Introduction
Tuberculosis (TB) remains a significant health
problem in developing countries and 9 million people are thought to
have developed TB in 2013 (1,2). TB may
occur at various anatomic locations and cases of tuberculous
peritonitis (TBP) are increasing (3). TBP poses a diagnostic challenge due to
the lack of specific clinical, radiological or laboratory findings
(4). Due to its excellent accuracy
and speed, direct observation of the entire peritoneal space and
allowing for multiple targeted biopsies of the suspicious lesion,
laparoscopy is the diagnostic method of choice (5–7).
However, the diagnostic failure of laparoscopy may
be as high as 14% and mainly arises from interference of adhesions
due to primary disease or previous surgery (5). Laparoscopic procedures are not
completely risk-free. Laparoscopic entry is a blind procedure,
which may pose a risk for injuries to the gastrointestinal tract
and major blood vessels when attempting to gain access to the
peritoneal cavity (8).
The central venous catheter (CVC) is a surgical tool
frequently used during cardiac anesthesia and intensive care
(9). Placement of a CVC is performed
using the Seldinger technique (10),
which is mastered by most surgeons. CVCs have also been used for
continuous drainage of peritoneal fluid (11). As the CVC set has provided easier and
safer access to the peritoneal cavity, the present study
implemented it to devise a simple and rapid method for laparoscopic
peritoneal biopsy. The present study presented a case series of
patients subjected to laparoscopic peritoneal biopsy with CVC at
our department to evaluate this novel technique for its utility and
safety.
Patients and methods
Patients
A total of 12 patients diagnosed with TBP from
October 2012 to November 2013 at the Department of
Gastroenterology, Shenzhen People's hospital (Shenzhen, China) were
enrolled in the present case series study. The inclusion criteria
were suspected TBP due to exudative ascites without a clear
pathological reason that was accompanied by a serum-ascites albumin
gradient (SAAG) of <11 g/l. The exclusion criteria included i)
ascites due to systemic illness, cirrhotic ascites, nephrotic
ascites and ascites of heart failure (SAAG of >11 g/l), ii)
abdominal trauma or acute abdominal pathology, iii) intraperitoneal
fluid of any etiology during pregnancy, iv) defective coagulation,
low platelet count (<60,000/mm3) or an international
normalized ratio of >1.5, v) previous abdominal surgery and iv)
TB confirmed through computed tomography (CT)-guided
aspiration.
The present study was approved by the Shenzhen
people's Hospital Medical Ethics Committee (Shenzhen, China). All
of the recruited patients provided written informed consent.
Data collection
The clinical features of the patients, including
their age, major symptoms and the results of TB tests were
evaluated. Prior to laparoscopy, all patients were subjected to a
purified protein derivatives (PPD) skin test, enhanced CT scan and
ascitic fluid examination. All of the patients then underwent the
modified technique for laparoscopic peritoneal diagnosis and biopsy
with CVC. Variables including time taken to undertake the
laparoscopy and duration of hospital stay were noted. All adverse
events that occurred during surgery, including severe bleeding or
bowel perforation or any adverse events occurring post-surgery were
recorded.
Clinical assessment of patients
Prior to laparoscopy, the patients were assessed by
biochemical analysis of ascites and serum tuberculosis antibodies
(TB-Ab). CT was used to assess peritoneal thickness and the
presence of nodules. A tuberculin skin test was performed using the
PPD method according to standard techniques (12). PPD tuberculin units were diluted with
sterile saline into different concentrations of ~5 tuberculin units
and 0.1 ml was intradermally injected into the volar aspect of the
left forearm. The injection area was then examined for a reaction
after 72 hours. A rash appearance was regarded as the standard
examination criterion, but local hard sections were also
considered. If a slight swelling or a needle-size red dot at the
needle injection site were present and the diameter of the hard
section was >0.5 cm, it was defined as negative reaction. If the
hard section at the injection site was between 0.5 and 1.5 cm in
diameter, it was defined as a positive reaction. If the skin
reactions around the injection site were strong or the hard section
diameter ≥1.5 cm, it was defined as strongly positive reaction.
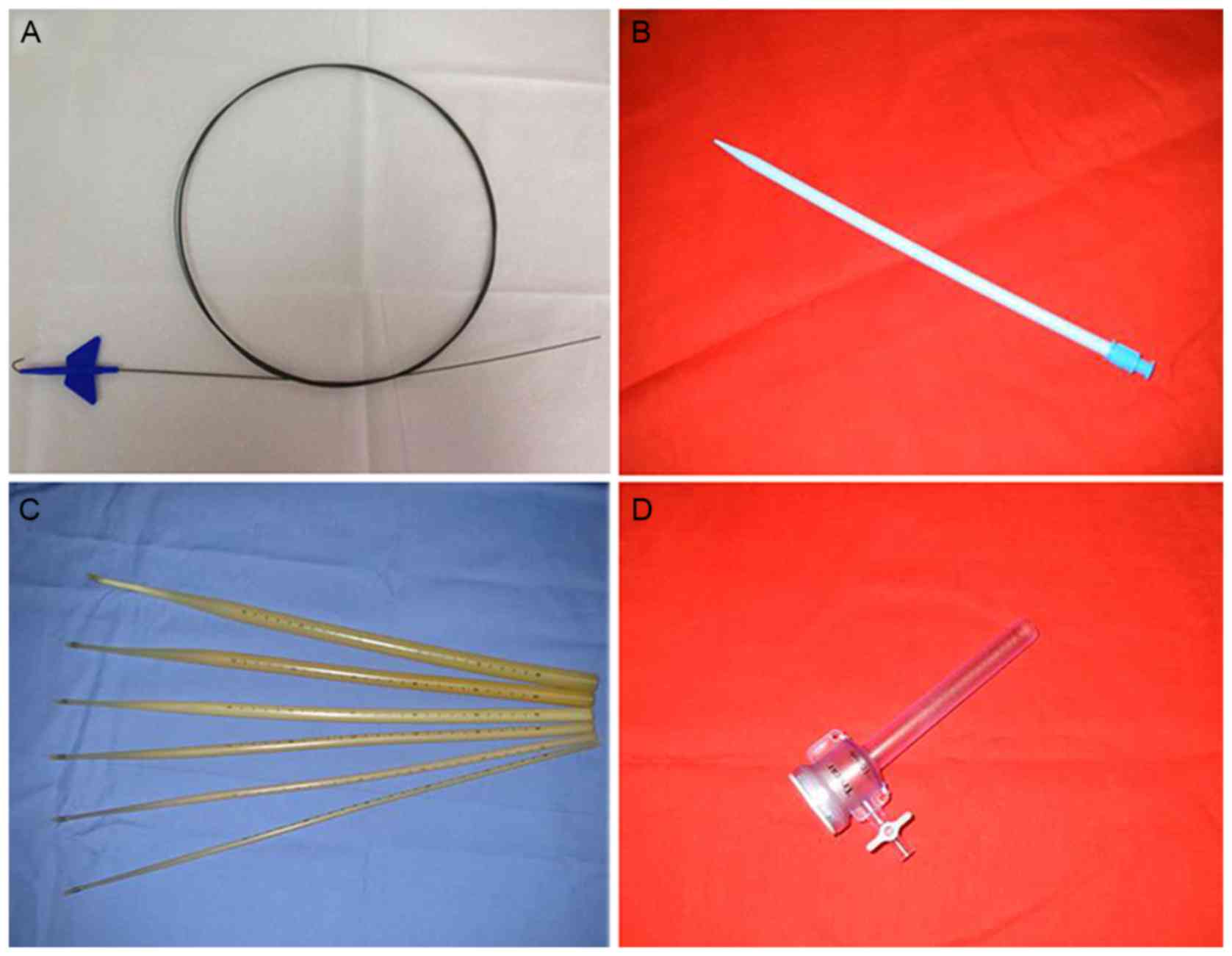
Laparoscopic method
The procedure took place in an aseptic room under
aseptic conditions. The equipment, including the guide-wire,
dilators and trocar used during the laparoscopy procedure are shown
in Figs. 1, and Fig. 2 shows the steps involved in the
procedure. The patients were placed in a supine position under
conscious sedation, which was achieved by intravenous
administration of midazolam (0.06 mg/kg) and pethidine
hydrochloride (1.2 mg/kg). An entry site was selected in the left
lower quadrant of the abdomen. The abdominal wall was cleansed with
iodine and the center of the cleansed area was tropical
anesthetized with 2% lidocaine from the local skin to the fascia.
After local anesthesia, a small incision was made in the skin and
using the Seldinger technique, a central venous catheter
(dual-chamber; 7 Fr; 20 cm) was inserted in the abdominal cavity
(Fig. 2A). CO2
insufflation was performed through the catheter (Fig. 2B) and the intra-abdominal pressure
was maintained at 8–10 mmHg. After adequate pneumoperitoneum had
been obtained, a guide-wire (260 cm in length with 3-mm flexional
leading end and a 0.035-inch diameter; Fig. 1A) was passed into the peritoneal
cavity using the Seldinger technique (Fig. 2C). In order to obtain a suitable
access tract, a 16F dilator (length, 20 cm; diameter, 4 mm;
Fig. 1B) was used to dilate the
tract through the guide-wire (Fig.
2D), and subsequently, shortened Savary-Gilliard dilators
(diameter, 5, 7 or 9 mm; length, 40 cm; Fig. 1C) were utilized to progressively
dilate the tract (Fig. 2E). A
single-use 10-mm trocar (Spekath, Foshan, China; 10-mm sleeve
sheath; 10-mm stem; Fig. 1D) was
placed over the Savary-Gilliard dilators (Fig. 2F and G). A GIF XP260 gastroscope
(Olympus Co. Ltd., Tokyo, Japan) was inserted through the trocar
into the peritoneal cavity (Fig.
2H). A detailed observation of the peritoneum and
intra-abdominal organs was performed from the left lower to the
left upper abdomen, finally to the right lower abdomen, in an
anti-clockwise direction. If there were any abnormalities such as
nodules or patches, biopsy forceps were inserted through the
endoscopic channel to perform a biopsy. When necessary, argon
plasma coagulation was used for hemostasis. After the examination
was complete, in order to monitor complications, a drainage tube
was inserted and fixed to the abdominal wall, and the trocar wounds
were sutured with stitches (Fig.
2I).
Results
Patient characteristics
Table I shows the
clinical features of the patients with TBP. The mean age of the
patients was 41 years and 33% were male. The majority of the
patients (67%) presented with ascites, including five who had an
abdominal sense of flexibility, while no abdominal mass was found.
CT results showed peritoneal thickening in five cases and
mesenteric lymph nodes in seven cases. Ascitic fluid analysis was
performed in all patients. The results are presented in Table II. Direct examination of ascitic
fluids revealed an elevation of white cells. The mean concentration
of lactate dehydrogenase (LDH) was 596.25 U/l and the serum-ascites
albumin gradient (SAAG) was <11 g/l in all patients.
 | Table I.Clinical features of the 12 patients
with tuberculosis peritonitis that underwent laparoscopy through a
central venous catheter. |
Table I.
Clinical features of the 12 patients
with tuberculosis peritonitis that underwent laparoscopy through a
central venous catheter.
| Case no. | Age (years) | Sex | Chief complaint | PPD | TB-Ab | History of pulmonary
tuberculosis | CT showed whitish
granular nodule | CT showed thickened
parietal peritoneum | CT shows
adhesions | Operation time
(min) | Severe
complications |
|---|
| 1 | 28 | F | Low fever,
ascites | P | P | P | Yes | No | No | 46 | No |
| 2 | 63 | F | Ascites | N | N | N | Yes | No | Yes | 56 | No |
| 3 | 54 | M | Ascites | N | N | N | Yes | Yes | No | 48 | No |
| 4 | 57 | F | Ascites | N | N | N | No | Yes | Yes | 52 | No |
| 5 | 37 | M | Ascites | N | P | N | Yes | No | No | 47 | No |
| 6 | 25 | F | Hiccups, ascites | N | N | N | No | Yes | Yes | 40 | No |
| 7 | 50 | F | Ascites | N | N | N | No | Yes | Yes | 49 | No |
| 8 | 37 | M | Dyspepsia | N | N | N | Yes | No | No | 48 | No |
| 9 | 45 | F | Low fever | P | P | N | Yes | No | Yes | 72 | No |
| 10 | 38 | M | Weight-loss | N | N | N | Yes | No | No | 45 | No |
| 11 | 24 | F | Ascites | N | P | N | Yes | No | No | 43 | No |
| 12 | 34 | F | Weight loss | N | N | N | No | Yes | Yes | 61 | No |
| Table II.Ascites test results for 12 patients
with tuberculosis peritonitis that underwent laparoscopy through a
central venous catheter. |
Table II.
Ascites test results for 12 patients
with tuberculosis peritonitis that underwent laparoscopy through a
central venous catheter.
| Case no. | White blood cells
(n/mm3) | Total protein
(g/l) | Albumin (g/l) | LDH (U/l) | SAAG (g/l) |
|---|
| 1 | 625 | 32 | 28 | 600 | 8 |
| 2 | 700 | 32 | 27 | 201 | 7.8 |
| 3 | 350 | 29 | 23 | 369 | 6 |
| 4 | 525 | 37 | 31 | 606 | 9.2 |
| 5 | 900 | 35 | 29 | 487 | 5.9 |
| 6 | 609 | 30 | 27 | 554 | 6.3 |
| 7 | 1,001 | 31 | 26 | 587 | 7.2 |
| 8 | 789 | 28 | 25 | 625 | 7 |
| 9 | 863 | 30 | 25 | 492 | 6.9 |
| 10 | 647 | 26 | 22 | 879 | 10 |
| 11 | 539 | 39 | 32 | 791 | 8.2 |
| 12 | 896 | 28 | 23 | 964 | 6.4 |
Evaluation of the laparoscopic
procedure
The mean operation time was 50.6 min (range, 40–72
min), the median duration of hospital stay was 7 days (range, 5–10
days). The bleeding volume ranged from 0–50 ml. The post-operative
drainage time was 3 days.
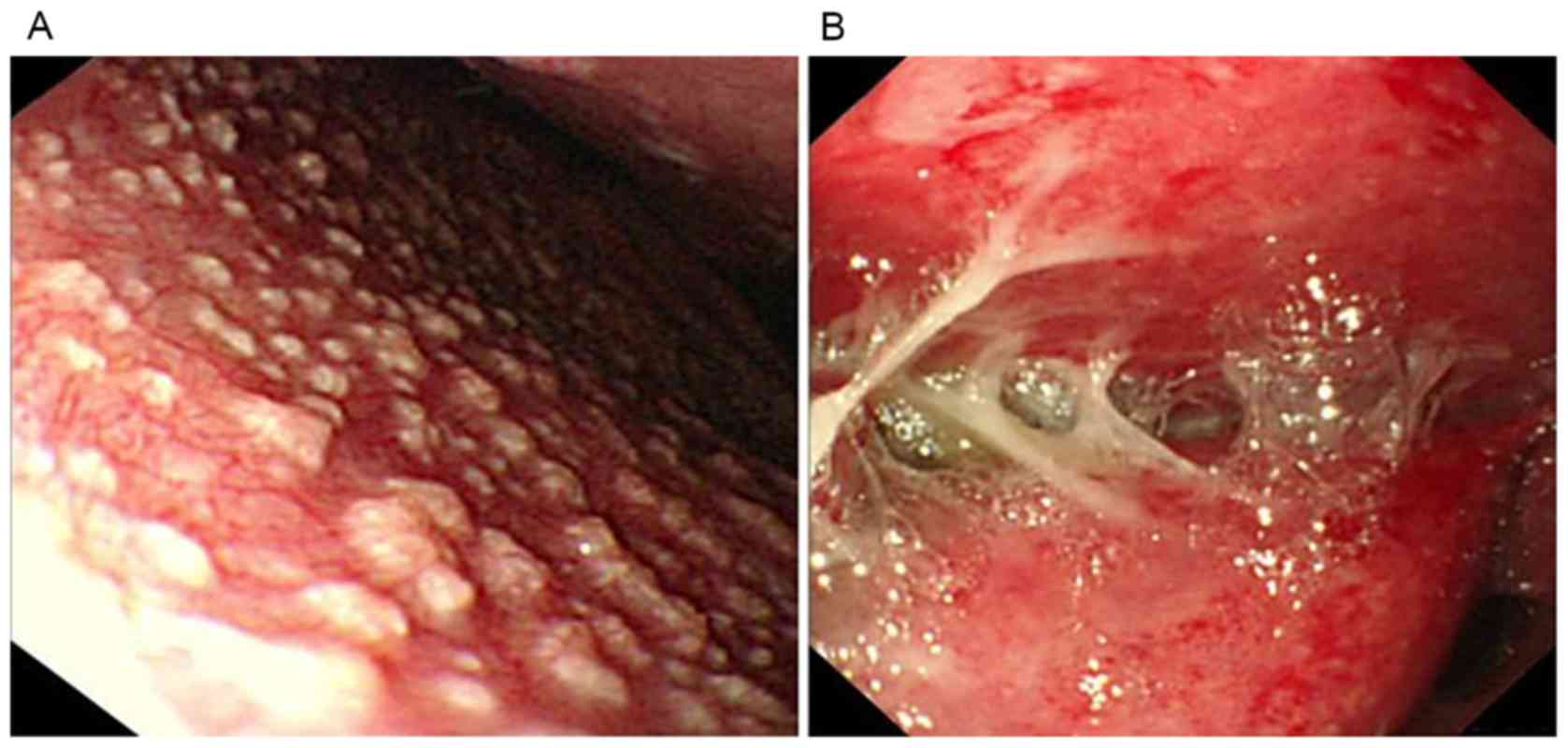
Diagnostic laparoscopy was completed in all 12
patients with TBP. Examples of images from the laparoscopy are
shown in Fig. 3. Certain patients
presented with thickened, hyperemic peritoneum with ascites and
whitish granular nodules (<5 mm) scattered over the peritoneum
(Fig. 3A). Furthermore, markedly
thickened parietal peritoneum, at times with yellowish nodules and
caseous material or multiple thickened adhesions were observed in
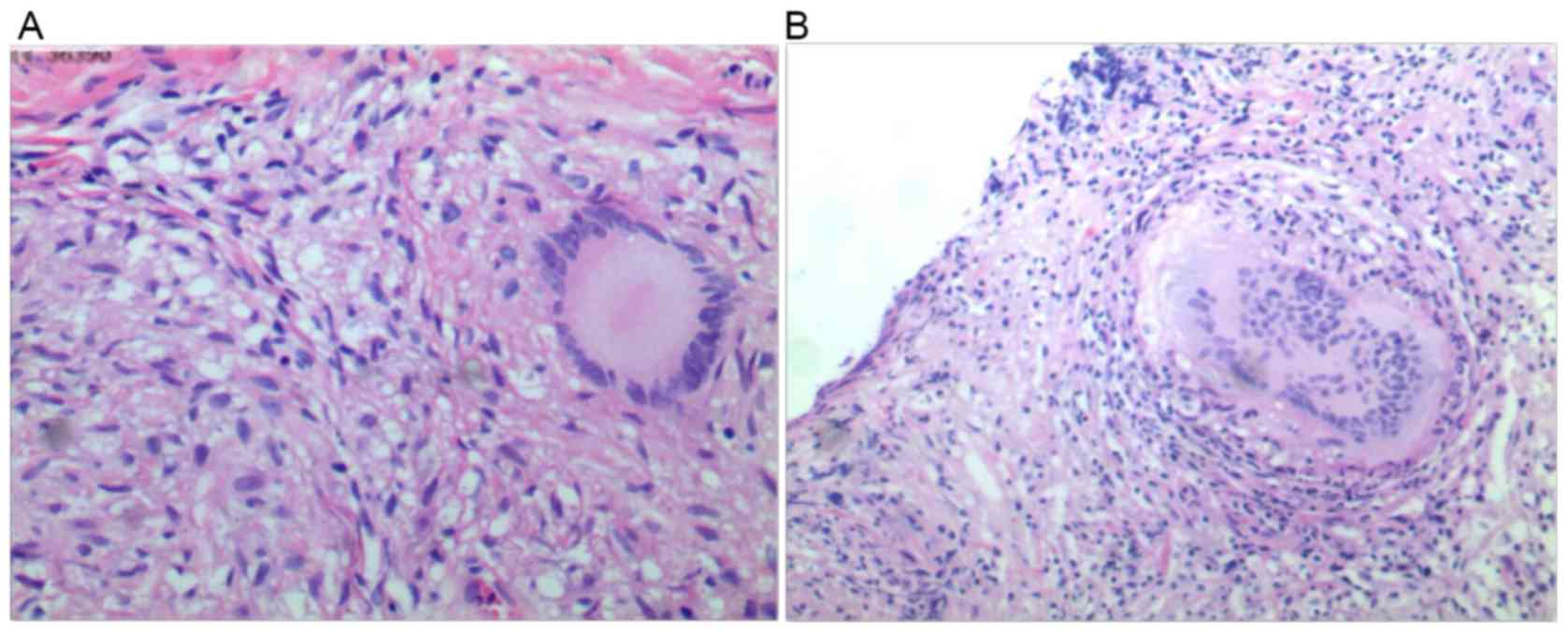
certain patients (Fig. 3B). Targeted
biopsies were taken from all of the patients and revealed caseous
granulomatous inflammation, which is the pathological diagnostic
criterion for TBP. Examples of typical histological samples for
caseous necrosis and granulomas with epithelioid cells are shown in
Fig. 4.
All of the patients tolerated the examination
without any severe intra- or post-operative severe complications,
such as significant bleeding or digestive tract perforation.
Discussion
The aim of the present case series was to evaluate a
novel laparoscopic method using a CVC for patients with TBP. The
procedure was successfully undertaken in all 12 patients and all of
the patients tolerated the examination without any severe intra- or
post-operative complications. The mean operation time was 50.6 min
and the median duration of hospital stay was 7 days.
Laparoscopic diagnosis with biopsy allows for fast
and accurate diagnosis of TBP, which is important for early
treatment and better patient prognosis (13). Although in certain situations,
laparoscopic diagnosis alone may provide false positive rates in
18%, these are avoided when supported with histopathology and
ascitic fluid analysis (14).
Conventionally, there are two methods of entry into the peritoneal
cavity: The closed technique (Veress needle) and the open technique
(Hasson technique) (15). There is
no clear consensus for the best method, while Veress needle
insertion is the most popular technique (16).
Meta-analysis and large multicenter studies have
reported an incidence of vascular and bowel injury caused by Veress
needles and subsequent trocars of 0.2 and 0.4 per 1,000,
respectively (17), and a small
number of complications associated with mortality occurred
(18). In addition, the conventional
methods have other limits: The techniques require a long time to
perform, have a high cost and require endotracheal intubation and
mechanical ventilation. Furthermore, they are techniques performed
only by surgeons. In terms of TBP specifically, certain patients in
whom adhesions occur during the disease course may require
conversion to laparotomy as insertion becomes restricted (19). This problem is likely to become more
evident as the disease progresses, making it safer to perform
laparoscopy during the earlier stages of TBP (20).
From 2006, laparoscopy has been applied to patients
with TBP by entry through the umbilicus under conscious sedation,
but the rate of complications was found to be higher in patients
with TBP due to Mycobacterium tuberculosis-induced
peritoneal adhesions. In 2007, our group reported our experience
with natural orifice transluminal endoscopic surgery (NOTES)
applied to TBP (21). NOTES allows
access into the abdominal cavity through a natural orifice
(22). However, this method requires
to be performed by an experienced endoscopist. Hence, a novel
method for laparoscopic diagnosis and peritoneal biopsy with CVC
was introduced in our hospital in 2012. The average time taken for
the procedure was 50.6 min. All of the patients underwent an
uneventful course. No complication occurred, regardless of the
level of adhesions. This method allowed us to make a correct
diagnosis within four days. The method clearly displays the point
which allowed for direct entry into the peritoneal cavity in the
majority of the cases, while the abdominal wall is distant from the
underlying viscera and vessels at all times. After entering into
the peritoneal cavity, the flexible laparoscope is conveniently
controlled, allowing for careful observation of the peritoneum,
intra-abdominal organs and mesentery. If necessary, it was possible
to perform direct biopsies. This method was found to have the
following potential benefits: i) Entry-associated injury, such as
gastrointestinal tract perforation and bleeding rarely occur. ii)
It is easy to learn and quick to perform, particularly for a
physician. iii) The flexible laparoscope has a wide-angel lens with
high definition and reversal, which allows for convenient
observation of the peritoneum and intra-abdominal organs. iv) It
may shorten the patient's hospital stay and reduce the cost, which
is important in a developing country.
The present study has certain limitations: As the
patient cohort was relatively small, the number of complications
was expected to be low. As the study only reported on a case series
and was not a randomized controlled trial, allowing comparison with
other techniques, the potential benefits require to be demonstrated
in further studies.
In conclusion, the novel method of laparoscopy with
CVC was safe and effective in the present case series.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
RZ, ZX, YZ performed the surgical procedures. RS
analyzed and interpreted the patient data. LW, YM performed and
analyzed ascites tests. JY, DZ, ML performed the histological
examination. RZ was a major contributor in writing the manuscript.
All authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Shenzhen
people's Hospital Medical Ethics Committee (Shenzhen, China). All
of the recruited patients provided written informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Corbett EL, Watt CJ, Walker N, Maher D,
Williams BG, Raviglione MC and Dye C: The growing burden of
tuberculosis: Global trends and interactions with the HIV epidemic.
Arch Intern Med. 163:1009–1021. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
WHO: Global Tuberculosis Report 2014.
World Health Organization, Geneva, Switzerland. 2014.
|
|
3
|
Mas MR, Comert B, Sağlamkaya U, Yamanel L,
Kuzhan O, Ateşkan U and Kocabalkan F: CA-125; a new marker for
diagnosis and follow-up of patients with tuberculous peritonitis.
Dig Liver Dis. 32:595–597. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Inadomi JM, Kapur S, Kinkhabwala M and
Cello JP: The laparoscopic evaluation of ascites. Gastrointest
Endosc Clin N Am. 11:79–91. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sanai FM and Bzeizi KI: Systematic review:
Tuberculous peritonitis-presenting features, diagnostic strategies
and treatment. Aliment Pharmacol Ther. 22:685–700. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Krishnan P, Vayoth SO, Dhar P, Surendran S
and Ponnambathayil S: Laparoscopy in suspected abdominal
tuberculosis is useful as an early diagnostic method. ANZ J Surg.
78:987–989. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang WN, Wallack MK, Barnhart S, Kalani AD
and Storrs SL: Tuberculous peritonitis: Definitive diagnosis by
laparoscopic peritoneal biopsy. Am Surg. 74:1223–1224.
2008.PubMed/NCBI
|
|
8
|
Varma R and Gupta JK: Laparoscopic entry
techniques: Clinical guideline, national survey, and medicolegal
ramifications. Surg Endosc. 22:2686–2697. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cotogni P and Pittiruti M: Focus on
peripherally inserted central catheters in critically ill patients.
World J Crit Care Med. 3:80–94. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Higgs ZC, Macafee DA, Braithwaite BD and
Maxwell-Armstrong CA: The Seldinger technique: 50 years on. Lancet.
366:1407–1409. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mercadante S, Intravaia G, Ferrera P,
Villari P and David F: Peritoneal catheter for continuous drainage
of ascites in advanced cancer patients. Support Care Cancer.
16:975–978. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nayak S and Acharjya B: Mantoux test and
its interpretation. Indian Dermatol Online J. 3:2–6. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chahed J, Mekki M, Mansour A, Ben Brahim
M, Maazoun K, Hidouri S, Krichene I, Sahnoun L, Jouini R, Belgith
M, et al: Contribution of laparoscopy in the abdominal tuberculosis
diagnosis: Retrospective study of about 11 cases. Pediatr Surg Int.
26:413–418. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wani M, Mir SA, Bhat JA and Moheen HA:
Ancillary tests to improve the accuracy of laparoscopy in the
diagnosis of tuberculous peritonitis. Can J Surg. 57:E542014.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vilos GA, Ternamian A, Dempster J and
Laberge PY: CLINICAL PRACTICE GYNAECOLOGY COMMITTEE: Laparoscopic
entry: A review of techniques, technologies, and complications. J
Obstet Gynaecol Can. 29:433–447. 2007.(In English, French).
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Merlin TL, Hiller JE, Maddern GJ, Jamieson
GG, Brown AR and Kolbe A: Systematic review of the safety and
effectiveness of methods used to establish pneumoperitoneum in
laparoscopic surgery. Br J Surg. 90:668–679. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chu CM, Lin SM, Peng SM, Wu CS and Liaw
YF: The role of laparoscopy in the evaluation of ascites of unknown
origin. Gastrointest Endosc. 40:285–289. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Schäfer M, Lauper M and Krähenbühl L:
Trocar and veress needle injuries during laparoscopy. Surg Endosc.
15:275–280. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Abdelaal A, Alfkey R, Abdelaziem S,
Abunada M, Alfaky A, Ibrahim WH, Toro A and Di Carlo I: Role of
laparoscopic peritoneal biopsy in the diagnosis of peritoneal
tuberculosis. A seven-year experience. Chirurgia (Bucur).
109:330–334. 2014.PubMed/NCBI
|
|
20
|
Miyaoka H, Uesugi K, Shigematsu S, Miyake
T, Furukawa E, Okita S, Okada T, Abe M, Murakami H, Matsuura B, et
al: Clinical course of tuberculous peritonitis determined by
laparoscopy. Intern Med. 49:293–297. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhu H, Li Y, Wang L, Shi R, Huang X, Wang
Q and Luo W: Trans-gastric peritoneoscopy with technique of
natural-orifice transluminal endoscopic surgery for diagnosis of
tuberculosis peritonitis: A report of 20 cases. Chin J Dig Endosc.
28:252–255. 2011.(In Chinese).
|
|
22
|
Song S, Itawi EA and Saber AA: Natural
orifice translumenal endoscopic surgery (NOTES). J Invest Surg.
22:214–217. 2009. View Article : Google Scholar : PubMed/NCBI
|