Introduction
Atlantoaxial rotatory fixation (AARF) is a condition
in which the first two cervical vertebrae (C1 and C2) are fixed in
rotational malalignment. The underlying cause of AARF remains to be
fully elucidated (1). Mechanically,
there is temporary atlantoaxial instability resulting in
subluxation between C1 and C2, and failure to reduce spontaneously
may lead to AARF (2). The condition
is not unique to children, but it most frequently affects the
growing skeleton. Subluxation may be associated with several
underlying conditions, including acute acquired torticollis,
clavicle fracture, upper-respiratory-tract infection, surgery in
the head and neck area or minor trauma, although no identifiable
predisposing factors are mandatory for the diagnosis. Long-term
morbidity in cases of AARF is likely if the condition remains
untreated, with instability in the atlantoaxial joint (3), and subsequent remodeling of the
vertebrae to a non-anatomic form renders late spontaneous reduction
impossible, highlighting the requirement for early surgical
intervention (4). Missed AARF may
result in paralysis, nerve damage and fatality (5).
Clinicians should always be aware of AARF when
treating a child presenting with neck pain and an abnormal position
of the head. Typically, the child is unable to return the head to a
neutral position and turn it past the midline, but their
neurological status is almost always normal. In cases where
symptoms have lasted for more than a few days without spontaneous
relief, AARF requires to be ruled out. However, the diagnosis of
AARF is frequently delayed. Plain radiographs are difficult to
interpret, albeit they are usually used in primary imaging for
practical reasons (6–8). Computer tomography (CT) is valuable for
measuring the rotatory angle and the distance between the atlas
(C1) and dens (C2) (atlas-dens index), which reflects anterior
displacement of the atlas (9).
Children with benign torticollis or slight Fielding type 1 AARF
present with a normal C1-C2 association in CT scans (6). Three-dimensional (3D) spiral CT is
considered to be the best diagnostic tool to evaluate AARF
(10–12). Dynamic CT covering the skull base and
upper cervical spine with the head rotated to the maximal left and
maximal right positions is recommended as a method of choice for
the diagnosis of AARF, despite its poor reliability and
reproducibility (7,13). Subluxation is classified into four
groups, according to the CT findings (14): Type 1, unilateral anterior rotation
of the atlas pivoting around the dens; type 2, unilateral anterior
rotation of the atlas with an atlas-dens index of 3–5 mm; type 3,
bilateral anterior subluxation with an atlas-dens index of >5
mm; type 4, posterior displacement of the atlas relative to the
axis. Magnetic resonance imaging (MRI) of the brain and cervical
spine is recommended for acquired torticollis if the CT findings
are negative (9). MRI is superior in
recognizing the potential associated ligamentous injuries in soft
tissues (1).
It is known that early reduction of subluxation
results in good outcomes and a low rate of recurrent subluxation,
whereas subjects with a longer history of subluxation may require
skeletal traction and halo/rigid collar immobilization or surgical
reduction and fusion (15).
Specifically, a Fielding type 2 (or higher) condition requires
skeletal traction (16). Therefore,
any neck pain and head malrotation persisting for more than a few
days usually merit close investigation, i.e. static and/or dynamic
CT scans. However, MRI has certain advantages over CT regarding the
diagnostic performance and due to the lack of associated ionizing
radiation (1). The present study
reports on the pioneering practice of utilizing 1.5 Tesla (T)
interventional MRI in the treatment of a pediatric patient with
suspected acute AARF. In addition, the current literature regarding
the imaging modalities used in cases of AARF for diagnostic
purposes and during reduction was reviewed.
Materials and methods
Treatment strategy
In the present study, a radiation-free method for
the treatment of AARF in a pediatric patient is described and it is
based on interventional MRI instead of CT. The technique is
explained in detail and its feasibility in the treatment of a young
child was closely evaluated. The present study was based on the
urgent ad hoc clinical treatment of the patient. It was
considered, a priori, that this experimental study treatment
method that utilizes interventional MRI instead of dynamic CT in
confirming the reduction, would be safer with regard to radiation
exposure and superior in the visualization of soft-tissue pathology
than the traditional method using CT (1). Hence, ethics board approval was
considered to not be required, also in the light of the poor
condition of the patient and risks associated with delayed
treatment, implying the urgency of intervention. However, besides
interventional MRI, the treating team was still prepared to perform
traditional care with using dynamic CT if required.
Literature review
A literature search was performed in the MEDLINE
biomedical literature database, with an advanced search in PubMed
using the following search terms: ‘atlantoaxial rotation(al)
fixation’, ‘atlantoaxial rotation(al) subluxation’, ‘nasopharyngeal
torticollis’ and ‘Grisel syndrome’. The same terms were used for a
search in the Google Scholar database, while the non-scientific
citations retrieved were ignored. Primarily, original studies and
case reports in English and those with at least an English abstract
were reviewed to study imaging practices and treatment techniques.
Articles in languages other than English were excluded.
Furthermore, beyond the systematic search described above, all
reference lists of the published articles retrieved in these
searches were reviewed to identify further relevant studies. The
focus of the literature review was the role of static MRI in the
early stage of diagnosis and the possible role in interventional
investigation. Studies on patients with a growing skeleton and/or
those of <16 years of age were considered eligible. Studies on
fracture cases, syndromic patients and chronic AARF were excluded.
The major focus of the present literature review was to identify
imaging modalities used for diagnostic purposes in the acute stage
of AARF and also to identify any published experience of using MRI
as an interventional method during AARF reduction in children. The
search included studies published between January 1st, 1998 and
March 31st, 2018. Finally, a total of 28 original studies and case
reports were included (Table I).
 | Table I.A literature review of studies
published since 1998 regarding imaging modalities and treatment
methods for AARF in pediatric patients. |
Table I.
A literature review of studies
published since 1998 regarding imaging modalities and treatment
methods for AARF in pediatric patients.
| Author (year) | Cases (n) | Study design | Patient age
(years) | Imaging methods
used | Treatment | (Refs.) |
|---|
| Beier et al
(2012) | 40 | 9-year
retrospective |
| 3D-CT and MRI | Rigid cervical
collar. There was alar ligament damage | (18) |
| Mihara et al
(2001) | 35 |
| Mean 6.5 | N/A | Halter traction 2–3
weeks, 25.7% recurrence | (19) |
| Pang and Li
(2005) | 29 | Prospective |
| Dynamic CT |
| (14) |
| Subach et al
(1998) | 20 | 7-year
retrospective | Mean 6.4 | Plain radiographs +
dynamic CT | Rigid collar (n=5)
and traction (n=15) | (15) |
| Mezue et al
(2002) | 13 | 2-year
retrospective case series | 3–12 | X-ray, CT, MRI | Neck collar,
NSAIDs, rest, halter traction for AARF (n=3) | (20) |
| Ciftdemir
(2012) | 12 | Retrospective case
series |
| X-ray and axial
CT | Traction treatment,
3 weeks collar. All recovered | (21) |
| Deichmueller and
Welkoborsky (2010) | 12 | Retrospective case
series | Mean 7.1 | X-ray, ultrasound,
CT, MRI | 4 required closed
reduction and external fixation with Halo-vest, 8 had a spontaneous
reduction | (22) |
| Tauchi et al
(2011) | 7 |
|
| 3D-CT | Halo-vest | (4) |
| Lee et al
(2002) | 2 (+4 chronic) | 5-year
retrospective case series | Mean 9 (7–12) | X-ray, CT | Non-operative
care | (23) |
| Rahimi et al
(2003) | 6 (AARF) (of total
23) | 12-year
retrospective case series | Mean 7.5
(1.8–14.6) | X-ray, dynamic
CT | Immobilization with
collar, traction | (24) |
| Been et al
(2007) | 2 (of total 4) | Case series | 6.5 | CT, 3D-CT | Spontaneous
reduction of benign torticollis | (25) |
| Fernández Cornejo
(2003) | 4 | 7-year
retrospective |
| CT + 3D-CT | Non-operative
care | (26) |
| Holcomb et
al (2001) | 4 | 2-year
retrospective case series | N/A | N/A | N/A | (27) |
| Martinez-Lage et
al (2001) | 4 | 5-year
retrospective | Mean 8.2 | X-ray and CT of
all, 3D-CT of 3, MRI of 1 |
| (28) |
| Ortiz et al
(2013) | 3 | Case series | N/A | X-ray, CT, MRI | NSAIDs,
immobilization, traction/surgery | (29) |
| Muniz and Belfer
(1999) | 2 | Case series | N/A | N/A | Non-operative | (30) |
| Meek et al
(2001) | 1 | Case report | 4 | Plain
radiographs | Non-operative care
for 1 week | (31) |
| Galer et al
(2005) | 1 | Case report | 3 (female) | Dynamic CT | Non-operative | (32) |
| Sobolewski et
al (2008) | 1 | Case report | 5 (male) | Dynamic CT | Manual reduction
under sedation | (33) |
| Pilge et al
(2011) | 1 | Case report | 11 (female) | X-ray, CT | Manual reduction
under GA, cervical collar for 2 weeks + antibiotics | (34) |
| Wurm et al
(2004) | 1 | Case report | 3 (male; 5 days of
symptoms) | CT and MRI | Manual reduction
under GA, antibiotics for upper respiratory tract infection,
Minerva | (35) |
| Missori et
al (2005) | 1 | Case report | 7 (female) | X-ray, CT, MRI | Cervical brace | (36) |
| Maile and Slongo
(2007) | 1 | Case report | 3 (male) | 3D-CT | 24 h skeletal
traction, followed by 3 weeks of cervical soft brace | (16) |
| Gourin et al
(2002) | 1 | Case report | 7 (male) | X-ray, CT, MRI | Halo-traction | (37) |
| Park et al
(2013) | 1 | Case report | 9 (male) | Dynamic CT,
Fielding 2, static MRI | Neck brace, halter
traction, 14-day follow-up with dynamic CT and MRI | (38) |
| Sia et al
(2012) | 1 | Case report | 7 (male) | X-ray, CT, | Cervical collar,
medicines, traction 2 weeks later | (39) |
| Barcelos et
al (2014) | 1 | Case report | 7 (1 weeks'
torticollis) | CT | Soft cervical
collar | (17) |
| Tsai and Chou
(2005) | 1 | Case report | 4 (female; 1 week
after fall) | 3D-CT | Manipulation under
GA | (40) |
Results
AARF treatment approach using
interventional MRI
As a major feature of the present study, a
radiation-free orthopedic technique was developed. The treatment
comprised of simultaneous manual axial traction and manual closed
reduction of AARF, with the patient lying in the supine position
under general anesthesia, with interventional MRI during the same
period of anesthesia to make sure that reduction is achieved and
held. For the present study, interventional MRI is classified as a
therapeutic orthopedic procedure performed under special
circumstance that allows unrestricted use of interventional MRI
with viewing monitors close to the operating table and equipment
for general anesthesia. The reduction maneuver is based on turning
the head first maximally right and then left during traction, in a
manner similar to that performed in the procedure called dynamic CT
(13). Thereafter, a rigid cervical
collar was used for several weeks to stabilize the vertebras in the
correct position.
Case presentation
A female patient aged 4 years with neck pain and the
head tilted to the left for 1 week presented at the pediatric
orthopedic unit Oulu University Hospital (Oulu, Finland; March
2018). The patient had not suffered any injury or accident and
there was no sign of upper or lower-respiratory-tract infection.
Movement of the head was impossible due to the pain associated with
it; there was also no evidence of the patient turning her head
while sleeping. The sternocleidomastoid muscle was not prominent
and the clavicle was intact. The neurological status was normal.
Since the symptoms had lasted for 1 week, AARF was suspected. The
condition justified early plain radiographs, but as a result of
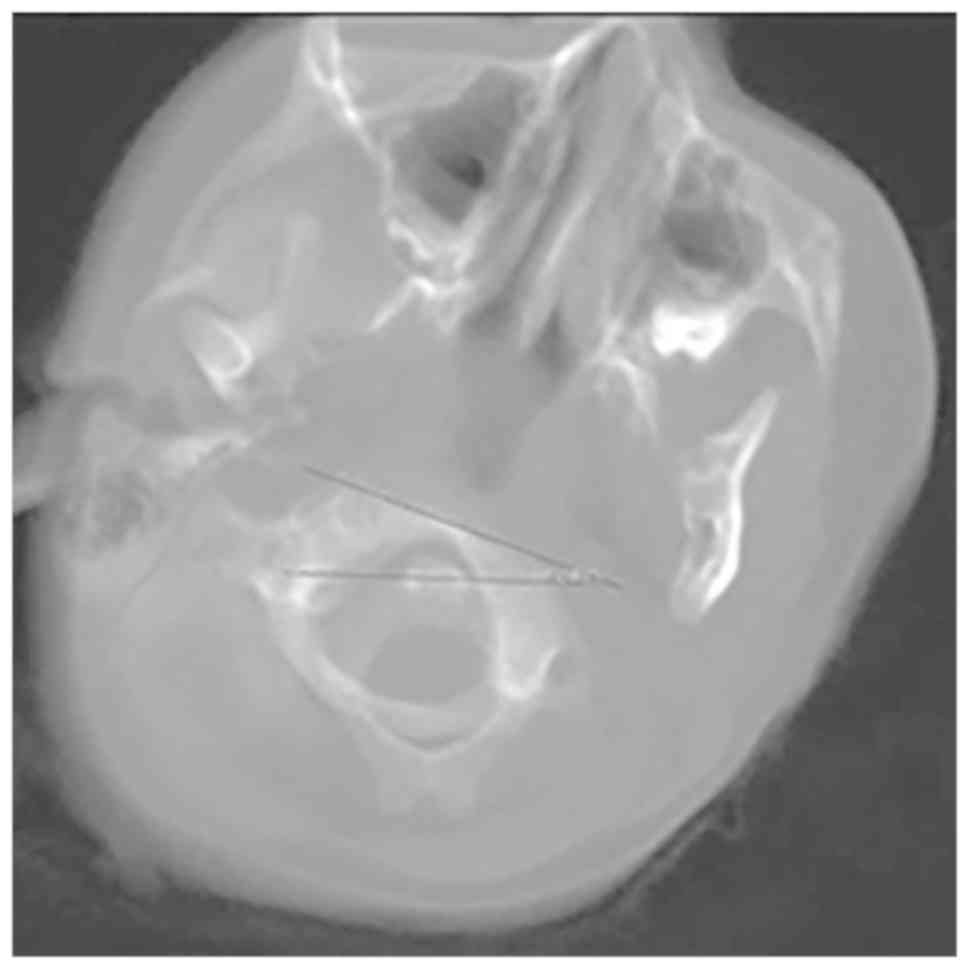
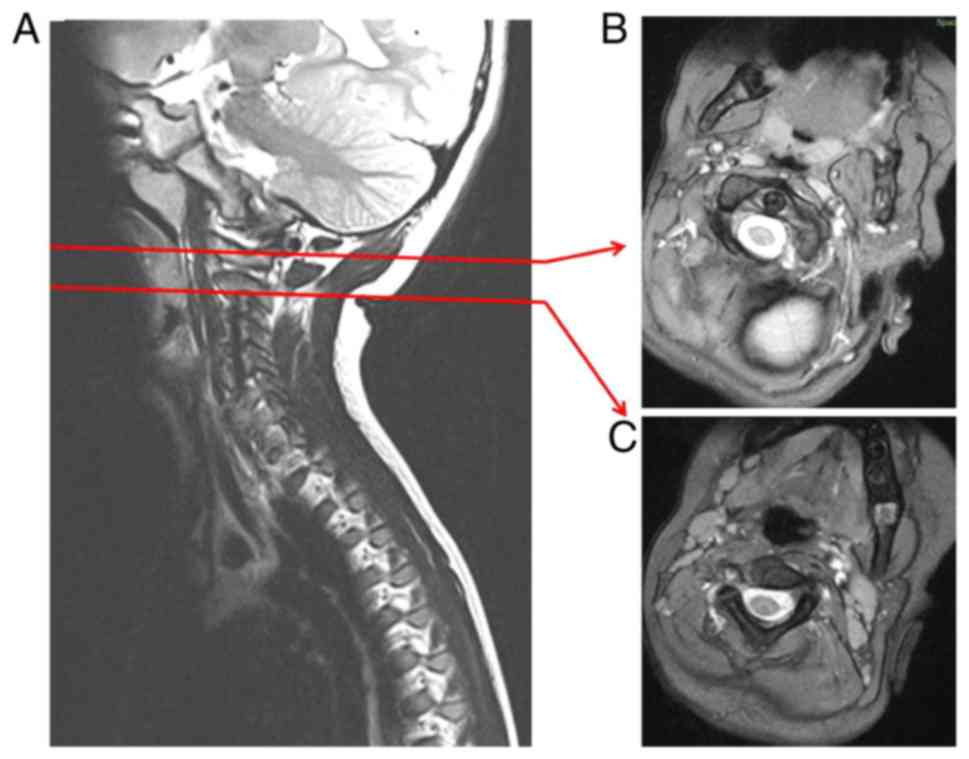
poor cooperation, plain radiographs were not available. Static CT
and conventional static MRI scans were performed and rotational
positioning without an increased distance between the dens and the
arc of C1 was determined, suggesting Fielding type 1 AARF (Figs. 1 and 2). There was no indication of trauma and no
vertebral anomalies were observed. Aiming at expedited diagnosis
and treatment, dynamic CT was first considered as a diagnostic
procedure and also during manipulation. However, it was not
considered optimal due to the ionizing nature of the radiation and
lack of soft-tissue identification. Therefore, a new study protocol
(termed as interventional MRI for AARF in the present study) was
set up: Scanning of the upper cervical spine by means of 1.5T
interventional MRI (Siemens Magnetom Espree, Siemens Healthcare
GmbH, Erlangen, Germany) with a single T2-weighted sequence to
ensure a fast-operating time with reliable diagnostic accuracy.
General anesthesia (GA) was required due to the severe pain
associated with the movement of the cervical spine. The patient's
head was carefully manipulated by a pediatric orthopedic surgeon
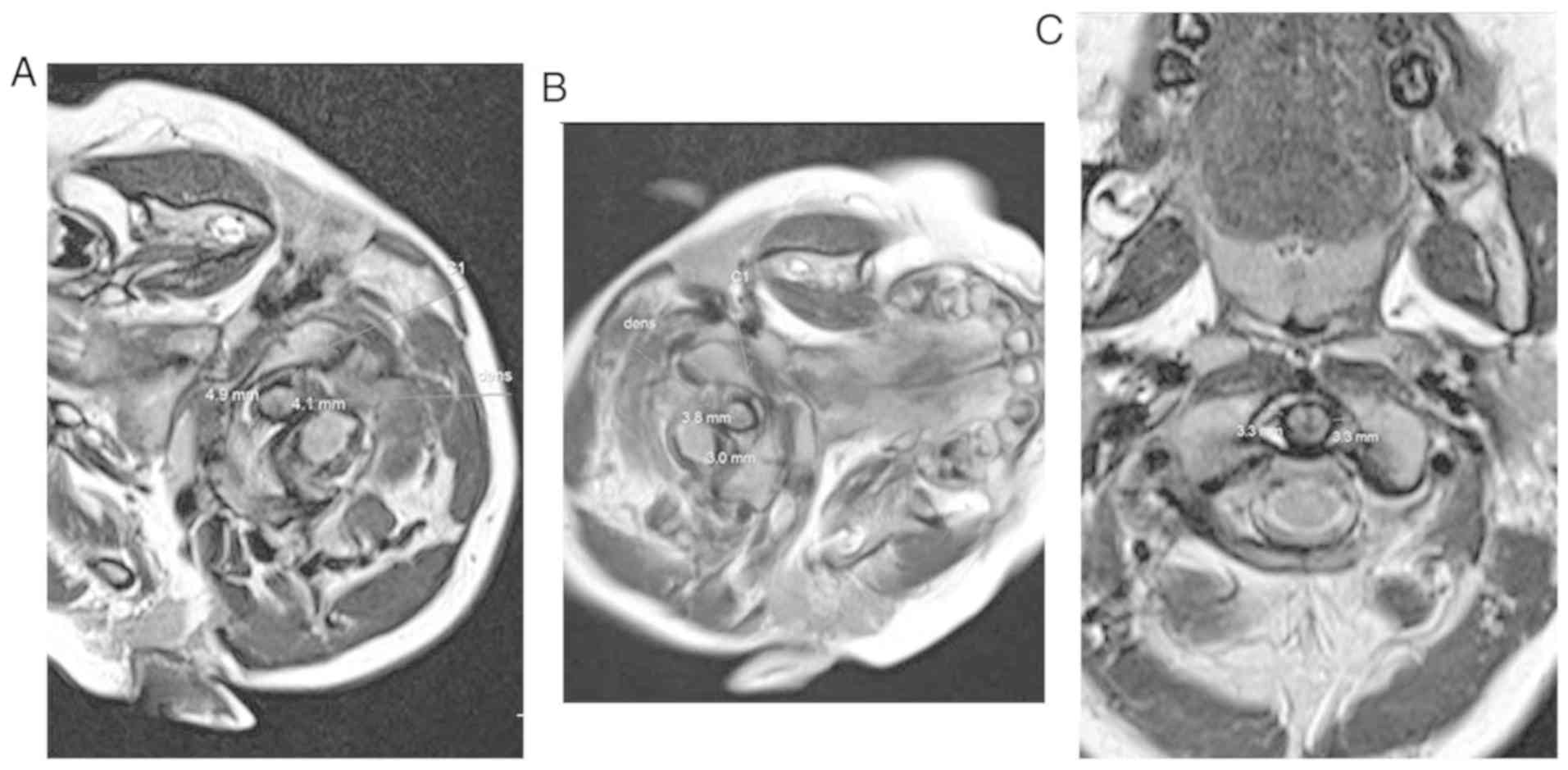
(JS) under GA, and a T2-weighted sequence was obtained with the
head rotated maximally to the right. Axial traction of the head was
manually maintained during the manipulation. Subsequently, the head
was rotated maximally to the left in the primary malposition
direction and the interventional MRI sequence was repeated. A
pediatric radiologist experienced in childhood musculoskeletal
trauma (MP) reviewed all interventional MRI findings and C1-C2
fixation was determined to be reduced (Fig. 3). A clinician also had access to
images to determine the immediate result of the treatment. A
correct association between C1 and C2 remained stable despite
movements of the head. The head was immobilized using a rigid neck
collar (Aspen© Pediatric Collar, size 5; Aspen Medical
Products, Irvine, CA, USA) in a neutral position and prior to
awakening of the patient, one more interventional MRI scan was
performed to ensure maintenance of the reduction. No dynamic CT
scans were required, and clinical recovery was complete at the
6-month follow-up.
Imaging modalities in the current
literature
Among the published original studies reviewed, the
major modality for imaging AARF was CT, but plain radiographs,
3D-CT, dynamic CT and MRI were also used. A few comprehensive
review articles were published, usually in connection with case
reports, and 3D-CT and dynamic CT were regarded as the current
methods (17). None of the studies
reported on the use of interventional MRI as an elementary part of
orthopaedic treatment, in the same manner as dynamic CT. Dynamic CT
is classified as repeated static CT images during the reduction
manoeuvre, with the head turned in several positions, rather than
real-time CT-monitoring or CT fluoroscopy. Systematic analysis of
the literature was based on 28 original clinical studies and case
reports published on the subject including 207 patients in total
(4,14–40).
About half of the studies were retrospective patient series, mostly
with just a few patients, while 13 were case reports. A comparison
of the features of the studies is provided in Table I.
Discussion
A normal cervical spine allows for a great range of
motion and most of the rotational torsion occurs at the
atlantoaxial joint. When a patient presents with acutely diminished
rotational movement, numerous different etiologies are possible,
but fixed rotation of the atlantoaxial joint should be considered.
Atlantoaxial subluxation remains a rare pediatric orthopedic
condition, but it may result in permanent dysfunction of the C1-C2
joint, with a requirement for surgical fixation. When the condition
is suspected (beyond benign torticollis), expedited diagnosis and
treatment are crucial to minimize long-term sequelae (41).
Due to the complex structure of the first and second
vertebrae of the cervical spine, it is challenging for radiologists
and clinicians to interpret plain radiographs in acute conditions.
These vertebrae are unique compared with the rest of the spinal
column, and their anatomy allows for wide rotational motion. The C1
vertebra has no vertebral body per se. For that reason, in
the case of pediatric patients with suspected AARF, CT is the
current means to investigate potential unilateral facet subluxation
and anterior displacement between the arch of C1 and the dens
(42). However, given that dynamic
CT with ionizing radiation exposure and poor soft-tissue resolution
is not optimal in young pediatric patients, interventional MRI was
used in the present study as the primary imaging modality in the
orthopaedic treatment of a patient with low-grade AARF to monitor
reduction performed under GA. The interventional MRI method was
proven to be feasible for investigating AARF and ensuring that
reduction is achieved during the procedure. This orthopedic
technique, performed using interventional MRI, was further analyzed
in the light of the published literature. A systematic and
comprehensive literature search was performed to determine the
current means of practice in AARF. The literature search was
performed using an appropriate search strategy in two different
international databases: PubMed and Google Scholar. The reference
lists of all relevant articles were reviewed in order to identify
any studies not identified in the above searches. In the studies
finally included, a considerable number of patients (n=207)
suffering the rare condition were analyzed. Several different
investigation methods were reported in these studies. CT and/or
dynamic CT were used in 24 out of 28 studies and it is also the
recommended method in certain handbooks (43). On the other hand, conventional MRI
was used for evaluating AARF in several articles included in this
literature review (n=9/28 of the articles; Table I). However, none of these previous
studies appeared to use interventional MRI as a method for testing
and assessment of reduction.
The present study was based on a radiation-free
intervention for treating AARF in pediatric patients. A limitation
of the present study was that only one case was reported and not a
large cohort of patients. There was no plan for a prospective trial
and no prior ethics board approval was obtained. However, the
procedure was considered to be safer than conventional dynamic CT
and therefore, no ethics board approval was required. Avoiding
ionizing radiation is preferred, if alternative methods are
available. A considerable amount of radiation exposure is averted
when MRI is used instead of CT. Diagnostic CT was performed
initially to exclude bone fractures; closed manual reduction of
concomitant AARF is not recommended in fracture cases, but open
surgical fixation is favored. The present study does not suggest
using interventional MRI in treating syndromic patients due to
potential anaesthetical challenges, with the shorter treatment time
of dynamic CT preferred. Furthermore, the treatment was scheduled
as urgent, as delayed reduction may lead to poor outcomes, and
timely treatment was considered necessary. The present study
reported on an encouraging approach for low-stage AARF treatment
with interventional MRI demonstrated to be fit for purpose. The
present findings may lead to future improvements in the care of
pediatric patients suffering from acute AARF.
In conclusion, the present study demonstrated the
feasibility of interventional MRI in AARF treatment for a pediatric
patient. The preliminary results merit further investigation to
evaluate interventional MRI prior to it being considered the method
of choice for AARF diagnostics and treatment. Therefore, a larger
study involving randomization of patients between dynamic CT and
interventional MRI may be required.
Acknowledgements
The Emil Aaltonen foundation and Foundation of
Pediatric Research supported the present study.
Funding
No funding was received.
Availability of data and materials
The datasets, including closer clinical
characteristics used during the present study, are available from
the corresponding author on reasonable request.
Authors' contributions
JH and JS drafted, wrote and revised the manuscript
for submission. MP, NS, WS and RBS drafted and revised the
manuscript. All authors have contributed in the study protocol and
to the initiative in reporting the issue. All authors read and
approved the final manuscript.
Ethical approval and consent to
participate
Not applicable.
Patient consent for publication
The legal guardian of the patient provided informed
consent for the publication of this didactic case with the patient
not identifiable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Maheshwaran S, Sgouros S, Jeyapalan K,
Chapman S, Chandy J and Flint G: Imaging of childhood torticollis
due to atlanto-axial rotatory fixation. Child Nerv Sys. 11:667–671.
1995. View Article : Google Scholar
|
|
2
|
Fielding JW and Hawkins RJ: Atlanto-axial
rotatory fixation. (Fixed rotatory subluxation of the atlanto-axial
joint). J Bone Joint Surg Am. 59:37–44. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schwarz N: The fate of missed
atlanto-axial rotatory subluxation in children. Arch Orthop Trauma
Surg. 117:288–289. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tauchi R, Imagama S, Kanemura T, Yoshihara
H, Sato K, Deguchi M, Kamiya M and Ishiguro N: The treatment of
refractory atlanto-axial rotatory fixation using a halo vest:
Results of a case series involving seven children. J Bone Joint
Surg Br. 93:1084–1087. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Osiro S, Tiwari KJ, Matusz P, Gielecki J,
Tubbs RS and Loukas M: Grisel's syndrome: A comprehensive review
with focus on pathogenesis, natural history, and current treatment
options. Child Nerv Syst. 28:821–825. 2012. View Article : Google Scholar
|
|
6
|
Hicazi A, Acaroglu E, Alanay A, Yazici M
and Surat A: Atlantoaxial rotatory fixation-subluxation revisited:
A computed tomographic analysis of acute torticollis in pediatric
patients. Spine (Phila Pa 1976). 27:2771–2775. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Alanay A, Hicazi A, Acaroglu E, Yazici M,
Aksoy C, Cila A, Akalan N and Surat A: Reliability and necessity of
dynamic computerized tomography in diagnosis of atlantoaxial
rotatory subluxation. J Pediatr Orthop. 22:763–765. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Johnson DP and Fergusson CM: Early
diagnosis of atlanto-axial rotatory fixation. J Bone Joint Surg Br.
68:698–701. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Haque S, Bilal Shafi BB and Kaleem M:
Imaging of torticollis in children. Radiographics. 32:557–571.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pang D: Atlantoaxial rotatory fixation.
Neurosurgery. 66 (Suppl 3):S161–S183. 2010. View Article : Google Scholar
|
|
11
|
Nicholson P, Higgins T, Forgarty E, Moore
D and Dowling F: Three-dimensional spiral CT scanning in children
with acute torticollis. Int Orthop. 23:47–50. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dagtekin A, Avci E, Kara E, Uzmansel D,
Dagtekin O, Koseoglu A, Talas D and Bagdatoglu C: Posterior cranial
fossa morphometry in symptomatic adult Chiari I malformation
patients: Comparative clinical and anatomical study. Clin Neurol
Neurosurg. 113:399–403. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
McGuire KJ, Silber J, Flynn JM, Levine M
and Dormans JP: Torticollis in children: Can dynamic computed
tomography help determine severity and treatment. J Pediatr Orthop.
22:766–770. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pang D and Li V: Atlantoaxial rotatory
fixation: Part 2-new diagnostic paradigm and a new classification
based on motion analysis using computed tomographic imaging.
Neurosurgery. 57:941–953. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Subach BR, McLaughlin MR, Albright AL and
Pollack IF: Current management of pediatric atlantoaxial rotatory
subluxation. Spine (Phila Pa 1976). 23:2174–2179. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Maile S and Slongo T: Atlantoaxial
rotatory subluxation: Realignment and discharge within 48 h. Eur J
Emerg Med. 14:167–169. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Barcelos AC, Patriota GC and Netto AU:
Nontraumatic atlantoaxial rotatory subluxation: Grisel syndrome.
Case report and literature review. Global Spine J. 4:179–186. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Beier AD, Vachhrajani S, Bayerl SH,
Aguilar CY, Lamberti-Pasculli M and Drake JM: Rotatory subluxation:
Experience from the hospital for sick children. J Neurosurg
Pediatr. 9:144–148. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mihara H, Onari K, Hachiya M, Toguchi A
and Yamada K: Follow-up study of conservative treatment for
atlantoaxial rotatory displacement. J Spinal Disord. 14:494–499.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mezue W, Taha Z and Bashir E: Fever and
acquired torticollis in hospitalized children. J Laryngol Otol.
116:280–284. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ciftdemir M, Copuroğlu C, Ozcan M, Ulusam
AO and Yalnız E: Non-operative treatment in children and
adolescents with atlantoaxial rotatory subluxation. Balkan Med J.
29:277–280. 2012.PubMed/NCBI
|
|
22
|
Deichmueller C and Welkoborsky H: Grisel's
syndrome-a rare complication following ‘small’ operations and
infections in the ENT region. Eur Arch Otorhinolaryngol.
267:1467–1473. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lee SC, Lui TN and Lee ST: Atlantoaxial
rotatory subluxation in skeletally immature patients. Br J
Neurosurg. 16:154–157. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rahimi SY, Stevens EA, Yeh DJ, Flannery
AM, Choudhri HF and Lee MR: Treatment of atlantoaxial instability
in pediatric patients. Neurosurg Focus. 15:ECP12003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Been HD, Kerkhoffs GM and Maas M:
Suspected atlantoaxial rotatory fixation-subluxation: The value of
multidetector computed tomography scanning under general
anesthesia. Spine (Phila Pa 1976). 32:E163–E167. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fernández Cornejo VJ, Martínez-Lage JF,
Piqueras C, Gelabert A and Poza M: Inflammatory atlanto-axial
subluxation (Grisel's syndrome) in children: Clinical diagnosis and
management. Childs Nerv Syst. 19:342–347. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Holcomb JD, Jaffe DM, Greinwald JH Jr,
Bauman NM and Smith RJ: Nontraumatic atlantoaxial rotary
subluxation in the pediatric otolaryngology patient: A report of
four cases. Ann Otol Rhinol Laryngol. 110:1137–1140. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Martinez-Lage J, Martinez Perez M,
Fernandez Cornejo V and Poza M: Atlanto-axial rotatory subluxation
in children: Early management. Acta Neurochir (Wien).
143:1223–1228. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ortiz GL, Pratts I and Ramos E: Grisel's
syndrome: An unusual cause of torticollis. J Pediatr Rehabil Med:.
6:175–180. 2013.PubMed/NCBI
|
|
30
|
Muñiz AE and Belfer RA: Atlantoaxial
rotary subluxation in children. Pediatr Emerg Care. 15:25–29. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Meek M, Hermens R and Robinson P: La
maladie de Grisel: Spontaneous atlantoaxial subluxation. Cleft
Palate Craniofac J. 38:268–270. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Galer C, Holbrook E, Treves J and Leopold
D: Grisel's syndrome: A case report and review of the literature.
Int J Pediatr Otorhinolaryngol. 69:1689–1692. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sobolewski BA, Mittiga MR and Reed JL:
Atlantoaxial rotary subluxation after minor trauma. Pediatr Emerg
Care. 24:852–856. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Pilge H, Prodinger PM, Bürklein D,
Holzapfel BM and Lauen J: Nontraumatic subluxation of the
atlanto-axial joint as rare form of acquired torticollis: Diagnosis
and clinical features of the Grisel's syndrome. Spine (Phila Pa
1976). 36:E747–E751. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Wurm G, Aichholzer M and Nussbaumer K:
Acquired torticollis due to Grisel's syndrome: Case report and
follow-up of non-traumatic atlantoaxial rotatory subluxation.
Neuropediatrics. 35:134–138. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Missori P, Miscusi M, Paolini S, DiBiasi
C, Finocchi V, Peschillo S and Delfini R: A C1-2 locked facet in a
child with atlantoaxial rotatory fixation: Case report. J
Neurosurg. 103 (Suppl 6):S563–S566. 2005.
|
|
37
|
Gourin CG, Kaper B, Abdu WA and Donegan
JO: Nontraumatic atlanto-axial subluxation after retropharyngeal
cellulitis: Grisel's syndrome. Am J Otolaryngol. 23:60–65. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Park SH, Park SH and Lee SH: Grisel
syndrome: Pathophysiological evidence from magnetic resonance
imaging findings. Ann Rehabil Med. 37:713–716. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Sia KJ, Tang IP, Kong CK and Nasriah A:
Grisel's syndrome: A rare complication of tonsillectomy. J Laryngol
Otol. 126:529–531. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Tsai SW and Chou CS: A case report of
manipulation under anesthesia of posttraumatic type II
occipital-atlantoaxial rotatory subluxation in a 4-year-old girl. J
Manipulative Physiol Ther. 28:352–355. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Pang D and Li V: Atlantoaxial rotatory
fixation: Part 3-a prospective study of the clinical manifestation,
diagnosis, management, and outcome of children with alantoaxial
rotatory fixation. Neurosurgery. 57:954–972. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Neal KM and Mohamed AS: Atlantoaxial
rotatory subluxation in children. J Am Acad Orthop Surg.
23:382–392. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Li V and Pang D: Atlantoaxial rotatory
fixation. Pang D.: Disorders of the Pediatric Spine (New York).
Raven Press. 531–553. 1995.
|