Introduction
Critically ill patients typically have high blood
glucose levels, which is a stress indicator for patients with no
history of diabetes (1–6). High blood glucose levels need to be
controlled (2,7–13).
Various studies have demonstrated that tight glycemic control (TGC)
can reduce the risk of mortality and complications, as well as have
other benefits. Tran et al (14) and Pham et al (15) reported that TGC is necessary in
children with severe burns. A prospective randomized trial revealed
that it can reduce the risk of mortality in patients with sepsis
(5). Vlasselaers et al
(16) indicated that intraoperative
TGC can protect the myocardium and reduce infection in neonatal
patients with severe heart disease. Furthermore, Day et al
(17) revealed that TGC benefits
critically ill pediatric patients with meningococcal sepsis. In
addition, a study conducted at Leuven University in Belgium
indicated that intensive insulin therapy (i.e., TGC) can reduce
mortality in critically ill adult and pediatric patients (9,18).
However, the optimal blood glucose control target for critically
ill children remains uncertain, and some researchers have
questioned proposed glucose control targets and, more generally,
the benefit of TGC (19–21). In the present study, the
characteristics of pediatric patients at first admission were
examined, and the effects of blood glucose control [TGC,
conventional insulin therapy (CIT) and no insulin] were analyzed
using data from critically ill children. The length of stay in the
pediatric intensive care unit (PICU), total length of
hospitalization, mortality, occurrence of secondary coma,
development of secondary hepatic or renal dysfunction, incidence of
hypoglycemia and blood glucose reduction were compared among
groups. Furthermore, correlations between blood glucose levels and
mortality, secondary coma, and secondary hepatic and renal
dysfunction following insulin therapy were examined. Blood glucose
levels were observed at the time of PICU admission and 24, 48, 72
and 96 h thereafter in the TGC, CIT and control groups. Overall,
the benefits of blood glucose control and non-use of insulin
therapy were evaluated and the spontaneous resolution of the blood
glucose level without insulin therapy was assessed. The study
findings suggested that the blood glucose level could return to
normal spontaneously, without insulin therapy and with no
associated risk, in critically ill pediatric patients with stress
hyperglycemia.
Materials and methods
Ethics and written informed
consent
The Ethics Committee of the Shunde Women's and
Children's Healthcare Hospital (Foshan, China) approved the present
study. Prior to the start of the research, written informed consent
was obtained from next of kin, carers and/or guardians on behalf of
the children enrolled in the study.
Study population
All subjects included in the present study were
admitted to the Shunde Women's and Children's Healthcare Hospital
and Yuexiu District Children's Hospital of Guangzhou between June
2009 and June 2017. Clinical data was collected from 302 critically
ill infants with hyperglycemia who were admitted to the hospitals'
PICUs. The following data were extracted from patient medical
records: Patient age (range, 1–12 months), sex (male, n=156; femal,
n=146), diagnosis (22), history of
diabetes, steroid use, nutrition delivery, SOFA-associated
indicators, length of PICU stay, total length of hospitalization,
mortality, occurrence of secondary coma, development of secondary
hepatic and renal dysfunction, incidence of ketoacidosis, blood
glucose level at PICU admission and change in blood glucose level
(at 24, 48, 72 and 96 h), blood ketone level, urine ketone response
and blood pH values at first admission and at 24, 48, 72 and 96 h,
Eligible subjects met the following criteria: i) Critically ill
infants (aged, 1 to 12 months) with stress hyperglycemia; ii)
patients examined had with no past history of diabetes (considering
both parents); and iii) patients examined had recorded steroid use
prior to recruitment.
Patient evaluation
Sepsis and septic shock were evaluated using the
Sequential (Sepsis-Related) Organ Failure Assessment (SOFA) and
defined according to the Third International Consensus Definitions
for Sepsis and Septic Shock (Sepsis-3) (23). Stress hyperglycemia was defined
according to the American Diabetes Association's Diabetes in
Hospitals Writing Committee Guidelines (fasting blood glucose ≥7.0
mmol/l or random blood glucose ≥11.1 mmol/l) (22). Severe hyperglycemia was defined as a
blood glucose level ≥25.00 mmol/l at first admission (22). Secondary coma, secondary hepatic
dysfunction and secondary renal dysfunction in patients with sepsis
were defined according to the Sepsis-3 (23). Secondary coma was defined as a
Glasgow score <8 following hospitalization; secondary hepatic
dysfunction was defined as a total bilirubin level >4 mg/dl (72
mmol/l) or alanine aminotransferase level of at least two times the
upper limit of the normal level for the patient's age; and
secondary renal dysfunction was defined as a serum creatinine level
of at least two times the upper limit of the normal level for the
patient's age or a 2-fold increase in the baseline creatinine level
during the PICU stay. Hypoglycemia was defined as a blood glucose
level <2.8 mmol/l, and severe hypoglycemia was defined as a
level ≤2.2 mmol/l (24).
Ketoacidosis was defined according to the International Society for
Pediatric and Adolescent Diabetes biochemical criteria as a blood
glucose level >11 mmol/l and venous pH <7.3 following
hospitalization, and presence of ketonemia and ketonuria (25,26).
Grouping method
The patients were into three groups: TGC (n=85), CIT
(n=89) and control (no insulin use; n=128) groups. Blood glucose
control points were as follows: <6.1 to 4.4 mmol/l for the TGC
group and 10.0 mmol/l or less per liter (4,9) for the
CIT group. Insulin administration was stopped in the two groups
when the target range was reached. Patients who did not receive
insulin therapy were assigned to the control group.
Insulin therapy and nutritional
support treatment
Continuous short-acting insulin infusion was
delivered with a micropump. The insulin dose was 0.5–1 IU/kg·day,
and was adjusted according to the blood glucose level. Blood
glucose levels were measured with a bedside glucose meter (Free
Style Optium Neo; model XEMV168-026F; Abbott Diabetes Care Ltd.,
Chicago, IL, USA) every 30 min following insulin adjustment.
Enteral nutrition was initiated as early as possible for all
patients. Nutrition standards were established according to
nutritional support treatment guidelines (27), with total calories set to 20–30
kcal·kg−1·24 h−1 (nitrogen, 0.08–0.25
g·kg−1·24 h−1; 20–40% fat emulsion).
Statistical analyses
Statistical analyses were performed with SPSS
statistical software (version 17.0; SPSS, Inc., Chicago, IL, USA).
Figures were generated using GraphPad software (La Jolla, CA, USA;
version 5.01). P<0.05 was considered to indicate a statistically
significant difference. Kolmogorov-Smirnov testing was used to
investigate the distribution of blood glucose levels in the TGC,
CIT and control groups. The results indicated that these
distributions were normal (Z=0.935, P=0.080; Z=0.912, P=0.088; and
Z=0.917, P=0.091, respectively). The χ2 test was used
for intergroup comparison of count data (sex, mortality, secondary
coma, secondary hepatic dysfunction, secondary renal dysfunction
and incidence of hypoglycemia). Age, SOFA score, length of PICU
stay, total length of hospitalization, and blood glucose levels at
PICU admission and thereafter were presented as the mean ± standard
deviation. Results were compared between multiple groups using
one-way ANOVA, while a Neuman-keuls test was applied to compare
differences among these groups. Pearson's test was applied to
examine correlations between blood glucose levels following insulin
therapy and mortality, secondary coma, and secondary hepatic and
renal dysfunction in all patients.
Results
A total of 302 patients (156 male patients and 146
female patients), with a mean age at enrollment of 7 months (range,
1 to 12 months), were assessed in the present study. Patients had
the following diseases: Sepsis (n=67), septic shock (n=23), severe
pneumonia (n=120), meningoencephalitis (n=28), acute lung
hemorrhage (n=18), acute laryngeal obstruction (n=11), persistent
asthma (n=10), acute myocarditis (n=11), acute nephritis (n=8) and
necrotic enteritis (n=6). Among critically ill patients with stress
hyperglycemia in the TGC (n=85), CIT (n=89) and control (n=128)
groups, these venous blood glucose levels did not differ
significantly between male (n=156) and female patients (n=146;
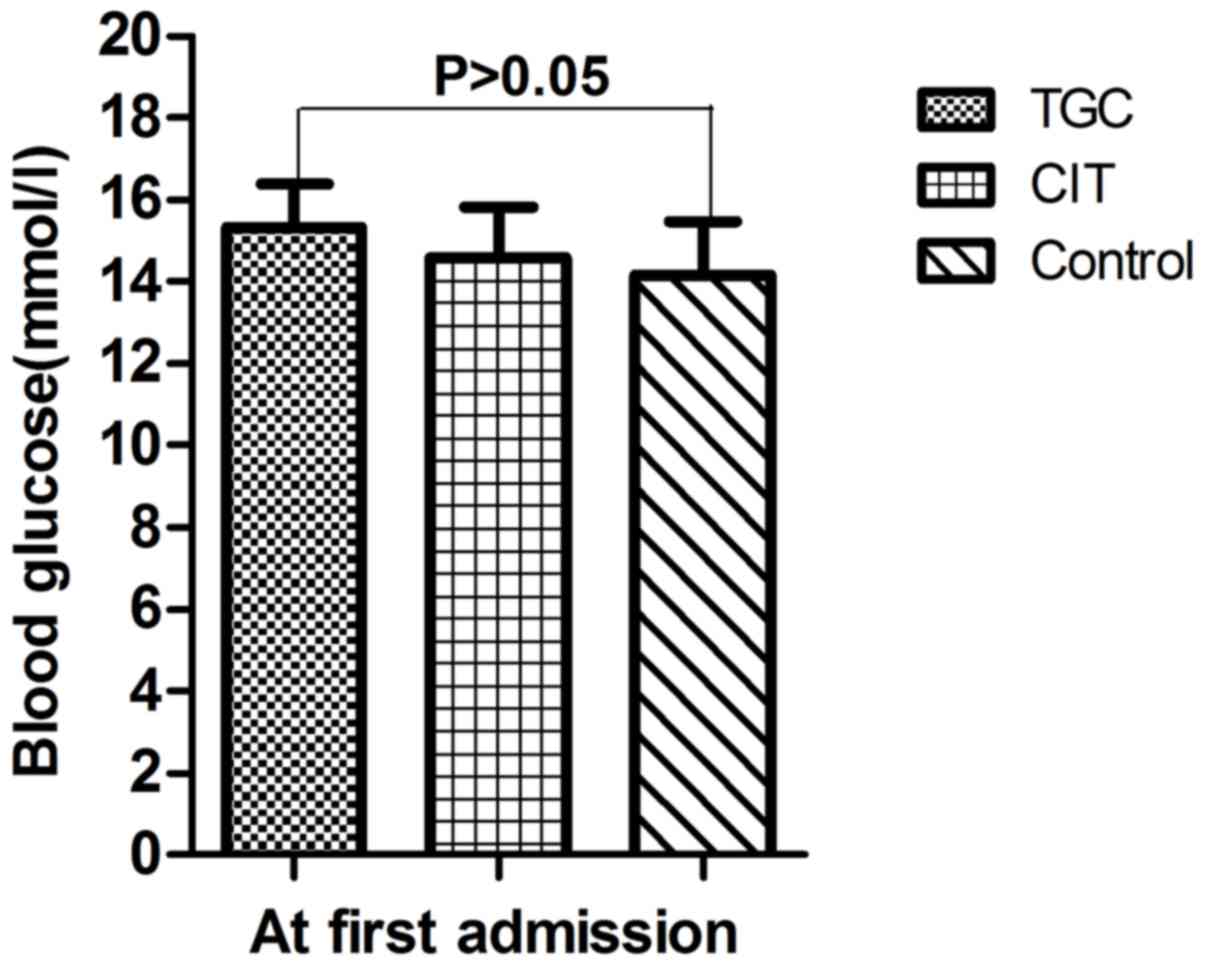
14.7±1.9 and 14.6±1.8 mmol/l respectively; P>0.05; Table I). No patient had severe stress
hyperglycemia (blood glucose level >25.00 mmol/l). There was not
significant difference in mean venous blood glucose levels at first
admission (15.2±3.8, 14.6±4.5 and 14.2±4.7 mmol/l, respectively;
P>0.05; Table II, Fig. 1). Certain characteristics of
pediatric patients at first administration did not differ among
groups (Table II), including age,
male sex, blood glucose, arterial oxygen saturation, PaO2/FI O2,
systolic blood pressure and MAP.
 | Table I.Blood glucose levels at first
admission according to pathology and sex. |
Table I.
Blood glucose levels at first
admission according to pathology and sex.
|
| Total | Male | Female |
|---|
|
|
|
|
|
|---|
| Factor | n | Blood glucose
(mmol/l) | n | Blood glucose
(mmol/l) | n | Blood glucose
(mmol/l) |
|---|
| Disease |
|
|
|
|
|
|
|
Sepsis | 67 | 15.0±1.6 | 35 | 15.1±1.1 | 32 | 14.8±2.1 |
| Septic
shock | 23 | 16.7±2.0 | 12 | 16.8±2.0 | 11 | 16.5±1.9 |
| Severe
pneumonia | 120 | 14.7±1.5 | 62 | 14.6±1.2 | 58 | 14.8±1.7 |
|
Meningoencephalitis | 28 | 14.1±1.8 | 13 | 14.1±1.5 | 15 | 14.0±2.1 |
| Acute
lung hemorrhage | 18 | 15.0±1.4 | 10 | 15.1±1.1 | 8 | 14.8±1.7 |
| Acute
laryngeal obstruction | 11 | 14.5±1.5 | 6 | 14.8±1.3 | 5 | 14.1±1.7 |
|
Persistent asthma | 10 | 13.1±1.6 | 6 | 13.0±1.5 | 4 | 13.1±1.7 |
| Acute
myocarditis | 11 | 13.4±1.9 | 5 | 12.7±2.3 | 6 | 14.0±1.5 |
| Acute
nephritis | 8 | 12.6±1.5 | 4 | 12.5±1.4 | 4 | 12.7±1.6 |
|
Necrotic enteritis | 6 | 13.6±1.6 | 3 | 13.1±2.1 | 3 | 14.0±1.1 |
| Disease total | 302 |
| 156 | 14.7±1.9 | 146 | 14.6±1.8 |
| Table II.Characteristics of patients at first
admission. |
Table II.
Characteristics of patients at first
admission.
| Variable | TGC group | CIT group | Control group | P-value |
|---|
| Number of
subjects | 85 | 89 | 128 | – |
| Age (months) |
7±4.9 |
7±4.5 |
7±4.6 | 0.22 |
| Male (%) | 51.66 | 52.54 | 51.44 | 0.71 |
| Blood glucose,
mmol/l | 15.2±3.8 | 14.6±4.5 | 14.2±4.7 | 0.66a, 0.69b and 0.67c |
| Arterial oxygen
saturation, % | 81±11.5 | 80±21.4 | 82±20.1 | 0.29 |
| PaO2/FI
O2, kPa | 28.7±15.7 | 30.5±14.3 | 29.6±12.7 | 0.30 |
| Systolic blood
pressure, mmHg | 71±15.2 | 70±86.4 | 73±35.6 | 0.19 |
| MAP, mm Hg | 51±18.2 | 53±11.5 | 51±17.7 | 0.32 |
| pH value | 7.2±0.2 | 7.2±0.5 | 7.2±0.4 | 0.59 |
| Hemoglobin,
g/l | 87±17 | 89±35 | 89±24 | 0.26 |
| Platelet,
10×109/l | 9.1±0.7 | 9.0±0.3 | 9.0±0.6 | 0.32 |
| Total bilirubin,
µmol/l | 19±8.7 | 18±9.4 | 19±11.8 | 0.25 |
| ALT, U/l | 39±19 | 37±15 | 37± 2 | 0.27 |
| Creatinine,
mg/dl | 1.1±0.8 | 1.0±0.7 | 1.0±0.5 | 0.30 |
| C-reactive protein,
mg/l | 49±22.7 | 47±19.0 | 47±27.4 | 0.26 |
| Procalcitonin,
mg/l | 3±1.1 | 3±1.4 | 3±1.3 | 0.49 |
| Blood lactic acid,
mmol/l | 3±0.9 | 3±1.1 | 3±1.2 | 0.53 |
| Urine volume,
ml/kg·h· | 0.6±0.3 | 0.6±0.1 | 0.6±0.3 | 0.97 |
| GCS, score | 10±2.2 | 10±2.7 | 10±2.6 | 0.54 |
| SOFA, score | 8.67±3.14 | 8.79±2.55 | 8.80±2.61 | 0.28 |
Length of PICU stay and total length of
hospitalization were shorter in the TGC group when compared with
the CIT and control groups; however this difference was not
significant (P>0.05). Mortality and the occurrence of secondary
coma, secondary hepatic dysfunction and secondary renal dysfunction
did not significantly differ among groups (P>0.05). At 24, 48
and 72 h, blood glucose levels in TGC, CIT and control groups
differed significantly [7.4±2.5, 11.2±3.8 and 14.5±4.1 mmol/l
(P<0.01); 4.8±2.6, 7.9±2.5 and 9.5±3.5 mmol/l (P<0.01); and
4.7±1.5, 6.3±1.1 and 6.8±1.7 mmol/l (P<0.05), respectively]. No
significant difference between groups was noted at 96 h (5.0±1.2,
4.9±1.3, and 5.1±0.9 mmol/l, respectively; P>0.05; Fig. 2).
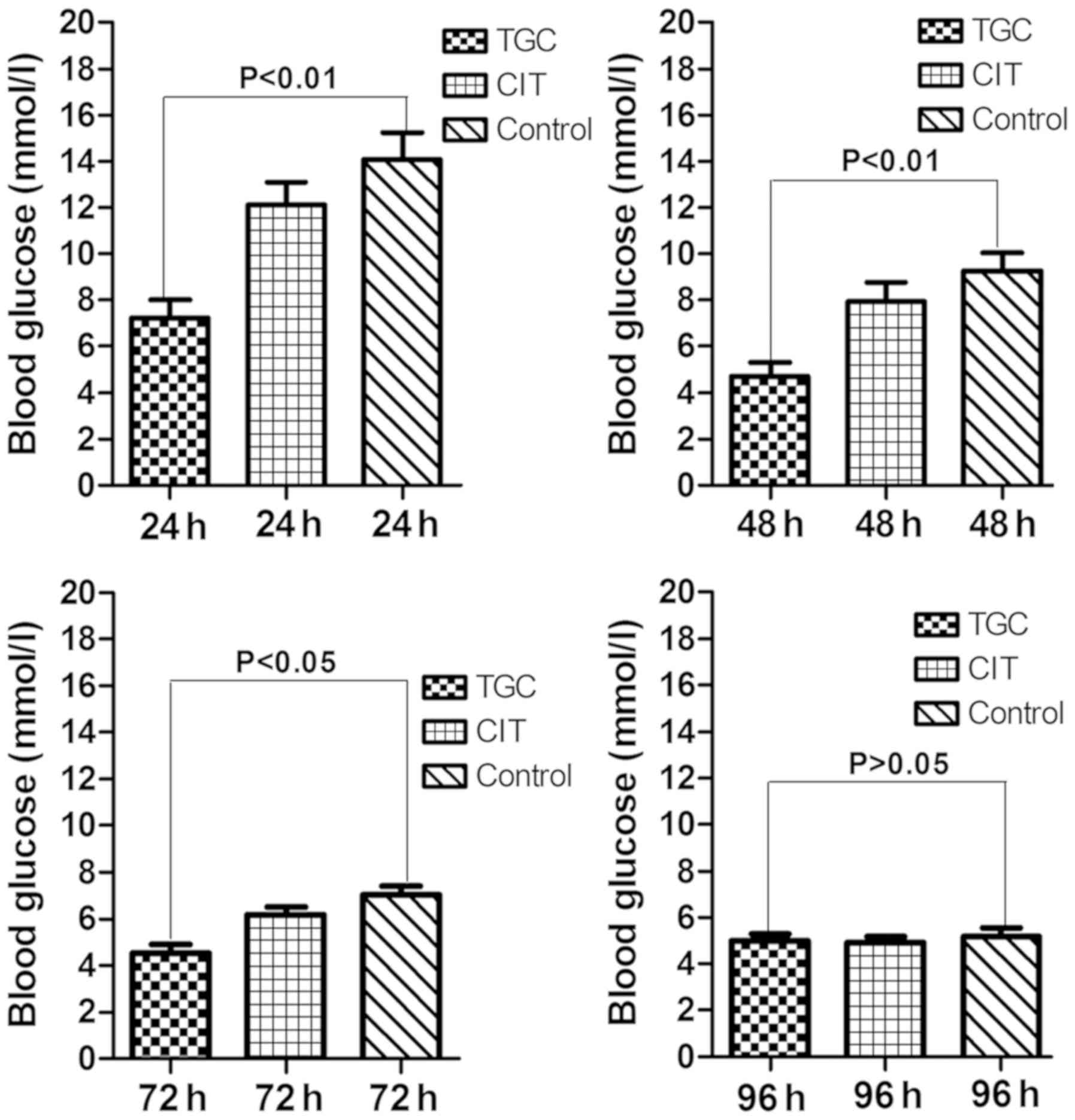 | Figure 2.At 24 and 48 h following admission,
blood glucose levels in the TGC, CIT and control groups were
7.4±2.5, 11.2±3.8, and 14.5±4.1 mmol/l (P=0.007, P<0.01) and
4.8±2.6, 7.9±2.5 and 9.5±3.5 mmol/l (P=0.008, P<0.01),
respectively; these levels at 72 and 96 h were 4.7±1.5, 6.3±1.1 and
6.8±1.7 mmol/l (P=0.039, P<0.05) and 5.0±1.2, 4.9±1.3 and
5.1±0.9 mmol/l (P>0.05), respectively. TGC, tight glycemic
control; CIT, conventional insulin therapy. |
Notably, 5 patients in the TGC group exhibited
hypoglycemia [blood glucose range, 2.6–2.10 mmol/l: 2.3, 2.6 and
2.7 mmol/l in 3 (3.53%) patients; and severe hypoglycemia (2.10 and
2.15 mmol/l) in 2 (2.35%) patients] following 26, 29, 38, 43 and 47
h of insulin therapy, respectively. The incidence of hypoglycemia
was 5.88%. No patient in the CIT or control group exhibited
hypoglycemia. Comparison of the incidence of hypoglycemia between
multiple groups was significantly different (χ2=15.62
P<0.01; Table III). During the
entire administration period, blood glucose levels were not
correlated with mortality, secondary coma, hepatic dysfunction or
renal dysfunction (Table IV).
| Table III.Comparison of data from the TGC, CIT
and control groups. |
Table III.
Comparison of data from the TGC, CIT
and control groups.
| Variable | N | PICU length of stay
(day) | Total length of
stay (day) | Mortality n
(%) | Secondary coma n
(%) | Secondary hepatic
dysfunction n (%) | Secondary renal
dysfunction n (%) | Hypoglycemia n
(%) |
|---|
| Groups |
|
|
|
|
|
|
|
|
|
TGC | 85 | 5±2.4 | 11±8.6 | 10 (11.76) | 5 (5.38) | 7 (7.53) | 6 (7.06) | 5 (5.88) |
|
CIT | 89 | 5±8.9 | 11±1.2 | 11 (12.36) | 5 (5.62) | 8 (7.84) | 8 (7.84) | 0 (0.00) |
|
Control | 128 | 6±1.8 | 12±1.7 | 15 (11.72) | 7 (5.47) | 11 (8.59) | 9 (7.03) | 0 (0.00) |
| χ2 |
| 1.16 | 1.27 | 1.25 | 0.83 | 0.97 | 1.04 | 15.62 |
| P-value |
|
>0.05 |
>0.05 |
>0.05 |
>0.05 |
>0.05 |
>0.05 |
<0.01 |
|
|
| P>0.05 | P>0.05 | P>0.05 | P>0.05 | P>0.05 | P>0.05 | a,bP<0.01 |
|
|
|
|
|
|
|
|
| cP>0.05 |
| Table IV.Correlations of blood glucose levels
with correlative factors during the entire administration period in
the TGC, CIT and control groups. |
Table IV.
Correlations of blood glucose levels
with correlative factors during the entire administration period in
the TGC, CIT and control groups.
|
| Pearson's test | F test |
|
|---|
|
|
|
|
|
|---|
| Correlative
factor | r | P-value | F | P-value | R2 |
|---|
| Mortality | 0.171 | 0.12 | 19.315 | 0.11 | 0.154 |
| Coma | 0.150 | 0.09 | 17.713 | 0.10 | 0.148 |
| Hepatic
dysfunction | 0.166 | 0.10 | 18.431 | 0.11 | 0.148 |
| Renal
dysfunction | 0.156 | 0.11 | 19.376 | 0.12 | 0.154 |
Ketone was not detected upon exhaled breath in
patients, and blood ketosis and urine ketone response results were
negative. At first admission and at 24, 48, 72 and 96 h, pH values
in the TGC, CIT and control groups did not differ significantly
(P>0.05; Table V).
| Table V.pH values in the TGC, CIT and control
groups. |
Table V.
pH values in the TGC, CIT and control
groups.
|
| pH values |
|---|
|
|
|
|---|
| Groups | At first | 24 h | 48 h | 72 h | 96 h |
|---|
| Group |
|
|
|
|
|
|
TGC | 7.2±0.2 | 7.3±0.1 | 7.3±0.2 | 7.4±0.2 | 7.4±0.2 |
|
CIT | 7.2±0.5 | 7.3±0.1 | 7.3±0.2 | 7.4±0.2 | 7.4±0.2 |
|
Control | 7.2±0.4 | 7.3±0.2 | 7.3±0.1 | 7.4±0.1 | 7.4±0.1 |
| F | 0.29 | 0.32 | 0.29 | 0.29 | 0.29 |
| P-value | >0.05 | >0.05 | >0.05 | >0.05 | >0.05 |
Discussion
Stress hyperglycemia and insulin resistance are
common in critically ill patients, particularly those with sepsis
(3,28). Multiple pathogenetic mechanisms are
responsible for this metabolic syndrome; however, increased release
of pro-inflammatory mediators and counter-regulatory hormones may
serve a pivotal role (28). This
process leads to accelerated catabolism and strengthened dysplasia
function of glucose, which in turn results in stress hyperglycemia
(28). This condition is caused by a
decrease in insulin secretion under stress and represents a
temporary state of insulin resistance and concomitant relative
insulin deficiency (3–6). In early studies, Van den Berghe et
al (9) proposed the use of
insulin therapy for TGC (blood glucose level <6.1 mmol/l) to
reduce mortality and complications in critically ill patients in
surgical ICUs. Reports have indicated that this application of
insulin therapy can shorten the PICU stay and reduce the mortality,
infection and organ dysfunction rates in critically ill patients
with stress hyperglycemia (5,9,13,15–17,29,30).
However, other studies have documented advantages of freestyle
glycemic control using insulin (24,31). The
use of TGC is controversial. For example, a study conducted at
Leuven University demonstrated beneficial responses to TGC
(9), but follow-up studies could not
confirm these results (18,20,21,32).
Furthermore, a systematic review and network meta-analysis of
randomized controlled trials revealed no benefit of TGC with regard
to the length of hospitalization or death in critically ill
patients (8). The persisting
disparities in results reflect the difficulty of replicating such
research.
Severe stress hyperglycemia (blood glucose level
>25.00 mmol/l) was observed in no patients (0.00%) in the
present sample; 100% of patients had mild to moderate stress
hyperglycemia. This high blood glucose state seems to cause limited
harm to the body, but information on this issue is limited. In the
present study, no significant difference in the length of PICU stay
or total length of hospitalization among the TGC, CIT and control
groups was indicated. In addition, no correlation between the blood
glucose level and mortality, occurrence of secondary coma, or
development of secondary hepatic dysfunction and renal dysfunction
was indicated following treatment. These findings suggest no
superiority of TGC over other approaches, which is in agreement
with previously reported results (8,20). Thus,
the present findings did not demonstrate a benefit of insulin
therapy or risk associated with its non-use. Although we are not
aware of previous reports on the latter, the present retrospective
study demonstrated that transient mild to moderate stress
hyperglycemia does not typically cause harm and does not
necessitate insulin therapy. The results of the study suggest that
the blood glucose level can spontaneously return to normal as the
severe inflammatory reaction subsides and the patient's condition
improves. Marik and Raghavan (28)
indicated that only persistently high blood glucose levels can
cause organ damage. In the control group in the present study,
blood glucose levels had dropped to 9.5±3.5 mmol/l at 48 h
following PICU admission, were 6.8±1.7 mmol/l at 72 h, and were
considered normal (5.2±0.9 mmol/l) at 96 h. However, further
investigation is required to confirm these findings.
The present observation of hypoglycemia following
therapy in 5 patients in the TGC group (severe in 2 cases) is in
agreement with the results of a meta-analysis, which documented an
increased risk of hypoglycemia that was associated with target
blood glucose levels <110 mg/dl (6.1 mmol/l) (20). Although no correlation between the
blood glucose level and mortality or other complications was
identified, the potential risk of hypoglycemia associated with the
deterioration of patients' conditions cannot be excluded. Studies
with larger samples may help to clarify this issue.
Ketoacidosis generally occurs in children aged <5
years with type I diabetes and low levels of effective insulin
action (29,33). In the present study, no evidence of
this condition was indicated, even in patients who received no
insulin therapy. Due to its transient nature, stress hyperglycemia
may not cause ketoacidosis in non-diabetic patients (4).
Insulin therapy revealed no benefit in terms of the
length of hospitalization or risk of organ dysfunction or fatality,
and thus was not associated with improved clinical outcomes in
critically ill infants with stress hyperglycemia. Even without
insulin therapy, the blood glucose level may spontaneously return
to normal with no associated risk. However, further prospective
randomized controlled trials are required to confirm the findings
of the present study.
The mechanisms why insulin therapy exhibited no
benefit in pediatric patients with stress hyperglycemia in the
present study remain clear. Because this is a retrospective study,
all patients lacked data regarding insulin, c-peptide response and
inflammatory factors. Future prospective randomized controlled
trials will explore these mechanisms.
Acknowledgements
Not applicable.
Funding
The study was supported by the Department of Science
and Technology of Guangdong Province in 2011 (grant no.
2011B031800134).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
FW and YZ conceived and designed the experiments of
the current study. YZ, CL, MD and JfZ performed the experiments. FW
and JfZ analyzed the data. JpZ contributed
reagents/materials/analysis tools. FW and CL wrote the
manuscript.
Ethics approval and consent to
participate
The current study was approved by the ethics
committee of the Shunde Women and Children's Healthcare Hospital
(Foshan, China).
Patient consent for publication
All parents and guardians of the children enrolled
in the current study provided written informed consent.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ali Abdelhamid Y, Kar P, Finnis ME,
Phillips LK, Plummer MP, Shaw JE, Horowitz M and Deane AM: Stress
hyperglycaemia in critically ill patients and the subsequent risk
of diabetes: A systematic review and meta-analysis. Crit Care.
20:3012016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sanches LC, Pontes Azevedo LC, Salomao R,
Noguti MA, Brunialti M, Lourenco DM and Machado FR: Association
between early glycemic control and improvements in markers of
coagulation and fibrinolysis in patients with septic shock-induced
stress hyperglycemia. J Crit Care. 29:884.e1–e6. 2014. View Article : Google Scholar
|
|
3
|
Clowes GH Jr, Martin H, Walji S, Hirsch E,
Gazitua R and Goodfellow R: Blood insulin responses to blood
glucose levels in high output sepsis and spetic shock. Am J Surg.
135:577–583. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
NICE-SUGAR Study Investigators, ; Finfer
S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, Bellomo R,
Cook D, Dodek P, et al: Intensive versus conventional glucose
control in critically ill patients. N Engl J Med. 360:1283–1297.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cappi SB, Noritomi DT, Velasco IT, Curi R,
Loureiro TC and Soriano FG: Dyslipidemia: A prospective controlled
randomized trial of intensive glycemic control in sepsis. Intensive
Care Med. 38:634–641. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Robinson LE and van Soeren MH: Insulin
resistance and hyperglycemia in critical illness: role of insulin
in glycemic control. AACN Clin Issues. 15:45–62. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Agus MS, Hirshberg E, Srinivasan V,
Faustino EV, Luckett PM, Curley MA, Alexander J, Asaro LA,
Coughlin-Wells K, Duva D, et al: Design and rationale of heart and
lung failure-pediatric INsulin titration trial (HALF-PINT): A
randomized clinical trial of tight glycemic control in
hyperglycemic critically ill children. Contemp Clin Trials.
53:178–187. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yamada T, Shojima N, Hara K, Noma H,
Yamauchi T and Kadowaki T: Glycemic control, mortality, secondary
infection, and hypoglycemia in critically ill pediatric patients: A
systematic review and network meta-analysis of randomized
controlled trials. Intensive Care Med. 43:1427–1429. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Van den Berghe G, Wouters PJ, Bouillon R,
Weekers F, Verwaest C, Schetz M, Vlasselaers D, Ferdinande P and
Lauwers P: Outcome benefit of intensive insulin therapy in the
critically ill: insulin dose versus glycemic control. Crit Care
Med. 31:359–366. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
van Steen SC, Rijkenberg S, Limpens J, van
der Voort PH, Hermanides J and DeVries JH: The clinical benefits
and accuracy of continuous glucose monitoring systems in critically
Ill patients-a systematic scoping review. Sensors (Basel). 17(pii):
E1462017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Perez-Calatayud AA, Guillen-Vidana A,
Fraire-Felix IS, Anica-Malagon ED, Briones Garduno JC and
Carrillo-Esper R: Metabolic control in the critically ill patient
an update: Hyperglycemia, glucose variability hypoglycemia and
relative hypoglycemia. Cir Cir. 85:93–100. 2017.(In Spanish).
PubMed/NCBI
|
|
12
|
Kaminska H, Wieczorek P, Skala-Zamorowska
E, Deja G and Jarosz-Chobot P: Dysglycemia in critically ill
children. Pediatr Endocrinol Diabetes Metab. 22:21–25. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Plummer MP, Finnis ME, Phillips LK, Kar P,
Bihari S, Biradar V, Moodie S, Horowitz M, Shaw JE and Deane AM:
Stress induced hyperglycemia and the subsequent risk of type 2
diabetes in survivors of critical Illness. PLoS One.
11:e01659232016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tran NK, Godwin ZR, Steele AN, Wolf SE and
Palmieri TL: Clinical impact of accurate Point-of-care glucose
monitoring for tight glycemic control in severely burned children.
Pediatr Crit Care Med. 17:e406–e412. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pham TN, Warren AJ, Phan HH, Molitor F,
Greenhalgh DG and Palmieri TL: Impact of tight glycemic control in
severely burned children. J Trauma. 59:1148–1154. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Vlasselaers D, Mesotten D, Langouche L,
Vanhorebeek I, van den Heuvel I, Milants I, Wouters P, Wouters P,
Meyns B, Bjerre M, et al: Tight glycemic control protects the
myocardium and reduces inflammation in neonatal heart surgery. Ann
Thorac Surg. 90:22–29. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Day KM, Haub N, Betts H and Inwald DP:
Hyperglycemia is associated with morbidity in critically ill
children with meningococcal sepsis. Pediatr Crit Care Med.
9:636–640. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vlasselaers D: Blood glucose control in
the intensive care unit: Discrepancy between belief and practice.
Crit Care. 14:1452010. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Agus MS: Tight glycemic control in
children-is the target in sight? N Engl J Med. 370:168–169. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yatabe T, Inoue S, Sakaguchi M and Egi M:
The optimal target for acute glycemic control in critically ill
patients: A network meta-analysis. Intensive Care Med. 43:16–28.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Asencio Y, Lamy F and Paut O: Is it
necessary to obtain a tight glycemic control in critically ill
children? Ann Fr Anesth Reanim. 29:570–572. 2010.(In French).
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Clement S, Braithwaite SS, Magee MF,
Ahmann A, Smith EP, Schafer RG and Hirsch IB: Management of
diabetes and hyperglycemia in hospitals. Diabetes Care. 27:553–591.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Singer M, Deutschman CS, Seymour CW,
Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche
JD, Coopersmith CM, et al: The third international consensus
definitions for sepsis and septic shock (Sepsis-3). JAMA.
315:801–810. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kar P, Plummer MP, Bellomo R, Jenkins AJ,
Januszewski AS, Chapman MJ, Jones KL, Horowitz M and Deane AM:
Liberal glycemic control in critically Ill patients with type 2
diabetes: An exploratory study. Crit Care Med. 44:1695–1703. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zucchini S, Scaramuzza AE, Bonfanti R,
Buono P, Cardella F, Cauvin V, Cherubini V, Chiari G, d'Annunzio G,
Frongia AP, et al: A multicenter retrospective survey regarding
diabetic ketoacidosis management in Italian children with type 1
diabetes. J Diabetes Res. 2016:57194702016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Abstracts for the 42nd annual meeting of
the international society for pediatric and adolescent diabetes
(ISPAD), . 26-29–October;2016.Valencia, Spain: Pediatr Diabetes. 17
(Suppl 24):S5–S176. 2016. View Article : Google Scholar
|
|
27
|
Joffe A, Anton N, Lequier L, Vandermeer B,
Tjosvold L, Larsen B and Hartling L: Nutritional support for
critically ill children. Cochrane Database Syst Rev.
2209:CD0051442009.
|
|
28
|
Marik PE and Raghavan M:
Stress-hyperglycemia, insulin and immunomodulation in sepsis.
Intensive Care Med. 30:748–756. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Van den Berghe G, Wouters P, Weekers F,
Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P,
Lauwers P and Bouillon R: Intensive insulin therapy in critically
ill patients. N Engl J Med. 345:1359–1367. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Aberegg SK: Intensive insulin therapy in
the medical ICU. N Engl J Med. 354:2069–2071. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Luethi N, Cioccari L, Crisman M, Bellomo
R, Eastwood GM and Martensson J: Prevalence of ketosis, ketonuria,
and ketoacidosis during liberal glycemic control in critically ill
patients with diabetes: An observational study. Crit Care.
20:2972016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Branco RG, Xavier L, Garcia PC, Piva JP,
Fiori HH, Baldisserotto M, Fiori RM and Tasker RC: Prospective
operationalization and feasibility of a glycemic control protocol
in critically ill children. Pediatr Crit Care Med. 12:265–270.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Szypowska A, Ramotowska A,
Grzechnik-Gryziak M, Szypowski W, Pasierb A and Piechowiak K: High
frequency of diabetic ketoacidosis in children with newly diagnosed
type 1 diabetes. J Diabetes Res. 2016:95827932016. View Article : Google Scholar : PubMed/NCBI
|