Introduction
Colorectal cancer (CRC) is one of the most prevalent
malignancies in the world, and is a primary cause of
tumor-associated mortality. Previous data has indicated that
incidence of CRC in China increased from 12.8 in 2003 to 16.8 per
100,000 in 2011, while the mortality rate increased from 5.9 to 7.8
per 100,000 and is expected to reach 8.6 per 100,000 in 2020
(1). Pain is one of the most typical
symptoms in patients with cancer, and malignant tumor-associated
pain occurs throughout all stages and courses of treatment,
including surgery, radiotherapy and chemotherapy (2).
The use of opioid analgesics in clinical practice
for the management of cancer-related pain is widely accepted
(3). Morphine is one of the most
frequently used opioid analgesics in the treatment of various
pains, including cancer-associated pain; however, morphine may
induce detrimental side effects such as opioid-induced hyperalgesia
or may result in patients developing a tolerance to opioids
(3). Supplementation of morphine
with adjuvant agents is the preferred method of providing adequate
pain relief and may also reduce the occurrence of adverse side
effects (4,5). As a noncompetitive
N-methyl-D-aspartate-receptor antagonist, ketamine has previously
been shown to be synergistic with morphine (6). When co-administered with morphine,
ketamine is able to reduce hyperalgesia and delay the development
of tolerance to opioids via enhancing opioid-induced
antinociception and decreasing morphine consumption (6). The co-administration of ketamine and
morphine has been described in a number of clinical trials, and
ketamine is usually administered off-label in combination with
opioids at subanesthetic doses to treat pain associated with cancer
(7).
Patients with cancer typically exhibit
immunosuppression (8,9). It is widely reported that host
immunosuppression may influence anti-tumor immune responses
(8–10).
Given that cluster of differentiation
(CD)4+T cells serves a crucial role in the regulation of
all antigen specific immune responses, their potential involvement
in antitumor immunity is of interest to tumor immunologists
(11). T-helper (Th)1 and Th2 cells
are the classical subsets of CD4+ T cells. Th1 cells
produce interferon (IFN)-γ and favor cell-mediated immune
responses. Th2 cells produce interleukin(IL)-4 and/or IL-10 and are
associated with humoral immunity in terms of control of antibody
production (12). The imbalance of
Th cells, particularly decreased Th1/Th2 ratios, has been
associated with mortality and complications in patients with
gastrointestinal tumors (13,14).
It has previously been demonstrated that anesthetic
and sedative agents exhibit immunomodulatory activity (15). For example, the effects of morphine
and ketamine on the differentiation of Th cells have been
demonstrated in previous studies in healthy volunteers in
vitro (16,17). To the best of our knowledge, no
previous studies have investigated whether morphine and ketamine
are able to alter the differentiation of Th cells in patients with
tumors; therefore, this study was designed to assess the effects of
morphine and ketamine on the differentiation of CD4+ T
cells induced by phorbol-myristate-acetate (PMA) and ionomycin in
patients with CRC.
Materials and methods
Ethics approval
The present study was approved by the Ethics and
Research Committee of Shandong Academy of Medical Sciences (Jinan,
Shandong). All participants included in the study gave their
informed consent for the tests to be performed, and the present
study was conducted in adherence with the Declaration of
Helsinki.
Study population
A total of 20 patients with primary CRC (10 males,
10 females) and 20 healthy subjects (10 males, 10 females), with an
age range of 45–65 years and body mass indices from 18–25
kg/m2, were enrolled as research subjects in the present
study between October 2014 and May 2015 at Shandong Cancer Hospital
affiliated to Shandong University (Jinan, China). Routine blood
tests were performed on patients in the CRC group including
lymphocyte counts and calculation of these as a proportion of total
cells. No patients had a history of long-term medication use, drug
abuse, transfusion, diabetes mellitus, recent infection, systemic
inflammatory disease or immunological deficiency, and patients did
not have any other tumors. None of the patients had previously been
treated using immunosuppression, radiotherapy or chemotherapy. All
patients in the normal group were either healthy or had benign
noninflammatory conditions of the large bowel which were diagnosed
via barium enema or colonoscopy.
Reagents
Ketamine (Shanghai Hengrui Pharmaceutical Co., Ltd.,
Shanghai, China) was diluted to different concentrations (25, 50,
and 100 µM) with distilled water. Morphine (Shenyang Pharmaceutical
University, Shenyang, China) was diluted to 50 ng/ml with distilled
water.
Peripheral blood mononuclear cell
(PBMC) isolation
PMBCs were isolated from the blood samples harvested
from CRC and normal groups as previously described (18). Briefly, peripheral blood from the
ulnar vein (5 ml) was placed in a heparinized tube and layered
using density gradient sedimentation. Following centrifugation (500
× g; 20°C for 20 min) PBMC were collected from the interface
and washed three times in culture medium. Atrypan blue dye test
(17) was conducted to ensure that
cell viability >95%. Qualifying cells were suspended
(1×106 cells) in RPMI Medium1640 (Thermo Fisher
Scientific, Inc., Waltham, MA, USA) supplemented with 10% FBS
(Thermo Fisher Scientific, Inc.) and incubated for 30 min. PBMCs
were then stimulated using 2 µl/ml of a leukocyte activation
cocktail containing PMA and ionomycin (P550583; 1X; BD Biosciences,
Franklin Lanes, NJ, USA) in the presence or absence of ketamine and
morphine, in an atmosphere containing 5% CO2 at 95%
humidity and 37°C for 4 h, prior to analysis.
Study groups
Cells isolated from healthy subjects were assigned
to one of the following groups: Group 0, healthy, untreated control
group; or group 1, healthy group, treated with PMA and ionomycin
but not ketamine or morphine. Cells isolated from patients with CRC
were assigned to one of the following groups: Group 2, CRC control
group not treated with PMA and ionomycin; group 3, CRC group
treated with PMA and ionomycin without ketamine or morphine; group
4, CRC group treated with ketamine (25 µM), PMA and ionomycin;
group 5, CRC group treated with ketamine (50 µM), PMA and
ionomycin; group 6, CRC group treated with ketamine (100 µM), PMA
and ionomycin; or group 7, CRC group treated with morphine (50
ng/ml), PMA and ionomycin.
Th cell subset analysis
Cells were harvested and subsequently counted using
a FACS Caliburflow cytometer (BD Biosciences). Subsets of Th1 and
Th2 cells were detected via the surface antigen CD3, CD8 and
intracellular cytokines IFN-γ or IL-4. Briefly, the cells
(1×106) were stained with fluorescein
isothiocyanate-mouse anti-human CD3 (561806) and phycoerythin
(PE)-Cy5 mouse anti-human CD8antibodies (561946; both BD
Biosciences), fixed, permeabilized, and stained with PE-mouse
anti-human IFN-γ (557074) or PE-mouse anti-human IL-4 antibodies
(551774; both BD Biosciences). Th1 cells were marked as
CD3+CD8−IFN-γ+ and Th2 cells were
marked as CD3+CD8−IL-4+. The cell
counts were presented as the percentage of total CD3-positive
cells.
Statistical analysis
SPSS19.0 statistical software (IBM SPSS, Armonk, NY,
USA) was used for all data analysis. Data are presented as the mean
± standard error of the mean. The Shapiro-Wilk test was performed
and the percentages of T helper cell subsets were found to be
normally distributed. Tests of variant homogeneity were followed by
Bartlett's test (when data were normally distributed) or Levene's
test (when data were not normally distributed). The percentages of
T helper cell subsets were compared using one-way analysis of
variance followed by least-significant difference or Dunnett's T3
post hoc test based on the homogeneity of variance. As the Th1/Th2
ratio did not follow a normal distribution, the data were presented
as medians (range). Friedman tests were performed to establish
Th1/Th2 ratio. The significant effects were investigated post hoc
using Wilcoxon-signed-ranks tests. P<0.05 was considered to
indicate a statistically significant difference.
Results
Cell viability
Cell viability in all groups was >95% with or
without PMA and ionomycin treatment, as confirmed via trypan blue
staining.
CD3+ cell counts
There was no significant difference in the number of
CD3+ cells in the eight groups prior to PMA and
ionomycin stimulation (Fig. 1).
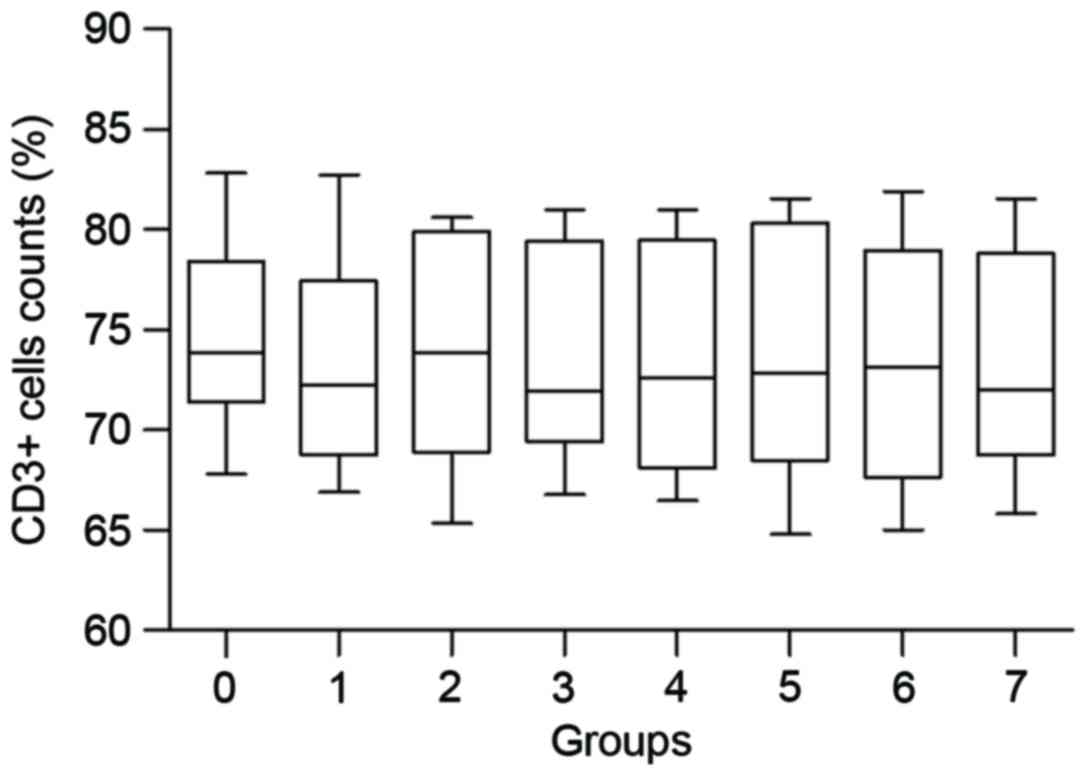 | Figure 1.Percentages of CD3+ cells
in eight groups. Group 0, healthy control group without PMA and
ionomycin treatment; group 1, healthy patient group treated with
PMA and ionomycin but not ketamine or morphine; group 2, CRC
control group without PMA and ionomycin; group 3, CRC group treated
with PMA and ionomycin but not ketamine or morphine; group 4, CRC
group treated with ketamine (25 µM), PMA and ionomycin; group 5,
CRC group treated with ketamine (50 µM), PMA and ionomycin; group
6, CRC group treated with ketamine (100 µM), PMA and ionomycin;
group 7, CRC group treated with morphine (50 ng/ml), PMA and
ionomycin. CD3+, cluster of differentiation
3+; PMA, phorbol-myristate-acetate; CRC, colorectal
cancer. |
Th cell differentiation in normal
subjects and patients with CRC
In the absence of PMA and ionomycin stimulation,
there were few Th1 cells [<0.10% in the healthy subject group
(group 0) compared to 0.12% in the CRC group (group 2); P>0.05]
and Th2 cells [<0.10% in the healthy subject group (group 0)
compared to 0.13% in the CRC group (group 2); P>0.05]. However,
the proportion of Th1 and Th2 cells were significantly increased
following stimulation with PMA and ionomycin in the healthy and CRC
group cell populations [Th1 cells from <0.10 to 9.69±1.31%, and
from 0.120 to 6.38±1.00% in the healthy subject and CRC groups
(group 1 and group 3), respectively, P<0.001; Fig. 2); Th2 cells from <0.10 to
3.99±0.60% and from 0.13 to 3.93±0.91% in the healthy subject and
CRC groups (group1 and group 3), respectively, P<0.001; Fig. 3]. Following PMA and ionomycin
stimulation, the number of Th1 cells in group 1 compared with group
3 were significantly different (9.69±1.31 and 6.38±1.00%,
respectively; P<0.001; Fig. 2),
whereas the number of Th2 cells were not significantly different
between group 1 and group 3 (3.99±0.60 vs. 3.93±0.91%; P=0.82,
Fig. 3). The Th1/Th2 ratio therefore
significantly differed in group 1 compared with the group 3 (2.48
and 1.63, respectively; P<0.001) following stimulation with PMA
and ionomycin (Fig. 4).
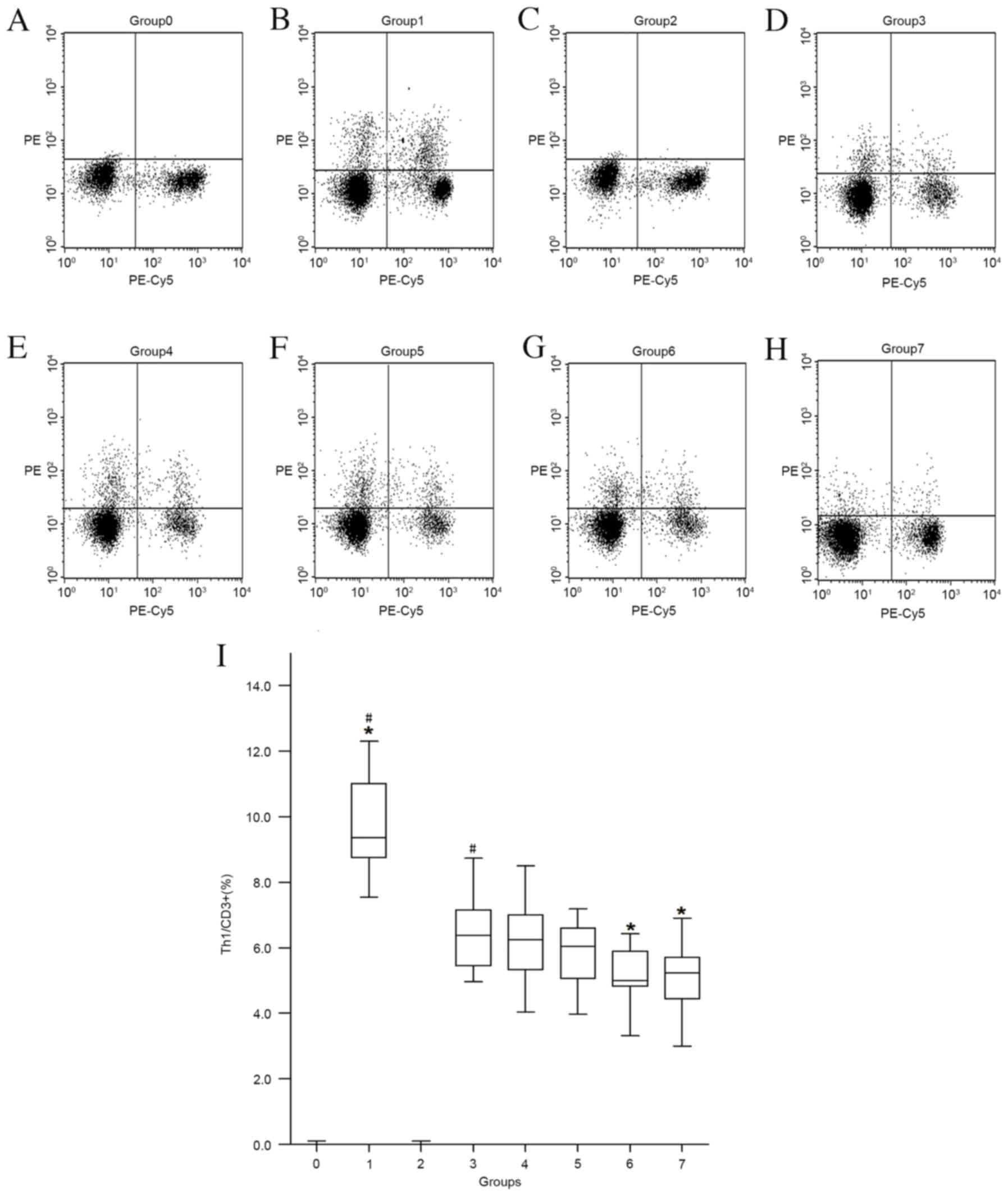 | Figure 2.Th1 cell counts in the presence of
ketamine or morphine following PMA and ionomycin stimulation in
healthy control and CRC groups. (A) Group 0, healthy control group
without PMA and ionomycin treatment. (B) Group 1, healthy patient
group treated with PMA and ionomycin but not ketamine or morphine.
(C) Group 2, CRC control group without PMA and ionomycin. (D) Group
3, CRC group treated with PMA and ionomycin but not ketamine or
morphine. (E) Group 4, CRC group treated with ketamine (25 µM), PMA
and ionomycin. (F) Group 5, CRC group treated with ketamine (50
µM), PMA and ionomycin. (G) Group 6, CRC group treated with
ketamine (100 µM), PMA and ionomycin (H) Group 7, CRC group treated
with morphine (50 ng/ml), PMA and ionomycin. (I)
CD3+CD8−IFN-γ+cells, labeled as
Th1 cells, in dot plots. Data are presented as the mean ± standard
error of the mean. #P<0.001 vs. group 0; *P<0.001
vs. group 3. Th1, T helper 1; PMA, phorbol-myristate-acetate; CRC,
colorectal cancer; CD, cluster of differentiation;
IFN-g+, interferon γ. |
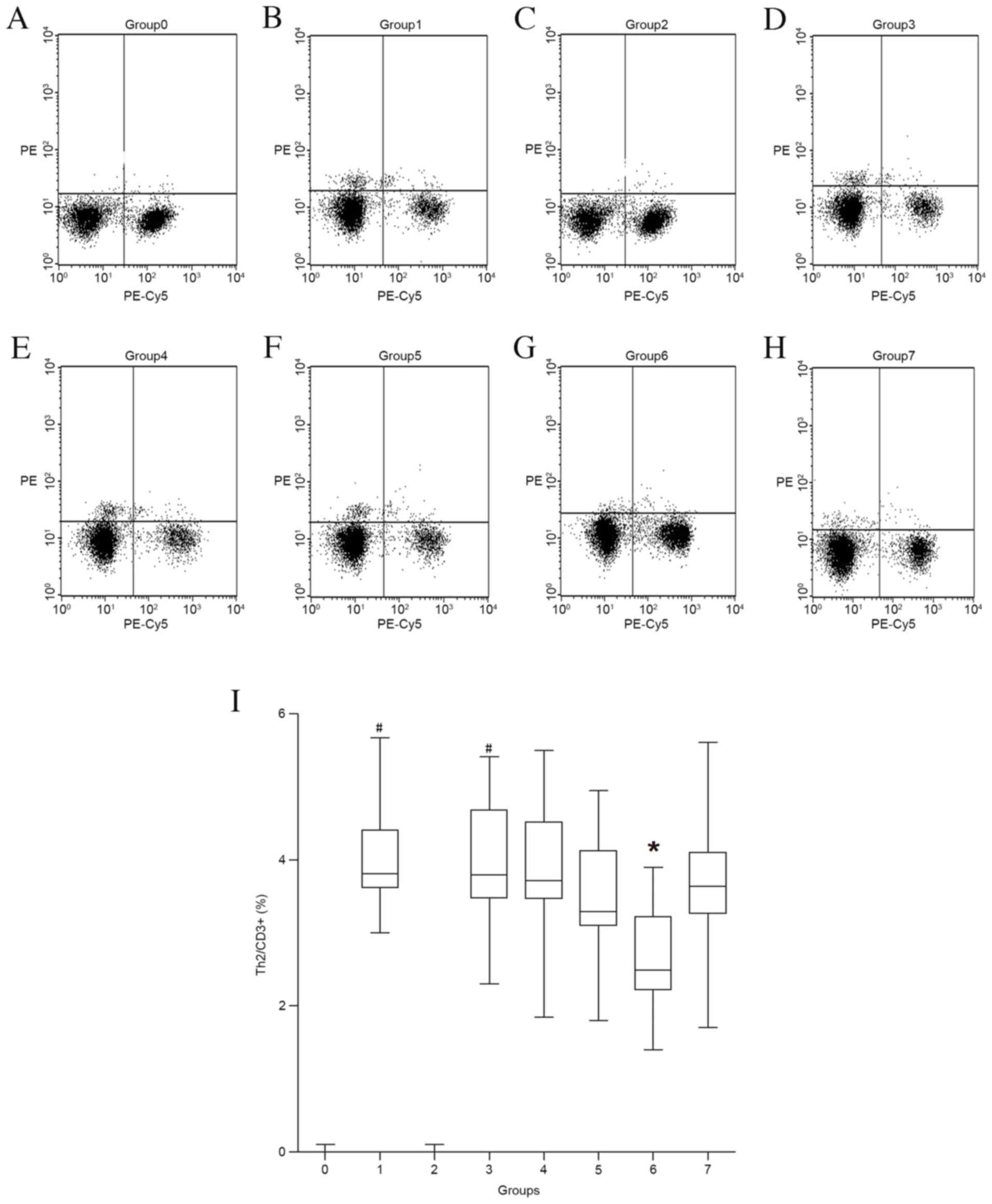 | Figure 3.Th2 cell counts in the presence of
ketamine or morphine following PMA and ionomycin stimulation in
healthy control and CRC groups. (A) Group 0, healthy control group
without PMA and ionomycin treatment. (B) Group 1, healthy patient
group treated with PMA and ionomycin but not ketamine or morphine.
(C) Group 2, CRC control group without PMA and ionomycin. (D) Group
3, CRC group treated with PMA and ionomycin but not ketamine or
morphine. (E) Group 4, CRC group treated with ketamine (25 µM), PMA
and ionomycin. (F) Group 5, CRC group treated with ketamine (50
µM), PMA and ionomycin. (G) Group 6, CRC group treated with
ketamine (100 µM), PMA and ionomycin (H) Group 7, CRC group treated
with morphine (50 ng/ml), PMA and ionomycin. (I)
CD3+CD8−IL-4+cells, labeled as Th2
cells, in dot plots. Data are presented as the mean ± standard
error of the mean. #P<0.001 vs. group 0; *P<0.001
vs. Group 3. Th2, T helper 2; PMA, phorbol-myristate-acetate; CRC,
colorectal cancer; CD, cluster of differentiation;
IFN-g+, interferon γ. |
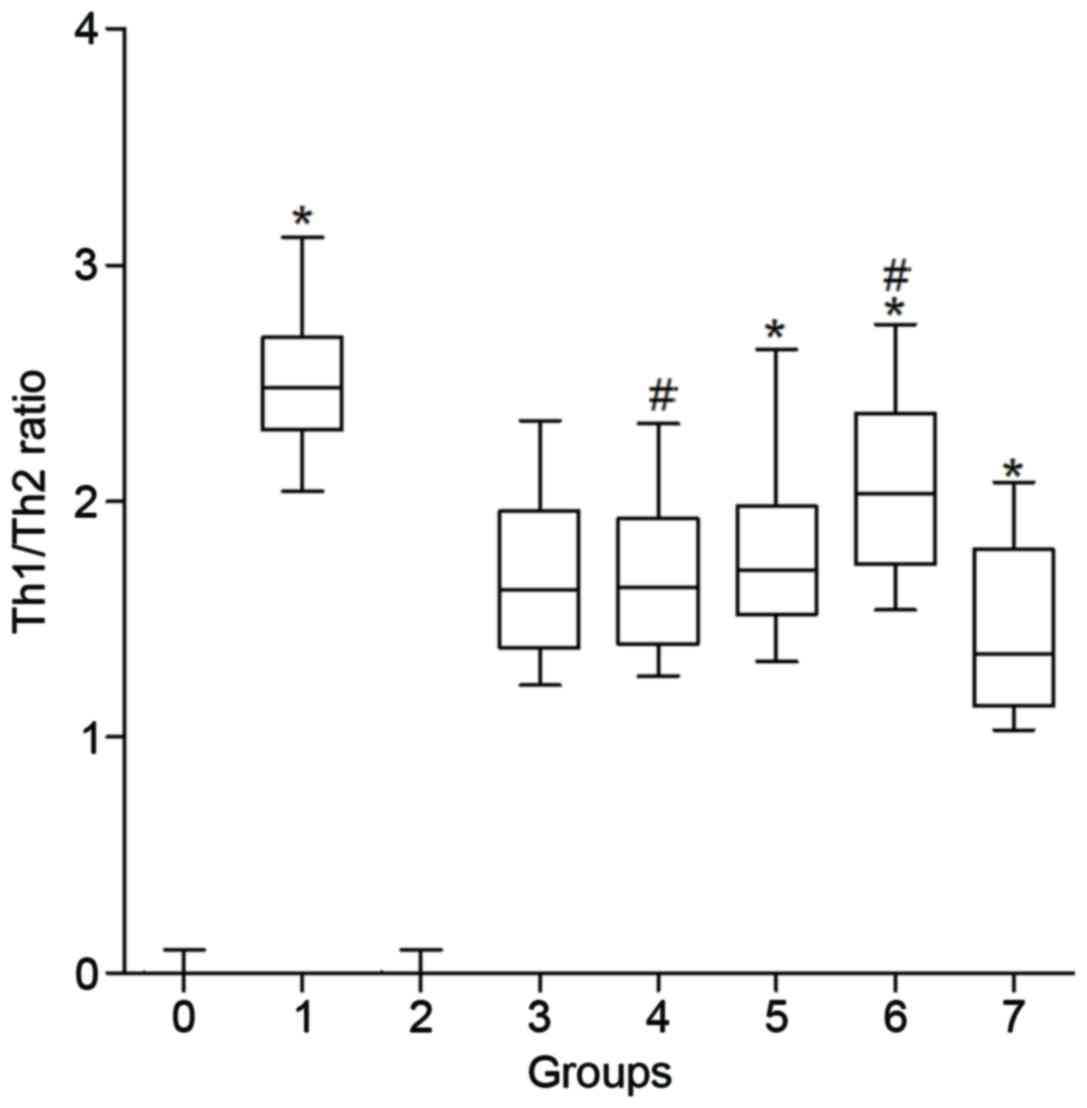 | Figure 4.Th1/Th2 ratio in the presence of
ketamine or morphine following PMA and ionomycin stimulation in the
normal control and CRC groups. Group 0, healthy control group
without PMA and ionomycin treatment; group 1, healthy patient group
treated with PMA and ionomycin but not ketamine or morphine; group
2, CRC control group without PMA and ionomycin; group 3, CRC group
treated with PMA and ionomycin but not ketamine or morphine; group
4, CRC group treated with ketamine (25 µM), PMA and ionomycin;
group 5, CRC group treated with ketamine (50 µM), PMA and
ionomycin; group 6, CRC group treated with ketamine (100 µM), PMA
and ionomycin; group 7, CRC group treated with morphine (50 ng/ml),
PMA and ionomycin. Data are presented as the mean ± standard error
of the mean. *P<0.001 vs. group 3; #P<0.001 vs.
group 5. PMA, phorbol-myristate-acetate; CRC, colorectal cancer;
Th, T helper. |
Effects of ketamine on Th1 and Th2
subsets following PMA and ionomycin stimulation in the CRC
groups
Ketamine treatment of CRC group cells at a
concentration of 100 µM (following PMA and ionomycin treatment)
significantly decreased the proportion of Th1 cells from 6.38±1.00%
in group 3 CRC patient cell populations to 5.14±0.80% (P<0.001;
Fig. 2) and Th2 cells from
3.93±0.91% in group 3 CRC patient cell populations to 2.61±0.64%
(P<0.001; Fig. 3); however, these
measures were not significantly altered by 50 µM ketamine
treatment.
Ketamine at 50 and 100 µM significantly increased
the Th1/Th2 ratio in CRC groups from 1.62 (group 3) to 1.71 (group
4; P<0.001) and to 2.03 (group 6; P<0.001), respectively
(Fig. 4), acting in a dose-dependent
manner. Ketamine at a concentration of 25 µM did not significantly
affect the proportion of Th1 cells, Th2 cells or the Th1/Th2 ratio
in the presence of PMA and ionomycin.
Effects of morphine on Th1 and Th2
subsets following PMA and ionomycin stimulation in the CRC
groups
Morphine significantly decreased the number of Th1
cells from 6.38±1.00 (in group 3 CRC cell populations) to
5.04±0.94% (P<0.001; Fig. 2), and
the Th1/Th2 ratio from 1.62 to 1.35 (group 7; P<0.001) (Fig. 4) following PMA and ionomycin
stimulation in the CRC group; however, no significant difference
was observed in the number of Th2 cells (3.93±0.60% in group 3 vs.
3.70±0.98%; P=0.374; Fig. 3).
Discussion
It is established that Th cells modulate immune
responses and serve an important role in immune protection
(19). Furthermore, it has recently
been demonstrated that CD4+Th cells are important for
effective antitumor immunity (20).
According to their cytokine synthesis profile, CD4+Th
cells maybe classified as Th1 and Th2 subsets. The Th1 subset,
which was the first identified group of Th cells, selectively
expresses IFN-c, tumor necrosis factor (TNF)-α, TNF-β and other
proinflammatory cytokines (21). Th1
cells are therefore important for regulating innate and
T-cell-mediated immune responses, and protecting the host from
obligate intracellular pathogens. Th2 cells were identified at the
same time as Th1 cells in the early 1980s. An important function of
Th2 cells is the production of IL-4, IL-5, IL-9, IL-10 and IL-13.
Th2 cells also produce immunoglobulins by inducing differentiation
in B cells (22). Therefore, Th2
cells are important in the humoral response and in resistance
against extracellular pathogens. It is generally believed that
polarization of Th cells toward either Th1 or Th2 typing may
significantly influence the later immune responses during
carcinogenesis (22).
In the present study, counts were performed in
vitro to assess the number of Th1 and Th2 cells in the
peripheral blood of patients with CRC. The results demonstrated
that the number of Th1 cells and the Th1/Th2 ratio were
significantly lower in patients with CRC compared with healthy
subjects following administration of PMA and ionomycin, whereas
there was no significant difference in the number of Th2 cells.
These results are supported by the findings of previous studies, in
which the cytokines produced by Th1 cells, such as IFN-c, TNF-α and
IL-2, were significantly reduced in CRC patients, whereas the
cytokines produced by Th2 cells, such as IL-6 and IL-4 showed no
marked change (23). Furthermore,
Kanazawa et al (24)
demonstrated that patients with gastric or colorectal cancer have a
lower Th1/Th2 ratio compared with healthy subjects, and Tabata
et al (25) demonstrated Th2
dominance in patients with gastrointestinal tract cancer.
Domino et al (26) demonstrated that, following
intravenous administration of 2 mg/kg ketamine, the blood
concentration of ketamine may reach 27 µg/ml (100 µM), and it may
therefore provide an analgesic effect in vivo at a
concentration of 0.5 mg/kg (26). It
has been suggested that the strength of this effect would be
dose-dependent (27); therefore the
following serial concentrations of ketamine were used in the
present study: 6.25 µg/ml (25 µM), 12.5 µg/ml (50 µM) and 25 µg/ml
(100 µM). It has previously been demonstrated that a morphine
plasma concentration of 50 ng/ml is within the analgesic range
(28); therefore, a morphine
concentration of 50 ng/ml was used in the present study.
Additionally, the culture conditions including temperature, osmotic
pressure and pH value were kept in normal ranges for all groups to
ensure that the results would not be affected by differences in
culture.
The results of the present study indicated that
morphine had a negative effect on Th cell balance as it decreased
the counts of Th1 cells and the ratio of Th1/Th2 in the CRC group.
Gao et al (17) previously
demonstrated that morphine is able to suppress the differentiation
of Th cells and the subsequent secretion of cytokines, and decrease
the ratios of Th1/Th2 and IFN-γ/IL-4. Given that patients with CRC
are Th2 dominant, it may be hypothesized that analgesia with
morphine may result in a further imbalance of the Th1/Th2 ratio.
These changes may inhibit the immunological response and hasten
tumor invasion, recurrence and metastasis of cancer in patients
with CRC. However, in the present study, ketamine shifted the
balance of Th1/Th2 toward Th1, suggesting that it may have a
beneficial immunoregulatory effect in patients with CRC. This
supports the findings of a previous study in healthy participants,
in which ketamine suppressed the differentiation of Th cells and
secretion of cytokines, whereas the Th1/Th2 ratio was increased in
the presence of PMA and ionomycin (16).
The results of the present study demonstrate that
ketamine affects the differentiation of Th cells in a
concentration-dependent manner, as with increased concentrations,
the effect of ketamine on the differentiation of Th cells was
increased. However, at a concentration of 25 µM, ketamine did not
induce any significant changes in the number of Th1 and Th2 cells
or the Th1/Th2 ratio. This suggests that a low dose of ketamine,
combined with morphine, may provide sufficient pain relief without
increasing immune suppression in patients with CRC.
There are numerous cytokine analysis methods
available, such as ELISA, reverse transcription-polymerase chain
reaction, and immunohistochemistry (29,30).
ELISA is widely used due to the ease with which it is performed;
however, it is unable to identify the cellular source of cytokines
in the plasma (29). Intracellular
cytokine staining, a flow cytometry method, is currently the only
technique that can enumerate antigen-specific T cells and determine
their phenotype simultaneously (31). It has previously been used to
investigate cytokine production at the single-cell level following
polyclonal stimulation with mitogens with a short incubation time,
which depending on the retention of cytokines in cells, typically
peaks between 4 (for TNF-α) to 8 h (for IFN-γ and IL-2) and up to
12 h for IL-12 (31,32). Furthermore, two or more cytokines may
be simultaneously detected within a single cell by multiparameter
flow cytometry in the presence of cytokine secretion inhibitors;
therefore, it maybe used to determine the Th1/Th2 ratio directly
(33). A modified method using whole
blood has also been developed, which requires less time as PBMC
isolation is not required (34);
however, some components of the serum may interfere with the
results, and therefore PBMCs isolated from patients with CRC were
used in the present study.
It has been reported that phytohaemagglutinin is
able to activate Th cells; however, it takes 48 h for this to occur
(16). As PMA and ionomycin are able
to activate Th cells within 4–6 h, they were selected in the
present study to minimize incubation time of PBMCs in vitro
and maintain cell viability. As PMA and ionomycin are able to down
regulate CD4 expression, Th1 and Th2 lymphocytes with
CD3+ and CD8− were labeled in the present
study, a detection method that has been used in previous studies
(16,35). Additionally, trypan blue staining was
performed to assess the extent of cell death over the course of the
present study. The results indicated that there was no significant
cell death in the presence or absence of PMA and ionomycin. In
preliminary experiments, there were few Th1 and Th2 cells in the
presence of morphine or ketamine. Therefore, in the CRC groups,
there was no subgroup in which only morphine or ketamine were
administered without incubating with PMA and ionomycin.
In the present study, patients with CRC exhibited
Th2 dominance. Furthermore, morphine and ketamine with
concentrations over the subanesthestic level (<100 µM)
suppressed the differentiation of Th cells in vitro.
Morphine induced a decrease in the Th1/Th2 ratio, whereas ketamine
increased the Th1/Th2 ratio and did not affect the differentiation
of Th cells at the subanesthestic concentration. With increasing
concentration, the effect of ketamine on the differentiation of Th
cells was increased. These findings suggest that in clinical
practice, combinatorial treatment with morphine and a low dose of
ketamine may reduce morphine consumption and the risk of adverse
reactions, alleviate immune inhibition and improve the quality of
life in patients with CRC.
In conclusion, the present study demonstrated that
CRC shifts the balance of Th1/Th2 towards Th2 by inducing an
immunological response. Morphine is able to suppress the
differentiation of Th cells; however, it induces a decrease in the
Th1/Th2 ratio. Furthermore, ketamine is able to affect the
differentiation of Th cells in a dose-dependent manner; therefore,
the findings of the present study may provide a novel clinical
approach for treatment of patients with CRC.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Natural
Science Foundation of Shandong Province, China (grant no.
ZR2011HM039).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MH designed and implemented the current study,
acquired data, analyzed and interpreted, results and drafted the
manuscript. KW and FX conceived and designed the present study, and
provided their assistance and critical review when drafting the
manuscript. NZ, HL, BW, XiuW, XinW and TJ acquired and interpreted
the data.
Ethics approval and consent to
participate
The present study was approved by the Ethics and
Research Committee of Shandong Academy of Medical Science. All
patients included in the current study provided their informed
consent and the current study was performed in accordance with the
Declaration of Helsinki.
Patient consent for publication
All patients included in the study gave their
informed consent for publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Zhu J, Tan Z, Hollis-Hansen K, Zhang Y, Yu
C and Li Y: Epidemiological trends in colorectal cancer in China:
An ecological study. Dig Dis Sci. 62:235–243. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Marcus DA: Epidemiology of cancer pain.
Curr Pain Headache Rep. 15:231–234. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gomes T, Juurlink DN, Dhalla IA,
Mailis-Gagnon A, Paterson JM and Mamdani MM: Trends in opioid use
and dosing among socio-economically disadvantaged patients. Open
Med. 5:e13–e22. 2011.PubMed/NCBI
|
|
4
|
Hynninen MS, Cheng DC, Hossain I, Carroll
J, Aumbhagavan SS, Yue R and Karski JM: Non-steroidal
anti-inflammatory drugs in treatment of postoperative pain after
cardiac surgery. Can J Anaesth. 47:1182–1187. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lahtinen P, Kokki H, Hendolin H, Hakala T
and Hynynen M: Propacetamol as adjunctive treatment for
postoperative pain after cardiac surgery. Anesth Analg. 95:813–819.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Parikh B, Maliwad J and Shah VR:
Preventive analgesia: Effect of small dose of ketamine on morphine
requirement after renal surgery. J Anaesthesiol Clin Pharmacol.
27:485–488. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kerr C, Holahan T and Milch R: The use of
ketamine in severe cases of refractory pain syndromes in the
palliative care setting: A case series. J Palliat Med.
14:1074–1077. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Umansky V: Immunosuppression in the tumor
microenvironment: Where are we standing? Semin Cancer Biol.
22:273–274. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Draghiciu O, Nijman HW and Daemen T: From
tumor immunosuppression to eradication: Targeting homing and
activity of immune effector cells to tumors. Clin Dev Immunol.
2011:4390532011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Munhoz RR and Postow MA: Recent advances
in understanding antitumor immunity. F1000Res. 5:25452016.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Protti MP, De Monte L and Di Lullo G:
Tumor antigen-specific CD4+T cells in cancer immunity: From antigen
identification to tumor prognosis and development of therapeutic
strategies. Tissue Antigens. 83:237–246. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kurosawa S and Kato M: Anesthetics, immune
cells, and immune responses. J Anesth. 22:263–277. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tosolini M, Kirilovsky A, Mlecnik B,
Fredriksen T, Mauger S, Bindea G, Berger A, Bruneval P, Fridman WH,
Pagès F and Galon J: Clinical impact of different classes of
infiltrating T cytotoxic and helper cells (Th1, th2, treg, th17) in
patients with colorectal cancer. Cancer Res. 71:1263–1271. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ubukata H, Motohashi G and Tabuchi T,
Nagata H, Konishi S and Tabuchi T: Evaluations of
interferon-γ/interleukin-4 ratio and neutrophil/lymphocyte ratio as
prognostic indicators in gastric cancer patients. J Surg Oncol.
102:742–747. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hunter JD: Effects of anaesthesia on the
human immune system. Hosp Med. 60:658–663. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gao M, Jin W, Qian Y, Ji L, Feng G and Sun
J: Effect of N-methyl-D-aspartate receptor antagonist on T helper
cell differentiation induced by phorbol-myristate-acetate and
ionomycin. Cytokine. 56:458–465. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gao M, Sun J, Jin W and Qian Y: Morphine,
but not ketamine, decreases the ratio of Th1/Th2 in CD4-positive
cells through T-bet and GATA3. Inflammation. 35:1069–1077. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Nicholl DS, Daniels HM, Ira Thabrew M,
Grayer RJ, Simmonds MS and Hughes RD: In vitro studies on the
immunomodulatory effects of extracts of Osbeckia aspera. J
Ethnopharmacol. 78:39–44. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Abbas AK, Murphy KM and Sher A: Functional
diversity of helper T lymphocytes. Nature. 383:787–793. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Adotévi O, Dosset M, Galaine J, Beziaud L,
Godet Y and Borg C: Targeting antitumor CD4 helper T cells with
universal tumor-reactive helper peptides derived from telomerase
for cancer vaccine. Hum Vaccin Immunother. 9:1073–1077. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wan YY: Multi-tasking of helper T cells.
Immunology. 130:166–171. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Olson NC, Sallam R, Doyle MF, Tracy RP and
Huber SA: T helper cell polarization in healthy people:
Implications for cardiovascular disease. J Cardiovasc Transl Res.
6:772–786. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Evans CF, Galustian C, Bodman-Smith M,
Dalgleish AG and Kumar D: The effect of colorectal cancer upon host
peripheral immune cell function. Colorectal Dis. 12:561–569. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kanazawa M, Yoshihara K, Abe H, Iwadate M,
Watanabe K, Suzuki S, Endoh Y, Takita K, Sekikawa K, Takenoshita S,
et al: Effects of PSK on T and dendritic cells differentiation in
gastric or colorectal cancer patients. Anticancer Res. 25:443–449.
2005.PubMed/NCBI
|
|
25
|
Tabata T, Hazama S, Yoshino S and Oka M:
Th2 subset dominance among peripheral blood T lymphocytes in
patients with digestive cancers. Am J Surg. 177:203–208. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Domino EF, Zsigmond EK, Domino LE, Domino
KE, Kothary SP and Domino SE: Plasma levels of ketamine and two of
its metabolites in surgical patients using a gas chromatographic
mass fragmentographic assay. Anesth Analg. 61:87–92. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Atkins D, Best D, Briss PA, Eccles M,
Falck-Ytter Y, Flottorp S, Guyatt GH, Harbour RT, Haugh MC, Henry
D, et al: Grading quality of evidence and strength of
recommendations. BMJ. 328:14902004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hammoud HA, Aymard G, Lechat P,
Boccheciampe N, Riou B and Aubrun F: Relationships between plasma
concentrations of morphine, morphine-3-glucuronide,
morphine-6-glucuronide, and intravenous morphine titration outcomes
in the postoperative period. Fundam Clin Pharmacol. 25:518–527.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Pala P, Hussell T and Openshaw PJ: Flow
cytometric measurement of intracellular cytokines. J Immunol
Methods. 243:107–124. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Whiteside TL: Cytokine assays.
Biotechniques Suppl. 4-8(10): 12–15. 2002.
|
|
31
|
Freer G and Rindi L: Intracellular
cytokine detection by fluorescence-activated flow cytometry: Basic
principles and recent advances. Methods. 61:30–38. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Mackenzie NM and Pinder AC: Flow cytometry
and its applications in veterinary medicine. Res Vet Sci.
42:131–139. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Foster B, Prussin C, Liu F, Whitmire JK
and Whitton JL: Detection of intracellular cytokines by flow
cytometry. Curr Protoc Immunol Chapter. 6:Unit 6.24. 2007.
View Article : Google Scholar
|
|
34
|
Papadogiannakis EI, Kontos VI, Tamamidou M
and Roumeliotou A: Determination of intracellular cytokines
IFN-gamma and IL-4 in canine T lymphocytes by flow cytometry
following whole-blood culture. Can J Vet Res. 73:137–143.
2009.PubMed/NCBI
|
|
35
|
Palma-Nicolás JP, Hernández-Pando R,
Segura E, Ibarra-Sánchez MJ, Estrada-García I, Zentella-Dehesa A
and López-Marín LM: Mycobacterial di-O-acyl trehalose inhibits Th-1
cytokine gene expression in murine cells by down-modulation of MAPK
signaling. Immunobiology Immunobiology signaling. Immunobiology.
215:143–152. 2010. View Article : Google Scholar : PubMed/NCBI
|














