Introduction
Behcet's disease (BD) is a chronic multisystem of
relapsing vasculitis with an unknown etiology that is characterized
by oral and genital ulceration, cutaneous lesions, ocular
inflammation, arthritis and vascular manifestations (1).
The diagnosis of BD is clinical and no specific
laboratory findings are included in the diagnostic criteria
(1). BD associated vasculitis
affects vessels of all sizes in the arterial and venous systems
(2–4). Vasculitis with thrombosis in large
vessels is common, with lower extremity deep vein thrombosis being
the most common form of BD vascular involvement (2–4).
Budd-Chiari syndrome (BCS) is caused by the thrombotic or
non-thrombotic obstruction of the venous outflow tract that
transports blood from hepatic veins into the inferior vena cava
(1,2). Patients with BCS are at a high risk of
portal hypertension and liver failure, but thrombosis is the
primary cause of BCS (5). It has
been reported that ~5% of patients with BCS in western countries,
9% in Turkey and 13% in Egypt may be attributed to BD (6–9).
However, misdiagnosis is a common occurrence in cases of BD
associated BCS (BD-BCS) (8,9). Certain patients exhibit no overt
symptoms and others experience abdominal pain, jaundice, nausea,
enlarged liver/spleen and ascites (8,9).
Inappropriate or delayed treatment may therefore occur if other
symptoms of BD are unnoticed. Although BD-BCS is more common in the
Middle and Far East, it has been rarely observed in China. Herein,
two cases of BD-BCS are reported and a literature review is
presented. The clinical characteristics, treatments and outcomes of
the patients admitted to The First Affiliated Hospital of Sun
Yat-sen University between 2004 and 2016 were assessed.
Case report
Ethics statement
The present study was performed in accordance with
the Declaration of Helsinki and the protocol was approved by the
Ethics Committee of The First Affiliated Hospital of Sun Yat-sen
University [Guangzhou, China; Project identification code: (1481)
541729]. Informed consent was obtained from each patient for
publication.
Case 1
A 49-year-old Chinese man was admitted on January
2010 to the First Affiliated Hospital of Sun Yat-sen University
(Guangzhou, China) with a choking sensation in the chest, and
abdominal distention with epigastric pain of an unknown origin. The
pain was gradually worsening and was not accompanied by
constipation, diarrhea or urinary symptoms. A review of the
patient's medical history revealed that they had experienced oral
and genital ulcers for >10 years. Oral ulcers occurred >10
times per year and genital ulcers were exhibited 5–6 times per
year, all in the same location. The patient also reported episodes
of uveitis. Physical examination identified oral ulcers,
bilaterally decreased pulmonary breathing sounds, hepatomegaly
without pressing pain, jugular varicosity and varicose veins over
the abdominal wall.
The laboratory results were as follows: White blood
cell count, 11.14×109/l (normal range,
4–10×109/l; assessed using the Mindray BC-6900 kit;
Mindray, Shenzhen, China); C-reactive protein (CRP), 49.9 mg/l
(normal range, 0.00–10.00 mg/l; assessed using the CRP-M100 kit;
Mindray); erythrocyte sedimentation rate (ESR), 38 mm/h (normal
range for males, 0–15 mm/h); Total bilirubin (TBIL), 22.7 µmol/l
(normal range, 3.0–22.0 µmol/l); Glutamic pyruvic transaminase
(ALT), 137 U/l (normal range, 0–40 U/l); Glutamic oxaloacetic
transaminase (AST), 208 U/l (normal range, 29–35 U/l); Serum
albumin (ALB), 22.3 g/l (normal range, 35.0–50.0 g/l). ESR, TBIL,
ALT, AST and ALB were all assessed using the Beckman Coulter power
processor that contained all the required reagents (Beckman
Coulter, Inc., Brea, CA, USA). The patient was tested negative for
the anti-nuclear antibody (ANA), anticycloplasmic antibody (ANCA)
and anti-cardiolipin antibody (ANA, ANCA and anti-cardiolipin
antibody were assessed using Oumeng Euroline Plus (Laboratory
Overall Solution, Beijing, China; with its self-contained
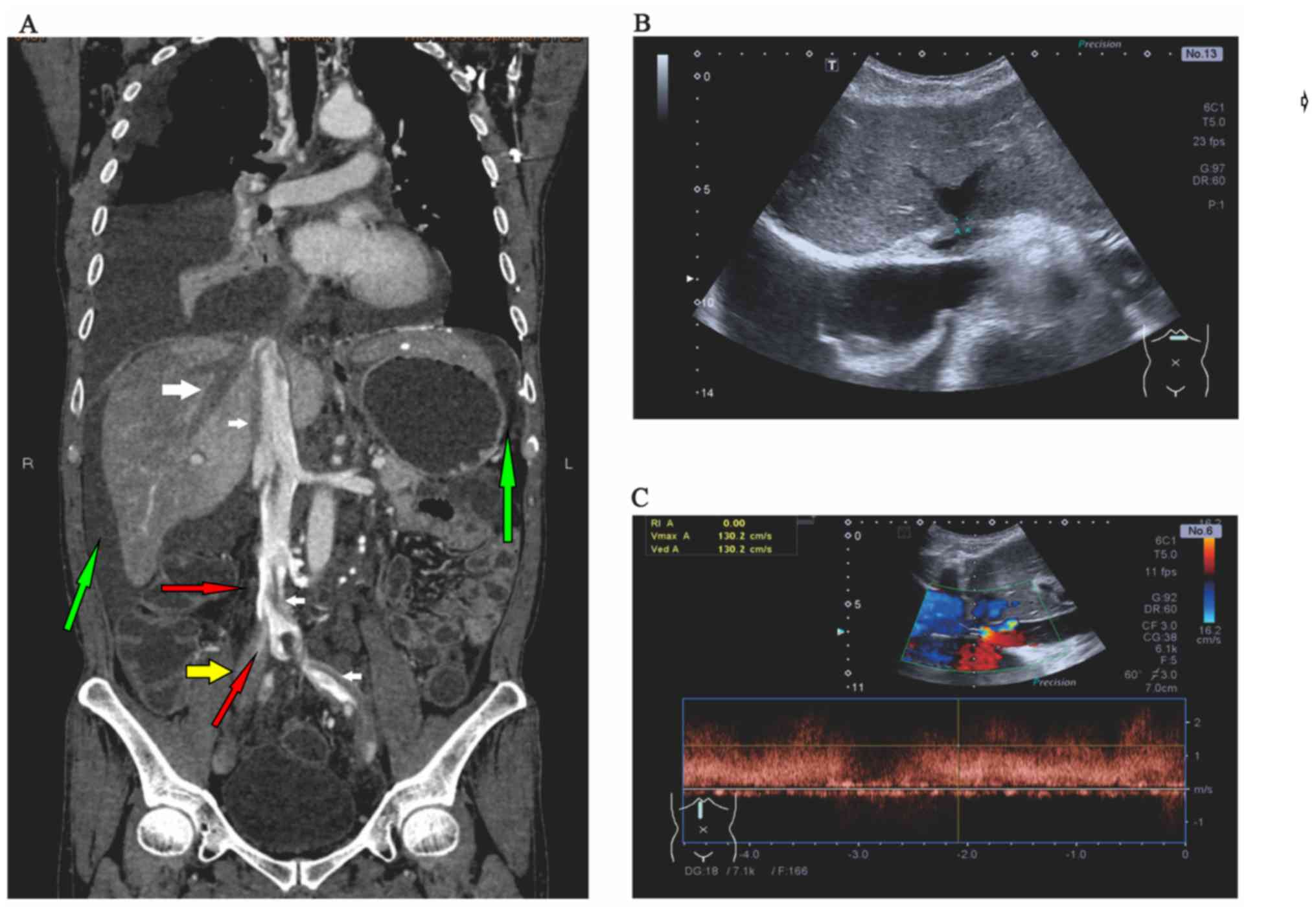
reagents). Abdominal computed tomography (CT) presented thrombus in
the hepatic vein (Fig. 1A; large
white arrow), mural thrombus in the inferior vena cava (Fig. 1A; small white arrows) and thrombus in
the right common iliac vein (Fig.
1A; yellow arrow). There was also evidence of free fluid
(Fig. 1A; green arrows) and
collaterals (Fig. 1A; red arrows).
An ultrasound revealed stenosis of the second hepatic hilum
(Fig. 1B) and evidence of pleural
effusion and ascites. Color Doppler sonography revealed stenosis of
the inferior vena cava and increased blood flow at the site of
stenosis (Fig. 1C). Together, these
results lead to the diagnosis of BCS.
Following the diagnosis of BCS due to BD, the
patient received IV methylprednisolone (60 mg) once a day for 2
weeks and pulse intravenous cyclophosphamide (CYC; 600 mg every 2
weeks). However, pleural fluid and abdominal distention persisted.
The patient was then administered infliximab (5 mg/kg) in addition
to ongoing IV CYC and methylprednisolone treatment. The case study
responded well to this treatment following 2 doses of infliximab
(repeated after 2 weeks) at which point the symptoms resolved, and
CRP fell to a normal level. Methylprednisolone was then adminstered
orally and tapered to 4–8 mg per week.
However, following discharge after ~1 month of
hospital admission, the patient terminated infliximab treatment due
to financial issues. He was admitted to two other hospitals
multiple times every 2–3 months and was administered aperiodic
anticoagulants including warfarin (the specific dose or
administration frequency could not be obtained). During IV CYC
treatment, the patient complained of increasing abdominal
distension and abdominal pain, but refused a CT scan. A year
following the initial diagnosis, he was readmitted for hemoptysis
and severe abdominal distention. On arrival, he was confused and
oxygen saturation was 72% at 10 l/min oxygen (normal values,
>90%). The doctors suggested intensive care but the family
refused and left the hospital without further notification.
Case 2
A 43-year-old Chinese man was admitted in September
2012 with fatigue, dyspnea following exercise, abdominal distension
and swelling of the legs and scrotum. In the previous 2 years, the
patient had experienced recurrent abdominal distension and swelling
of the legs. He had no history of drug use or other diseases.
Moderate alcoholism was reported, but no smoking or family history
of liver disease or thrombosis was indicated. The patient had been
diagnosed with liver cirrhosis in other hospitals prior to
presentation to The First Affiliated Hospital of Sun Yat-sen
University, (Guangzhou, China).
Physical examination revealed fever, tachycardia,
oral ulceration, swelling of the scrotum, pitting edema of leg
skin, acneiform eruptions on the legs and an increasing abdominal
volume. Laboratory tests are as follows: White blood cell count,
10.99×109/l (normal range, 4–10×109/l;
assessed with Mindray BC-6900, Mindray, Shenzhen, China); CRP, 9.35
mg/l (normal range, 0.00–3.00 mg/l; assessed with Mindray CRP-M100,
Shenzhen, China); ESR, 38 mm/h (normal male range, 0–15 mm/h);
TBIL, 21.4 µmol/l (normal range, 3.0–22.0 µmol/l); ALT, 60 U/l
(normal range, 0–40 U/l); AST, 134 U/l (normal range, 29–35 U/l);
ALB, 24.7 g/l (normal range, 35.0–50.0 g/l). ESR, TBIL, ALT, AST
and ALB were all assessed using the Beckman Coulter power processor
that contined all the required reagents (Beckman Coulter, Inc.).
The patient tested negative for ANA, ANCA and anti-cardiolipin
antibody (assessed using the Oumeng Euroline Plus kit, Beijing,
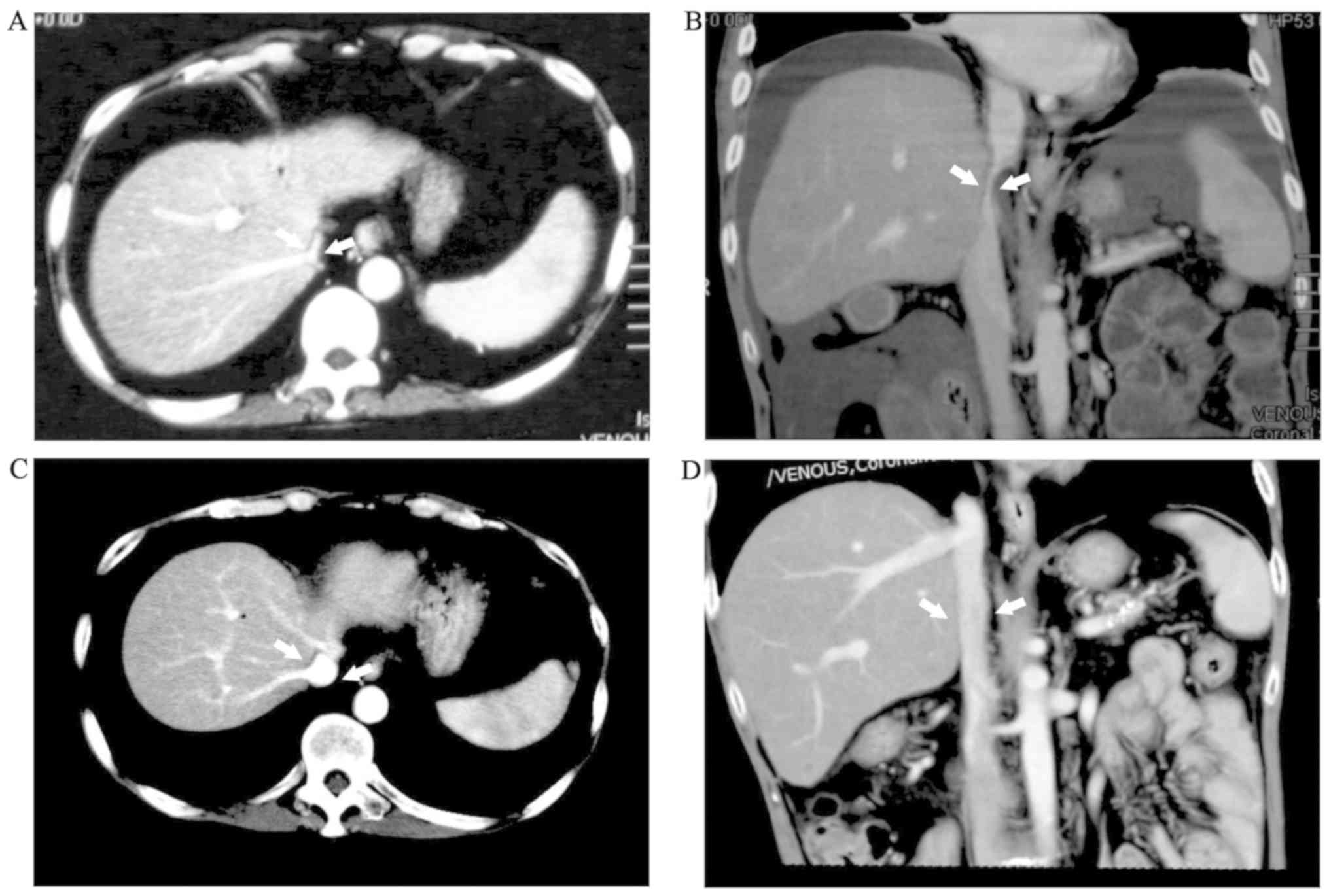
China). An abdominal CT scan revealed a narrow inferior vena cava
(Fig. 2A and B).
The patient was treated with anticoagulants and
responded poorly. Following a consultation with a rheumatologist
and a subsequent diagnosis of BD with BCS, the patient was
administered oral prednisone (30 mg/day), thalidomide (50 mg/day)
and pulse intravenous CYC (500 mg every 2 weeks). The symptoms
resolved following 3 weeks of treatment. The patient was
subsequently discharged from the hospital and continued CYC
treatment for a further 6 doses (over 12 weeks). However, the
patient returned 3 months later with recurrence of ascites and
swelling of the legs. He received prednisone and CYC as previously,
but little improvement was observed. He was then administered IV
infliximab (5 mg/kg; administered at week 0, week 2, weeks 6 and
then every 8 weeks) and oral methotrexate (MTX; 15 mg weekly). The
patient responded well to infliximab and symptoms resolved 10 days
following 2 weeks of one repeated treatment. Abdominal CT
re-examination revealed that the inferior vena cava diameter was
within the normal range, which confirmed the efficacy of the
treatment (Fig. 2C and D). The
patient was discharged and remained on the same dosage of
infliximab therapy for 6 weeks, then treatment with infliximab (5
mg/kg) every 8 weeks. Following 20 months of infliximab therapy, an
attack of pneumococcal pneumonia occurred on a very small steroid
dose (prednisone, 5 mg/day). Infliximab and immunosuppressant
therapy was stopped and the patient was treated with cefuroxime
(500 mg, twice a day for 7 days). Following resolution of the
infection, the patient was discharged and MTX (10–15 mg per week)
was administered for 1.5 years. Corticosteroid treatment was
gradually stopped, and no recurrences of BCS symptoms were observed
up to the time of last review, which occurred 38 months following
discharge.
Discussion
Vascular BD can lead to thromboses, occlusions and
aneurysms, and patients are at risk of developing vessel-associated
complications, resulting in a poor prognosis (10). Among all vascular involvements, lower
extremity deep vein and large artery lesions are the most common
(11).
Occlusion of the major hepatic veins, the adjacent
inferior vena cava, or both, is termed BCS and is rarely seen in
BD. It has been reported that BD-BCS accounts for 3% BCS diagnoses
(12,13) and BCS is estimated to occur in 1–3%
patients with BD (14). BCS can be
asymptomatic for a long duration and a small proportion of cases
present as fulminant hepatic failure (14). The condition of the patient depends
on the rate of hepatic vein blockage and the compensatory
collateral circulation (15,16). In countries where BD is prevalent,
awareness of BCS is important (6).
As a serious complication of BD, BD-BCS is associated with a high
mortality rate (12); however,
efficient medical intervention may lead to favorable outcomes.
Early diagnosis is therefore important for patients with BCS to
receive prompt and specific treatment (12). Furthermore, misdiagnosis may occur if
the patient is not diagnosed with BD prior to BCS (8,9). Case 2
initially presented with symptoms of liver cirrhosis and was given
non-specific treatment, but was diagnosed with BD 6 months later at
The First Affiliated Hospital of Sun Yat-sen University. It is
therefore important that rheumatologists are included at
consultations for these patients. The case also revealed that
corticosteroids and CYC treatment induced the first observed
remission.
Treatment choices for BD-BCS are not standardized
due to the lack of high quality randomized controlled trials;
however, glucocorticoids, CYC, azathioprine and thalidomide are the
most advocated therapies (17).
Immunosuppressive agents have also been associated with favorable
outcomes in numerous cases, meaning that surgical/endovascular
intervention may be avoided (17).
However, anticoagulation alone or in combination with surgery has
not been demonstrated to be as effective as immunosuppressive
agents (9). The use of
anticoagulants therefore remains controversial. A previous study
has demonstrated that patients who received only anticoagulation
therapy had favorable outcomes (9).
However, the 2008 Eular recommendation discouraged the use of
anticoagulants, as they were associated with a higher risk of
aneurysm rupture and bleeding (18).
The present study included two cases in which
initial CYC treatment induced remission, but this was not
sustained. Case 1 was unique as hemoptysis occurred during CYC
treatment, which was indicative of pulmonary vascular involvement.
Multiple vessel lesions and associated complications in ≥2 sites
are common in BD (19). However, BCS
and pulmonary vascular involvement occurring at the same time has
not been frequently reported (19).
It appeared that CYC treatment was not sufficient in case 1;
however, this patient was occasionally administered anticoagulants,
which may explain the observed pulmonary bleeding. An inadequate
response to initial conventional immunosuppressive treatment may
occur in certain patients. Tumor necrosis factor-α (TNF-α)
inhibitors have been reported to be a successful alternative in CYC
refractory vasculo-BD cases (20–24). The
patients described in the present study were administered add-on
infliximab, either following failure of conventional therapy or
relapse, and fast responses were observed. Case 2 was able to
terminate their use of corticosteroids, infliximab and CYC, and a
sustained remission was exhibited whilst taking MTX. Case 1
responded quickly to infliximab; however, the patient was prevented
from completing therapy. TNF-α inhibitors were useful in reduced
and sustained remission in the presented cases. TNF-α blockers have
been used to treat various manifestations of BD (25). Previous studies have demonstrated
that successful infliximab and adalimumab therapy has been achieved
in vasculo-BD, uveoretinitis, entero-BD, neuro-BD and BD arthritis
(25,26). TNF-α is considered a key element in
the inflammatory pathway of BD. Previous studies have identified
that TNF-α expression produced by γδ T cells is increased in the
peripheral blood of patients with active BD and TNF-α mRNA
expression was revealed to decrease following TNF-α blocker
treatment (27,28). Overall, the present study indicates
that TNF-α targeted treatment in BD may be effective. With the
advantage of producing a fast response, TNF-α blockers are
relatively safe and highly tolerable compared with CYC (26). However, whether TNF-α blockers should
be included in the first line treatment of BD-BCS is yet to be
determined.
In summary, BCS is a rare but potentially
threatening complication of BD and multiple vessel lesions in ≥2
sites are common. Misdiagnosis may occur if other symptoms of BD
are unnoticed. Therefore, the early diagnosis and appropriate
treatment of BD may lead to favorable outcomes. Furthermore, CYC
and corticosteroids are effective in the majority of cases.
Acknowledgements
Not applicable.
Funding
The present study was supported by the National
Natural Science Foundation of China (grant no. 81102270) and the
Guangdong Natural Science Foundation (grant nos. 2014A030313053 and
2016A030313217).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request, but no information infringing on the privacy of the
participants will be given.
Authors' contributions
FL and JZ conceived and designed the current study.
YW, HX and FL collected the data. JZ, YW, YL and HZ analyzed the
data, JZ and FL wrote the manuscript. All authors read and approved
the final manuscript
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Declaration of Helsinki, and the protocol was approved by the
Ethics Committee of the First Affiliated Hospital of Sun Yat-sen
University [Guangzhou, China; Project identification code, (1481)
541729].
Patient consent for publication
All patients provided their consent for the
publication of their data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
International Team for the Revision of the
International Criteria for Behçet's Disease (ITR-ICBD): The
international criteria for Behçet's disease (ICBD): A collaborative
study of 27 countries on the sensitivity and specificity of the new
criteria. J Eur Acad Dermatol Venereol. 28:338–347. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Calamia KT, Schirmer M and Melikoglu M:
Major vessel involvement in Behçet disease. Curr Opin Rheumatol.
17:1–8. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tascilar K, Melikoglu M, Ugurlu S, Sut N,
Caglar E and Yazici H: Vascular involvement in Behçet's syndrome: A
retrospective analysis of associations and the time course.
Rheumatology (Oxford). 53:2018–2022. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sarica-Kucukoglu R, Akdag-Kose A, KayabalI
M, Yazganoglu K, Disci R, Erzengin D and Azizlerli G: Vascular
involvement in Behçet's disease: A retrospective analysis of 2319
cases. Int J Dermatol. 45:919–921. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Valla DC: Primary Budd-Chiari syndrome. J
Hepatol. 50:195–203. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Uskudar O, Akdogan M, Sasmaz N, Yilmaz S,
Tola M and Sahin B: Etiology and portal vein thrombosis in
Budd-Chiari syndrome. World J Gastroenterol. 14:2858–2862. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sakr M, Barakat E, Abdelhakam S, Dabbous
H, Yousuf S, Shaker M and Eldorry A: Epidemiological aspects of
Budd-Chiari in Egyptian patients: A single-center study. World J
Gastroenterol. 17:4704–4710. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Carvalho D, Oikawa F, Matsuda NM and
Yamada AT: Budd-Chiari syndrome in association with Behçet's
disease: Review of the literature. Sao Paulo Med J. 129:107–109.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Desbois AC, Rautou PE, Biard L, Belmatoug
N, Wechsler B, Resche-Rigon M, Zarrouk V, Fantin B, de Chambrun MP,
Cacoub P, et al: Behcet's disease in Budd-Chiari syndrome. Orphanet
J Rare Dis. 9:1042014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yazici Y, Yurdakul S and Yazici H:
Behcet's syndrome. Curr Rheumatol Rep. 12:429–435. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ozen S, Bilginer Y, Besbas N, Ayaz NA and
Bakkaloglu A: Behçet disease: Treatment of vascular involvement in
children. Eur J Pediatr. 169:427–430. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ben Ghorbel I, Ennaifer R, Lamloum M,
Khanfir M, Miled M and Houman MH: Budd-chiari syndrome associated
with Behçet's disease. Gastroenterol Clin Biol. 32:316–320. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Batur A, Dorum M, Yüksekkaya HA and Koc O:
Budd-chiari syndrome and renal arterial neurysms due to Behcet
disease: A rare association. Pan Afr Med J. 21:842015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Springer J and Villa-Forte A: Thrombosis
in vasculitis. Curr Opin Rheumatol. 25:19–25. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hadengue A, Poliquin M, Vilgrain V,
Belghiti J, Degott C, Erlinger S and Benhamou JP: The changing
scene of hepatic vein thrombosis: Recognition of asymptomatic
cases. Gastroenterology. 106:1042–1047. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Langlet P, Escolano S, Valla D,
Coste-Zeitoun D, Denie C, Mallet A, Levy VG, Franco D, Vinel JP,
Belghiti J, et al: Clinicopathological forms and prognostic index
in Budd-Chiari syndrome. J Hepatol. 39:496–501. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Barnes CG: Treatment of Behçet's syndrome.
Rheumatology (Oxford). 45:245–247. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hatemi G, Silman A, Bang D, Bodaghi B,
Chamberlain AM, Gul A, Houman MH, Kötter I, Olivieri I, Salvarani
C, et al: EULAR recommendations for the management of Behçet
disease. Ann Rheum Dis. 67:1656–1662. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jayachandran NV, Rajasekhar L,
Chandrasekhara PK, Kanchinadham S and Narsimulu G: Multiple
peripheral arterial and aortic aneurysms in Behcet's syndrome: A
case report. Clin Rheumatol. 27:265–267. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Baki K, Villiger PM, Jenni D, Meyer T and
Beer JH: Behçet's disease with life threatening haemoptoe and
pulmonary anerusyms: Complete remission after infliximab treatment.
Ann Rheum Dis. 65:1531–1532. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Endo LM, Rowe SM, Romp RL, Buckmaster MA
and Atkinson TP: Pulmonary aneurysms and intracardiac thrombi due
to Behçet's disease in an African-American adolescent with
oculocutaneous albinism. Clin Rheumatol. 26:1537–1539. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lee SW, Lee SY, Kim KN, Jung JK and Chung
WT: Adlimumab treatment for life threatening pulmonary artery
aneurysms in Behçet disease: A case report. Clin Rheumatol.
29:91–93. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Schreiber BE, Noor N, Juli CF and Haskard
DO: Resolution of Behçet's syndrome associated pulmonary arterial
aneurysms with infliximab. Semin Arthritis Rheum. 41:482–487. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Aamar S, Peleg H, Leibowitz D,
Chajek-Shaul T, Hiller N and Heyman SN: Efficacy of adalimumab
therapy for life-threatening pulmonary vasculitis in Behçet's
disease. Rheumatol Int. 34:857–860. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Comarmond C, Wechsler B, Bodaghi B, Cacoub
P and Saadoun D: Biotherapies in Behçet's disease. Autoimmun Rev.
13:762–769. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Saleh Z and Arayssi T: Update on the
therapy of Behçet disease. Ther Adv Chronic Dis. 5:112–134. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Misumi M, Hagiwara E, Takeno M, Takeda Y,
Inoue Y, Tsuji T, Ueda A, Nakamura S, Ohno S and Ishigatsubo Y:
Cytokine production profile in patients with Behçet's disease
treated with infliximab. Cytokine. 24:210–218. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Parlakgul G, Guney E, Erer B, Kılıcaslan
Z, Direskeneli H, Gul A and Saruhan-Direskeneli G: Expression of
regulatory receptors on γδ T cells and their cytokine production in
Behcet's disease. Arthritis Res Ther. 15:R152013. View Article : Google Scholar : PubMed/NCBI
|