Introduction
Pulmonary fibrosis, particularly idiopathic
pulmonary fibrosis (IPF), is a serious interstitial lung disease of
unknown etiology, posing a major threat to human health. Due to the
lack of effective drugs or treatments, the mortality rate
associated with this condition is high. The median survival time of
patients with IPF is estimated to be 3–5 years (1), which is worse compared with that of
certain types of cancer (2). While
the pathogenesis of pulmonary fibrosis is complex and has remained
to be fully elucidated, the prevailing hypothesis is that repeated
injury to the alveolar epithelium, together with a subsequent
ineffective wound healing response and fibroblast activation,
ultimately leads to pulmonary fibrosis (3–5).
The current understanding of the detailed
pathogenesis of pulmonary fibrosis primarily relies on the use of
animal models (6). An ideal animal
model must resemble the basic characteristics of the human disease
to allow for testing of specific hypotheses and their feasibility
of constructing such a model in order to improve the understanding
of the underlying mechanisms (7). To
date, a number of animal species have been used as experimental
models for studying pulmonary fibrosis, including mice, rats, dogs,
hamsters, guinea pigs and primates (8). When using experimental animals,
multiple external interventions have been reported as capable of
inducing pulmonary fibrosis, including bleomycin (BLM), silica or
asbestos exposure, as well as cytokine overexpression, fluorescent
isothiocyanate (FITC) and radiation (7,9–11). Among them, FITC is a chemical
compound used to induce experimental pulmonary fibrosis.
Fluorescein acts as a hapten and binds to airway proteins, thus
acting as a depot for prolonged exposure to the injurious stimulus
leading to fibrotic responses within 2–4 weeks that persist up to
24 weeks. Disadvantages of this model include absence of
representative UIP characteristics and predominant inflammatory
infiltrates that precede fibrosis (11). Although different animal models
employing different interventions have their specific advantages
and drawbacks, no single model has fully reproduced the
histological pattern of interstitial pneumonia characteristic for
human IPF to date. However, it is worth noting that animal models
provide a key link between preclinical research and application of
treatments in human clinical trials, and represent the foundation
and a prerequisite for the development of treatments for human
diseases. A recent consensus reached in an official American
Thoracic Society workshop is that the use of the intratracheal BLM
mouse model is the best-characterized animal model available for
preclinical testing (12). BLM is a
pro-fibrotic agent that causes DNA single- and double-strand
breaks, with result in cell apoptosis and fibrosis. The advantage
of intratracheal administration of BLM in mice is that it requires
only a single instillation, which may better reproduce the
development of fibrotic disease within a short period of time
(7). For the treatment of IPF, a
number of clinical trials have been completed based on preclinical
studies in animal models, and two candidate drugs, namely
pirfenidone and nintedanib, have emerged as potential treatments
for IPF (13,14). The two drugs were proven effective at
slowing the progression of pulmonary fibrosis, although the
treatment is not curative (3).
With the advancements in biological and medical
technology, stem cell transplantation has been demonstrated to have
a potential application in the treatment of various diseases. In
this regard, bone marrow mesenchymal stem cells (BMSCs) have been
indicated to be promising for inhibiting the onset and treating
pulmonary fibrosis (15–18). BMSCs represent a class of
non-hematopoietic stem cells in the bone marrow interstitium, with
a high degree of self-replication and multidirectional
differentiation potential. Of note, BMSCs have a strong
immunosuppressive capacity with low immunoreactivity, rendering
them safe as autografts or allografts (19). BMSCs have also been indicated to
ameliorate BLM-induced pulmonary inflammation and fibrosis
(20). A recent study using a
similar model in aged mice reported that early intervention with
allogeneic adipose-derived mesenchymal stromal cells attenuated
lung and skin fibrosis and accelerated wound healing (21). In animal models, with regard to the
frequency of dosing and the selection of treatment time-points, the
majority of the experiments have examined the effects of a single
intratracheal administration of BLM, and the selected time of
treatment was usually within 1–7 days after BLM exposure (22–24).
However, this type of approach examines the therapeutic effect on
acute inflammation rather than on chronic fibrosis, limiting its
application in human IPF.
Based on the abovementioned data, the present study
aimed to examine the efficacy of BMSC intervention on BLM-induced
pulmonary fibrosis models and compare the difference in efficacy
between early and late intervention, focusing on pathology,
including alveolitis and pulmonary fibrosis scores. By reviewing
these preclinical data and providing a meta-analysis, the present
study aimed to clarify certain issues, including the timing of
treatment and its effectiveness on pulmonary fibrosis and, finally,
the relevance of animal model studies in human IPF.
Materials and methods
Search strategy
The present study followed the Preferred Reporting
Items for Systematic Reviews and Meta-Analysis guidelines (25). Studies examining the effect of BMSCs
on animal models of pulmonary fibrosis published in Chinese or
international biomedical journals between 2005 and 2017 were
retrieved. All searches were performed in 2017 and the language was
limited to English and Chinese. The search terms included ‘bone
marrow mesenchymal stem cells’, ‘pulmonary fibrosis’, ‘bleomycin’
and ‘animal model’. The search was performed in the PubMed,
MEDLINE, Chinese Knowledge Infrastructure and WanFang databases to
obtain comprehensive information.
Inclusion criteria and study
selection
According to the specified inclusion and exclusion
criteria, studies were first assessed by reading the title and
abstract. The inclusion criteria were as follows: The study design
focused on in vivo experiments of BLM-induced murine
pulmonary fibrosis and the intervention was injection of BMSCs via
the tail vein; the studies included a sufficient amount of samples
(experimental and control groups); the exposure factor was
intratracheal instillation of BLM; the intervention was injection
of BMSCs via the tail vein; the gold standard for diagnosis and
staging of diseases with increased fibrous tissue was
histopathological analysis and the primary outcome was
histopathological changes, including alveolar inflammation score
and pulmonary fibrosis score; the inclusion of the design and
research methods described above were similar and the data were
complete. If the exposure factor was not BLM, if the intervention
included cells other than BMSCs, or if the alveolitis or pulmonary
fibrosis scores were not assessed, the study was excluded.
Data extraction and quality
assessment
Two authors (E-GZ and YY) performed the search and
selection of studies and disagreements were resolved by
consultation. Data were entered into an Excel database by two
authors (E-GZ and YY). The following data were extracted: The basic
components of the selected studies (strains, sample size,
intervention measures, number of injected cells, transplant time
and outcome time) and the outcome indicators (alveolitis and
pulmonary fibrosis scores). The methodological qualities were
evaluated by two independent reviewers (E-GZ and YY) and
differences were resolved by consulting a third reviewer (S-YC).
The following items were assessed according to the standards
recommended by the Cochrane Handbook 5.0 (26) and the SYRCLE animal experimental bias
risk assessment tool (27). The
biases assessed included randomization, blinding for researchers,
blinding for outcome evaluators, selective reporting, concealed
allocation and other biases.
Statistical analysis
Data were analyzed with Review Manager software,
version 5.0 (Cochrane, London, UK). For continuous data, the mean
difference (MD) and 95% confidence interval (CI) were determined to
assess the treatment effects. Data were pooled using the
fixed-effects model (FEM), but the random-effects model (REM) was
also considered to ensure the robustness of the model (28,29). The
percentage of variability across trials attributable to
heterogeneity beyond chance was estimated using I2
statistics, which was deemed significant when P<0.05 or
I2>50% (30). In case
of significant heterogeneity (I2>50%), the
DerSimonian method and Laird REM were adopted as the pooling
method. Subgroup analyses were performed according to different
outcome times in the animal models after early BMSC
transplantation. P<0.05 was considered to indicate a
statistically significant difference.
Results
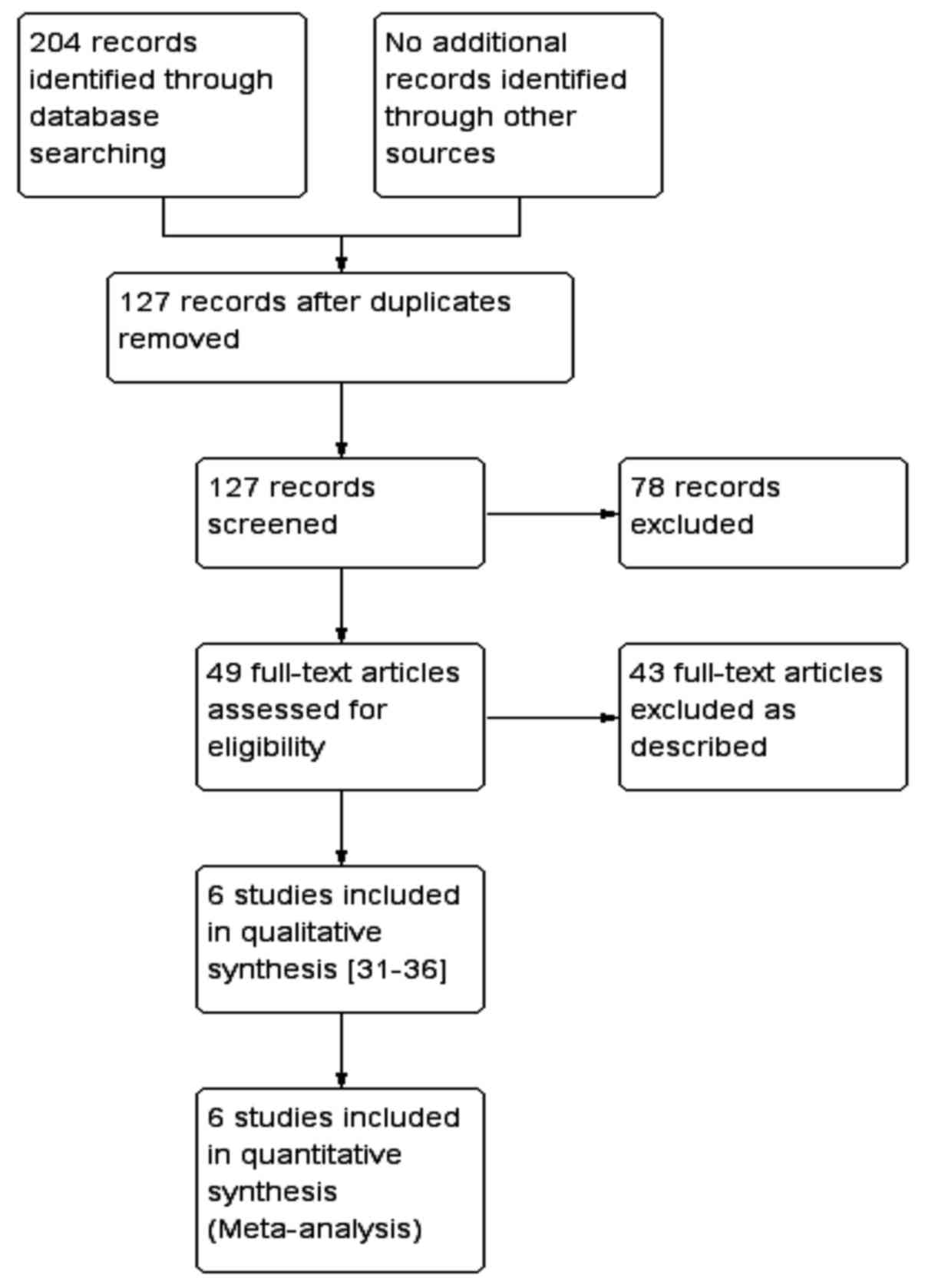
Search results
After a comprehensive search, a total of 204 studies
were retrieved, among which 6 were finally included according to
the previously described inclusion criteria (31–36). A
schematic of the screening process and selection of studies for
inclusion in the meta-analysis is provided in Fig. 1.
Characteristics of included
studies
The 6 experimental animal studies included in the
present meta-analysis (31–36) comprised 228 model rats; of these, 131
were subjected to treatment and 97 were used as controls. All of
the 6 studies were performed with a single tracheal injection of
bleomycin at a dose of 5 mg/kg. The studies mainly evaluated the
histopathological changes in the lung after early and late
transplantation of BMSCs. Early transplantation was defined as
immediate transplantation of BMSCs after BLM administration. All of
the 6 studies reported a score for alveolitis and pulmonary
fibrosis after early transplantation of BMSCs. A total of 168 rats
were included in the 6 studies. Late transplantation was defined as
the transplantation of BMSCs on day 14 after administration of BLM
to the rats, and a total of 3 studies, including 48 rats, evaluated
the score of alveolitis and pulmonary fibrosis after late
transplantation of BMSCs (31,34,35).
Detailed information on each study is presented in Table I. The results of the bias risk
assessment for each of the included studies is provided in Table II. Only Huang et al (33) reported that sequence generation was
grouped by the random number table method, the other studies did
not describe a specific randomization method. No study described a
concealed allocation, blinding for researchers and outcome
evaluators.
 | Table I.Characteristics of the included
studies. |
Table I.
Characteristics of the included
studies.
|
|
| Intervention
measures |
|
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|---|
| Author, year | Number of samples
(T/C) | T | C | Number of injected
cells | Transplant time
after modeling (days) | Outcome time
(days) | Outcome
indicator | (Refs.) |
|---|
| Yang et al,
2016 | 30/15 | BLM+BMSCs | BLM+saline |
0.2×107 | 1,14 | 7,14,28 | a,b | (31) |
| Cui et al,
2007 | 16/16 | BLM+BMSCs | BLM+PBS |
2.5×106 | 1,7 | 28 | a,b | (32) |
| Huang et al,
2012 | 18/18 | BLM+BMSCs | BLM+saline |
2.5×106 | 1 | 7,14,28 | a,b | (33) |
| Wang et al,
2014 | 24/12 | BLM+BMSCs | BLM+saline |
1×106 | 1,14 | 28 | a,b | (34) |
| Wang et al,
2009 | 28/21 | BLM+BMSCs | None | 5 ml/kg | 1,14 | 7,14,28 | a,b | (35) |
| Zeng et al,
2016 | 15/15 | BLM+BMSCs | BLM+saline |
5×105 | 1 | 7,14,21 | a,b | (36) |
| Table II.Bias risk assessment of the included
studies. |
Table II.
Bias risk assessment of the included
studies.
| Author, year | Randomization | Concealed
allocation | Researcher
blinding | Outcome evaluator
blinding | Selective
reporting | Other biases | (Refs.) |
|---|
| Yang et al,
2016 | Not described | Not clear | Not clear | Not clear | Not clear | Not clear | (31) |
| Cui et al,
2007 | Not described | Not clear | Not clear | Not clear | Not clear | Not clear | (32) |
| Huang et al,
2012 | Random number table
method | Not clear | Not clear | Not clear | Not clear | Not clear | (33) |
| Wang et al,
2014 | Not described | Not clear | Not clear | Not clear | Not clear | Not clear | (34) |
| Wang et al,
2009 | Not described | Not clear | Not clear | Not clear | Not clear | Not clear | (35) |
| Zeng et al,
2016 | Not described | Not clear | Not clear | Not clear | Not clear | Not clear | (36) |
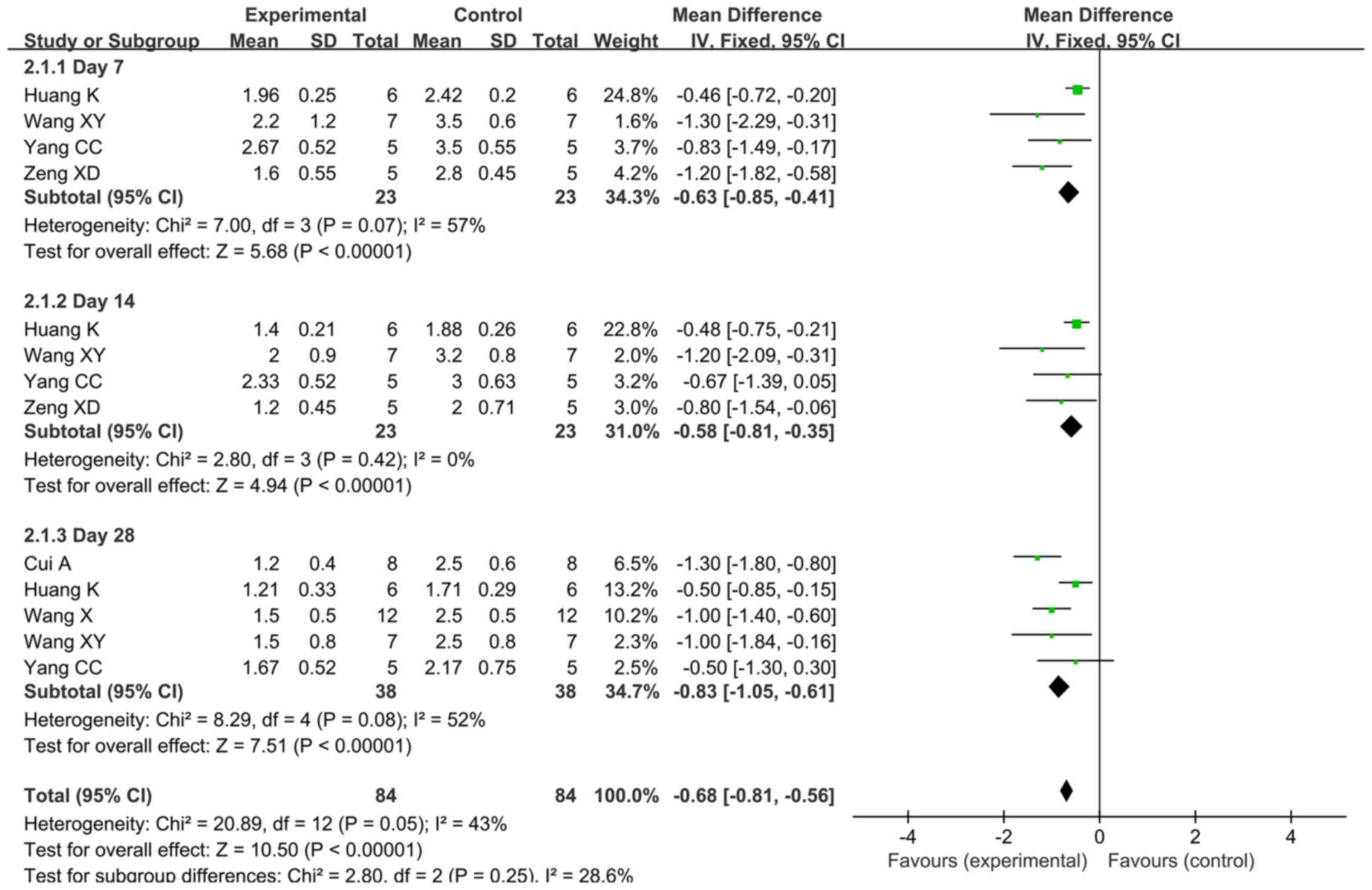
Amelioration of alveolitis after early
transplantation of BMSCs
FEM was used for meta-analysis, since the
heterogeneity of the alveolitis score after early transplantation
was 43% (<50%). The meta-analysis results demonstrated that the
alveolitis score in the early BMSC transplantation group was
superior to that in the control group, with a statistically
significant difference [MD=−0.68, 95% CI (−0.81, −0.56),
P<0.00001]. The forest plot of the comparison is provided in
Fig. 2. Further meta-analysis was
performed for three subgroups defined by outcome time (day 7, 14
and 28). A total of 4 studies provided alveolitis score on days 7
and 14 after early transplantation in a total of 46 rats (31,33,35,36). For
day 7, the REM was used for the meta-analysis, since heterogeneity
existed among the 4 studies regarding the score on day 7 (P=0.07,
I2=57%). For day 14, the FEM was used for meta-analysis,
since there was no heterogeneity among the 4 studies regarding the
score for that day (P=0.42, I2=0%). The results
demonstrated that the alveolitis score for the early
transplantation group was significantly better compared with that
in the control group on day 7 [MD=−0.84, 95% CI (−1.28, −0.40),
P=0.0002] and 14 [MD=−0.58, 95% CI (−0.81, −0.35),
P<0.00001].
The alveolitis score on day 28 after early
transplantation was reported by 5 studies including a total of 76
rats (31–35). The REM was used for meta-analysis,
since heterogeneity was present among these 5 studies (P=0.08,
I2=52%). The results demonstrated that the alveolitis
score of the early transplantation group was better compared with
that of the control group, with a statistically significant
difference [MD=−0.86, 95% CI (−1.20, −0.52), P<0.00001].
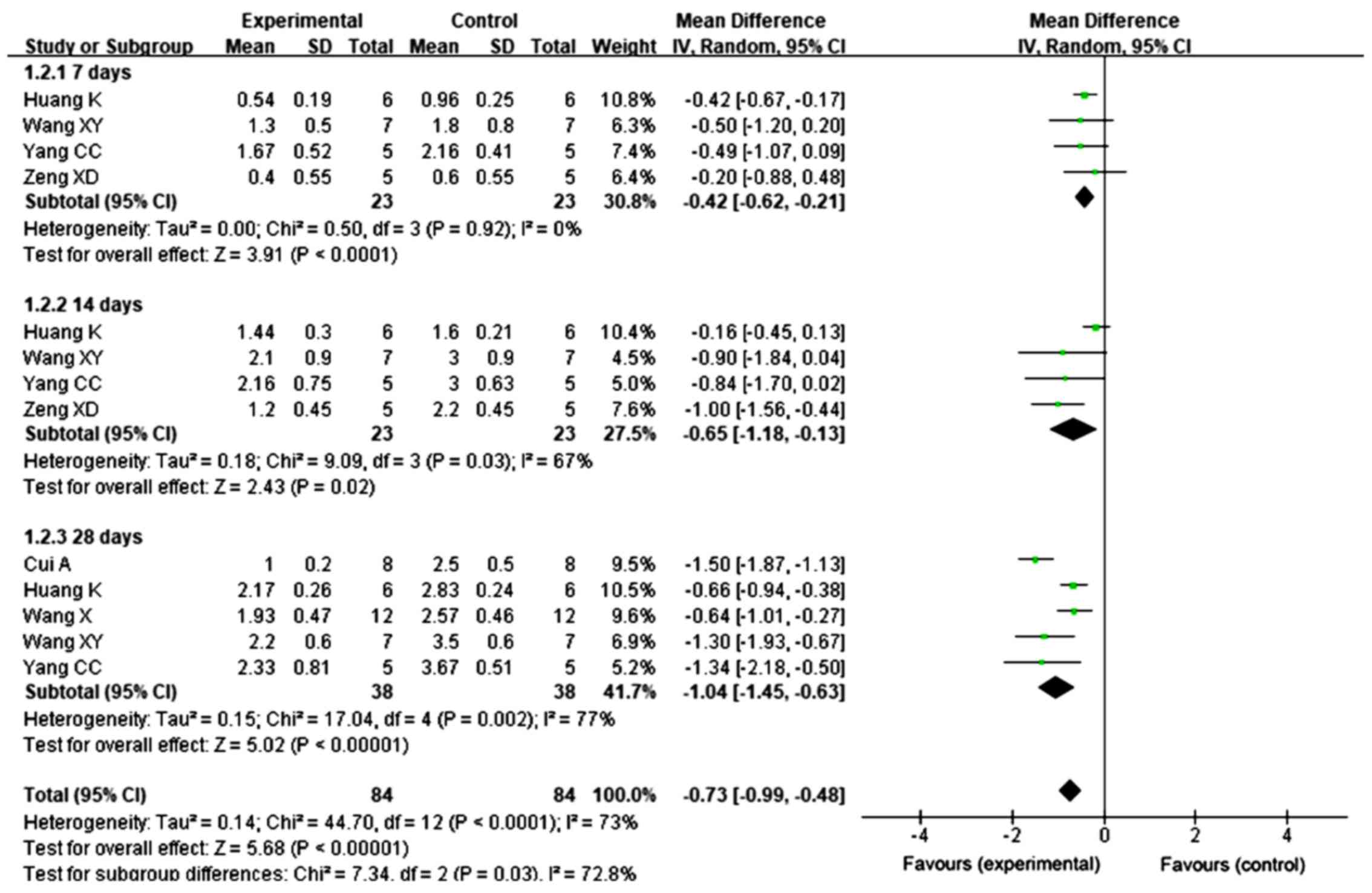
Improvement of pulmonary fibrosis
after early transplantation of BMSCs
REM was used for meta-analysis, since the
heterogeneity of the pulmonary fibrosis score after early
transplantation was 73% (>50%). The meta-analysis results
demonstrated that the pulmonary fibrosis score was significantly
improved in animals undergoing early BMSC transplantation compared
with that in the control group [MD=−0.73, 95% CI (−0.99, −0.48),
P<0.00001]. The forest plot of the comparison is provided in
Fig. 3. Further meta-analysis was
performed for 3 subgroups by outcome time (day 7, 14 and 28).
A total of 4 studies reported a score for pulmonary
fibrosis on days 7 and 14 after early transplantation in 46 rats
(31,33,35,36). The
FEM was used for the meta-analysis for day 7, since no
heterogeneity was among these 4 studies regarding the score on day
7 (P=0.92, I2=0%). For day 14, the REM was employed for
meta-analysis, since heterogeneity was present among the 4 studies
regarding the score on day 14 (P=0.03, I2=67%). The
results demonstrated that the pulmonary fibrosis score in the early
transplantation group was significantly different from that in the
control group on day 7 [MD=−0.42, 95% CI (−0.62, −0.21),
P<0.0001] and day 14 [MD=−0.65, 95% CI (−1.18, −0.13),
P=0.02].
A total of 5 studies reported on the pulmonary
fibrosis score on day 28 after early transplantation, in a total of
76 rats (31–35). The REM was used for meta-analysis,
since heterogeneity existed among these 5 studies (P=0.002,
I2=77%). The results demonstrated that the pulmonary
fibrosis score of the early transplantation group was better
compared with that of the control group, with a statistically
significant difference [MD=−1.04, 95% CI (−1.45, −0.63),
P<0.00001].
Improvement of alveolitis following
late transplantation of BMSCs
A total of 3 studies reported on the alveolitis
score following late transplantation of BMSCs (31,34,35). The
FEM was used for meta-analysis, since no heterogeneity was present
among the 3 studies regarding the alveolitis score on day 28
(P=0.82, I2=0%). The results demonstrated that the
alveolitis score on day 28 in the late transplantation group was
better compared with that in the control group, with a
statistically significant difference [MD=−0.46, 95% CI (−0.76,
−0.16), P=0.003; Fig. 4].
Pulmonary fibrosis score after late
transplantation of BMSCs revealed no evidence of improvement
A total of 3 studies reported on the pulmonary
fibrosis score following late transplantation of BMSCs (31,34,35). The
REM was used for meta-analysis, since heterogeneity was present
among these 3 studies for the score on day 28 (P=0.05,
I2=66%). No significant difference was observed in the
score for pulmonary fibrosis following transplantation of BMSCs on
day 14 after administration of BLM [MD=−0.51, 95% CI (−1.03, 0.00),
P=0.05; Fig. 5].
Sensitivity analysis
In order to assess the stability of the results of
the present study, the included studies were sequentially excluded,
and the combined effect was re-estimated, and changes in the
P-value and effect size were assessed. For the alveolitis scores,
following late transplantation of BMSCs, upon exclusion of the data
by Wang et al (34), which
resulted in MD=−0.36, 95% CI (−0.99, 0.27) and P=0.27, the
heterogeneity did not change. For the pulmonary fibrosis scores,
following late transplantation of BMSCs, upon exclusion of the data
from the study of Wang et al (34), which resulted in MD=−0.79, 95% CI
(−1.22, −0.36) and P=0.0003, the heterogeneity was reduced to 0%
(I2=0%), indicating that the results of the late
transplantation were sensitive and less stable. In order to explain
this result, the study by Wang et al (34) was again reviewed. The number of BMSCs
used in the study by Wang et al (34) (1×106) was lower than that
of the amount of cells injected in the other studies (Table I), and this and may be one of the
potential factors associated with bias. It may not be excluded that
any further potential factors led to this result. Of note, this
result must be interpreted with caution, and higher-quality and
more rigorous studies are required to validate the authenticity and
reliability of the result of late transplantation in the
future.
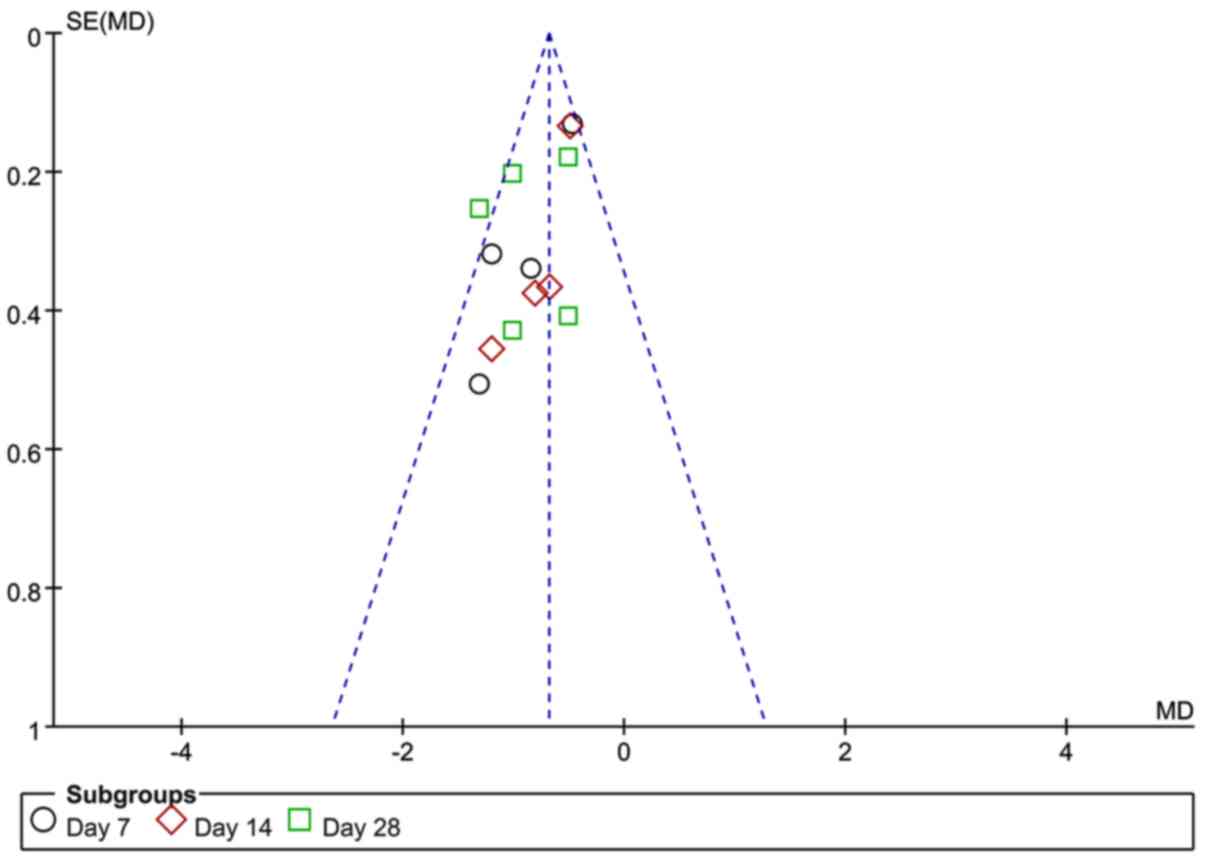
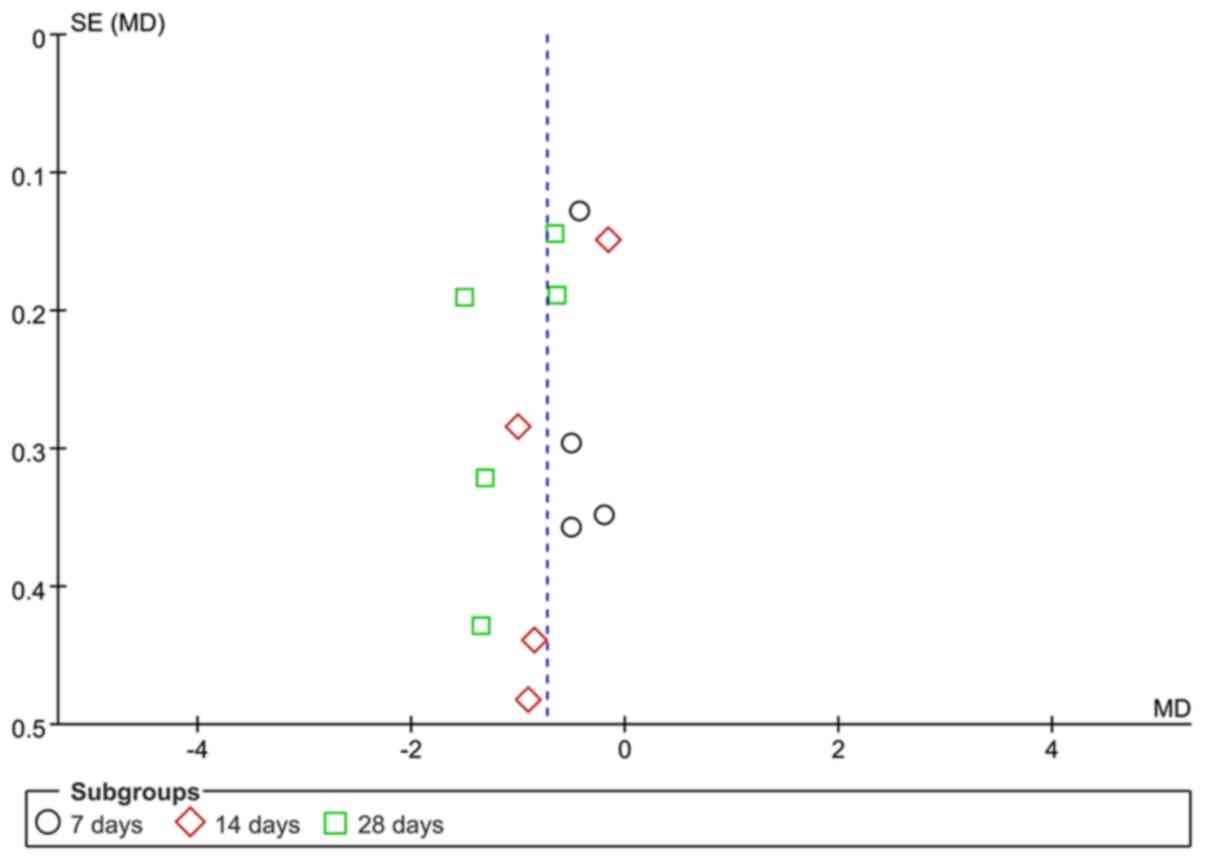
Analysis of publication bias
The scores of alveolitis and pulmonary fibrosis were
analyzed by funnel plots. The funnel plot for the alveolitis score
after early transplantation of BMSCs was less symmetrical,
suggesting the possible presence of publication bias (Fig. 6). The funnel plot for the pulmonary
fibrosis score after early transplantation of BMSCs revealed that
the two sides exhibited a degree of symmetry. Due to the limited
number of studies involved, publication bias cannot be excluded
(Fig. 7).
Discussion
In the present study, previously published
experimental animal studies on BMSC transplantation for the
treatment of BLM-induced pulmonary fibrosis we reviewed and
subjected to a meta-analysis. The aim of the present study was to
gain insight into the efficacy of this procedure and whether it may
be employed as a potential approach for the treatment of human IPF.
Specifically, histopathological changes, including alveolitis and
pulmonary fibrosis scores, were examined in order to compare the
efficacy of early transplantation of BMSCs with that of
transplantation at a late stage on BLM-induced fibrosis in animal
models. Early transplantation refers to BMSCs being injected on the
same day after administration of BLM, with the rats sacrificed on
days 7, 14 and 28, followed by assessment of alveolitis and
pulmonary fibrosis. Late transplantation refers to the BMSCs
injected on day 14 after administration of BLM, with the rats
sacrificed on day 28 and the efficacy assessed in terms of
alveolitis and pulmonary fibrosis. The criteria for scoring
alveolitis and pulmonary fibrosis in the studies included were
based on the method of Szapiel et al (37). In brief, alveolitis was evaluated
using hematoxylin and eosin-stained sections and was graded as
described therein, and fibrosis was determined using Masson's
trichrome-stained sections and again graded according to the
criteria described. The criteria for alveolitis scoring in the
study by Yang and Wu (31) were also
as described above, and scoring of pulmonary fibrosis was a
modification of that described by Szapiel et al (37), as described by Briggs et al
(38), who reported subtle
differences in the scores. Clearly, the approaches used to define
these conditions were largely uniform. After review of the
literature, a total of 6 studies were included in the present
meta-analysis. The results of these studies demonstrated that
alveolitis and pulmonary fibrosis scores were significantly
improved at 7, 14 and 28 days in the early transplantation group,
indicating that early transplantation of BMSCs was able to
ameliorate alveolitis and pulmonary fibrosis induced by BLM. In the
late transplantation group, the results demonstrated that the
alveolitis score, but not the pulmonary fibrosis score, were
significantly different on day 28 after BMSC injection, suggesting
that late transplantation of BMSCs may only lead to improvement of
alveolitis. However, when the study by Wang et al (34) was excluded, since the number of
injected cells or other potential factors were sources of bias in
that study, the P-values of the scores of alveolitis and pulmonary
fibrosis after late transplantation of BMSCs vs. the control were
markedly changed, indicating that the sensitivity was higher and
the stability of the result was lower. The results of the present
meta-analysis demonstrated that late transplantation of BMSCs
improves alveolitis, but there was no clear evidence regarding
improvement of pulmonary fibrosis. However, this result must be
interpreted with caution and higher-quality and more rigorous
studies are required to validate the authenticity and reliability
of these results in the future.
BLM is a chemotherapeutic antibiotic and has been
identified as a pro-fibrotic agent (11). BLM-induced pulmonary fibrosis in
animals has been considered to be the most commonly used
experimental model. Of note, the severity of the course in
BLM-induced pulmonary fibrosis in experimental animals depends on
their age and sex. Previous studies reported that higher age and
male sex may increase pulmonary inflammation and formation of
fibrotic lesions, and that aged male C57BL/6 mice develop more
severe BLM-induced pulmonary fibrosis compared with that of
aged-matched female mice or younger mice of either sex (11). However, in general, pulmonary
fibrosis induced by BLM usually develops rapidly through the
following stages: i) Overproduction of reactive oxygen species in
the first 3 days, leading to massive epithelial cell death; ii)
formation of a large inflammatory cell infiltrate on days 3–9; iii)
activation of fibroblasts with the deposition of a large amount of
extracellular matrix and consequent occurrence of fibrosis on days
10–28 (8,11,39,40). The
first 7 days after exposure to BLM represent the acute inflammatory
phase, after which time lung fibrosis gradually forms and peaks on
the 14th day at the molecular and histological levels (8,11). Thus,
drug intervention during the first 1–7 days after exposure to BLM
actually prevents inflammation, but not fibrosis per se. In
the present meta-analysis, the appearance of inflammation occurred
at the same time as the early transplantation of BMSCs, explaining
for the higher effectiveness of this treatment in preventing
fibrosis. Late transplantation of BMSCs was performed exactly on
day 14 after BLM exposure, when fibrosis is at its peak. Therefore,
treatment intervention at day 14 was efficacious in the treatment
of acute fibrosis, and this result is of relevance in human
IPF.
It has been previously reported that transplanting
BMSCs at different time-points after treatment exhibited
differential efficacy in treating pulmonary fibrosis in animal
models. Early transplantation exerted a better effect compared with
late transplantation (41). It is
also noteworthy that, in previous studies with mice exposed to
ionizing radiation and subsequently receiving late transplantation
of BMSCs carrying green fluorescent protein, a transformation from
macrophages to fibroblasts was observed, which defines the period
of rapid development of fibrosis (42). Therefore, late transplantation of
BMSCs may even accelerate pulmonary fibrosis. However, the present
review provided evidence that BMSC therapy is beneficial in rodents
with BLM-induced pulmonary fibrosis, and that the efficacy of early
transplantation appears to be more satisfactory.
Of note, the present study has certain strengths and
limitations. Through assessing the scores for alveolitis and
pulmonary fibrosis, the present meta-analysis systematically
evaluated the efficacy of early and late BMSC transplantation for
the treatment of BLM-induced pulmonary fibrosis in rats. Data from
animal studies provide important insight into the processes
underlying pulmonary fibrosis, which may enhance the current
understanding of the initiation, progression and development of
human IPF. The results of the present study indicated that stem
cell transplantation applied as an early intervention appears to be
more effective. This is most likely due to the effect of early
transplantation to inhibit inflammation in the early stage. This,
in turn, suggests that early intervention by anti-inflammatory
drugs may be effective in treating IPF in humans. Unfortunately, no
effective biomarkers are currently available for early detection of
human IPF, which makes early intervention difficult. While the
animal models allow for the examination of the steps involved in
the progression to fibrosis, it has not been fully elucidated
whether similar changes occur during the development of human
IPF.
Although late transplantation of BMSCs was able to
reduce alveolitis, there was no clear evidence regarding the
improvement of pulmonary fibrosis. However, for the alveolitis and
pulmonary fibrosis scores following late transplantation of BMSCs
were sensitive and less stable. Higher-quality and more rigorous
studies are required to address the effectiveness of late
intervention, since this strategy more closely resembles the
treatment in humans.
Of note, the present study has certain limitations.
For instance, the animal models reviewed only included rats.
Previous studies reported that C57BL/6J mice are highly susceptible
to lung injury following intratracheal BLM administration.
Therefore, this strain may be an alternative model for
investigating BLM-induced pulmonary fibrosis (43,44).
Another limitation was that the number of studies included was
small and certain studies may have publication bias. Table II presents information on bias
regarding allocation concealment, blinding and random assignments.
For instance, only Huang et al (33) reported that rats were grouped by the
random number table method, the other studies did not describe a
specific random method. No study described concealed allocation,
blinding for researchers and outcome evaluators (Table II). Although all studies used the
tail vein injection route for cell transplantation, the transplant
BMSC number was not equal (Table I).
Of note, certain studies reported that exogenous transplanted BMSCs
for silicosis exerted an antagonistic effect, with enhanced
pathological pulmonary fibrotic changes due to excessive BMSC
transplantation (17). The presence
of a dose-effect association was evident. However, in the present
study, it was not possible to determine whether the number of
exogenous transplanted BMSCs affects BLM-induced pulmonary
fibrosis. In addition, the SD was high in several studies, which
may have affected the pooled data. Of note, the sensitivity
analysis of the meta-analysis suggested that the results of late
transplantation of BMSCs were sensitive and less stable. Therefore,
it is required to interpret the results with caution.
Higher-quality and more rigorous studies are required to validate
the results of the present meta-analysis in the future.
In conclusion, the present study provided evidence
that early transplantation of BMSCs improves the scores of
alveolitis and pulmonary fibrosis induced by BLM in rat models.
However, late transplantation of BMSCs was able to reduce
alveolitis, but the majority of studies provided no evidence
indicating improvement of pulmonary fibrosis. Although BMSC therapy
appears to be beneficial in rodent models of BLM-induced pulmonary
fibrosis, the efficacy of early transplantation appears to be more
satisfactory, indicating that the efficacy of transplantation of
BMSCs at the acute inflammatory phase is more effective compared
with that at the chronic fibrosis stage. Of note, regarding the
scores following late transplantation of BMSCs, the results were
sensitive and less stable, and this result must therefore be
interpreted with caution. More rigorous studies are required in the
future to confirm the results of the present meta-analysis. In
addition, most of the present data refer to the effect of early
BMSC transplantation on the improvement of pulmonary fibrosis,
while limited results are available for late transplantation.
Therefore, it is recommended that future studies focus on
transplantation of BMSCs at a more advanced stage and its long-term
benefits.
Acknowledgements
Not applicable.
Funding
This study was supported by grants from the National
Natural Science Foundation of China (grant no. 81602893), the
Natural Science Foundation of Shandong Province (grant nos.
ZR2015YL049 and ZR2018MH036), the Medical and Health Technology
Development Plan Project of Shandong Province (grant no.
2016WS0540), the Key Research and Development Plan of Shandong
Province (nos. 2017GSF18186 and 2018GSF118018) and the Innovation
Project of Shandong Academy of Medical Science.
Availability of data and materials
The datasets generated and analyzed during the
present study are available from the corresponding author upon
reasonable request.
Authors' contributions
HS and ZD obtained funding and designed the study.
EZ and YY performed the analysis and interpretation of the data,
and wrote the manuscript. JZ, GD and SC performed the analysis and
interpretation of data. AJY, CP and MFL provided technical support
for the analysis and critical revision of the manuscript. All
authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
BMSCs
|
bone marrow mesenchymal stem cells
|
|
BLM
|
bleomycin
|
|
IPF
|
idiopathic pulmonary fibrosis
|
|
MD
|
mean difference
|
|
CI
|
confidence interval
|
|
ATS
|
American Thoracic Society
|
|
REM
|
random effects model
|
|
FEM
|
fixed effects model
|
References
|
1
|
Raghu G, Weycker D, Edelsberg J, Bradford
WZ and Oster G: Incidence and prevalence of idiopathic pulmonary
fibrosis. Am J Respir Crit Care Med. 174:810–816. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tzouvelekis A, Bonella F and Spagnolo P:
Update on therapeutic management of idiopathic pulmonary fibrosis.
Ther Clin Risk Manag. 11:359–370. 2015.PubMed/NCBI
|
|
3
|
Ahluwalia N, Shea BS and Tager AM: New
therapeutic targets in idiopathic pulmonary fibrosis. Aiming to
rein in runaway wound-healing responses. Am J Respir Crit Care Med.
190:867–878. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ryu JH, Moua T, Daniels CE, Hartman TE, Yi
ES, Utz JP and Limper AH: Idiopathic pulmonary fibrosis: Evolving
concepts. Mayo Clin Proc. 89:1130–1142. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tzouvelekis A and Kaminski N: Epigenetics
in idiopathic pulmonary fibrosis. Biochem Cell Biol. 93:159–170.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Degryse AL and Lawson WE: Progress toward
improving animal models for idiopathic pulmonary fibrosis. Am J Med
Sci. 341:444–449. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mouratis MA and Aidinis V: Modeling
pulmonary fibrosis with bleomycin. Curr Opin Pulm Med. 17:355–361.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Moore BB and Hogaboam CM: Murine models of
pulmonary fibrosis. Am J Physiol Lung Cell Mol Physiol.
294:L152–L160. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dong LH, Jiang YY, Liu YJ, Cui S, Xia CC,
Qu C, Jiang X, Qu YQ, Chang PY and Liu F: The anti-fibrotic effects
of mesenchymal stem cells on irradiated lungs via stimulating
endogenous secretion of HGF and PGE2. Sci Rep. 5:87132015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fireman E: A silica-induced pulmonary
fibrosis model: Are we closer to ‘real life’ ? Int Arch Allergy
Immunol. 158:211–212. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tashiro J, Rubio GA, Limper AH, Williams
K, Elliot SJ, Ninou I, Aidinis V, Tzouvelekis A and Glassberg MK:
Exploring animal models that resemble idiopathic pulmonary
fibrosis. Front Med (Lausanne). 4:1182017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jenkins RG, Moore BB, Chambers RC,
Eickelberg O, Königshoff M, Kolb M, Laurent GJ, Nanthakumar CB,
Olman MA, Pardo A, et al: An official American thoracic society
workshop report: Use of animal models for the preclinical
assessment of potential therapies for pulmonary fibrosis. Am J
Respir Cell Mol Biol. 56:667–679. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
King TE Jr, Bradford WZ, Castro-Bernardini
S, Fagan EA, Glaspole I, Glassberg MK, Gorina E, Hopkins PM,
Kardatzke D, Lancaster L, et al: A phase 3 trial of pirfenidone in
patients with idiopathic pulmonary fibrosis. N Engl J Med.
370:2083–2092. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Richeldi L, du Bois RM, Raghu G, Azuma A,
Brown KK, Costabel U, Cottin V, Flaherty KR, Hansell DM, Inoue Y,
et al: Efficacy and safety of nintedanib in idiopathic pulmonary
fibrosis. N Engl J Med. 370:2071–2082. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li X, Wang Y, An G, Liang D, Zhu Z, Lian
X, Niu P, Guo C and Tian L: Bone marrow mesenchymal stem cells
attenuate silica-induced pulmonary fibrosis via paracrine
mechanisms. Toxicol Lett. 270:96–107. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ni S, Wang D, Qiu X, Pang L, Song Z and
Guo K: Bone marrow mesenchymal stem cells protect against
bleomycin-induced pulmonary fibrosis in rat by activating Nrf2
signaling. Int J Clin Exp Pathol. 8:7752–7761. 2015.PubMed/NCBI
|
|
17
|
Zhao MM, Cui JZ, Cui Y, Li R, Tian YX,
Song SX, Zhang J and Gao JL: Therapeutic effect of exogenous bone
marrow-derived mesenchymal stem cell transplantation on silicosis
via paracrine mechanisms in rats. Mol Med Rep. 8:741–746. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhou MI, Chen DL, Jiang T, Feng YM and Han
XL: Effects of bone marrow-derived mesenchymal stem cells
transfected with survivin on pulmonary fibrosis in mice. Exp Ther
Med. 10:1857–1864. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Abumaree M, Al Jumah M, Pace RA and
Kalionis B: Immunosuppressive properties of mesenchymal stem cells.
Stem Cell Rev. 8:375–392. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yu SH, Liu LJ, Lv B, Che CL, Fan DP, Wang
LF and Zhang YM: Inhibition of bleomycin-induced pulmonary fibrosis
by bone marrow-derived mesenchymal stem cells might be mediated by
decreasing MMP9, TIMP-1, INF-γ and TGF-β. Cell Biochem Funct.
33:356–366. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rubio GA, Elliot SJ, Wikramanayake TC, Xia
X, Pereira-Simon S, Thaller SR, Glinos GD, Jozic I, Hirt P, Pastar
I, et al: Mesenchymal stromal cells prevent bleomycin-induced lung
and skin fibrosis in aged mice and restore wound healing. J Cell
Physiol. 233:5503–5512. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ortiz LA, Dutreil M, Fattman C, Pandey AC,
Torres G, Go K and Phinney DG: Interleukin 1 receptor antagonist
mediates the antiinflammatory and antifibrotic effect of
mesenchymal stem cells during lung injury. Proc Natl Acad Sci USA.
104:11002–11007. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ortiz LA, Gambelli F, McBride C, Gaupp D,
Baddoo M, Kaminski N and Phinney DG: Mesenchymal stem cell
engraftment in lung is enhanced in response to bleomycin exposure
and ameliorates its fibrotic effects. Proc Natl Acad Sci USA.
100:8407–8411. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rojas M, Xu J, Woods CR, Mora AL, Spears
W, Roman J and Brigham KL: Bone marrow-derived mesenchymal stem
cells in repair of the injured lung. Am J Respir Cell Mol Biol.
33:145–152. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hutton B, Salanti G, Caldwell DM, Chaimani
A, Schmid CH, Cameron C, Ioannidis JP, Straus S, Thorlund K, Jansen
JP, et al: The PRISMA extension statement for reporting of
systematic reviews incorporating network meta-analyses of health
care interventions: Checklist and explanations. Ann Intern Med.
162:777–784. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Higgins JP and Sally G: Cochrane Jandbook
for Systematic Reviews of Interventions. A John Wiley & Sons,
Ltd.; West Sussex: 2009
|
|
27
|
Hooijmans CR, Rovers MM, de Vries RB,
Leenaars M, Ritskes-Hoitinga M and Langendam MW: SYRCLE's risk of
bias tool for animal studies. BMC Med Res Methodol. 14:432014.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
DerSimonian R and Kacker R: Random-effects
model for meta-analysis of clinical trials: An update. Contemp Clin
Trials. 28:105–114. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials. Control Clin Trials. 7:177–188. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lau J, Ioannidis JP and Schmid CH:
Quantitative synthesis in systematic reviews. Ann Intern Med.
127:820–826. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Yang CC and Wu XM: Inhibitory effect of
bone mesenchymal stem cells on pulmonary fibrosis in rats. Chin J
Int Med. 14:1091–1094. 2016.(In Chinese).
|
|
32
|
Cui A, Dai HP, Dai JW, Pang BS, Niu SJ, Lü
YP and Wang C: Effects of bone marrow mesenchymal stem cells on
bleomycin induced pulmonary fibrosis in rats. Zhonghua Jie He He Hu
Xi Za Zhi. 30:677–682. 2007.(In Chinese). PubMed/NCBI
|
|
33
|
Huang K, Wu XM, Wang XY, Kang XW, Xiao JL,
Li ZG and Lu P: The effect of marrow mesenchymal stem cell
transplantation on pulmonary fibrosis in rats. Zhonghua Jie He He
Hu Xi Za Zhi. 35:659–664. 2012.(In Chinese). PubMed/NCBI
|
|
34
|
Wang X, Zeng Y and Peng H: Inhibitory
effect of mesenchymal stem cells on pulmonary fibrosis in rats.
Acta Med Univ Sci Technol Huazhong. 3:300–303. 2014.
|
|
35
|
Wang XY, Wu XM, Huang K, Kang XW, Li B,
Chen FH and Bai L: The treatment of experimental pulmonary fibrosis
with bone mesenchymal stem cells transplantation. Chin J Rehab.
3:149–152. 2009.(In Chinese).
|
|
36
|
Zeng XD, Zhang W and Kang XH: Experimental
study of mesenchymal stem cell transplantation in the treatment of
bleomycin-induced pulmonary fibrosis in rats. J Gannan Med Uni.
1:20–23. 2016.
|
|
37
|
Szapiel SV, Elson NA, Fulmer JD,
Hunninghake GW and Crystal RG: Bleomycin-induced interstitial
pulmonary disease in the nude, athymic mouse. Am Rev Respir Dis.
120:893–899. 1979.PubMed/NCBI
|
|
38
|
Briggs BA, Bradley TM, Vernon P, Cooke NT,
Drinkwater C, Gillett MK and Snashall PD: Measurement of lung
tissue mass, thoracic blood and interstitial volumes by
transmission/emission scanning using [99mTc]pertechnetate. Clin Sci
(Lond). 73:319–327. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Schrier DJ, Kunkel RG and Phan SH: The
role of strain variation in murine bleomycin-induced pulmonary
fibrosis. Am Rev Respir Dis. 127:63–66. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Janick-Buckner D, Ranges GE and Hacker MP:
Alteration of bronchoalveolar lavage cell populations following
bleomycin treatment in mice. Toxicol Appl Pharmacol. 100:465–473.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhu HX, Gao JL, Zhao MM, Li R, Tian YX,
Wang X, Zhang J and Cui JZ: Effect of bone marrow mesenchymal stem
cell transplantation on silicosis fibrosis in different time
windows in rats. Chin J Immun. 193–196. 209:2015.
|
|
42
|
Epperly MW, Guo H, Gretton JE and
Greenberger JS: Bone marrow origin of myofibroblasts in irradiation
pulmonary fibrosis. Am J Respir Cell Mol Biol. 29:213–224. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Hoyt DG and Lazo JS: Alterations in
pulmonary mRNA encoding procollagens, fibronectin and transforming
growth factor-beta precede bleomycin-induced pulmonary fibrosis in
mice. J Pharmacol Exp Ther. 246:765–771. 1988.PubMed/NCBI
|
|
44
|
Stefanov AN, Fox J, Depault F and Haston
CK: Positional cloning reveals strain-dependent expression of
Trim16 to alter susceptibility to bleomycin-induced pulmonary
fibrosis in mice. PLoS Genet. 9:e10032032013. View Article : Google Scholar : PubMed/NCBI
|