Introduction
Extensive bone defect is frequently encountered in
the treatment of orthopedic trauma, tumors, infection and some
congenital diseases and it is hard to deal with. The traditional
methods for bone defect repair, such as autogenous, allogeneic and
heterogeneous bone transplantations, are clinically limited since
extra trauma can be caused, and there is limited supply and
immunogenicity thereof. However, the bone tissue engineering
technology with the model of ‘scaffolding material plus seed cell
plus growth factor’ provides a new pathway for solving the above
problems (1). Scaffolding material
with both the osteoconduction and osteoinductivity has been used to
load autologous seed cells for repairing the extensive bone defect.
This solves the clinical issue, improves technological and
industrialization development, leading to significant socioeconomic
benefits.
The interaction between angiogenesis and
osteogenesis is a complex process when considering the growth and
development of bones and regeneration and repair of bone trauma. So
far the key factor for the difficult repair of extensive bone
defect is the deficiency in sources of blood supply of specific
anatomic sites. Therefore, the tissue-engineered bone
vascularization is the base to ensure the survival of the
transplants, and constitutes the key technology for the bone tissue
engineering (2–4). Given that the decalcified bone
scaffolds reserve the natural network multi-pore structure of
cancellous bone, they are well-characterized by degradability and
biocompatibility (5). In order to
further study the transplantation effect of decalcified bone
scaffolds after pre-vascularization, the bone defect repair in the
posterior limbs of mice implanted with pre-vascularization
decalcified bone scaffolds in vitro and non-treatment
decalcified bone scaffolds, and the osteogenic efficiency for the
two scaffold materials were evaluated.
Materials and methods
Experimental materials
A total of 21 male Sprague-Dawley (SD) mice (8–12
weeks old, weighing 250–350 g) were obtained from Beijing Vital
River Laboratory Animal Technology, Co., Ltd. (Beijing, China). All
mice were housed in controlled conditions (12 h light/dark cycle,
22±0.5°C, 50–60% relative humidity) and they were fed with
commercial rodent chow and tap water ad libitum. After 7
days of adaptive feeding, the mice were randomly divided into group
A, B and C. Decalcified bone scaffolds with pre-vascularization
in vitro and decalcified bone scaffolds were used.
Experimental methods
Thigh bone defect model of mice and material
implantation were prepared. Twenty-one SD mice were randomly
assigned to group A, B and C, and anesthesia was induced with
intraperitoneal injection of 2% of pentobarbital sodium (0.02
ml/100 g). After local hair cropping in the right posterior limb of
each mouse and disinfection with iodophor, the operating knife was
used to cut the muscle layer open. Kirschner wire was adopted to
make a bone defect area of ~1.5 cm in length in the thigh bone.
Decalcified bone scaffolds with pre-vascularization in vitro
were implanted in the broken bones for group A; decalcified bone
scaffolds were implanted in the broken bones for group B; and no
material was implanted for group C. Tight suturing of all layers
was carried out followed by disinfection. Intramuscular injection
with 40,000 units of penicillin G and sodium salt was given into
the thigh after the operation and the mice were fed in separate
cages. The study was approved by the Ethics Committee of the
Affiliated Yantai Yuhuangding Hospital of Qingdao University
(Yantai, China).
Gross observation
The postoperative daily life of mice was observed.
At 4 weeks after operation the sacrifice of all groups of mice was
conducted, and the sites with implanted materials were opened layer
by layer. The peripheral tissues and the growth of the injured
parts were observed.
Imaging observation
After the sacrifice of mice (4 weeks) the
corresponding posterior limbs of all mice were taken down, and
micro-CT (SkyScan 1176; Bruker microCT, Kontich, Belgium) was
performed to scan the thigh bones of mice (scanning resolution: 18
µm, rotation angle: 360°, increase of rotation angle: 0.72°,
voltage: 88 kV, power: 40 W, electric current: 80 µA, average
number of frames: 6, binning: 1×1). Then, the repair of sites with
bone defect was observed in all groups to determine whether they
had synostosis and bone tissue molding.
Histopathological examination
The thigh bones of mice were taken after the
sacrifice of mice, at 4 weeks after operation, and peripheral
muscle tissues of bone tissues were removed. Neutral formalin (10%)
was used for fixation for 3 days, after which 10% of
ethylenediamine tetraacetic acid (EDTA, pH 7.2) was used for
decalcification for 1 month. Then, the sections were
paraffin-embedded and H&E and Masson's staining was performed.
New bone formation, inflammatory response, bone cell growth,
angiogenesis, material degradation, calcium deposition and ossein
growth were observed.
Results
Gross observation and analysis
results
The mice woke 30 min after the operation. On the day
of operation all sites moved freely except for the operation site,
and normal feeding was observed. After several days of
postoperative observation, no infection was shown in the sutured
sites, good healing was observed and there were no deseased mice,
indicating a successful operation of material implantation and good
biocompatibility for the materials without inducing any
immunological rejection. After the sacrifice of the mice, the
operation site was opened layer by layer. No swelling and water
percolation were observed, and normal growth of the muscular
tissues was shown, further suggesting good biocompatibility of the
materials. In group A, the defect areas of the thigh bones of all
mice were healed with no obvious difference from the other bone
tissues, and the implanted scaffolds had completely degraded. In
group B, the defect areas of the thigh bones of all mice were
basically healed, and the regenerated bone tissues in other defect
areas had no obvious differences from the other bone tissues,
except for that part of cortical bones that were completely
repaired, and the implanted scaffolds had completely degraded. In
group C, the defect areas of the thigh bones of all mice were
filled with fibrous tissues, and no similar structure of bone
tissues was observed in the defect areas. The results showed that
osteanagenesis occurred in the defect areas of the thigh bones of
the mice in group A, and bone defect areas were completely replaced
by new bone tissues, suggesting a complete repair for defect areas.
Steanagenesis also occurred in the defect areas of the thigh bones
of mice in group B, and most of bone defect areas were replaced by
new bone tissues, suggesting a basic repair for defect areas. In
group C, no osteanagenesis occurred in the defect areas of thigh
bones of mice, and bone defect areas were replaced by muscular
tissues or fibrous tissues.
Imaging observation and analysis
results
Fig. 1 shows the
three-dimensional reconstruction of defect areas scanned by
micro-CT. As can be seen from Fig.
1A, the defect area was not obvious in group A and it was
completely replaced by new bone tissue. Full connection of cortical
bone was shown and no development for implanted materials was
observed, indicating a complete degradation of the materials.
Fig. 1B shows that the edge of bone
defect area was not obvious in group B and most areas were replaced
by new bone tissues. The cortical bone showed no full connection,
and no development was observed for implanted materials, indicating
a complete degradation of materials. Fig. 1C shows that a small number of new
bone tissues were formed in the edge of bone defect area in group
C, the defect area was obvious, and it was not filled or replaced
by new bone tissues. The results revealed that the decalcified bone
scaffolds with pre-vascularization in vitro implanted in the
bone defect areas of mice can quickly induce the blood into the
inner scaffold and provide abundant nutrient substances and
mesenchymal stem cells for the defect areas, benefiting the
differentiation of mesenchymal stem cells into osteoblasts and
osteanagenesis in defect areas. Owing to the reservation of three
dimensional structure and collagen scaffold of original bone
tissues, the treated decalcified bone scaffolds can provide better
scaffold for cell crawling with the same and better effect of
inducing osteogenesis. However, it was lower in the effect of
inducing osteogenesis as compared with decalcified bone scaffolds
with pre-vascularization in vitro.
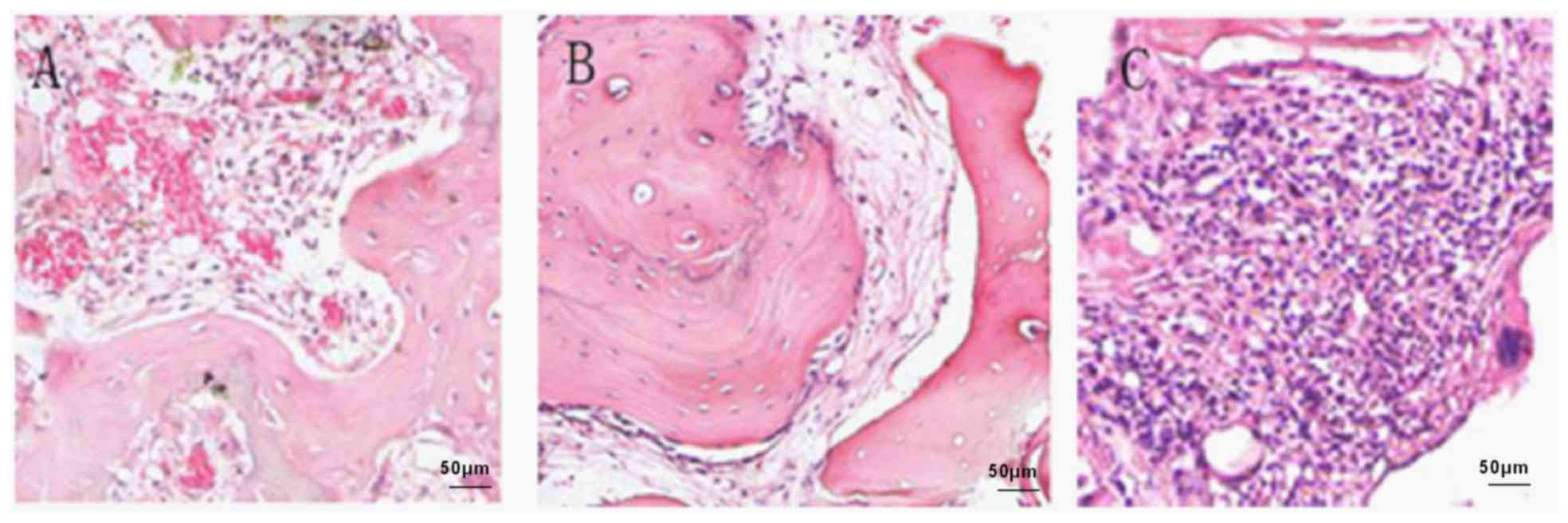
Histopathological examination and
analysis results
To evaluate the repair of sites with bone defect,
sampling was conducted using H&E staining detection, the
results of which can be seen in Fig.
2. At 4 weeks after operation, the mice in groups A and B
showed an obvious recovery sign, osteoblasts were shown in the
peripheral area, and a small number of structures of bone
trabeculas and marrow cavity with no complete remodeling were
observed (Fig. 2A and B). The
scaffold materials in group A (Fig.
2A) were completely degraded and absorbed, the aggregation of
vast osteoblasts and undifferentiated mesenchymal cells was seen in
the surface of new bones, and connective tissues accompanied by
abundant angiopoiesis were observed in the periphery. A relatively
small number of new-born bones grew into the implanted bones in a
finger-like form with basically no neovascularization in group B
(Fig. 2B). The blank control group
with no implantation of material (Fig.
2C) showed no sign of repair. Plenty of fat vacuoles, fibrous
tissues and other tissues had filled the defect areas, preventing
the process of bone repair. The implantation of pre-vascularization
decalcified bone scaffolds and decalcified bone scaffolds not only
promoted the adhesion, recruitment and growth of osteoblasts in the
initial stage of repair, but also prevented the invasion of cells
and tissues (such as epithelial cells, fibroblasts or connective
tissues) irrelevant to osteogenesis to some extent, providing a
favorable growing environment for the bone repair. No inflammatory
cell infiltration was observed in any of the groups.
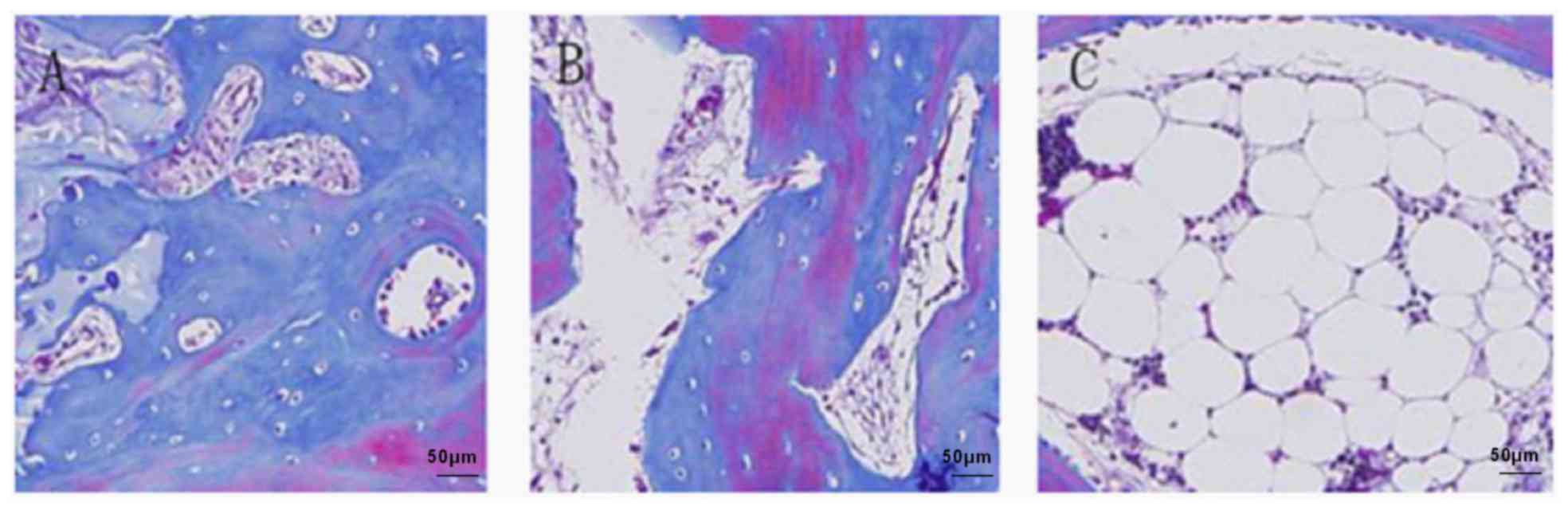
After the samples receiving Masson's compound
staining, the collagenous fiber was showed baby blue, new bone
blue, cell nucleus black blue, erythrocyte salmon pink and
decalcified bone red (Fig. 3). In
the 4th week after implantation, obvious bone repair signs and
accumulation of collagenous fiber tissues were shown in the defect
sites of the mice in groups A and B and vast new bone tissues had
filled the defect sites and had better integration with peripheral
normal old bone tissue. In group A (Fig.
3A) the repair effect was relatively better than group B
(Fig. 3B), an obvious absorption of
scaffold materials was shown, more new bones and abundant vascular
proliferation. However, for the blank control group (Fig. 3C) with no implantation of any
material, some fibrous connective tissues had accumulated in the
defect sites and the sign of bone repair was not obvious. This
experiment further showed that decalcified bone scaffolds with
pre-vascularization treatment implanted in the bone defect sites
have better repair effect and osteoconductive regeneration
capacity.
Discussion
With the continuous development of bone tissue
engineering technology, the extensive bone defect repair by use of
tissue-engineered bone has been a current research hotspot
(6–8). Considerable number of theories and
techniques have been accumulated in the field of bone tissue
engineering. However, the speed and quality of structuring
tissue-engineered bones using the existing technologies do not meet
the clinical requirements, limiting further development and final
clinical application of bone tissue engineering. The important
reason is that the existing technologies cannot ensure the early
survival in vivo of seed cells loaded by scaffold materials,
thereby exerting an influence on its long-term osteogenic
efficiency in vivo.
An effective way for solving the above problems is
abundant vasoganglions formed quickly within scaffold materials
(8,9). The seed cells need to take in oxygen
and nutrient substances through blood vessel and transfer
metabolites. For extensive bone defects, larger volumes of
implanted tissue-engineered bone are needed, so the vascularization
in the scaffold materials can play a vital role. A study has shown
that osteoblasts can only survive in the region, 100 µm away from
blood vessel (10). Therefore, the
way to build the vascularized tissue-engineered bone in a fast and
effective way has become a hot issue.
Researchers worldwide have put forward some methods
of vascularization construction from the perspectives of three
elements of tissue engineering, such as seed cells used for the
construction of blood vessel and bone jointly implanted in scaffold
materials, the adoption of growth factors for stimulating or
relevant genes for transfecting seed cells, and the preparation of
biological materials suitable for the angiogenesis. Although, some
effects have been achieved, an effective way for building
tissue-engineered bone with full vascularization is lacking, and
the reason for this is that peripheral capillaries had not grown in
the early stage when tissue-engineered bone was implanted in
vivo. This stage is important for the seed cell survival and
proliferation, and there is a certain time difference between the
vascularization and osteogenesis. Some studies used the property of
the vascular endothelial cells to form immature tubular structures
in the scaffold materials and implanted the endothelial cells in
the scaffold materials in advance, and after certain vasoganglions
were formed in vitro, they were implanted in vivo to
build tissue-engineered skins (11).
It was observed that the tubular structure can fuse and crosslink
with autologous vessels of the host. Some scholars applied this to
the construction of tissue engineered bone and the method of
‘pre-implantation’ of vascular endothelial cells was adopted for
‘pre-vascularization’ of scaffold materials (12). This novel method has provided a new
idea for solving the problem of early survival in vivo of
osteogenic seed cells, which, meanwhile, has conformed to the
purpose of the construction of vascularized tissue-engineered bone
with complete tissue structure.
The osteogenic efficiency of decalcified bone
scaffolds with pre-vascularization in vitro and decalcified
bone scaffolds was investigated in this study. The results showed
that decalcified bone scaffolds with pre-vascularization in
vitro are obviously better than the experimental group of
decalcified bone scaffolds in osteogenic efficiency. The reason for
this is that owing to the reservation of three dimensional
structures and collagen scaffold of original bone tissue,
decalcified bone scaffolds can provide a better scaffold for the
cell crawling, and after decalcified bone scaffolds with
pre-vascularization in vitro are implanted in the bone
defect areas of mice, they can induce the blood into the scaffold,
supplying the oxygen and nourishments needed by tissue repair,
promoting the generation and calcification of new bone tissues,
gradually replacing implanting materials, accelerating the
degradation of implanting materials, and finally completing the
repair process to make the defect areas filled with bone tissues
and achieve the complete connection with peripheral tissues.
Therefore, the vascularization of bone tissue engineering is an
effective way to deal with the problem of low oxygen environment in
the process of bone defect repair, and as the seed cells, growth
factors and scaffold materials, it has become the determining
factor for the successful repair of bone tissue engineering.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Shandong
Natural Science Foundation (ZR201808170124), Yantai Science and
Technology Develpment (2019YT06000140), and the National Natural
Science Foundation of China (81301570).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
XJ and HY were involved in the conception of the
study. BH and GL were also involved in the conception and design of
the study. KW contributed to the analysis and interpretation of the
data. YM assisted with the histopathological examination. CX helped
to perform the analysis, and offered constructive discussions. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
the Affiliated Yantai Yuhuangding Hospital of Qingdao University
(Yantai, China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Yousefi AM, James PF, Akbarzadeh R,
Subramanian A, Flavin C and Oudadesse H: Prospect of stem cells in
bone tissue engineering: A review. Stem Cells Int.
2016:61804872016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zhao T and Sun H: Insight into bone tissue
engineering scaffold materials and their vascularization. Zhongguo
Zu Zhi Gong Cheng Yan Jiu Yu Lin Chuang Kang Fu. 17:6832–6838.
2013.
|
|
3
|
Nakano K, Murata K, Omokawa S, Akahane M,
Shimizu T, Kawamura K, Kawate K and Tanaka Y: Promotion of
osteogenesis and angiogenesis in vascularized tissue-engineered
bone using osteogenic matrix cell sheets. Plast Reconstr Surg.
137:1476–1484. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mercado-Pagán ÁE, Stahl AM, Shanjani Y and
Yang Y: Vascularization in bone tissue engineering constructs. Ann
Biomed Eng. 43:718–729. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Xu Z, Wang G and Wang F:
Histocompatibility of demineralized bone matrix decorated with
poly-L-lysine for scaffolds. Orthopedic J China. 16:1493–1497.
2015.
|
|
6
|
Amini AR, Laurencin CT and Nukavarapu SP:
Bone tissue engineering: Recent advances and challenges. Crit Rev
Biomed Eng. 40:363–408. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhou J, Lin H, Fang T, Li X, Dai W, Uemura
T and Dong J: The repair of large segmental bone defects in the
rabbit with vascularized tissue engineered bone. Biomaterials.
31:1171–1179. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nguyen LH, Annabi N, Nikkhah M, Bae H,
Binan L, Park S, Kang Y, Yang Y and Khademhosseini A: Vascularized
bone tissue engineering: Approaches for potential improvement.
Tissue Eng Part B Rev. 18:363–382. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Almubarak S, Nethercott H, Freeberg M,
Beaudon C, Jha A, Jackson W, Marcucio R, Miclau T, Healy K and
Bahney C: Tissue engineering strategies for promoting vascularized
bone regeneration. Bone. 83:197–209. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lovett M, Lee K, Edwards A and Kaplan DL:
Vascularization strategies for tissue engineering. Tissue Eng Part
B Rev. 15:353–370. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bussolino F, Mantovani A and Persico G:
Molecular mechanisms of blood vessel formation. Trends Biochem Sci.
22:251–256. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Thottappillil N and Nair PD: Scaffolds in
vascular regeneration: Current status. Vasc Health Risk Manag.
11:79–91. 2015.PubMed/NCBI
|