit (Qiagen GmbH, Hilden, Germany) according to the
manufacturer's instructions. RT-qPCR assay was performed as
described previously (4). The
catalogue numbers for the primers used for qPCR were as follows:
STS, Hs00996676_m1; E-cadherin, Hs01023894_m1; Vimentin,
Hs00185584_m1; GAPDH, Hs00266705_g1 (Applied Biosystems; Thermo
Fisher Scientific, Inc.). The thermocycling conditions were: 20 sec
at 95°C followed by 40 cycles of 3 sec at 95°C and 30 sec at 60°C.
Data were then quantified using the 2−ΔΔCq method for
relative gene expression (20),
compared to that of GAPDH as internal control.
Western blot analysis
Western blotting was performed as previously
described (4). Primary antibodies
for STS (1:1,000) and β-actin (ab8226; 1:1,000; Abcam, Cambridge,
UK) were used for the present study. Goat anti-rabbit horseradish
peroxidase (HRP)-conjugated IgG and goat anti-mouse HRP-conjugated
IgG (nos. sc-2004 and sc-2005; 1:10,000; Santa Cruz Biotechnology)
were used as secondary antibodies. Immunoreactive bands were
visualized using ECL Prime Western Blotting Detection reagent (GE
Healthcare, Chicago, IL, USA).
Knockdown of STS
STS expression was transiently knocked down in T24
cells using Lipofectamine™ RNAiMAX (Invitrogen; Thermo
Fisher Scientific, Inc.) according to the manufacturer's
instructions. STS-specific small interfering (si)RNAs
(Silencer® Select siRNAs) were obtained from Thermo
Fisher Scientific, Inc. The sense sequences of siRNA for STS were
as follows: si-STSA, 5′-CUAGCAACAUGGACAUAUUTT-3′; and si-STS B,
5′-GGACAUAUUUCCUACAGUATT-3′. Non-targeting control siRNA (cat. no.
4390844; Silencer® Select Negative Control siRNA) was
obtained from Thermo Fisher Scientific, Inc. T24 cells
(1.5×105) were transiently transfected with 10 nM si-STS
A, si-STS B, or control siRNA in a 6-well plate. Following 48 h,
cells were trypsinized and used in additional assays.
Cell viability assay
To investigate the effect of STS knockdown on cell
proliferation, transfectants (1×104/well) were seeded in
a 96-well plate and grown in McCoy's 5A medium supplemented with
10% FBS at 37°C with 5% CO2. After 48 h, cell
proliferation was measured using a Cell Counting Kit-8 (Dojindo
Molecular Technologies, Inc., Kumamoto, Japan) according to the
manufacturer's instructions. The number of cells was measured using
a microplate reader (Bio-Rad Laboratories, Inc., Hercules, CA, USA)
at 450 nm.
Cell migration and invasion assay
Migration assay was performed using a Cell Culture
Insert with an 8.0-µm pore size PET filter (BD Biosciences,
Franklin Lakes, NJ, USA) and invasion was assessed via a Matrigel
invasion assay (BD Biosciences), according to the manufacturer's
protocol. Briefly, 2–3×104 cells in 500 µl serum-free
McCoy's 5A medium were seeded in the upper chamber, whereas the
lower chamber was loaded with medium containing 10% FBS. Following
a 24-h incubation at 37°C, the cells that remained inside the
inserts were removed with cotton swabs, and those that migrated or
invaded the reverse side of the inserts were fixed with 5%
glutaraldehyde for 15 min and stained with Giemsa for 30 min both
at room temperature. The cells that had migrated or invaded through
the membranes were counted by light microscopy (magnification,
×20).
Statistical analysis
Statistical analyses were performed with GraphPad
Prism 7 (GraphPad Software, Inc., La Jolla, CA, USA). Fisher's
exact test was used to evaluate the differences in incidence of STS
expression patterns among clinical and pathological parameters. The
recurrence-free survival was defined as the time between the date
of surgery and the last date of follow-up or the date of
recurrence. The curves were analyzed using the Kaplan-Meier method
with the log-rank test to assess statistical significance. For
multiple analyses, Cox proportional hazards analysis was used to
determine the relative contribution of various factors to the risk
of progression. One-way ANOVA followed by a Sidak's post hoc test
was used to assess the difference between the in vitro
assays. P<0.05 was considered to indicate a statistically
significant difference.
Results
Expression of STS, E-cadherin and
vimentin in cell lines and bladder cancer samples
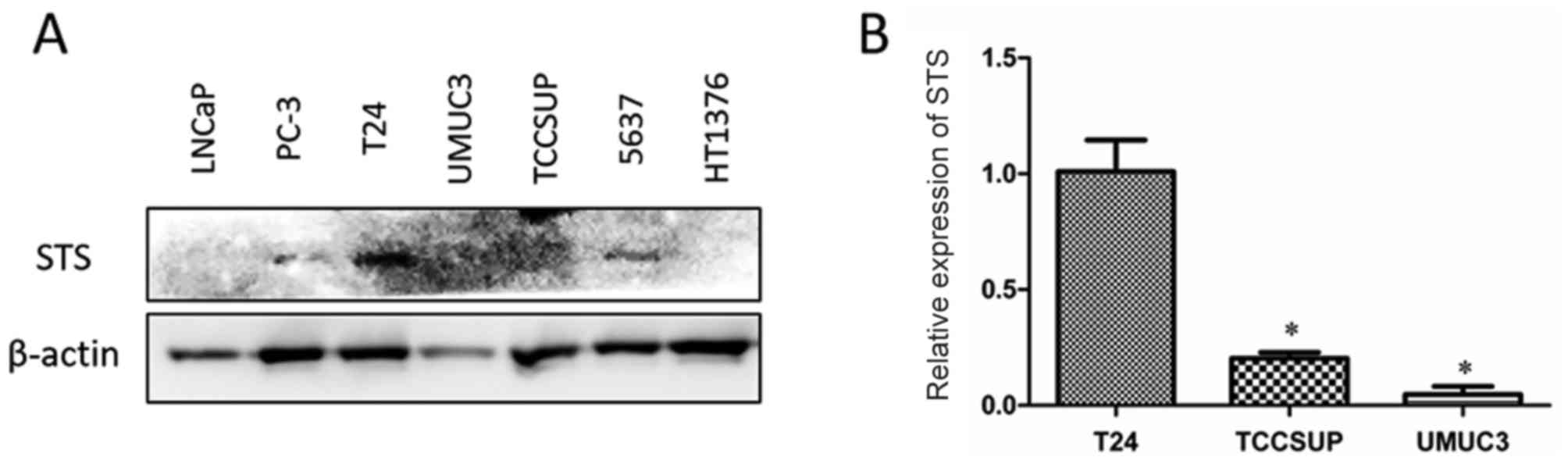
Western blot analysis demonstrated a strong
expression of STS in T24 cells, and a weak expression in PC-3 and
5637 cells, compared with those in other cell lines (Fig. 1A). The mRNA expression levels of STS
were analyzed by RT-qPCR in three bladder cancer cell lines with
invasive characteristics, T24, TCCSUP and UMUC3 cells (Fig. 1B). The expression level of STS was
significantly higher in T24 cells than in TCCSUP and UMUC3 cells;
therefore, T24 was selected for an in vitro knockdown
assay.
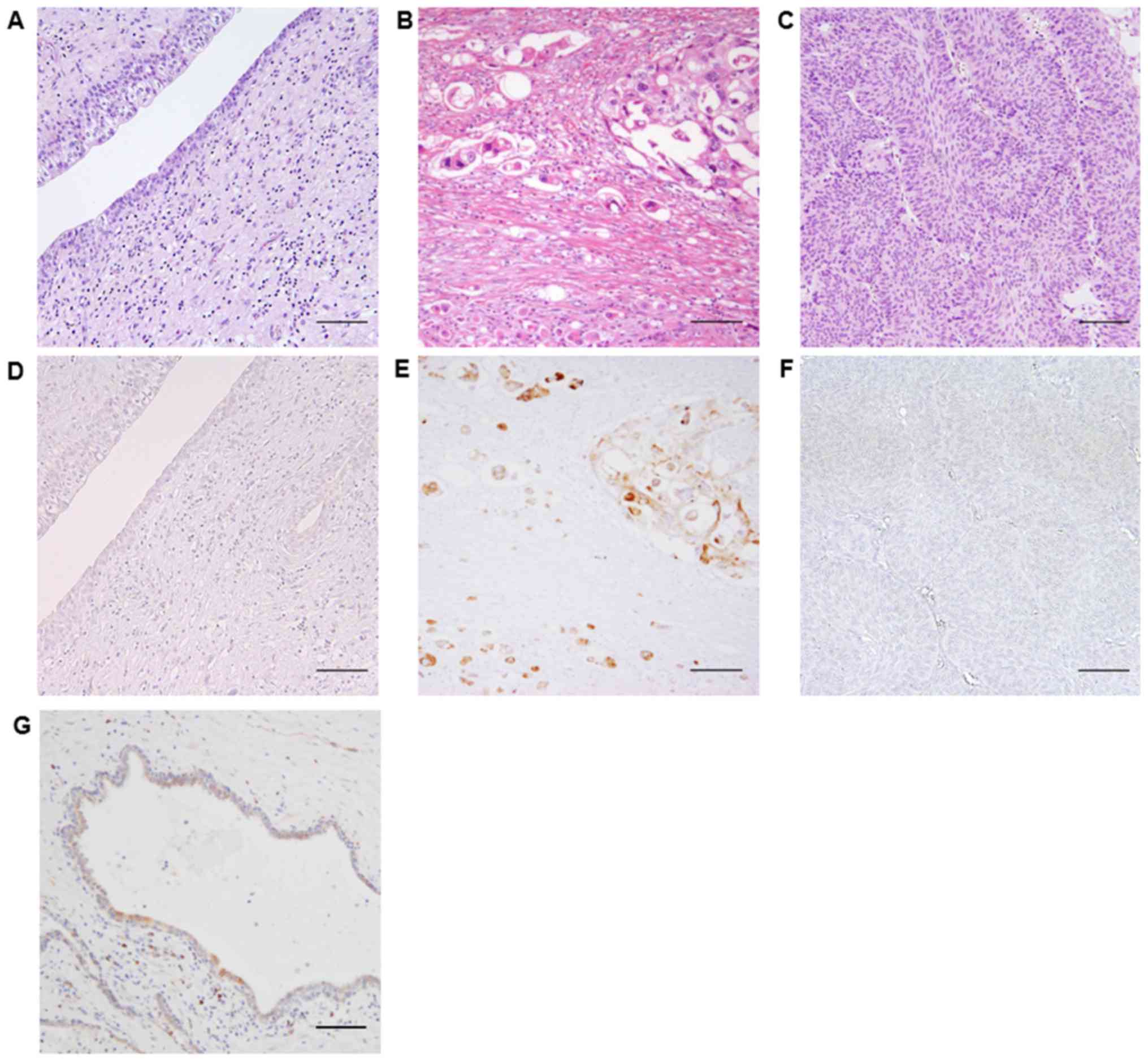
Immunohistochemical analysis of STS was performed
using 114 formalin-fixed, paraffin-embedded tissues from patients
with bladder cancers (Fig. 2).
Normal urothelium (Fig. 2A and D),
non-invasive bladder cancer (Fig. 2B and
E) and invasive bladder cancer (Fig.
2C and F) were compared with benign prostate tissue (Fig. 2G) as a positive control of STS.
Immunoreactivity of STS was observed in the cytoplasm of bladder
cancer cells in invasive areas of cancer (Fig. 2E), but not in the surface regions,
especially in papillary tumors (Fig.
2F). As summarized in Table I,
the incidence of STS-positive cancers was significantly higher in
muscle invasive bladder cancers (MIBCs; pT2 + pT3 + pT4; 37.1%)
than in non-muscle invasive bladder cancers (NMIBCs; pTa + pT1 +
pTis; 11.5%). No significant association was demonstrated with age
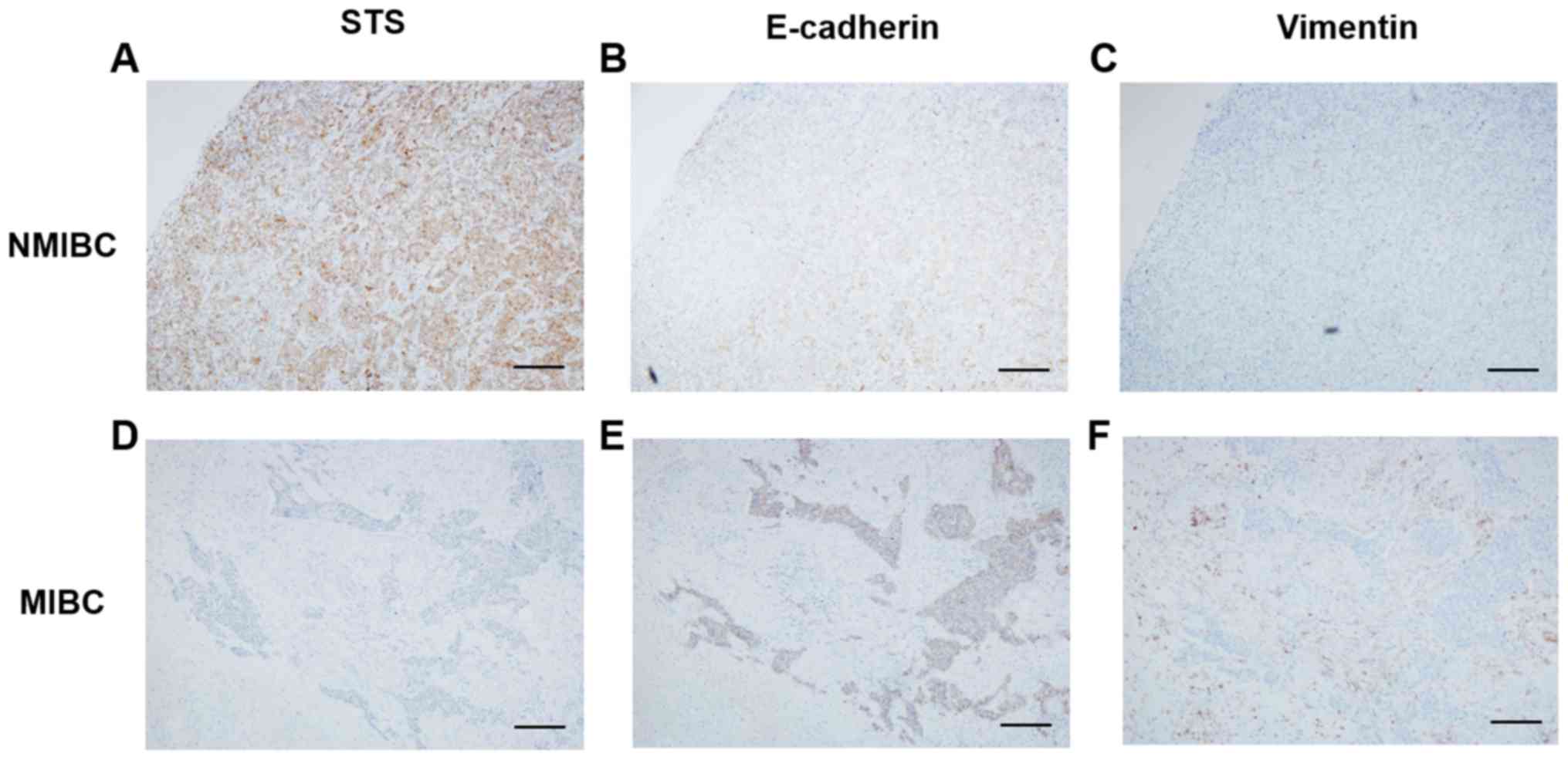
or sex. Immunohistochemical analyses of E-cadherin and vimentin
were performed using 10 NMIBC and 10 MIBC tissues to analyze the
association between STS and these EMT-related factors (Fig. 3). The expression of E-cadherin was
positive in 85% (17/20) of tissues, while vimentin was negative in
90% (18/20). There was no statistical significance in the
positivity of E-cadherin and vimentin between NMIBCs and MIBCs.
Also, no significant association was observed in the expression
between STS and these EMT-related markers (Table II).
| Table II.Association between steroid sulfatase
and epithelial-mesenchymal transition-related factors by
immunohistochemical analysis of E-cadherin and vimentin in
non-muscle-invasive bladder cancer (n=10) and muscle-invasive
bladder cancer (n=10). |
Table II.
Association between steroid sulfatase
and epithelial-mesenchymal transition-related factors by
immunohistochemical analysis of E-cadherin and vimentin in
non-muscle-invasive bladder cancer (n=10) and muscle-invasive
bladder cancer (n=10).
| A, Steroid
sulfatase positive cancers |
|---|
|
|---|
|
Parameter | Cancer
incidence, n (%) | P-value |
| E-cadherin |
| 0.531 |
|
Positive (n=17) | 9 (52.9) |
|
|
Negative (n=3) | 1 (33.3) |
|
| Vimentin |
| 0.224 |
|
Positive (n=2) | 2 (100) |
|
|
Negative (n=18) | 10 (55.6) |
|
|
| B, Muscle
invasive bladder cancers |
|
|
Parameter | Cancer
incidence, n (%) | P-value |
|
| E-cadherin |
| 0.0603 |
|
Positive (n=17) | 7 (41.2) |
|
|
Negative (n=3) | 3 (100) |
|
| Vimentin |
| 0.136 |
|
Positive (n=2) | 2 (100) |
|
|
Negative (n=18) | 8 (44.4) |
|
Follow-up of outcome in patients and
survival analysis
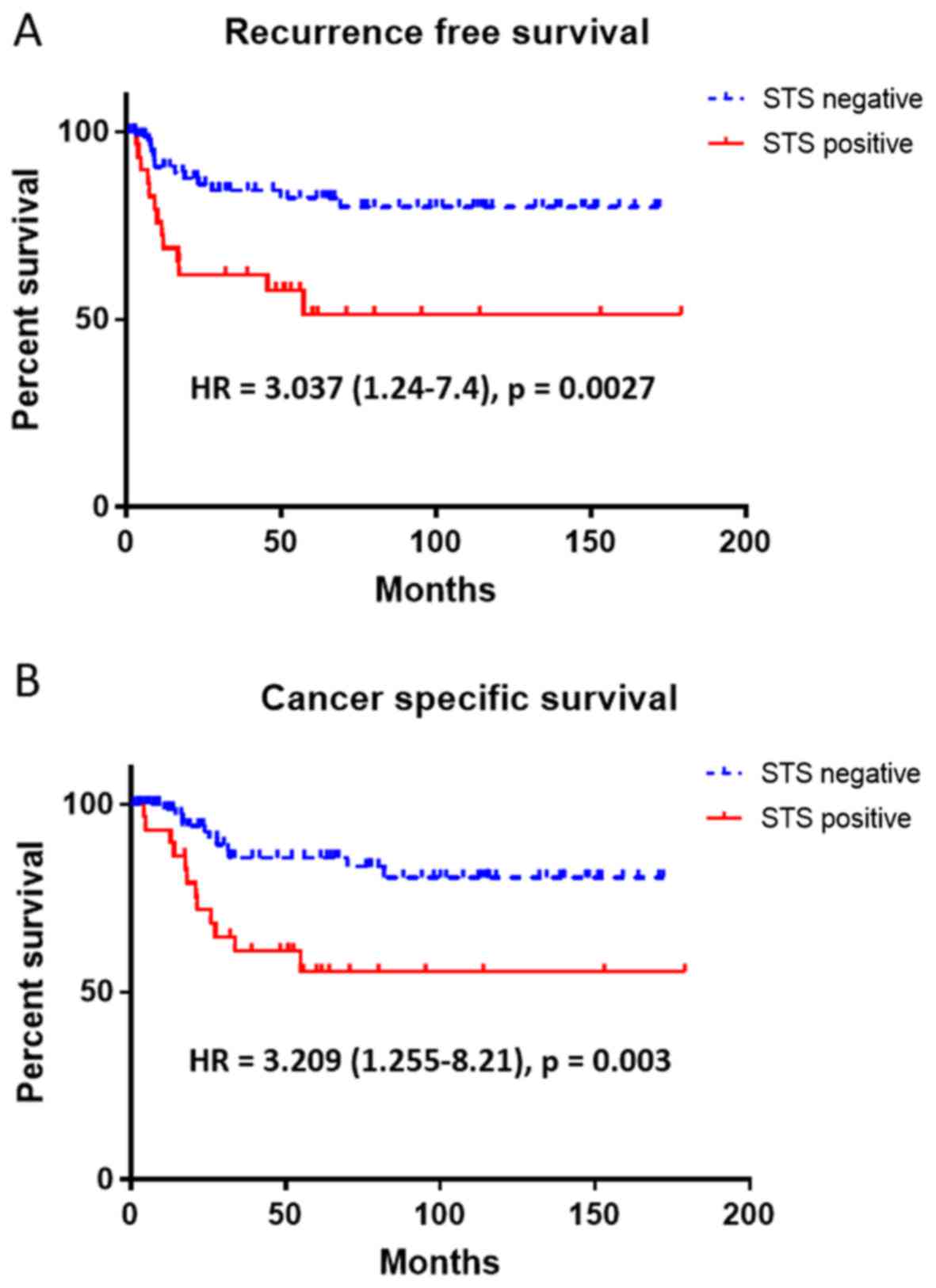
Correlation analysis of STS expression with clinical
outcomes in 114 patients with bladder cancer revealed worse
survival rates in patients with STS-positive cancer. Patients with
STS-positive cancer exhibited shorter recurrence-free survival
[RFS; Fig. 4A; hazard ratio
(HR)=3.037; P=0.0027] and cancer-specific survival (CSS; Fig. 4B; HR=3.209; P=0.003) than those with
STS-negative cancers. For patients treated with radical cystectomy,
univariate analyses of clinicopathological parameters and RFS or
CSS revealed the pathological stage (NMIBC vs. MIBC), lymph node
metastasis and STS expression as the major risk factors (Table III). Multivariate analysis
demonstrated that stage (MIBC vs. NMIBC) and positive lymph node
involvement were independent risk factors for RFS, and stage (MIBC
vs. NMIBC) was the only independent risk factor for CSS (Table IV).
| Table III.Univariate analyses of
clinicopathological parameters and the survivals of patients who
were treated with radical cystectomy (n=114). |
Table III.
Univariate analyses of
clinicopathological parameters and the survivals of patients who
were treated with radical cystectomy (n=114).
|
| Recurrence-free
survival | Cancer-specific
survival |
|---|
|
|
|
|
|---|
| Variable | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Stage | 5.977
(2.769–12.900) | 0.0002 | 7.25
(3.199–16.430) | 0.0002 |
| Grade | 1.393
(0.396–4.907) | 0.6504 | 1.44
(0.411–5.051) | 0.6195 |
| Lymph node
involvement | 5.117
(1.369–19.130) | <0.0001 | 5.439
(1.298–22.800) | <0.0001 |
| STS | 3.037
(1.247–7.400) | 0.0027 | 3.209
(1.255–8.210) | 0.0030 |
| Neoadjuvant
chemotherapy | 2.837
(1.248–6.447) | 0.0057 | 2.802
(1.381–5.683) | 0.0015 |
| Smoking
history | 1.067
(0.470–2.424) | 0.8049 | 1.471
(0.750–2.886) | 0.2433 |
| Table IV.Multivariate analyses of
clinicopathological parameters and the survival of patients who
were treated with radical cystectomy (n=114). |
Table IV.
Multivariate analyses of
clinicopathological parameters and the survival of patients who
were treated with radical cystectomy (n=114).
|
| Recurrence-free
survival | Cancer-specific
survival |
|---|
|
|
|
|
|---|
| Variable | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Stage | 4.686
(1.547–14.203) | 0.0063 | 10.004
(1.259–79.474) | 0.0294 |
| Lymph node
involvement | 2.8716
(1.287–6.410) | 0.01 | 2.023
(0.691–5.919) | 0.1983 |
| STS | 1.2496
(0.857–1.823) | 0.2472 | 1.4753
(0.895–2.436) | 0.1285 |
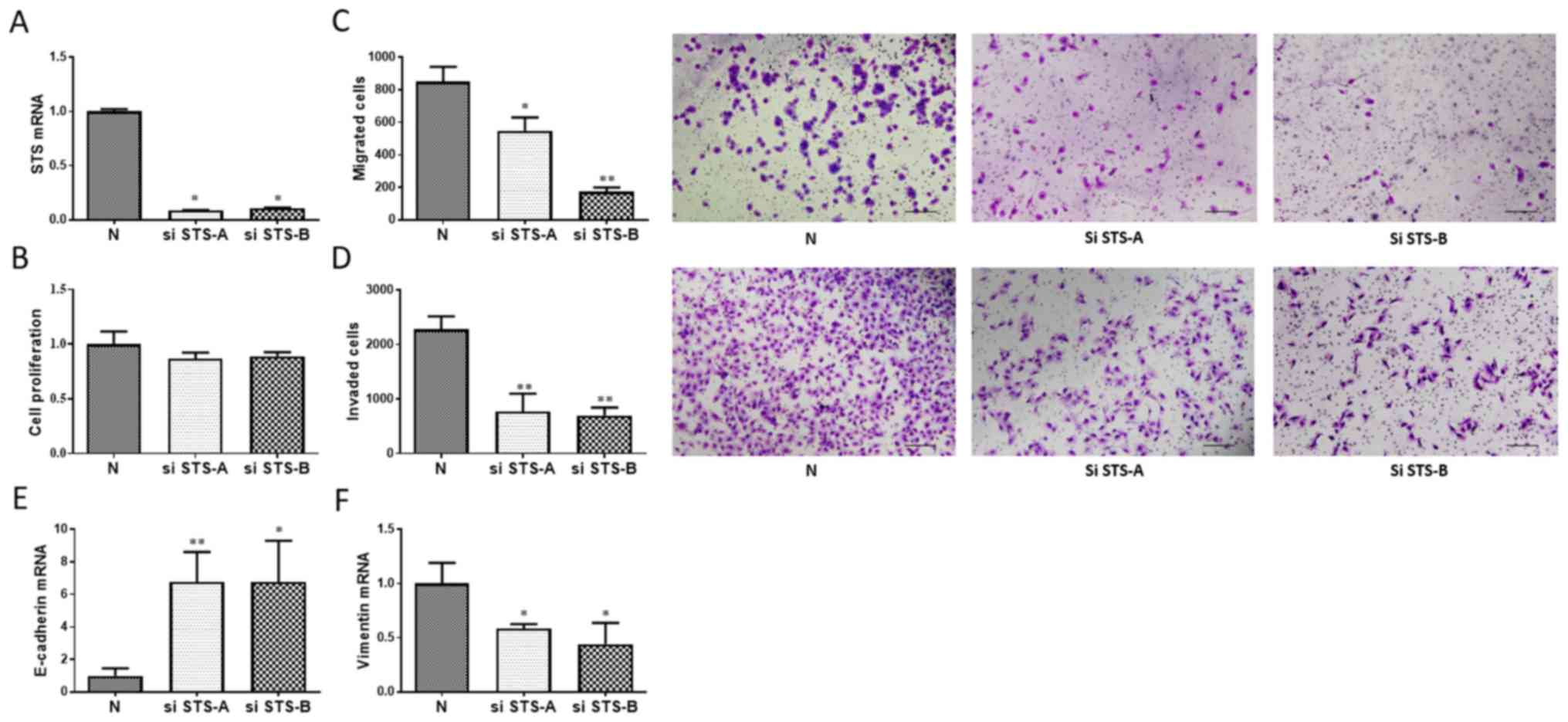
Effect of STS knockdown on cell
proliferation, migration, and invasion of bladder cancer cells
STS-specific siRNA reduced STS mRNA expression
levels by 86–90% compared with that in the negative control cells
(Fig. 5A). Knockdown of STS did not
significantly affect cell proliferation (Fig. 5B), but significantly inhibited cell
migration (35–80%; Fig. 5C) and
invasion (66–73%; Fig. 5D).
Effect of STS knockdown on the
expression of E-cadherin and vimentin
Total RNA was extracted from T24 cells transfected
with negative control siRNA, si-STS A or si-STS B. RT-qPCR
demonstrated that expression of E-cadherin was significantly
upregulated (fold change, 6.75–6.77) and that of vimentin was
significantly downregulated (fold change, 0.44–0.60) by STS
knockdown (Fig. 5E and F).
Discussion
In the present study, it was demonstrated that the
level of STS expression was significantly higher in MIBCs than in
NMIBCs. It was also demonstrated that STS-positive bladder cancers
exhibited shorter RFS and CSS. Furthermore, knockdown of STS
inhibited cell migration and invasion of bladder cancer cells, via
the regulation of E-cadherin and vimentin. To the best of our
knowledge, the present study is the first to demonstrate the
association between STS expression and invasion/progression of
bladder cancers.
Epithelial-mesenchymal transition (EMT) is the
critical process of invasion by which epithelial cells lose their
intracellular adhesion and acquire a mesenchymal phenotype
(21). Loss of E-cadherin is the
most well known change during EMT. In contrast, mesenchymal markers
such as vimentin, induce EMT (22).
In a study by McConkey et al, a strong inverse correlation
was observed between the expression of E-cadherin and vimentin in
bladder cancer (23). The present
study demonstrated that knockdown of STS inhibited the invasion
capacities of bladder cancer cells accompanied by the upregulation
of E-cadherin and downregulation of vimentin, thereby suggesting
that STS promoted invasion of bladder cancer by modifying EMT.
A major limitation of the present study, however, is
the small sample size. STS could not be indicated as an independent
prognostic factor for CSS of the patients with bladder cancer due
to the small number of cancer-specific mortalities. Also, the
association of STS and EMT-related markers could not be
demonstrated by immunohistochemistry. Unexpectedly, E-cadherin was
positive in 70% and vimentin was negative in 80% of MIBC tissues.
Alteration of the expression levels of E-cadherin and vimentin
might not occur simultaneously with the expression of STS in the
tissue of bladder cancer cells. To clarify the significance of STS
expression in clinical outcomes, further research is required.
Another limitation of the present study was that it could not
demonstrate whether the role of STS in bladder cancer invasion was
dependent on androgen/DHT signaling. Accordingly, further study on
the interaction network between STS and AR would elucidate the
behavior of STS in EMT.
With respect to the mechanism underlying the
upregulation of STS in cancers, Suh et al reported that
phosphatidylinositol 3-kinase/protein kinase B activation mediates
the induction of STS expression by tumor necrosis factor-α in human
prostate and breast cancer cells (24). Hughes et al previously
reported that stimulation of the extracellular signal-regulated
kinase (ERK)/mitogen-activated protein kinase (MAPK) pathways by
1α, 25-dihydroxyvitamin D3 may contribute to the increase in STS
expression (25). Shin et al
reported that STS induced Wnt/β-catenin signaling and EMT
transition in human prostate and cervical cancer cells (26). Further studies to evaluate
phosphatidylinositol 3-kinase/protein kinase B and ERK/MAPK
pathways would facilitate a better understanding of the role of STS
in invasive bladder cancer. In conclusion, the present study
demonstrates that STS could promote the invasion capability of
bladder cancer via regulating EMT, and could be a useful marker for
predicting the progression of bladder cancers and a novel target
for clinical therapy.
Acknowledgements
The authors are grateful to Ms. Rie Onodera, Ms.
Kaori Nakakubo, Ms. Azusa Inagaki, Ms. Keiko Sakata and Ms. Yuko
Hisabayashi (Department of Pathology, Osaka City University, Osaka,
Japan) for their technical assistance and to Ms. Yukiko Iura
(Deptartment of Pathology, Osaka City University, Osaka, Japan) for
her assistance in preparing this manuscript.
Funding
The present study was supported in part by a grant
from Grants-in-Aid for Scientific Research (grant no. 24592406),
from Japan Society for the Promotion of Science.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MK, HW, ST and MG were responsible for the
conception and design of the present study; YS, MK, MF, AK and YT
were responsible for the acquisition of data; and YS, MK, HW, TN
and MG were responsible for the analysis and/or interpretation of
data.
Ethics approval and consent to
participate
The Institutional Review Board at Osaka City
University Graduate School of Medicine (Osaka, Japan) approved the
use of the specimens and clinical data in accordance with the
Declaration of Helsinki and guidelines of Osaka City University
Graduate School of Medicine (study approval no. 1955). All 114
patients provided written informed consent for the collection and
use of their samples for the present study.
Patient consent for publication
All 114 patients included in this study provided
written informed consent for the publication of their results.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
STS
|
steroid sulfatase
|
|
RFS
|
recurrence-free survival
|
|
CSS
|
cancer-specific survival
|
|
AR
|
androgen receptor
|
|
DHT
|
dihydrotestosterone
|
|
EMEM
|
Eagle's minimum essential medium
|
|
MIBC
|
muscle-invasive bladder cancer
|
|
NMIBC
|
non-muscle-invasive bladder cancer
|
References
|
1
|
Siegel R, Ward E, Brawley O and Jemal A:
Cancer statistics, 2011: The impact of eliminating socioeconomic
and racial disparities on premature cancer deaths. CA Cancer J
Clin. 61:212–236. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hartge P, Harvey EB, Linehan WM, Silverman
DT, Sullivan JW, Hoover RN and Fraumeni JF Jr: Unexplained excess
risk of bladder cancer in men. J Natl Cancer Inst. 82:1636–1640.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hemelt M, Yamamoto H, Cheng KK and Zeegers
MP: The effect of smoking on the male excess of bladder cancer: A
meta-analysis and geographical analyses. Int J Cancer. 124:412–419.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kato M, Wei M, Yamano S, Kakehashi A,
Tamada S, Nakatani T and Wanibuchi H: DDX39 acts as a suppressor of
invasion for bladder cancer. Cancer Sci. 103:1363–1369. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Imada S, Akaza H, Ami Y, Koiso K, Ideyama
Y and Takenaka T: Promoting effects and mechanisms of action of
androgen in bladder carcinogenesis in male rats. Eur Urol.
31:360–364. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miyamoto H, Yang Z, Chen YT, Ishiguro H,
Uemura H, Kubota Y, Nagashima Y, Chang YJ, Hu YC, Tsai MY, et al:
Promotion of bladder cancer development and progression by androgen
receptor signals. J Natl Cancer Inst. 99:558–568. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shiota M, Takeuchi A, Yokomizo A,
Kashiwagi E, Tatsugami K, Kuroiwa K and Naito S: Androgen receptor
signaling regulates cell growth and vulnerability to doxorubicin in
bladder cancer. J Urol. 188:276–286. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mir C, Shariat SF, van der Kwast TH,
Ashfaq R, Lotan Y, Evans A, Skeldon S, Hanna S, Vajpeyi R, Kuk C,
et al: Loss of androgen receptor expression is not associated with
pathological stage, grade, gender or outcome in bladder cancer: A
large multi-institutional study. BJU Int. 108:24–30. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Johnson AM, O'Connell MJ, Miyamoto H,
Huang J, Yao JL, Messing EM and Reeder JE: Androgenic dependence of
exophytic tumor growth in a transgenic mouse model of bladder
cancer: A role for thrombospondin-1. BMC Urol. 8:72008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rainey WE, Carr BR, Sasano H, Suzuki T and
Mason JI: Dissecting human adrenal androgen production. Trends
Endocrinol Metab. 13:234–239. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Selcer KW, Kabler H, Sarap J, Xiao Z and
Li PK: Inhibition of steryl sulfatase activity in LNCaP human
prostate cancer cells. Steroids. 67:821–826. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Purohit A and Foster PA: Steroid sulfatase
inhibitors for estrogen- and androgen-dependent cancers. J
Endocrinol. 212:99–110. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nakamura Y, Suzuki T, Fukuda T, Ito A,
Endo M, Moriya T, Arai Y and Sasano H: Steroid sulfatase and
estrogen sulfotransferase in human prostate cancer. Prostate.
66:1005–1012. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sobin LH and Compton CC: TNM seventh
edition: What's new, what's changed: Communication from the
International Union Against Cancer and the American Joint Committee
on Cancer. Cancer. 116:5336–5339. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Montironi R and Lopez-Beltran A: The 2004
WHO classification of bladder tumors: A summary and commentary. Int
J Surg Pathol. 13:143–153. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tachibana H, Gi M, Kato M, Yamano S,
Fujioka M, Kakehashi A, Hirayama Y, Koyama Y, Tamada S, Nakatani T
and Wanibuchi H: Carbonic anhydrase 2 is a novel
invasion-associated factor in urinary bladder cancers. Cancer Sci.
108:331–337. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee WM, Jang KS, Bae J and Koh AR: The
role of steroid sulfatase as a prognostic factor in patients with
endometrial cancer. Yonsei Med J. 57:754–760. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gravdal K, Halvorsen OJ, Haukaas SA and
Akslen L: A switch from E-cadherin to N-cadherin expression
indicates epithelial to mesenchymal transition and is of strong and
independent importance for the progress of prostate cancer. Clin
Cancer Res. 13:7003–7011. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhang Q, Helfand BT, Jang TL, Zhu LJ, Chen
L, Yang XJ, Kozlowski J, Smith N, Kundu SD, Yang G, et al: Nuclear
factor-kappaB-mediated transforming growth factor-beta-induced
expression of vimentin is an independent predictor of biochemical
recurrence after radical prostatectomy. Clin Cancer Res.
15:3557–3567. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mendez MG, Kojima S and Goldman RD:
Vimentin induces changes in cell shape, motility, and adhesion
during the epithelial to mesenchymal transition. FASEB J.
24:1838–1851. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sánchez-Tilló E, Lázaro A, Torrent R,
Cuatrecasas M, Vaquero EC, Castells A, Engel P and Postigo A: ZEB1
represses E-cadherin and induces an EMT by recruiting the SWI/SNF
chromatin-remodeling protein BRG1. Oncogene. 29:3490–3500. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
McConkey DJ, Choi W, Marquis L, Martin F,
Williams MB, Shah J, Svatek R, Das A, Adam L, Kamat A, et al: Role
of epithelial-to-mesenchymal transition (EMT) in drug sensitivity
and metastasis in bladder cancer. Cancer Metastasis Rev.
28:335–344. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Suh BY, Jung JJ, Park N, Seong CH, Im HJ,
Kwon Y, Kim D and Chun YJ: Induction of steroid sulfatase
expression by tumor necrosis factor-α through phosphatidylinositol
3-kinase/Akt signaling pathway in PC-3 human prostate cancer cells.
Exp Mol Med. 43:646–652. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hughes PJ, Steinmeyer A, Chandraratna RA
and Brown G: 1alpha,25-dihydroxyvitamin D3 stimulates steroid
sulphatase activity in HL60 and NB4 acute myeloid leukaemia cell
lines by different receptor-mediated mechanisms. J Cell Biochem.
94:1175–1189. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Shin S, Im HJ, Kwon YJ, Ye DJ, Baek HS,
Kim D, Choi HK and Chun YJ: Human steroid sulfatase induces
Wnt/β-catenin signaling and epithelial-mesenchymal transition by
upregulating Twist1 and HIF-1α in human prostate and cervical
cancer cells. Oncotarget. 8:61604–61617. 2017. View Article : Google Scholar : PubMed/NCBI
|