Introduction
The incidence of nephrotic syndrome (NS) in children
is 0.16‰, and is a primary concern in pediatric nephrology. NS may
cause damage to the kidneys by enhancing glomerular basement
membrane permeability (1,2). The majority of diagnosed children have
steroid-sensitive nephrotic syndrome (SSNS), and ~20% of children
do not achieve complete remission and ultimately develop
steroid-resistant nephrotic syndrome (SRNS) (3). In addition, 80–90% of children with
SSNS undergo relapse, and in those that relapse, 50% experience
frequent relapses and develop steroid-dependent nephrotic syndrome
(SDNS) (4–6). Therefore, the treatment of pediatric
refractory nephrotic syndrome (PRNS), which includes SDNS and SRNS,
is challenging. Patients with PRNS are administered repeated,
long-term steroid therapy, which increases the risk of obesity,
cushingoid appearance, hypertension, growth retardation,
osteoporosis, infections and psychological problems (7).
Encouragingly, several investigations have used
tacrolimus (TAC), a steroid-sparing agent, to treat patients with
PRNS, which has improved responses and reduced adverse reactions to
steroid therapy (8–15). However, as a potent immunosuppressive
agent, the therapeutic window of TAC is narrow (16). Although adequate and continuous
immunosuppression is necessary, excessive immunosuppression may
give rise to severe adverse reactions, including infections and
toxicity. TAC pharmacokinetics (PK) have exhibited considerable
inter- and intra-individual variability, making it difficult to
define an optimal dosing schedule (16,17).
Using population PK (PPK), PK data may be acquired
by analyzing sparse data pooled from a group of people.
Furthermore, the PPK method is able to differentiate between inter-
and intra-individual variability. Thus, compared with traditional
PK, PPK has the power to verify the effect of multiple factors on
PK and may make it possible to determine an optimal dose schedule
(18). Currently, different TAC PPK
models have been set up in multiple populations, including patients
undergoing renal transplant (19–24),
liver transplant (25–30), hematopoietic stem cell transplant
(31) and lung transplant (32). However, the TAC PPK model for PRNS is
still unclear. The objective of the current study was to produce a
TAC PPK model in Chinese patients with PRNS and to analyze factors
involved in pharmacokinetic variability. The current study also
summarizes previous literature regarding TAC PPK models in
different pediatric diseases, including liver transplant (27,28,33–39),
kidney transplant (23) and
hematopoietic stem cell transplant (31).
Patients and methods
Patients and data collection
Patients <18 years of age, who were diagnosed
with PRNS and were receiving TAC therapy were recruited into the
present study. Patients were excluded if they presented with other
serious diseases, including kidney transplantation. A total of 65
Chinese patients (44 males and 21 females) with PRNS treated at the
Children's Hospital of Fudan University (Shanghai, China) between
January 2014 and October 2017 (2.4–16.4 years old; mean age,
7.6±3.9 years) were retrospectively analyzed. Drug concentrations
were collected from therapeutic drug monitoring (TDM) records and
relevant clinical information was acquired from medical records.
The study was approved by the Research Ethics Committee of the
Children's Hospital of Fudan University.
Information extracted from the medical records
included age, weight, daily dose of TAC (TAMT), albumin (ALB),
globulin (GLB), albumin/globulin (A/G), aspartate aminotransferase
(AST), alanine aminotransferase (ALT), creatinine (CR), total
protein (TP), cystatin-C (CYSC), gamma-glutamyl transpeptidase
(GGT), urea (UR), uric acid (UA), hematocrit (HCT), hemoglobin
(HGB), mean corpuscular hemoglobin (MCH), mean corpuscular
hemoglobin concentration (MCHC) and concomitant drugs
(corticosteroids, clarithromycin, ceftriaxone, warfarin,
simvastatin, cimetidine, ranitidine, omeprazole, nifedipine,
diltiazem, felodipine, fosinopril, dihydrochlorothiazide,
spirolactone, ciclosporin, mycophenolate mofetil, montelukast,
loratadine, piperazine ferulate, vitamin B6 and shegan mixture).
The information was verified for accuracy as comprehensively as
possible.
Drug administration
All patients received oral TAC (capsule, 1 and 0.5
mg). The initial TAC dose was 0.5–2.0 mg twice daily and the dose
range of TAC was 1.0–4.0 mg/day. The dose of TAC was adjusted based
on efficacy, adverse effects and the trough concentration in TDM.
All blood concentrations were collected prior to the subsequent
administration. The TAC concentrations used in the current research
were trough concentrations.
Analytical method
Whole blood concentrations of TAC were measured
using the Emit® 2000 Tacrolimus assay (Siemens
Healthineers, Erlangen, Germany), which was linear over the range
of 2.0–30.0 ng/ml and blood samples exceeding the upper limit of
the calibration range of 30.0 ng/ml were diluted according to the
manufacturer's protocol.
Population pharmacokinetic
modeling
Data were analyzed using a nonlinear mixed-effects
model computer program (NONMEM, version 7; ICON Development
Solutions, LLC, Ellicott City, MD, USA). The first-order
conditional estimation method with interaction option was used to
estimate PK parameters and their variability. A one-compartment
model with first-order elimination was used for describing the
absorption phase, since all the TAC concentrations in the current
research were trough concentrations. The bioavailability (F) and
absorption with a lag time could not be estimated because TAC was
orally administered and TAC concentration data were insufficient.
Thus, the PK parameters were comprised of apparent oral clearance
(CL/F) and apparent volume of distribution (V/F). The absorption
rate constant (Ka) of the model was set as 4.48 h−1,
according to what was previously set in the literature (28,40,41).
Random effect model
The inter-individual variability in PK parameters
was explored with additive, proportional and exponential error
models. The residual error variability was evaluated with additive,
proportional, exponential and mixed error models.
Covariate model
To determine the variability of PK parameters, the
associations were examined between covariates and all the PK
parameters where inter-individual variability was tested. The
possible covariates included age, weight, TAMT, ALB, GLB, A/G, AST,
ALT, CR, TP, CYSC, GGT, UR, UA, HCT, HGB, MCH, MCHC and concomitant
medication. The covariate model was established in a stepwise way.
To compare hierarchical models, a likelihood ratio test was
adopted. The change in objective function values (OFV) caused by
the inclusion of a covariate is proportional to twice the negative
log likelihood of the data and approximates a chi-square
distribution (42). In the
univariate analysis, a decrease in OFV >3.84 (P<0.05, degrees
of freedom = 1) was selected as a standard for inclusion of the
covariate in the base model. The significant covariates were
reserved in the model. When a full regression model was built, the
model was further validated by discarding the covariate of each
parameter one by one to acquire the final model. An increase in OFV
>6.64 (P<0.01, degrees of freedom = 1) was selected as a
standard to retain significant covariates in the final model.
Model validation
An internal validation bootstrap method was used to
evaluate the stability and reliability of parameter estimates in
the final model (43).
Goodness-of-fit plots applied to models were generated using R
software (version 3.4.2; http://www.r-project.org/). Bootstrapping was produced
using repeated random sampling with replacement of the original
data (44,45). This procedure was performed using the
software package Wings for NONMEM (version 7; ICON Development
Solutions, LLC) and repeated 2,000 times with different random
draws. Bootstrap outcomes with successful minimization and
acceptable covariance were applied for further analysis. The
medians and 2.5–97.5% percentiles in the bootstrap result set
parameters were compared with the parameter estimates of final
PK.
Summary of TAC PPK models in different
pediatric diseases
To investigate the differences and similarities in
TAC PPK models and factors that cause its variation among various
pediatric diseases, the study also provided a summary of previous
literature regarding TAC PPK models in pediatric patients with
PRNS, liver transplant, kidney transplant and hematopoietic stem
cell transplant. Studies between January 1995 and October 2017 were
retrieved from PubMed (https://www.ncbi.nlm.nih.gov/pubmed) and Web of
Science Knowledge (https://login.webofknowledge.com/). Search terms
included: Tacrolimus, population pharmacokinetics and relevant
pediatric diseases. Primary research papers matching the criteria
were identified and evaluated.
Results
Data collection
Whole blood concentration of TAC was evaluated in
147 samples from 65 Chinese patients with PRNS consisting of 44
males and 21 females, and data were made available for population
modeling. Patient characteristics and drug combinations are
summarized in Tables I and II, respectively.
 | Table I.Demographic and clinical
characteristics of patients (n=65). |
Table I.
Demographic and clinical
characteristics of patients (n=65).
| Characteristic | Mean ± SD | Median | Range |
|---|
| Age (years) |
7.61±3.92 | 6.8 |
2.4–16.4 |
| Weight (kg) |
30.85±17.12 | 25.0 |
13.5–86.5 |
| TAMT (mg) |
1.62±0.75 | 1.5 |
1.0–4.0 |
| A/G |
1.16±0.44 | 1.1 |
0.6–2.6 |
| ALB (g/l) |
25.41±8.87 | 24.1 |
12.3–45.3 |
| ALT (IU/l) |
9.91±6.48 | 8.0 |
2.0–35.0 |
| AST (IU/l) |
15.93±6.49 | 14.0 |
5.0–35.0 |
| CR (µmol/l) |
30.49±12.67 | 27.0 |
14.0–69.0 |
| GLB (g/l) |
22.16±3.32 | 22.6 |
15.2–31.2 |
| TP (g/l) |
47.51±10.22 | 46.9 |
29.5–69.1 |
| CYSC (mg/l) |
0.85±0.25 | 0.8 |
0.4–2.3 |
| GGT (IU/l) |
32.85±54.52 | 22.0 |
9.0–446.0 |
| UR (mmol/l) |
4.41±2.59 | 4.0 |
1.9–18.1 |
| UA (µmol/l) | 343.42±117.00 | 315.0 | 134.0–799.0 |
| HCT (%) | 42.62±4.94 | 42.6 |
27.4–55.3 |
| HGB (g/l) | 144.79±17.34 | 146.0 | 90.0–180.1 |
| MCH (pg) |
28.91±1.46 | 29.0 |
26.0–32.0 |
| MCHC (g/l) | 340.12±14.91 | 342.0 | 302.0–366.0 |
| Table II.Drug combinations administered to
patients. |
Table II.
Drug combinations administered to
patients.
| Drug | Category | n | % |
|---|
|
Corticosteroids | 0 | 1 | 1.5 |
|
| 1 | 64 | 98.5 |
| Clarithromycin | 0 | 64 | 98.5 |
|
| 1 | 1 | 1.5 |
| Ceftriaxone | 0 | 63 | 96.9 |
|
| 1 | 2 | 3.1 |
| Warfarin | 0 | 64 | 98.5 |
|
| 1 | 1 | 1.5 |
| Simvastatin | 0 | 64 | 98.5 |
|
| 1 | 1 | 1.5 |
| Cimetidine | 0 | 64 | 98.5 |
|
| 1 | 1 | 1.5 |
| Ranitidine | 0 | 64 | 98.5 |
|
| 1 | 1 | 1.5 |
| Omeprazole | 0 | 55 | 84.6 |
|
| 1 | 10 | 15.4 |
| Nifedipine | 0 | 64 | 98.5 |
|
| 1 | 1 | 1.5 |
| Diltiazem | 0 | 61 | 93.8 |
|
| 1 | 4 | 6.2 |
| Felodipine | 0 | 63 | 96.9 |
|
| 1 | 2 | 3.1 |
| Fosinopril | 0 | 52 | 80.0 |
|
| 1 | 13 | 20.0 |
|
Dihydrochlorothiazide | 0 | 42 | 64.6 |
|
| 1 | 23 | 35.4 |
| Spirolactone | 0 | 43 | 66.2 |
|
| 1 | 22 | 33.8 |
| Ciclosporin | 0 | 63 | 96.9 |
|
| 1 | 2 | 3.1 |
| Mycophenolate
mofetil | 0 | 63 | 96.9 |
|
| 1 | 2 | 3.1 |
| Montelukast | 0 | 63 | 96.9 |
|
| 1 | 2 | 3.1 |
| Loratadine | 0 | 63 | 96.9 |
|
| 1 | 2 | 3.1 |
| Piperazine
ferulate | 0 | 58 | 89.2 |
|
| 1 | 7 | 10.8 |
| Vitamin B6 | 0 | 64 | 98.5 |
|
| 1 | 1 | 1.5 |
| Shegan mixture | 0 | 61 | 93.8 |
|
| 1 | 4 | 6.2 |
Modeling and validation
A one-compartment model with first order absorption
and elimination was best fitted to the data. Ka was set at 4.48
h−1 according to the literature (28,40,41).
Furthermore, the Ka parameter was also tested using other values to
evaluate the sensitivity. Ka was increased or reduced 5-fold, from
0.896 to 22.4 h−1. However, the results of CL/F, V/F and
the OFV exhibited minimal changes. Using this method, it was
determined that the appropriate Ka value was 4.48 h−1.
The PK parameters of TAC, CL/F and V/F were estimated using NONMEM.
Inter-individual variability and residual variability were best
described by exponential and mixed error models, respectively. Of
all the tested covariates, only three had a significant effect on
PK parameters: Age, CYSC and TAMT on CL/F. No covariates notably
influenced V/F. The changes in OFV are presented in Table III. The final models were as
follows: CL/F = θCL/F × EXP(θAGE × age) ×
EXP(θCYSC × CYSC) × EXP (θTAMT × TAMT); V/F =
θV/F; where θCL/F and θV/F were
the typical population values of CL/F and V/F, respectively, and
θAGE, θCYSC and θTAMT were the
coefficients of age, CYSC and TAMT, respectively.
| Table III.Change of OFV in covariate
analysis. |
Table III.
Change of OFV in covariate
analysis.
| Step | Model
description | OFV | ∆OFV | P-value |
|---|
| Inclusion | Base model | 455.868 | N/A | N/A |
|
| Influence of age on
CL/F | 438.708 | −17.160 | <0.05 |
|
| Influence of CYSC
on CL/F | 427.426 | −11.282 | <0.05 |
|
| Influence of TAMT
on CL/F | 420.171 | −7.255 | <0.05 |
| Elimination | Full model | 420.171 | N/A | N/A |
|
| Eliminate age on
CL/F | 428.159 |
7.988 | <0.01 |
|
| Eliminate CYSC on
CL/F | 433.351 | 13.180 | <0.01 |
|
| Eliminate TAMT on
CL/F | 427.426 |
7.255 | <0.01 |
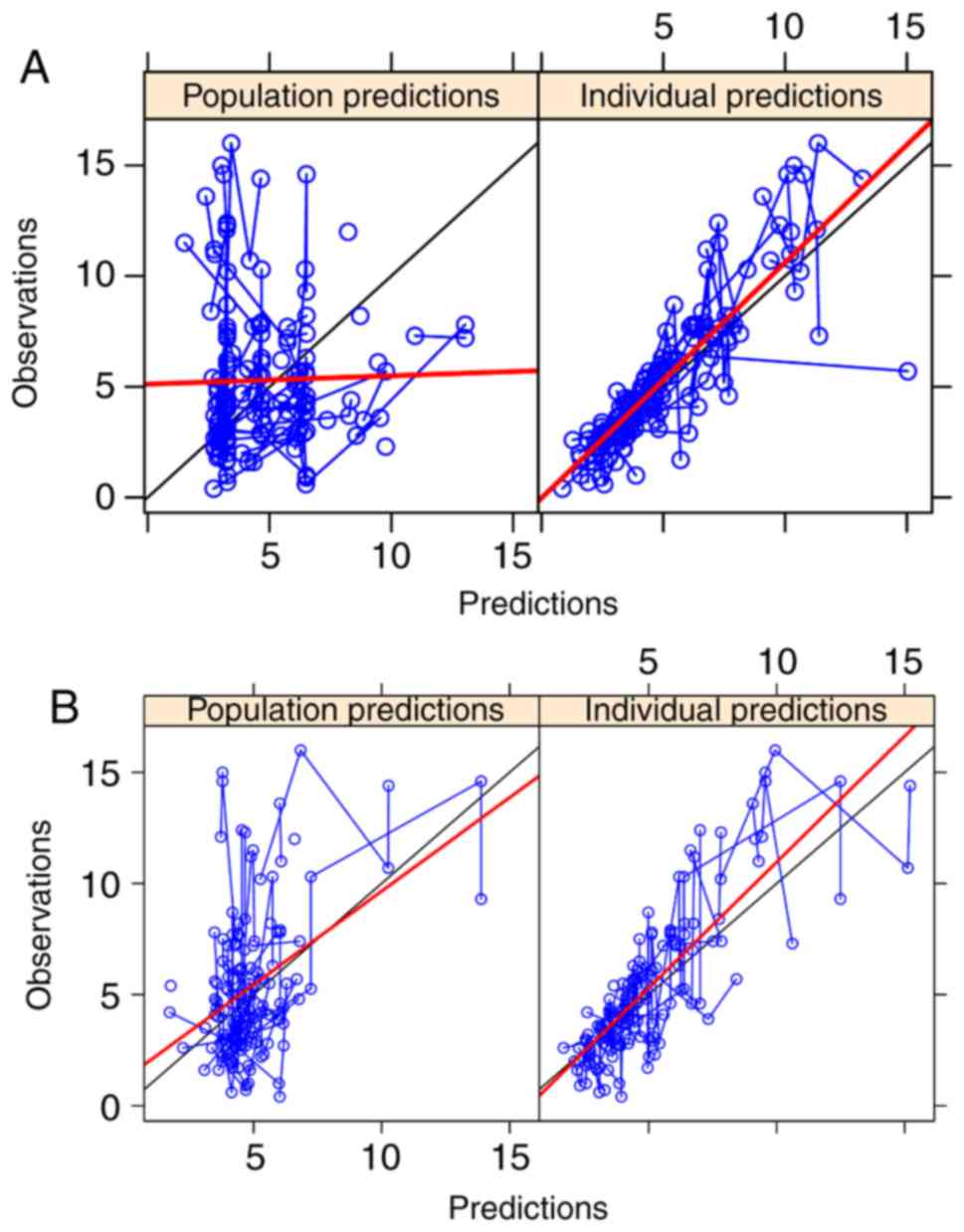
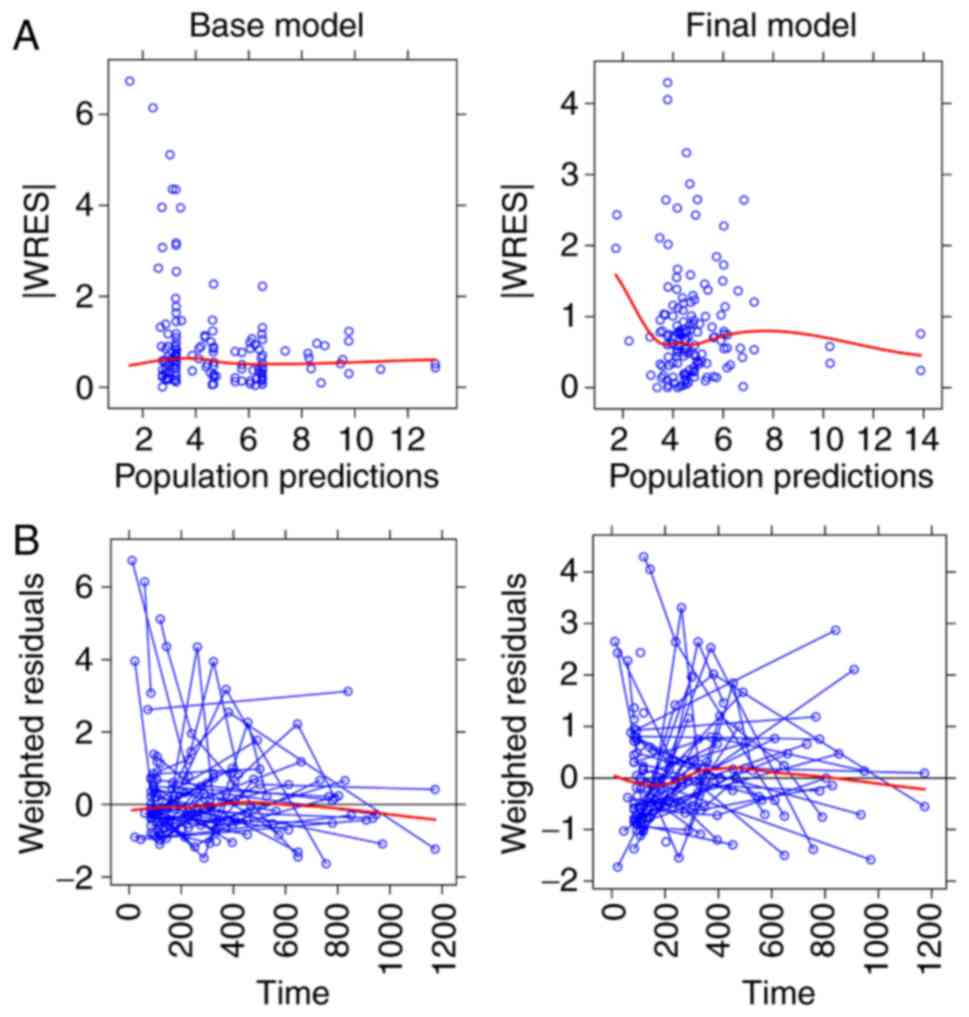
The goodness-of-fit plots of the final model
compared with the base model are presented in Figs. 1 and 2. From 2,000 bootstrap runs, 1,791 runs
were successfully minimized by covariance steps, and finally they
were added into the bootstrap analysis. The parameter estimates of
the final model and bootstrap validation are presented in Table IV. The median values of the
parameter estimated from bootstraps were near to the final model's
respective values, indicating that the PK parameter estimates from
the final model were precise and the model was reliable.
| Table IV.Parameter estimates of final model
and bootstrap validation. |
Table IV.
Parameter estimates of final model
and bootstrap validation.
|
|
|
| Bootstrap
(n=2000) |
|
|---|
|
|
|
|
|
|
|---|
| Parameter | Estimate | SE (%) | Median | 95% confidence
interval | Bias (%) |
|---|
| CL/F (l/h) | 5.4600 | 22.7 | 5.640 | [0.160, 9.895] | 3.297 |
| V/F (l) | 57.1000 | 46.8 | 59.500 | [0.298,
496.750] | 4.203 |
| Ka
(h-1) | 4.4800 (fixed) | N/A | N/A | N/A | N/A |
|
θAGE | 0.0323 | 35.0 | 0.033 | [0.007, 0.062] | 2.477 |
|
θCYSC | −0.3590 | 26.1 | −0.375 | [-0.719,
−0.087] | 4.457 |
|
θTAMT | 0.1480 | 47.9 | 0.140 | [0.012, 0.350] | −5.405 |
|
ωCL/F | 0.2220 | 18.5 | 0.216 | [0.053, 0.342] | −2.703 |
|
ωV/F | 0. 0020 | 48.5 | 0.001 | [0.001, 0.009] | −50.000 |
| σ1 | 0.3590 |
8.2 | 0.345 | [0.235, 0.417] | −3.900 |
| σ2 | 0.8040 | 31.5 | 0.806 | [0.003, 1.594] | 0.249 |
TAC PPK models in different pediatric
diseases
Twelve pediatric TAC PPK models were identified in
the literature, including the current PRNS model, nine liver
transplant models, one kidney transplant model and one
hematopoietic stem cell transplant model. Table V summarizes these PPK studies in
different pediatric diseases. However, TAC PPK models vary in
pediatric diseases, which indicates that disease state may lead to
differences in CL/F and V/F in different pediatric disease
populations.
| Table V.Population pharmacokinetics of
tacrolimus in different pediatric disease models. |
Table V.
Population pharmacokinetics of
tacrolimus in different pediatric disease models.
| Model | Reference | n | Age in years,
average (range) | Time
post-transplantation | Pharmacokinetic
parameters | BSV CL (%) | BSV V (%) | Refs. |
|---|
| Refractory
nephrotic syndrome | Current study | 65 | 6.8a (2.4–16.4) | NR | CL/F (l/h) = 5.46 ×
EXP(0.0323 × AGE) × EXP(−0.359 × CYSC) × EXP(0.148 × TAMT); V/F (l)
= 57.1; Ka (h−1) = 4.48 (fixed) | 22.2 | 0.2 | N/A |
| Liver
transplant | Yang et al,
2015 | 52 | 1.78b (0.42–17.8) | From the day after
transplantation | CL/F (l/h) = 5.72 ×
POD0.152 × (ALT/70)−0.111; V/F (l) = 131 ×
POD0.31 × (ALT/70)−0.317 ×
(TP/54)−2.01; Ka (h−1) = 4.48 (fixed) | 13.5 | 78.1 | 28 |
|
| Kassir et
al, 2014 | 30 | 7.3a (0.4–18.4) | ≤28 days, 8
patients; >28 days, 22 patients | CL/F (l/h) =12.1 ×
(WT/20)0.75; V1/F (l) = 31.3 ×
(WT/20)1; Q/F (l/h) = 30.7 × (WT/20)0.75;
V2/F (l) = 290 × (WT/20)1; Ka
(h−1) = 0.342 × (WT/20)−0.25; tlag
(h) =0.433 | 55.6 | 126.1 | 37 |
|
| Jalil et al,
2014 | 43 | 5b (0.65–17.56) | First year
post-transplantation | CL/F
(l/h)c = 12.9 ×
(WT/13.2)0.75 × e(−0.00158×POD) ×
e(0.428×hFLAG) | 40 | NR | 36 |
|
| Guy-Viterbo et
al, 2013 | 42 | 1.35a (0.53–10.93) | From the day after
transplantation until the patient experienced a rejection episode
or, alternatively, until the end of the first year | CL/F
(l/day)d = 0.001 × [1 +
(314×TIME) / (17.4 + TIME)] × [(Size / WT) / median (Size /
WT)]0.12 × (Hct/29)−0.85; V1/F (l)
= 253 × (WT/10.2)0.9; V2/F (l) =100 (fixed);
Q/F (l/day) = 115 | 54.8 | 77.5 | 35 |
|
| Wallin et
al, 2011 | 73 | 3.5a (0.4–16.9) | First year
post-transplantation | CL/F
(l/h/kg−0.75) = 0.148 + (1.37 × POD3.78) /
(5.383.78 + POD3.78); V/F (l/kg) = 27.2 | NR | 90 | 27 |
|
| Fukudo et
al, 2006 | 100 | 1.2a (0.1–15.0) | First 50 days
post-transplantation | CL/F
(l/h/kg)e = (0.134 ×
1.8iFLAG + 0.0181 × 2 hFLAG × XPOD) × 8.6 ×
(WT/8.6)0.341 × e(−0.0358×AST/53); V/F (l) =
17.1 × 8.6 × (WT/8.6)0.341 | 48.7 | 82.6 | 33 |
|
| Garcia Sanchez
et al, 2001 | 18 | 9.1a (0.3–16.0) | From 1 day to 6.8
years | CL (l/h) = 10.4 ×
(WT/70)0.75 × e(−0.00032T) ×
e(−0.057BILI) × (1 - 0.079 × ALT); F = 20% (fixed) | 24.3 | NR | 34 |
|
| Sam et al,
2000 | 20 | 3.7b (1.1–13.9) | 0–7 days | CL (l/h) = 1.46 ×
[1 + 0.339 × (AGE - 2.25)]; V (l) = 39.1 × [1 + 4.57 × (BSA-0.49)];
F (%) = 0.197 × (1 + 0.0887 × WT - 11.4), BILI <200 µmol/l; F
(%) = 0.197 × (1 + 0.0887 × WT - 11.4) × 1.61, BILI ≥200
µmol/l | 33.5 | 33 | 38 |
|
| Yasuhara et
al, 1995 | 33 | 4.2b (0.3–15) | 52 days | CL (l/h) = (0.0749
+ 0.000457 × POD) × [15 × (WT/15)0.29]; V (l) = 2.76 ×
[15 × (WT/15)0.29]; F =19% | 52.1 | 27.4 | 39 |
| Kidney
transplant | Zhao et al,
2009 | 50 | 10b (2–18) | During the initial
post-transplantation period (<2 months) | Ka (h−1)
= 0.462; tlag (h) =0.356; CL/F (l/h)f = 13.9 × (WT/70)0.75 ×
(2.26FLAG1) + 7.11 × (1.74 FLAG2);
V1/F (l) = 57.9 × (WT/70); V2/F (l) = 966 ×
(WT/70); Q/F (l) = 79.7 × (WT/70)0.75 | 41.9 | 132 | 23 |
| Hematopoietic stem
cell transplant | Wallin et
al, 2009 | 22 | 6b (0.5–18) | Within the first
year after stem cell transplantation | CL
(ml/h/kg−0.75) = 106 × [1 + 18.7 × (S-Crea−1
- S-Crea−1median)]; V (l/kg) = 3.71; F (%) =
15.7 × [1 + (−0.002) × POD - 14] | 50 | 122 | 31 |
Discussion
TAC has been used for the treatment of patients with
PRNS to improve their responses and reduce adverse reactions to
steroid therapy. Since TAC exhibits considerable inter- and
intra-individual PK variability, PPK analysis of TAC is crucial
(8–17). To the best of our knowledge, the
current model may be the first pediatric study of TAC PPK in
patients with refractory nephrotic syndrome. In the current study,
TAC PPK was performed in Chinese patients with PRNS using a
population modeling method, which was particularly applicable since
excessive blood sample collection is prohibited for pediatric
patients compared with traditional PK studies (46). A TAC PPK model that is able to
determine the pharmacokinetic process in individual patients with
PRNS may have important clinical applications.
In the current study, a one-compartment model with
first-order elimination was used for describing the absorption
phase, as all the TAC concentrations were trough concentrations,
and the Ka of the model was fixed at 4.48 h−1 (28,40,41). The
typical values of CL/F and V/F in the final TAC PPK model were 5.46
l/h and 57.1 l, respectively, and the CL/F value was similar to
that in a PPK model of TAC in Chinese pediatric patients shortly
after liver transplantation (28).
The current model also tested various covariates on different
parameters and the following covariates were determined to be
significant: Age, CYSC and TAMT on CL/F. Przepiorka et al
(47) also demonstrated that TAC
clearance was age-dependent in pediatric patients undergoing
hematopoietic stem cell transplant. Thus, CL/F of TAC was affected
by age in PRNS and pediatric hematopoietic stem cell
transplantation models; this may be associated with developmental
maturity and how this influences the clearance of TAC.
Cystatin-C, generated by all nucleated cells and
catabolized by proximal tubules, is a low molecular weight protein
that is part of the cysteine protease family (48). Cystatin-C is superior to creatinine
in estimating glomerular filtration rate (49) and is widely considered to be a
predictive biomarker in kidney and cardiovascular diseases
(50,51). Additionally, serum cystatin-C has
been confirmed as a more sensitive biomarker than serum creatinine
in predicting renal dysfunction in patients with primary NS
(49,52). This also supports the previous claim
that cystatin-C was a biomarker of NS and could predict the disease
progress (49,52,53). The
current study identified that CL/F was negatively associated with
cystatin-C, which indicated the progression of disease had an
impact on CL/F in a pediatric refractory nephrotic syndrome
model.
In addition to age and CYSC, another key factor
affecting TAC clearance was TAMT. It is established that TAC is
primarily metabolized by the oxidative enzyme cytochrome P450 (CYP)
3A subfamily in the intestine and liver, with CYP3A4 and the highly
polymorphic CYP3A5 as the major metabolizing enzymes (54). A previous study reported that
individuals with the CYP3A5*3/*3 genotype require less TAC
to attain objective concentrations compared with patients with the
CYP3A5*1 allele (55–57). Additionally, genetically-induced
CYP3A5 hyperactivity increases the TAC daily dose (58). Therefore, the effect of TAMT on CL/F
may be primarily derived from CYP3A5 gene polymorphisms.
Unfortunately, at present, CYP3A5 genotyping is not
routinely performed in Chinese patients with PRNS. Whether
CYP3A5 genotype could better assess the inter-individual
variability in the current model of CL/F on TAC in PRNS should be
determined in the future.
In addition, the current study provided a summary of
previous literature concerning TAC PPK models in several pediatric
diseases. Notably, TAC PPK models vary in different pediatric
diseases. To a certain extent, this may indicate that disease
situation may lead to differences in CL/F and V/F in different
populations.
In conclusion, the first TAC PPK model in patients
with PRNS was established using retrospective, routinely monitored
data. Age, CYSC and TAMT were identified as significant covariates
for CL/F. No covariates significantly influenced V/F. The current
study also provided a summary of previous literature concerning TAC
PPK models in different pediatric diseases.
Acknowledgements
Not applicable.
Funding
This study was supported by the Clinical Pharmacy
Key Specialty Construction Project of Shanghai (grant no.
YZ2017/5).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZL conceived and designed the study. DW, JL and QL
collected data and built the model. DW wrote the paper. JL and QL
reviewed and edited the manuscript. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Research Ethics
Committee of Children's Hospital of Fudan University (Shanghai,
China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Certikova-Chabova V and Tesar V: Recent
insights into the pathogenesis of nephrotic syndrome. Minerva Med.
104:333–347. 2013.PubMed/NCBI
|
|
2
|
2. Eddy AA and Symons JM: Nephrotic
syndrome in childhood. Lancet. 362:629–639. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
McKinney PA, Feltbower RG, Brocklebank JT
and Fitzpatrick MM: Time trends and ethnic patterns of childhood
nephrotic syndrome in Yorkshire, UK. Pediatr Nephrol. 16:1040–1044.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Koskimies O, Vilska J, Rapola J and
Hallman N: Long-term outcome of primary nephrotic syndrome. Arch
Dis Child. 57:544–548. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lombel RM, Gipson DS and Hodson EM; Kidney
Disease, : Improving Global Outcomes: Treatment of
steroid-sensitive nephrotic syndrome: New guidelines from KDIGO.
Pediatr Nephrol. 28:415–426. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tarshish P, Tobin JN, Bernstein J and
Edelmann CM Jr: Prognostic significance of the early course of
minimal change nephrotic syndrome: Report of the International
Study of Kidney Disease in Children. J Am Soc Nephrol. 8:769–776.
1997.PubMed/NCBI
|
|
7
|
Hodson EM, Willis NS and Craig JC:
Corticosteroid therapy for nephrotic syndrome in children. Cochrane
Database Syst Rev (4). CD0015332007.
|
|
8
|
Choudhry S, Bagga A, Hari P, Sharma S,
Kalaivani M and Dinda A: Efficacy and safety of tacrolimus versus
cyclosporine in children with steroid-resistant nephrotic syndrome:
A randomized controlled trial. Am J Kidney Dis. 53:760–769. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gulati A, Sinha A, Gupta A, Kanitkar M,
Sreenivas V, Sharma J, Mantan M, Agarwal I, Dinda AK, Hari P, et
al: Treatment with tacrolimus and prednisolone is preferable to
intravenous cyclophosphamide as the initial therapy for children
with steroid-resistant nephrotic syndrome. Kidney Int.
82:1130–1135. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gulati S, Prasad N, Sharma RK, Kumar A,
Gupta A and Baburaj VP: Tacrolimus: A new therapy for
steroid-resistant nephrotic syndrome in children. Nephrol Dial
Transplant. 23:910–913. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Loeffler K, Gowrishankar M and Yiu V:
Tacrolimus therapy in pediatric patients with treatment-resistant
nephrotic syndrome. Pediatr Nephrol. 19:281–287. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Roberti I and Vyas S: Long-term outcome of
children with steroid-resistant nephrotic syndrome treated with
tacrolimus. Pediatr Nephrol. 25:1117–1124. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sinha A, Gupta A, Kalaivani M, Hari P,
Dinda AK and Bagga A: Mycophenolate mofetil is inferior to
tacrolimus in sustaining remission in children with idiopathic
steroid-resistant nephrotic syndrome. Kidney Int. 92:248–257. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang W, Xia Y, Mao J, Chen Y, Wang D, Shen
H, Fu H, Du L and Liu A: Treatment of tacrolimus or cyclosporine A
in children with idiopathic nephrotic syndrome. Pediatr Nephrol.
27:2073–2079. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yang EM, Lee ST, Choi HJ, Cho HY, Lee JH,
Kang HG, Park YS, Cheong HI and Ha IS: Tacrolimus for children with
refractory nephrotic syndrome: A one-year prospective, multicenter,
and open-label study of Tacrobell®, a generic formula.
World J Pediatr. 12:60–65. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Venkataramanan R, Swaminathan A, Prasad T,
Jain A, Zuckerman S, Warty V, McMichael J, Lever J, Burckart G and
Starzl T: Clinical pharmacokinetics of tacrolimus. Clin
Pharmacokinet. 29:404–430. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jusko WJ, Thomson AW, Fung J, McMaster P,
Wong SH, Zylber-Katz E, Christians U, Winkler M, Fitzsimmons WE,
Lieberman R, et al: Consensus document: Therapeutic monitoring of
tacrolimus (FK-506). Ther Drug Monit. 17:606–614. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vadcharavivad S, Praisuwan S,
Techawathanawanna N, Treyaprasert W and Avihingsanon Y: Population
pharmacokinetics of tacrolimus in Thai kidney transplant patients:
Comparison with similar data from other populations. J Clin Pharm
Ther. 41:310–328. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Andreu F, Colom H, Grinyó JM, Torras J,
Cruzado JM and Lloberas N: Development of a population PK model of
tacrolimus for adaptive dosage control in stable kidney transplant
patients. Ther Drug Monit. 37:246–255. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Benkali K, Rostaing L, Premaud A, Woillard
JB, Saint-Marcoux F, Urien S, Kamar N, Marquet P and Rousseau A:
Population pharmacokinetics and Bayesian estimation of tacrolimus
exposure in renal transplant recipients on a new once-daily
formulation. Clin Pharmacokinet. 49:683–692. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bergmann TK, Hennig S, Barraclough KA,
Isbel NM and Staatz CE: Population pharmacokinetics of tacrolimus
in adult kidney transplant patients: Impact of CYP3A5 genotype on
starting dose. Ther Drug Monit. 36:62–70. 2014.PubMed/NCBI
|
|
22
|
Han N, Ha S, Yun HY, Kim MG, Min SI, Ha J,
Lee JI, Oh JM and Kim IW: Population
pharmacokinetic-pharmacogenetic model of tacrolimus in the early
period after kidney transplantation. Basic Clin Pharmacol Toxicol.
114:400–406. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhao W, Elie V, Roussey G, Brochard K,
Niaudet P, Leroy V, Loirat C, Cochat P, Cloarec S, André JL, et al:
Population pharmacokinetics and pharmacogenetics of tacrolimus in
de novo pediatric kidney transplant recipients. Clin Pharmacol
Ther. 86:609–618. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zuo XC, Ng CM, Barrett JS, Luo AJ, Zhang
BK, Deng CH, Xi LY, Cheng K, Ming YZ, Yang GP, et al: Effects of
CYP3A4 and CYP3A5 polymorphisms on tacrolimus pharmacokinetics in
Chinese adult renal transplant recipients: A population
pharmacokinetic analysis. Pharmacogenet Genomics. 23:251–261. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lu YX, Su QH, Wu KH, Ren YP, Li L, Zhou TY
and Lu W: A population pharmacokinetic study of tacrolimus in
healthy Chinese volunteers and liver transplant patients. Acta
Pharmacol Sin. 36:281–288. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Musuamba FT, Guy-Viterbo V, Reding R,
Verbeeck RK and Wallemacq P: Population pharmacokinetic analysis of
tacrolimus early after pediatric liver transplantation. Ther Drug
Monit. 36:54–61. 2014.PubMed/NCBI
|
|
27
|
Wallin JE, Bergstrand M, Wilczek HE,
Nydert PS, Karlsson MO and Staatz CE: Population pharmacokinetics
of tacrolimus in pediatric liver transplantation: Early
posttransplantation clearance. Ther Drug Monit. 33:663–672. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yang JW, Liao SS, Zhu LQ, Zhao Y, Zhang Y,
Sun XY, Rao W, Qu W, Li WZ and Sun LY: Population pharmacokinetic
analysis of tacrolimus early after Chinese pediatric liver
transplantation. Int J Clin Pharmacol Ther. 53:75–83. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zhang XQ, Wang ZW, Fan JW, Li YP, Jiao Z,
Gao JW, Peng ZH and Liu GL: The impact of sulfonylureas on
tacrolimus apparent clearance revealed by a population
pharmacokinetics analysis in Chinese adult liver-transplant
patients. Ther Drug Monit. 34:126–133. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhu L, Yang J, Zhang Y, Jing Y, Zhang Y
and Li G: Effects of CYP3A5 genotypes, ABCB1 C3435T and G2677T/A
polymorphism on pharmacokinetics of Tacrolimus in Chinese adult
liver transplant patients. Xenobiotica. 45:840–846. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wallin JE, Friberg LE, Fasth A and Staatz
CE: Population pharmacokinetics of tacrolimus in pediatric
hematopoietic stem cell transplant recipients: New initial dosage
suggestions and a model-based dosage adjustment tool. Ther Drug
Monit. 31:457–466. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Monchaud C, de Winter BC, Knoop C, Estenne
M, Reynaud-Gaubert M, Pison C, Stern M, Kessler R, Guillemain R,
Marquet P, et al: Population pharmacokinetic modelling and design
of a Bayesian estimator for therapeutic drug monitoring of
tacrolimus in lung transplantation. Clin Pharmacokinet. 51:175–186.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Fukudo M, Yano I, Masuda S, Goto M, Uesugi
M, Katsura T, Ogura Y, Oike F, Takada Y and Egawa H: Population
pharmacokinetic and pharmacogenomic analysis of tacrolimus in
pediatric living-donor liver transplant recipients. Clin Pharmacol
Ther. 80:331–345. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
García Sánchez MJ, Manzanares C,
Santos-Buelga D, Blázquez A, Manzanares J, Urruzuno P and Medina E:
Covariate effects on the apparent clearance of tacrolimus in
paediatric liver transplant patients undergoing conversion therapy.
Clin Pharmacokinet. 40:63–71. 2001. View Article : Google Scholar
|
|
35
|
Guy-Viterbo V, Scohy A, Verbeeck RK,
Reding R, Wallemacq P and Musuamba FT: Population pharmacokinetic
analysis of tacrolimus in the first year after pediatric liver
transplantation. Eur J Clin Pharmacol. 69:1533–1542. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Jalil MH, Hawwa AF, McKiernan PJ, Shields
MD and McElnay JC: Population pharmacokinetic and pharmacogenetic
analysis of tacrolimus in paediatric liver transplant patients. Br
J Clin Pharmacol. 77:130–140. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kassir N, Labbé L, Delaloye JR, Mouksassi
MS, Lapeyraque AL, Alvarez F, Lallier M, Beaunoyer M, Théorêt Y and
Litalien C: Population pharmacokinetics and Bayesian estimation of
tacrolimus exposure in paediatric liver transplant recipients. Br J
Clin Pharmacol. 77:1051–1063. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Sam WJ, Aw M, Quak SH, Lim SM, Charles BG,
Chan SY and Ho PC: Population pharmacokinetics of tacrolimus in
Asian paediatric liver transplant patients. Br J Clin Pharmacol.
50:531–541. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Yasuhara M, Hashida T, Toraguchi M,
Hashimoto Y, Kimura M, Inui K, Hori R, Inomata Y, Tanaka K and
Yamaoka Y: Pharmacokinetics and pharmacodynamics of FK 506 in
pediatric patients receiving living-related donor liver
transplantations. Transplant Proc. 27:1108–1110. 1995.PubMed/NCBI
|
|
40
|
Jusko WJ, Piekoszewski W, Klintmalm GB,
Shaefer MS, Hebert MF, Piergies AA, Lee CC, Schechter P and Mekki
QA: Pharmacokinetics of tacrolimus in liver transplant patients.
Clin Pharmacol Ther. 57:281–290. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Lindbom L, Pihlgren P and Jonsson EN:
PsN-Toolkit - a collection of computer intensive statistical
methods for non-linear mixed effect modeling using NONMEM. Comput
Methods Programs Biomed. 79:241–257. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Wang DD, Lu JM, Li Q and Li ZP: Population
pharmacokinetics of tacrolimus in paediatric systemic lupus
erythematosus based on real-world study. J Clin Pharm Ther.
43:476–483. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Lindbom L, Ribbing J and Jonsson EN:
Perl-speaks-NONMEM (PsN) - a Perl module for NONMEM related
programming. Comput Methods Programs Biomed. 75:85–94. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Brendel K, Dartois C, Comets E,
Lemenuel-Diot A, Laveille C, Tranchand B, Girard P, Laffont CM and
Mentré F: Are population pharmacokinetic and/or pharmacodynamic
models adequately evaluated? A survey of the literature from 2002
to 2004. Clin Pharmacokinet. 46:221–234. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Jolling K, Perez Ruixo JJ, Hemeryck A,
Vermeulen A and Greway T: Mixed-effects modelling of the
interspecies pharmacokinetic scaling of pegylated human
erythropoietin. Eur J Pharm Sci. 24:465–475. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kauffman RE and Kearns GL: Pharmacokinetic
studies in paediatric patients. Clinical and ethical
considerations. Clin Pharmacokinet. 23:10–29. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Przepiorka D, Blamble D, Hilsenbeck S,
Danielson M, Krance R and Chan KW: Tacrolimus clearance is
age-dependent within the pediatric population. Bone Marrow
Transplant. 26:601–605. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Hojs R, Bevc S, Ekart R, Gorenjak M and
Puklavec L: Serum cystatin C as an endogenous marker of renal
function in patients with mild to moderate impairment of kidney
function. Nephrol Dial Transplant. 21:1855–1862. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Dharnidharka VR, Kwon C and Stevens G:
Serum cystatin C is superior to serum creatinine as a marker of
kidney function: A meta-analysis. Am J Kidney Dis. 40:221–226.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Koenig W, Twardella D, Brenner H and
Rothenbacher D: Plasma concentrations of cystatin C in patients
with coronary heart disease and risk for secondary cardiovascular
events: More than simply a marker of glomerular filtration rate.
Clin Chem. 51:321–327. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Villa P, Jiménez M, Soriano MC and
Manzanares JP: Serum cystatin C concentration as a marker of acute
renal dysfunction in critically ill patients. Crit Care.
9:R139–R143. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
52
|
Zaffanello M, Franchini M and Fanos V: Is
serum Cystatin-C a suitable marker of renal function in children?
Ann Clin Lab Sci. 37:233–240. 2007.PubMed/NCBI
|
|
53
|
Cordeiro VF, Pinheiro DC, Silva GB Jr,
Lima JW, Mota RM, Libório AB and Daher EF: Comparative study of
cystatin C and serum creatinine in the estimative of glomerular
filtration rate in children. Clin Chim Acta. 391:46–50. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Kurzawski M and Droździk M:
Pharmacogenetics in solid organ transplantation: Genes involved in
mechanism of action and pharmacokinetics of immunosuppressive
drugs. Pharmacogenomics. 14:1099–1118. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Haufroid V, Mourad M, Van Kerckhove V,
Wawrzyniak J, De Meyer M, Eddour DC, Malaise J, Lison D, Squifflet
JP and Wallemacq P: The effect of CYP3A5 and MDR1 (ABCB1)
polymorphisms on cyclosporine and tacrolimus dose requirements and
trough blood levels in stable renal transplant patients.
Pharmacogenetics. 14:147–154. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Hesselink DA, van Schaik RH, van der
Heiden IP, van der Werf M, Gregoor PJ, Lindemans J, Weimar W and
van Gelder T: Genetic polymorphisms of the CYP3A4, CYP3A5, and
MDR-1 genes and pharmacokinetics of the calcineurin inhibitors
cyclosporine and tacrolimus. Clin Pharmacol Ther. 74:245–254. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Kuypers DR, de Jonge H, Naesens M and
Vanrenterghem Y: A prospective, open-label, observational clinical
cohort study of the association between delayed renal allograft
function, tacrolimus exposure, and CYP3A5 genotype in adult
recipients. Clin Ther. 32:2012–2023. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Quteineh L, Verstuyft C, Furlan V,
Durrbach A, Letierce A, Ferlicot S, Taburet AM, Charpentier B and
Becquemont L: Influence of CYP3A5 genetic polymorphism on
tacrolimus daily dose requirements and acute rejection in renal
graft recipients. Basic Clin Pharmacol Toxicol. 103:546–552. 2008.
View Article : Google Scholar : PubMed/NCBI
|