Introduction
Ultrasound-guided intervention has many benefits.
The visually clear real-time pathway guarantees negligible
radiation hazard, secures procedural safety for aspiration, biopsy,
and ablation in the treatment of multiple organ diseases, enhances
multi-dimensional capability, provides convenience, decreases
procedure time, and minimizes cost (1,2). Also,
the pre-operative sampling of tumor mass is suggested to confirm
the presence of cancer and ascertain morphological subtype before
neo-adjuvant chemotherapy may lead to the potential diagnostic
misinterpretation of tumor cells and difficulties in detecting
residual tumor after neoadjuvant chemotherapy of bulky malignant
tissues (3).
Ultrasound-guided intervention has technically
evolved with clinical procedures conducted at the abdomen, thorax
and urogenital system (4).
Transvaginal ultrasound (TVUS)-guided biopsy is safe and effective
in the diagnosis of pelvic lesions (5–15).
TVUS-guided gun biopsy of the uterus and ovaries in
the office setting histologically confirmed 19 of the 22 (86.4%)
preliminary equivocal ultrasound diagnosis of adenomyosis,
leiomyoma and benign ovarian mass (5). The diagnostic accuracy of TVUS using
histopathology as a gold standard in identifying endometrial
hyperplasia among 263 perimenopausal women presenting with abnormal
uterine bleeding was found to be 75.6% (6).
TVUS has a high negative predictive value (99.1%)
for an endometrial thickness of 10.8 mm in the evaluation of 100
women with post-menopausal bleeding (7). The TVUS biopsy diagnosis of peritoneal
carcinomatosis and recurrent pelvic malignancy was validated in a
cohort of 50/54 (93%) women by comparison with the histopathologic
specimen or clinical course and outcome (8). TVUS-guided core needle biopsy
adequately obtained tumor samples from 200 women with
abdominopelvic or pelvic masses with 190 of 200 (95.0%) verified
before treatment (9). Of the 200, 97
(48.5%) were inoperable tumors, 13 (6.5%) were metastatic, 45
(22.5%) were recurrent and 45 (22.5%) were rare tumors (9). In 55 women with pelvic masses detected
on computed tomography (CT) or magnetic resonance imaging (MRI)
before the biopsy, 46 (84%) of the pelvic samples from TVUS core
biopsy were confirmed to be either malignant or benign, and 5 (9%)
were inflammatory lesions showing an overall diagnostic accuracy of
51/55 (93%) (10). Of the 48 women
diagnosed by ultrasound alone as having adenomyosis, 37 (77%) were
histologically confirmed as having adenomyosis after TVUS-guided
biopsy (11). Samples obtained by
TVUS guided uterine core biopsy from 80 cases of pre-menopausal
women scheduled for hysterectomy proved to be useful in the
investigation of early pathogenesis of adenomyosis (12).
Transrectal ultrasound (TRUS)-guided core biopsy
confirmed recurrent carcinoma of the uterine cervix in 16/17 (94%)
of women with non-diagnostic vaginal cytology and transvaginal
punch biopsy (13). TRUS-guided
biopsy revealed recurrent pelvic malignancy in 5/8 (62%) in women
presenting with abdomino-pelvic and back pain (14). TRUS examination was assessed to have
high diagnostic power for polycystic ovary syndrome among 183
Korean women aged 21–32 years (15).
Of the 11 studies that reported safety and efficacy,
only one study reported vaginal bleeding, 10/55 (18%) and gross
hematuria, 2/55 (4%) as TVUS procedure-related complications
(10). There was no reported
complication with TRUS-guided biopsy in any of the reports.
This study aimed to determine the accuracy and
safety of transvaginal and transrectal core needle biopsy of pelvic
cavity masses under ultrasound guidance. The authors undertook this
study since there is scant literature on the histological findings
from biopsies taken directly from the pelvic cavity and from pelvic
floor lesions.
Materials and methods
Subjects
We randomly obtained medical records of female
patients. A consecutive series of 40 patients with the diagnosis of
pelvic or pelvic floor masses between July 2015 and August 2017 at
the Department of Ultrasound of the First Affiliated Hospital of
Medical University of Anhui (Hefei, China) were considered eligible
and chosen for satisfying the inclusion criteria. Inclusion
criteria were as follows: i) Mass was detected by MRI or positron
emission tomography (PET)/CT one month prior to biopsy, ii) primary
origin was undetermined; iii) mass was visible by either
transvaginal or transrectal ultrasound technique, iv) mass was in
proximity, v) accessible to either TVUS- or TRUS-guided biopsy for
tissue sampling, and vi) histological confirmation is needed for
further patient management. Exclusion criteria were as follows: i)
No ultrasound-guided needle path, ii) poor coagulation function,
iii) severe infection, and iv) severe heart and lung
insufficiency.
Clinical laboratory indicators of patient status and
risk of complication were evaluated. The laboratory indicators were
complete blood count, prothrombin time, international normalized
ratio, activated partial thromboplastin time. We retrospectively
analyzed extracted clinicopathologic data.
Informed consent and ethics
approval
Before the procedure, patients were informed of the
risk of complications and potential damage to adjacent structures
along the path of the needle. Consent to proceed with the biopsy
was obtained before the procedure.
Before inclusion into the retrospective study,
patients or legally authorized representatives of subjects were
contacted. All the participants gave their informed consent for
inclusion and use of patient information. The protocol of the study
was approved by the Medical University of Anhui Institutional
Review Board. The IRB approval project identification code is
AF/SC-08/02.0. The study was conducted as per the Declaration of
Helsinki.
Instrument and biopsy procedure
None of the included patients had contraindications
for biopsy. Every biopsy was performed by one of two experienced
physicians (CG, LW) who had worked at least five years at the
interventional ultrasound department using US instrument (Logiq E9;
GE Healthcare, Chicago, IL, USA). TVUS- and TRUS-guided biopsies
were performed in the lithotomy position with empty bladder after
sterilization of the vagina and anus (16). The procedure utilized a reusable
automatic biopsy gun (Bard Biopsy, Tempe, AZ, USA) compatible with
an 18 gauge 15 cm tru-cut needle. The needle was inserted parallel
to the transvaginal US probe and was directed to the lesion with an
attached needle guide.
Local anesthesia and conscious sedation were not
used. The biopsy needle with ultrasonic dynamic monitoring led the
passage avoiding bowel, blood vessels, and bladder. The
morphological characteristics of the mass, size, location,
relationship with the adjacent tissues, and proximity to the vagina
or rectum were observed before puncture. Upon reaching the lesion
edge and gaining a penetration depth of >2.0 cm with strong echo
lesions, biopsy specimens were drawn from different directions
(17). All the specimens obtained
were immediately placed on a sterile filter paper and fixed in 10%
formaldehyde solution (Sigma-Aldrich; Merck KGaA, Darmstadt,
Germany). Sections and slides from paraffin-embedded tissue blocks
as samples were stained with hematoxylin-eosin.
After the transvaginal procedures, three sterilized
cotton balls were immediately tucked into the biopsy sites for
hemostasis. Bleeding and other possible complications were checked
after the cotton balls were taken out after 30 min. Patients were
observed around 30 min to 1 h with frequent vital signs monitoring
in a dedicated area. Safety of the procedure was concluded if there
were no or minor complications. If without discomfort or
complications, patients were returned to the ward or sent home. The
procedure and diagnostic criteria of TRUS-guided biopsy were
similar to that of TVUS (18).
Radiologic, pathologic, and clinical
data analyses
All archived CT, MRI, and ultrasonography (US)
images from the picture archiving and communication system
(PathSpeed, GE Healthcare, Milwaukee, WI, USA) were re-evaluated.
Radiologists were aware of the history of the patient illness but
blinded to all other clinical information. Two radiologists
independently evaluated the pelvic lesions based on the: i) lesion
size, ii) lesion nature (e.g., solid or cystic) (19), and iii) lesion site. The biopsy core
number was counted from images, and the biopsy distance was
determined from the standard reports. The biopsy distance was
defined by the measured mean length of the biopsy needle seen on US
images. Disagreements of the evaluation of two radiologists were
resolved by consensus. If no agreement was reached, a third
evaluator was consulted for final consensus.
An experienced pathologist evaluated the histology
of the specimen. The pathologist was aware of the history of the
patient illness but blinded to all other clinical information
including the imaging results (20).
The step detects the presence or absence of malignancy thereby
detecting or excluding the diagnosis (21). Possible complications based on the
patients' medical records were evaluated using the Clavien-Dindo
classification (22).
Results
Of the 40 female patients included in the study, 39
had TVUS, and 1 had TRUS-guided biopsy. The mean age was 54 years
(range, 46–69 years). All laboratory results were within the
acceptable normal range of coagulation parameters (Table I). There were no complications
identified.
 | Table I.Normal values of coagulation in
patients undergoing TVUS- and TRUS-guided aspiration biopsy. |
Table I.
Normal values of coagulation in
patients undergoing TVUS- and TRUS-guided aspiration biopsy.
| Hematologic test | Normal range of
values (reference) | Cut-off |
|---|
| Activated partial
thromboplastin time | 28.0–42.0 | 45 |
| INR | 0.85–1.15 | 1.6 |
| Platelets,
109/l | 125–350 | 50 |
| Prothrombin time | 11.0–16.0 | 18 |
The median lesion size was 5.5 cm (range, 1–15 cm).
Thirty-four of the lesions were solid while six were cystic. The
mean distance of the biopsy was 2.4 cm (range, 1.4–5.6 cm). The
median number of biopsy cores obtained from each patient was 4.0
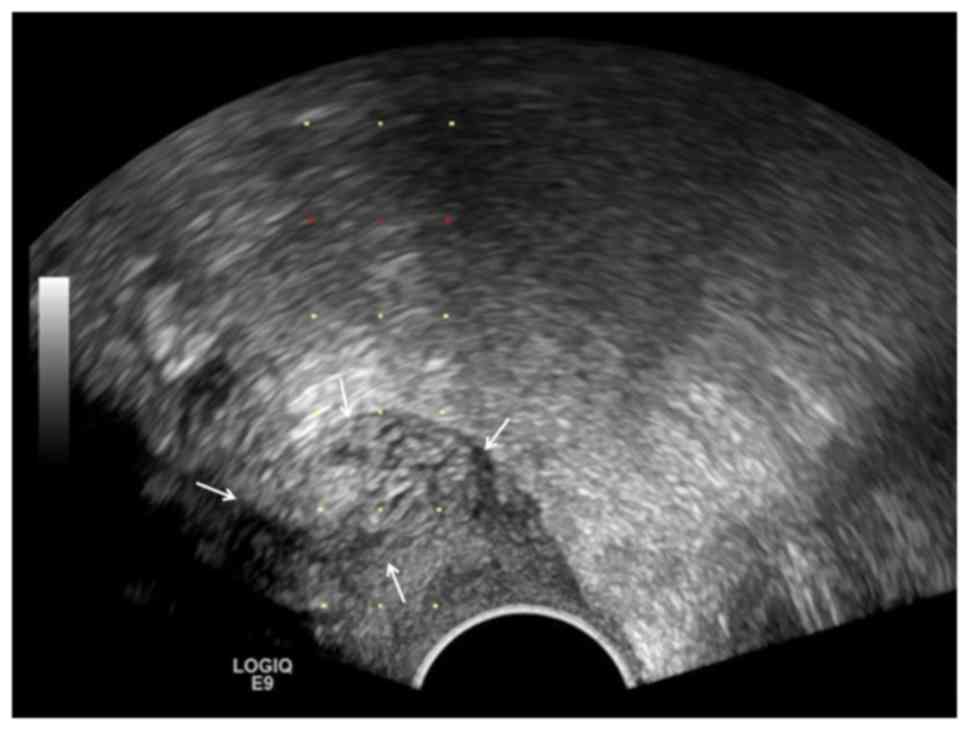
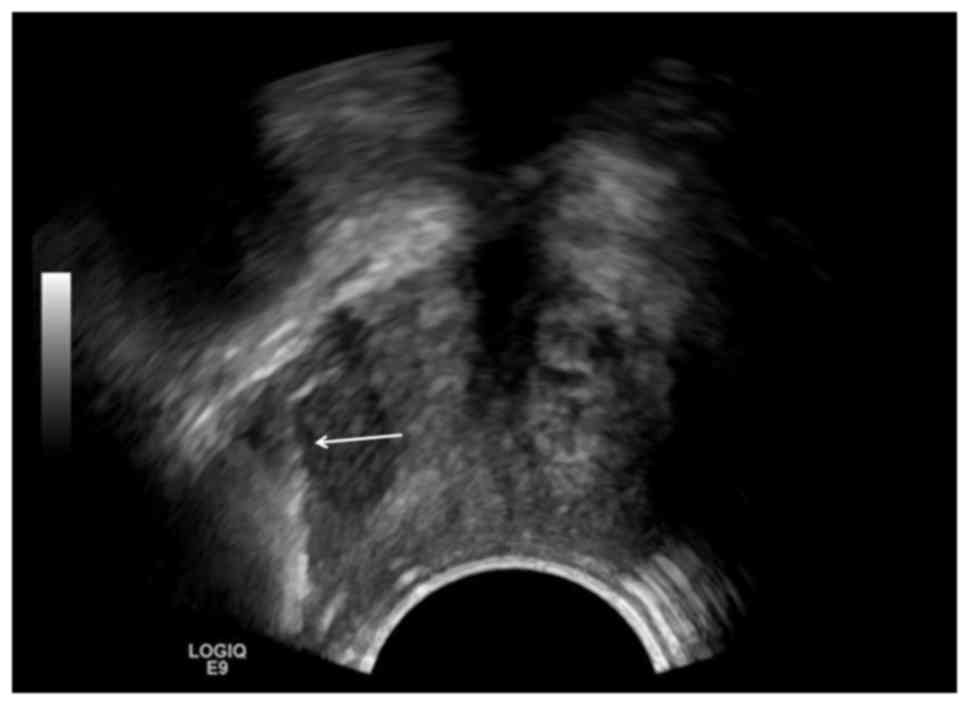
(range, 2–7 cores). The specimens (Table II) were obtained from pelvic cavity
and pelvic floor in 18 cases (45%), the vaginal stump in 6 cases
(15%), the cervix in 2 cases (5%) and the vaginal fornix in 13
cases (32.5%). Representative cases are shown in Figs. 1–4.
| Table II.Malignancy proven lesions from
transvaginal ultrasound-guided aspiration biopsies. |
Table II.
Malignancy proven lesions from
transvaginal ultrasound-guided aspiration biopsies.
| Patient | Age (years) | MRI and PET/CT
findings at sites | Pathomorphological
findings | Diagnosis |
|---|
| 1 | 84 | Pelvic cystic, solid
mass | Grayish white, poorly
differentiated cancer | Ovarian cancer |
| 2 | 67 | Vaginal stump
hypoechoic | Low-grade
adenocarcinoma | Ovarian cancer |
| 3 | 60 | Bottom of the pelvic
floor | Grayish white, poorly
differentiated adenocarcinoma | Ovarian cancer |
| 4 | 52 | Low echo above the
vaginal stump | Grayish white, poorly
differentiated squamous cell carcinoma | Cervical cancer |
| 5 | 46 | Cervical anterior lip
hypoechoic | Medium-differentiated
adenocarcinoma, metastatic carcinoma of the upper digestive source
may be large | Metastatic
adenocarcinoma, upper gastrointestinal |
| 6 | 68 | Pelvic floor
cervix | Gray-white, poorly
differentiated urothelial carcinoma may be large | Cervical cancer |
| 7 | 46 | Low echo above the
vaginal stump | Gray-white, poorly
differentiated cancer, combined with a history of breast cancer
metastasis may be large | Metastatic poorly
differentiated, breast |
| 8 | 54 | Right ovarian | Grayish white,
spindle cell lesion, solid lesion | Ovarian cancer no
excluding sex stromal tumor |
| 9 | 47 | Low echo of the left
uterus | 3 grayish white,
high-grade serous carcinoma, source of female reproductive
system | Ovarian cancer |
| 10 | 62 | Hypoechoic lesion on
the left side of the posterior vagina | 3 grayish white,
ovarian serous carcinoma metastasis | Ovarian cancer |
| 11 | 46 | Cervical anterior and
posterior lip hypoechoic, cervix 1, cervix 2, anterior vaginal
wall | High-grade squamous
intraepithelial neoplasia CIN3, suspicious microinvasive, chronic
inflammation of vaginal lesions | Cervical cancer |
| 12a | 47 | Cervical, ovary | 1 anterior lip of the
cervix, smooth muscle; 1 posterior lip of the cervix,
adenocarcinoma; 2 ovarian cancer, adenocarcinoma; | Straight B junction
tumor ovarian metastasis |
| 14 | 50 | Hypoepitic lesions
above the vagina | Grayish white 3,
leiomyoma | Uterine fibroids |
| 15 | 67 | Vaginal stump cystic,
solid mass | Poorly differentiated
cancer | Ovarian cancer |
| 16 | 60 | Right ovarian giant
cystic | Medium differentiated
adenocarcinoma | Metastatic non-small
cell lung cancer, adenocarcinoma |
| 17 | 47 | Vaginal stump | Poorly differentiated
cancer | Ovarian cancer |
| 18 | 52 | Pelvic mass | Poorly differentiated
cancer | Ovarian cancer |
| 19 | 62 | Cervical
hypoechoic | Squamous cell
carcinoma | Cervical cancer |
| 20 | 61 | Double ovarian solid
mass | Metastatic poorly
differentiated adenocarcinoma | Metastatic non-small
cell lung cancer, adenocarcinoma |
| 21 | 56 | Vaginal stump | Poorly differentiated
cancer | Cervical cancer |
| 22 | 61 | Vaginal wall
stump | Poorly differentiated
cancer | Cervical cancer |
| 23 | 48 | Left attachment
pocket solid mass | Serous carcinoma | Ovarian cancer |
| 24 | 71 | Vaginal stump | Endometriosis | Endometriosis |
| 25 | 45 | Left ovary
hypoechoic | Spindle cell
tumor | Sex cord stromal
tumor |
| 26 | 52 | Low echo of the
anterior wall of the vagina | Leiomyoma | Vaginal
leiomyoma |
| 27 | 43 | Pelvic cystic mixed
echo | Serous
carcinoma | Ovarian cancer |
| 28a | 54 | Left genital
hypoechoic lesion | Adenoid cystic
carcinoma | Ovarian cancer |
| 29 | 67 | Vaginal stump | Adenocarcinoma | Endometrial
cancer |
| 30 | 56 | Left ovarian solid
part and posterior lip lesion | Poorly
differentiated cancer | Ovarian cancer |
| 31 | 52 | Posterior wall of
the lower vagina | Leiomyoma | Uterine
fibroids |
| 32 | 64 | Above the vaginal
stump | Endometrial stromal
sarcoma | Uterine cancer |
| 33 | 70 | Cervical
hypoechoic | Inflammatory | Inflammatory cells,
cervix |
| 34 | 59 | Uterine rectal
fossa lesion | Serous
carcinoma | Ovarian cancer |
| 35 | 42 | Left echo low echo
nodule | Metastatic
cancer | Endometrial
cancer |
| 36 | 53 | Uterine rectal
fossa lesion | Serous
carcinoma | Ovarian cancer |
| 37 | 46 | Subcutaneous
hypoechoic | Adenoid cystic
carcinoma infiltration | Vaginal cancer |
| 38 | 42 | Pelvic mass | Low-grade
adenocarcinoma | Cervical
cancer |
| 39 | 41 | Vaginal stump | Squamous cell
carcinoma | Cervical
cancer |
| 40 | 54 | Uterine rectal
fossa | Left ovarian
granuloma | Ovarian cancer |
All the specimens were adequate for histologic
evaluation and diagnosis with 72% (28/39) being identified as
primary and 13% (5/39) as metastatic malignancy. There was one
diagnosed case of rectal cancer with a post-operative specimen from
the posterior wall of the anal canal obtained by TRUS-guided biopsy
(2.5%).
Discussion
A retrospective analysis was performed in our center
to determine whether TVUS- and TRUS-guided aspiration biopsy allows
the detection of a malignant pathology in the pelvic/pelvic floor.
The study shows detection in almost all suspicious clinical cases
by MRI or PET/CT consistent with a more than 90% adequacy and
accuracy of other studies (8–10). An
experienced pathologist provided the expertise that has optimized
the use of aspiration biopsy.
TVUS- or TRUS-guided aspiration biopsy has several
advantages. The biopsy is technically easy and does need
anesthesia. Either of the two techniques can be used as a
first-line investigation in the evaluation of women with pelvic or
pelvic floor masses (6,9). The biopsy can be supplemented with
procedures such as laparoscopy for lesions involving ovary and
cervix as experienced in the hospital. In addition to the
traditional benefits of ultrasound-guided biopsy (1,2), seeding
by malignant cells seems low risk (9). Also, it is not known whether the risk
of infection is high with the transrectal or transvaginal
approaches. Antibiotic prophylaxis is well-established in
transrectal biopsy of the prostate (23). However, whether infection and
subsequent antibiotic prophylaxis are necessary for TVUS-guided
biopsy remains to be observed.
The present study has several limitations. As a
retrospective analysis using medical chart reviews, data inputted
from medical records were not sufficient to determine diagnostic
performance. Analysis to provide valid and reliable diagnostic
performances (sensitivity, specificity, positive predictive value,
negative predictive value, accuracy) requires the identification of
a set of variables to provide the best prediction. Missing data
precluded the detection of increasing diagnostic certainty from
imaging to histopathology. Detection or exclusion of malignancy
using test-result based sampling or case-referent sampling is ideal
(21).
Second, the diagnostic test is almost always not
applied in isolation but in combination (21). Interacting variables (relevant
clinical variables, tumor markers, CT/MRI, clinical stage of
cancer) increase sample size and may not be easy to be obtained. To
conduct this kind of study, we may have to collaborate with other
hospital centers. Finally, there were case scenarios in the
management of cancer patients that were not encountered but are
potentially significant: i) A previously diagnosed benign tumor
turning out to be malignant, ii) distinguishing either a recurrence
or post-treatment fibrosis, iii) whether TRUS complements TVUS, and
iv) follow-up stage of cancer management.
Despite the limitations, the validity of the
pathomorphologic findings and final diagnosis were not compromised
because the pathologist was blinded to all other clinical
information including the imaging results.
Ultrasound-guided transvaginal or transurethral
biopsy seems to be a reliable and safe procedure for
histopathological evaluation of the pelvic cavity and pelvic mass
lesions. Prospective studies of adequate sample size are needed to
evaluate the usefulness of the procedures across various clinical
case scenarios.
Acknowledgements
Not applicable.
Funding
This study was supported by the National Scientific
Foundation Committee of China (No. 81801723) and the Clinical
Research Support Foundation of the Chinese PLA General Hospital
(No. 2017FC-CXYY-3005).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CG. participated in the analysis and interpretation
of data, and drafted the manuscript. XL made substantial
contributions to the conception and design of the study. CG, LW and
CZ carried out the study and collected the data. XL contributed to
revising the manuscript critically for important intellectual
content. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This retrospective medical record review was
approved by the Institutional Review Board/Clinical Medical
Research Ethics Committee of the First Affiliated Hospital of Anhui
Medical University (Approval no: AF/SC-08/02.0)
Patient consent for publication
Not applicable
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Copelan A, Scola D, Roy A and Nghiem HV:
The myriad advantages of ultrasonography in image-guided
interventions. Ultrasound Q. 32:247–257. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Park BK: Ultrasound-guided genitourinary
interventions: Principles and techniques. Ultrasonography.
36:336–348. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
McCluggage WG, Lyness RW, Atkinson RJ,
Dobbs SP, Harley I, McClelland HR and Price JH: Morphological
effects of chemotherapy on ovarian carcinoma. J Clin Pathol.
55:27–31. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dietrich CF and Numberg E: A Practical
Guide and Atlas. Intervention Ultrasound. 1st. Thieme; Stuttgart,
Germany: pp. 4042014
|
|
5
|
Walker J and Jones K: Transvaginal
ultrasound guided biopsies in the diagnosis of pelvic lesions.
Minim Invasive Ther Allied Technol. 12:241–244. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nazim F, Hayat Z, Hannan A, Ikram U and
Nazim K: Role of transvaginal ultrasound in identifying endometrial
hyperplasia. J Ayub Med Coll Abbottabad. 25:100–102.
2013.PubMed/NCBI
|
|
7
|
Menon S and Sreekumari I: Role of
transvaginal ultrasound in the assessment of endometrial pathology
in patients with post-menopausal bleeding. Int J Reprod Contracept
Obstet Gynecol. 6:1376–1380. 2017. View Article : Google Scholar
|
|
8
|
Dadayal G, Weston M, Young A, Graham JL,
Mehta K, Wilkinson N and Spencer JA: Transvaginal ultrasound
(TVUS)-guided biopsy is safe and effective in diagnosing peritoneal
carcinomatosis and recurrent pelvic malignancy. Clin Radiol.
71:1184–1192. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lin SY, Xiong YH, Yun M, Liu LZ, Zheng W,
Lin X, Pei XQ and Li AH: Transvaginal ultrasound-guided core needle
biopsy of pelvic masses. J Ultrasound Med. 37:453–461. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Park JJ, Kim CK and Park BK:
Ultrasound-guided transvaginal core biopsy of pelvic masses:
Feasibility, safety, and short-term follow-up. AJR Am J Roentgenol.
206:877–882. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Elkattan E, Omran E and Al Inany H: The
accuracy of transvaginal ultrasound and uterine artery Doppler in
the prediction of adenomyosis. Middle East Fertil Soc J. 15:73–78.
2010. View Article : Google Scholar
|
|
12
|
Tellum T, Qvigstad E, Skovholt EK and
Lieng M: In vivo adenomyosis tissue sampling using a transvaginal
ultrasound-guided core biopsy technique for research purposes:
Safety, feasibility, and effectiveness. J Minim Invasive Gynecol.
Feb 8–2019.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Roy D, Kulkarni A, Kulkarni S, Thakur MH,
Maheshwari A and Tongaonkar HB: Transrectal ultrasound-guided
biopsy of recurrent cervical carcinoma. Br J Radiol. 81:902–906.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Giede C, Toi A, Chapman W and Rosen B: The
use of transrectal ultrasound to biopsy pelvic masses in women.
Gynecol Oncol. 95:552–556. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lee DE, Park SY, Lee SR, Jeong K and Chung
HW: Diagnostic usefulness of transrectal ultrasound compared with
transvaginal ultrasound assessment in young Korean women with
polycystic ovary syndrome. J Menopausal Med. 21:149–154. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Plett SK, Poder L, Brooks RA and Morgan
TA: Transvaginal ultrasound-guided biopsy of deep pelvic masses:
How we do it. J Ultrasound Med. 35:1113–1122. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zikan M, Fischerova D, Pinkavova I, Dundr
P and Cibula D: Ultrasound-guided tru-cut biopsy of abdominal and
pelvic tumors in gynecology. Ultrasound Obstet Gynecol. 36:767–772.
2010. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Alborzi S, Rasekhi A, Shomali Z, Madadi G,
Alborzi M, Kazemi M and Hosseini Nohandani A: Diagnostic accuracy
of magnetic resonance imaging, transvaginal, and transrectal
ultrasonography in deep infiltrating endometriosis. Medicine
(Baltimore). 97:e95362018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fischerova D: Ultrasound scanning of the
pelvis and abdomen for staging of gynecological tumors: A review.
Ultrasound Obstet Gynecol. 38:246–266. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
de Groot JA, Bossuyt PM, Reitsma JB,
Rutjes AW, Dendukuri N, Janssen KJ and Moons KG: Verification
problems in diagnostic accuracy studies: Consequences and
solutions. BMJ 343 (aug02 3). d47702011.
|
|
21
|
Knottnerus JA, van Weel C and W Muris J:
Evaluation of diagnostic procedures. Evidence base of clinical
diagnosis. 324:(2nd). Knottnerus JA: BMJ Books. (London). 477–480.
2002.
|
|
22
|
Clavien PA, Barkun J, de Oliveira ML,
Vauthey JN, Dindo D, Schulick RD, de Santibañes E, Pekolj J,
Slankamenac K, Bassi C, et al: The Clavien-Dindo classification of
surgical complications: Five-year experience. Ann Surg.
250:187–196. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Noreikaite J, Jones P, Fitzpatrick J,
Amitharaj R, Pietropaolo A, Vasdev N, Chadwick D, Somani BK and Rai
BP: Fosfomycin vs. quinolone-based antibiotic prophylaxis for
transrectal ultrasound-guided biopsy of the prostate: A systematic
review and meta-analysis. Prostate Cancer Prostatic Dis.
21:153–160. 2018. View Article : Google Scholar : PubMed/NCBI
|