Introduction
The increase in the aging population has led to a
rise in the incidence of osteoarthritis (OA), which is accompanied
by a high economic burden on the whole society. OA is the most
common type of degenerative arthritis among individuals from
different countries; also, since it progresses slowly, it is not
detected and diagnosed at the early stage, causing a delay of
treatment and a limitation of its efficacy (1). OA frequently occurs in active joints,
including the knee and hip. According to epidemiological studies,
the incidence of individuals >55 years of age suffering from OA
is 44–70%, and 10% of patients experience pain in the joints, along
with reduced muscle strength and decline in joint stability and
mobility, which in turn results in walking difficulties and
severely affects daily life (2–4).
Typically, OA affects large weight-bearing joints, particularly the
knees, where the disease is disabling, as the knees participate in
several basic activities, including standing up from a seated
position, climbing, walking and running (5). Knee OA (KOA) has various clinical
symptoms, including pain associated with muscles and tendons, which
may decrease the range of motion, crepitus with movement and joint
effusion in the knee. Reportedly, the incidence of KOA among
individuals >60 years of age is 50% and that of individuals aged
>75 years is ~80% (6).
In recent years, there has been a growing interest
in shockwave treatment for orthopedic diseases, including KOA.
Several musculoskeletal diseases have been treated with shockwave
therapy (7). The effect of the
therapy includes pain relief, improvement of joint movement and
prevention of the progression of avascular necrosis (8,9).
Shockwave treatment has several advantages, including
non-invasiveness, low complication rate, no hospitalization and low
cost as compared to other approaches. Accordingly, shockwave
treatment is beneficial at the specific stage when surgery was
selected as the approach for several associated diseases (10,11).
Extracorporeal shockwave therapy (ESWT) has been increasingly used
in patients suffering from KOA (12–14), and
in clinical trials, ESWT was compared with physical therapy or
placebo. The outcome indicators included visual analog scale (VAS)
score, range of motion (ROM), Lequesne index (LI) and Western
Ontario and McMaster Universities osteoarthritis index (WOMAC). A
majority of the studies indicated that ESWT offered better pain
relief than placebo. Conversely, the study by Imamura et al
(15) did not demonstrate any
statistically significant difference between ESWT and placebo
treatment in pain control on patients with severe KOA and disabling
pain. In addition, the results regarding other outcome measures
were different among various studies. Thus, the present
meta-analysis was performed to ascertain whether ESWT is superior
to physical or placebo therapy with regard to all outcome
indicators.
Materials and methods
Search strategy
The present meta-analysis was in accordance with the
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
guidelines for the meta-analysis of intervention trials (16).
The PubMed, Medline, Embase, Web of Science,
Research Gate and the Cochrane Library were searched for
comparative studies involving ESWT for patients with KOA published
until February 2019. The search terms were as follows:
‘Extracorporeal shockwave therapy’ OR ‘physical therapy’ OR
‘exercise therapy’ AND ‘osteoarthritis’ OR ‘knee osteoarthritis’ OR
‘knee arthritis’. The language of the publications was limited to
English. The title and abstract of the studies identified in the
search were reviewed to exclude irrelevant studies. The reference
lists of all eligible studies and relevant reviews were searched
manually for additional trials.
Inclusion criteria and study
selection
First, the studies comparing ESWT to physical
therapy or ESWT to placebo in patients suffering from KOA were
identified. The primary outcomes included the pain score and ROM,
while the secondary outcomes were the LI and WOMAC. Subsequently,
studies comparing ESWT and physical therapy in patients with KOA
were selected, in which the primary outcomes included the pain
score and ROM, while the secondary outcome was the WOMAC. Studies
that reported on at least one outcome measure were included, and
those without the outcome measures of interest were excluded.
Furthermore, studies that did not contain data that could be used
for analysis were excluded. Letters, comments, editorials and
practice guidelines were also excluded.
Data extraction and quality
assessment
The authors read all titles and abstracts that were
identified according to the eligibility criteria. The articles
meeting the inclusion criteria were reviewed in further detail.
Further discussion amongst the listed authors settled any
differences in order to reach a consensus. The authors used
standardized tables to extract data on patient characteristics
(age, sex, and so on), interventions, and outcomes in duplicate.
Other formats data [i.e., median, interquartile range] were
converted to mean ± standard deviation according to the Cochrane
Handbook (17). If there was no
report in digital format then data was extracted from the figures
published by manual measurement. If necessary, we contacted the
corresponding author to confirm the information fulfilled the
criteria described above.
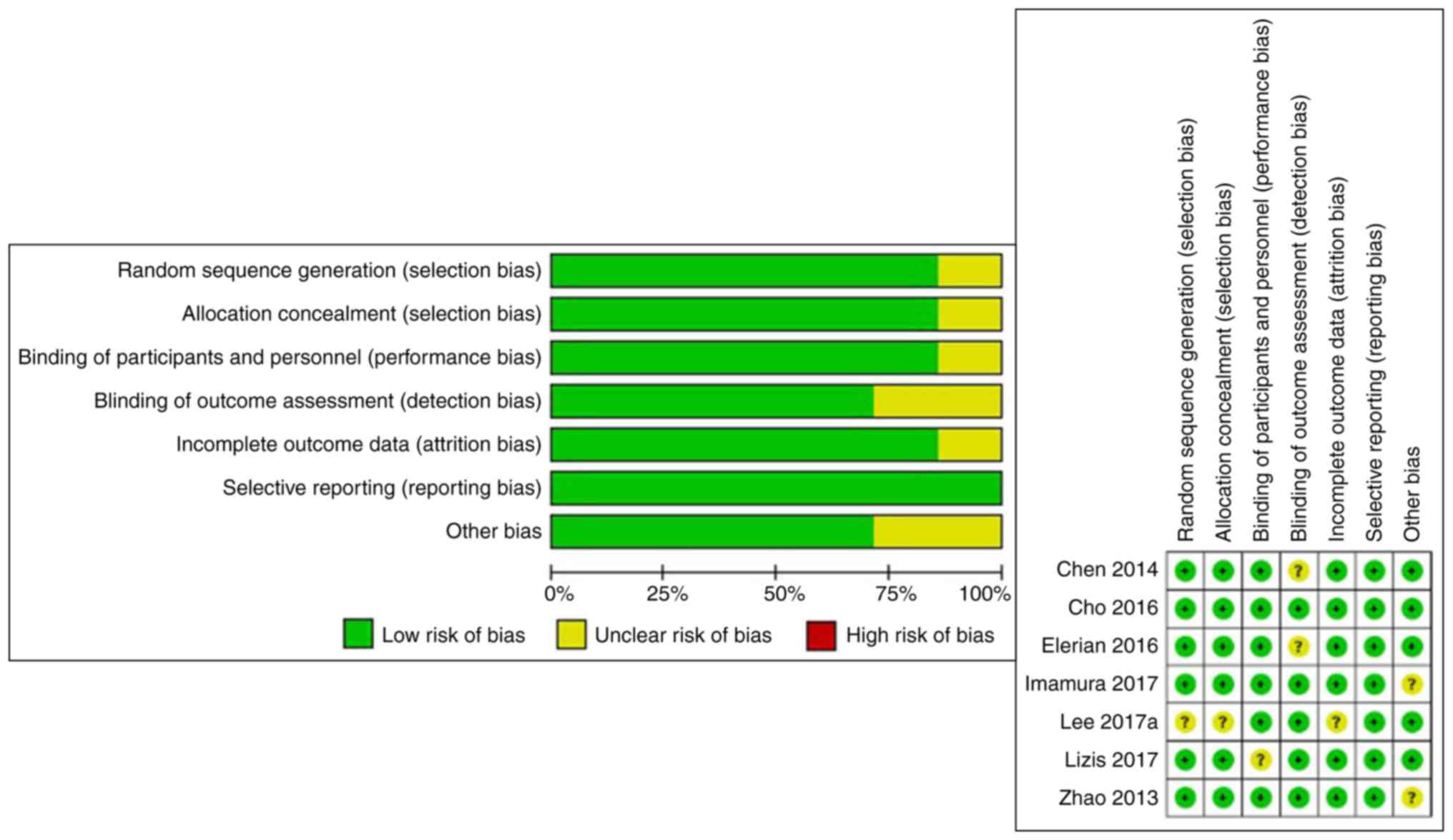
The risk of bias in each study was assessed. We
evaluated the rigor of the randomized process, the concealment of
treatment allocations, the process of blinding, data integrity and
the results according the Cochrane Collaboration Recommendations
(17). For the purpose of this
meta-analysis, randomization, concealment of treatment allocation,
and blinding and integrity were identified as key areas to
determine the risk of bias. In each study included, the risk of
bias was determined to be low when all key areas were fully
assessed. When one or more key areas are not clearly described, the
risk of bias is identified as unclear. When one or more key areas
are inadequate, the risk of bias is determined to be high. The
quality of evidence for each outcome was determined by considering
the risk of bias. The assessment of the risk of bias is shown in
Fig. 1.
All calculations were made using the mean difference
(MD) with a 95% CI that was calculated for continuous data using
RevMan v5.3 (16). The heterogeneity
among studies was estimated using I2 statistics and
substantial heterogeneity was considered if I2>50%.
The random-effects model was adopted for the meta-analysis of all
data. Because the random effect model could be used in all cases,
if the heterogeneity was small, then there would be no large
difference between random effect model and fixed effect model. When
the heterogeneity is large, only the random effect model could be
used therefore the random effect model was used in all cases.
P<0.05 was considered to indicate statistical significance.
Sensitivity analysis explored the impact of individual studies by
removing one study at a time in sequence.
Results
Search results
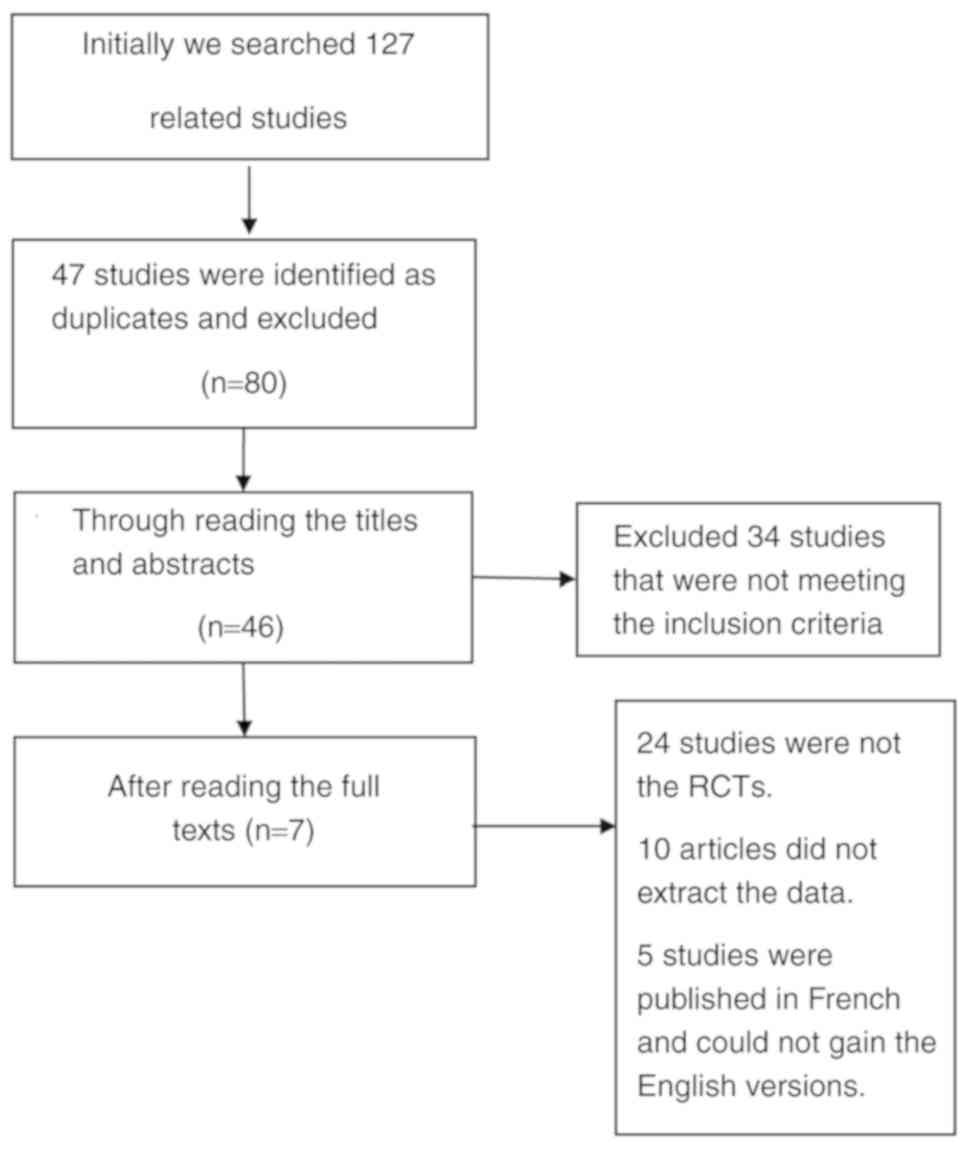
Initially, a total of 127 studies were retrieved,
among which 47 were identified as duplicates and were excluded. The
titles and abstracts of the remaining studies were read and 20
studies that did not fulfill the inclusion criteria were excluded.
Subsequently, 24 articles that were not randomized controlled
trials (RCTs) were also excluded (Fig.
2). Finally, seven studies comprising 366 patients were
included for data extraction and meta-analysis. Of these, 169
patients were in the ESWT group (15,18–23) and
140 in the placebo group (15,18–21) and
57 patients belonged to the physical therapy group (18,22,23).
Study characteristics and quality
assessment
The eligible studies included were published between
2013 and 2017. All of the studies were RCTs. The subjects in the
two groups had similar demographic data. All trials used ESWT,
except for the study by Imamura et al (15), which used radial ESWT. This may have
led to heterogeneity in data analysis. In the ESWT group, all
patients underwent treatment at least once per week and the total
number of sessions exceeded 3 times. In the placebo group, the
patients received the same number of impulses of sham stimulation
with an energy of 0 on the same area so that they did not realize
they were not treated. In the physical therapy group, participants
performed various exercises, including stretching, global
flexion-extension of the lower limb and strengthening. However, not
all studies assessed the same indicators. In the present
meta-analysis, the outcomes of muscle peak torques and the modified
Barthel index were not analyzed owing to insufficient data.
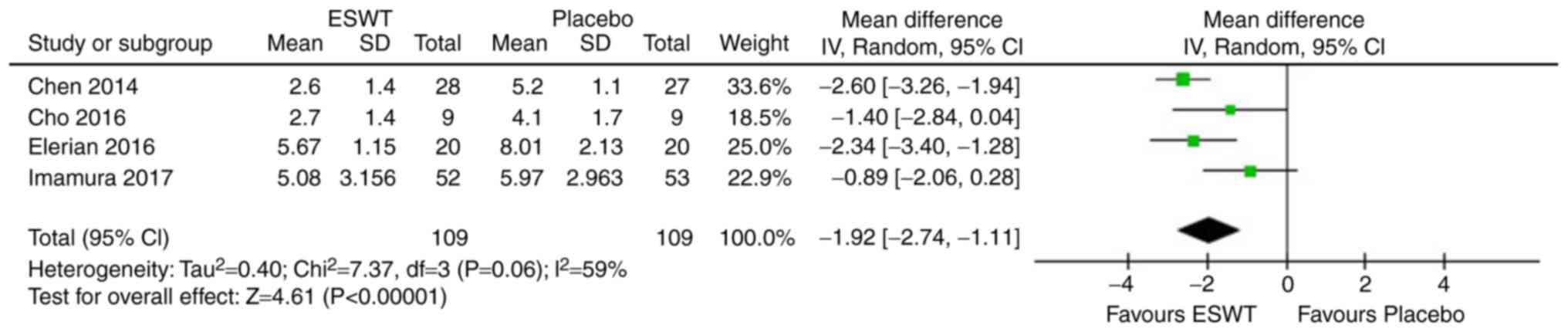
Meta-analysis of ESWT vs. placebo
A total of four studies (15,18–20)
involving 218 patients reported on the VAS score around 4 weeks
following completion of therapy. The statistical heterogeneity
between the studies was high as evaluated by a random-effects model
(P=0.06, I2=59%; Fig. 3).
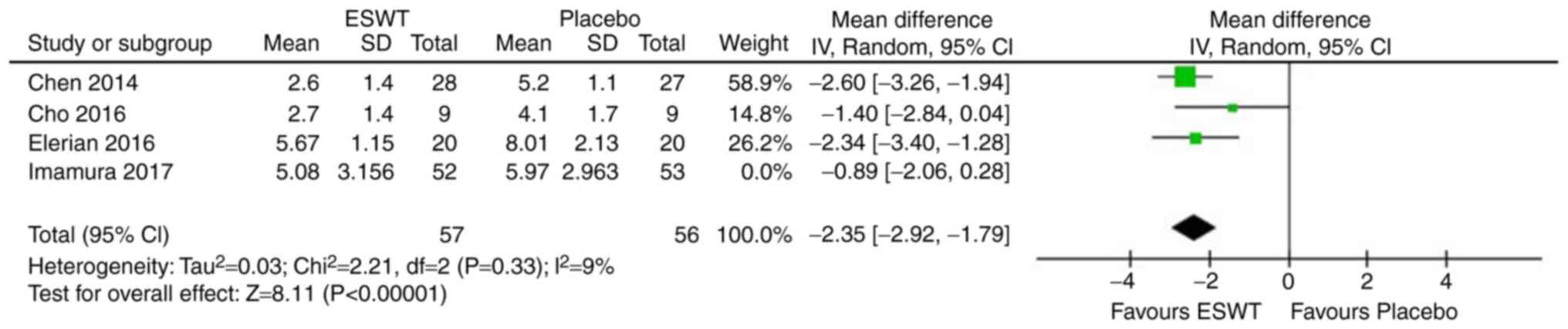
However, after the fourth study was removed, the statistical
heterogeneity of the remaining three studies was significantly
reduced (P=0.33, I2=9%; Fig.
4). Meta-analysis of the data revealed that the VAS scores of
ESTW patients were significantly lower than those in the
placebo-treated patients after therapy after 1 month (MD=−2.35, 95%
CI: −2.92 to −1.79, P<0.00001).
A total of two studies (18,20)
including 95 patients reported on the ROM of knees after therapy
for 1 month. The statistical heterogeneity between the studies was
low as assessed by a random-effects model (P=0.20,
I2=38%). The increase in the ROM scores in the ESWT
group was significantly higher than that in the placebo group after
treatment (MD=17.58, 95% CI: 12.88–22.28, P<0.00001; Fig. 5).
The LI after treatment for 1 month was assessed by
two studies (18,21) comprising 116 patients. The
statistical heterogeneity between the studies was reliable, as
assessed by a random-effects model (P=0.27, I2=18%). The
ESWT group scored significantly lower than the placebo group
(MD=−3.06, 95% CI: −3.90 to −2.21, P<0.00001; Fig. 6).
Meta-analysis of ESWT vs. physical
therapy
A total of two studies (18,22)
involving 75 patients reported on the pain score around 5 weeks
following completion of therapy. The statistical heterogeneity
between the studies was considerable according to the
random-effects model (P=0.13, I2=56%). The VAS scores of
the ESTW patients were significantly lower than of those with
physical therapy for ~1 month (MD=−1.98, 95% CI: −2.93 to −1.03,
P<0.00001; Fig. 7).
The ROM of knees around 5 weeks following completion
of therapy was reported by two studies (18,23)
including 95 patients. The statistical heterogeneity between the
studies was acceptable using a random-effects model (P=0.20,
I2=39%). The increase in the ROM scores during the
treatment in the ESWT group was significantly higher than that in
the physical therapy group (MD=11.69, 95% CI: 6.40–16.98,
P<0.00001; Fig. 8).
Furthermore, two studies (22,23)
comprising 60 patients described the WOMAC around 4 weeks following
completion of therapy. The statistical heterogeneity between the
studies was low according to analysis with the random-effects model
(P=0.77, I2=0%). The WOMAC in the ESWT patients
exhibited a greater decrease than that in the physical therapy
patients after treatment (MD=−15.38, 95% CI: −18.87 to −11.89,
P<0.00001; Fig. 9).
Discussion
To the best of our knowledge, the present study was
the first meta-analysis to investigate the efficacy and safety of
ESWT as compared to physical therapy or placebo for the treatment
of KOA. A series of RCTs on shockwave therapy has been performed
for OA. In the ESWT group vs. placebo group analysis, the outcome
indicators included were VAS, ROM and LI. Concerning pain control,
one of the studies (15) indicated
that shockwaves were not different from placebo in relieving severe
pain for KOA. However, the combined analysis indicated that the
shockwave group was significantly better than the placebo group,
which was consistent with the individual studies. Furthermore, when
the four studies were analyzed simultaneously, the heterogeneity
was high (P=0.06, I2=59%). When the fourth study
(15) was removed, the heterogeneity
became reliable (P=0.33, I2=9%). Thus, it may be
concluded that the heterogeneity of outcome indicators in this
group originates from the last study (15). In addition, Imamura et al
(15) used radial ESWT, which
differs from shockwave equipment used in the other research
studies. Furthermore, the patients selected were females and the
pain was generally severe. The VAS score reached 7 points prior to
the treatment whilst other studies reached around 5 points and this
may have been the source of heterogeneity. Two studies (18,20)
assessed ROM and LI. Of note, the comprehensive analysis
demonstrated that the patients in the shockwave group had a
significantly greater ROM than the placebo group after treatment,
and also, the LI was significantly reduced with acceptable
heterogeneity, and hence, the result was reliable. However, the
limited number of studies included in the present meta-analysis
weakened the strength of the results regarding certain outcome
measures such as ROM which only used 2 datasets, thereby
necessitating the substantiation of the future results by a large
number of RCTs.
In the ESWT group vs. physical therapy group
analysis, the outcome indicators included the VAS, ROM and WOMAC
scores. In terms of pain relief, the shockwave was significantly
superior to physical exercise, albeit the heterogeneity in the two
groups was slightly high (P=0.13, I2=56%). Thus, the
reliability of the results was limited and hence, domestic studies
from China were screened, revealing that the pain relief effect of
ESWT was better than that of pure physical exercise therapy
(3). Therefore, the small sample
size may be the cause of heterogeneity. Furthermore, there is a
similar meta-analysis (7), which
produced similar results, with future clinical studies likely to
confirm the results of the present study. Of note, in the ESWT
group, the ROM (18,23) and WOMAC (22,23)
score were significantly better than those in the physical therapy
group and no obvious heterogeneity was detected in the two groups
in the present study.
Of note, the present meta-analysis has several
limitations. First, the number of relevant RCTs on the treatment of
osteoarthritis was relatively low and the quality of the domestic
studies was unreliable. Also, only studies published in English
language were included, and hence, relevant studies published in
other languages may have been missed. Furthermore, only seven
studies were included and the sample size of each study was small,
which limited the statistical power of the present meta-analysis.
In addition, due to the limitation of the number of included
studies, the therapeutic effects of the shockwaves of different
energies were not analyzed, and all were combined into one
shockwave group, which may have led to deviations of the results.
Furthermore, the severity of OA prior to treatment may have also
led to high heterogeneity and affected the reliability of the
results. Finally, due to the limited literature, it was not
possible to evaluate publication bias or to analyze functional
outcomes e.g. post-operative quadriceps strength measures and the
treatment costs due to insufficient data. Therefore, high-quality
and large-scale clinical trials and systemic reviews are essential
to confirm these results in the future.
In conclusion, in the treatment of KOA, the effects
of ESWT are superior to those of placebo and physical therapy.
Besides the pain relief, ESWT increases the mobility of the knee
joint and may reduce the LI and WOMAC score. The evidence supported
the selection of shock wave for the treatment of KOA patients;
however, due to the lack of relevant high-quality literature and
similar previous meta-analyses, and the fact that certain studies
did not utilize a blinding method, the results require to be
further substantiated.
Acknowledgements
Not applicable.
Funding
This study was supported by the Beijing Natural
Science Foundation (grant no. 7182146), the Capital's Funds for
Health Improvement and Research (grant no. CFH2018-4-40611),
Beijing Municipal Science & Technology Commission (grant no.
Z181100001718058), the Fundamental Research Funds for the Central
Universities (grant no. 3332018168), Graduate Innovation Foundation
of Peking Union Medical College (grant no. 2017-1002-2-26) and the
National Natural Science Foundation of China (grant nos. 81672236,
81802224 and 81871830).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
WS and FG conceived and designed the study. TL, TZ
and JM collected the data and performed the literature search. All
authors were involved in writing the manuscript. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ESWT
|
extracorporeal shockwave therapy
|
|
OA
|
osteoarthritis
|
|
KOA
|
knee OA
|
|
ROM
|
range of motion
|
|
VAS
|
visual analogue score
|
|
LI
|
Lequesne index
|
|
WOMAC
|
Western Ontario and McMaster
Universities osteoarthritis index
|
|
RCT
|
randomized controlled trial
|
|
MD
|
mean difference
|
|
CI
|
confidence interval
|
|
SD
|
standard deviation
|
References
|
1
|
Ji Q, Wang P and He C: Extracorporeal
shockwave therapy as a novel and potential treatment for
degenerative cartilage and bone disease: Osteoarthritis. A
qualitative analysis of the literature. Prog Biophys Mol Biol.
121:255–265. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hsu SL, Cheng JH, Wang CJ, Ko JY and Hsu
CH: Extracorporeal shockwave therapy enhances expression of Pdia-3
which is a key factor of the 1α,25-dihydroxyvitamin D 3 rapid
membrane signaling pathway in treatment of early osteoarthritis of
the knee. Int J Med Sci. 14:1220–1230. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Li JW, Zheng SJ, Zhang JC, Huang JJ and
Liu XG: Effect of acupuncture plus different frequency shock-wave
interventions on pain reactions and motor function in knee
osteoarthritis patients. Zhen Ci Yan Jiu. 40:300–303. 2015.(In
Chinese). PubMed/NCBI
|
|
4
|
Pu W, Yujing Z, Xiaofei W, Xiaotian Y,
Chengqi H and Chuan L: Effects of extracorporeal shock wave therapy
on cartilage protection and subchondral bone remodeling in rabbits
osteoarthritis induced by ACLT. Ann Phys Rehabil Med. 57:e372014.
View Article : Google Scholar
|
|
5
|
Maricar N, Callaghan MJ, Parkes MJ, Felson
DT and O'Neill TW: Clinical assessment of effusion in knee
osteoarthritis-A systematic review. Semin Arthritis Rheum.
45:556–563. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kim JH, Kim JY, Choi CM, Lee JK, Kee HS,
Jung KI and Yoon SR: The dose-related effects of extracorporeal
shock wave therapy for knee osteoarthritis. Ann Rehabil Med.
39:616–623. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liao CD, Tsauo JY, Liou TH, Chen HC and
Huang SW: Clinical efficacy of extracorporeal shockwave therapy for
knee osteoarthritis: A systematic review and meta-regression of
randomized controlled trials. Clin Rehabil.
8:2692155198469422019.
|
|
8
|
Hou X.D..Liu H.B..Liu K.M.: Effects of
extracorporeal shock wave therapy on interleukin-1beta and matrix
metalloproteinase-13 expression in rabbits with knee
osteoarthritis. Zhong Guo Zu Zhi Gong Cheng Yan Jiu Za Zhi.
18:2397–2402. 2014.(In Chinese).
|
|
9
|
Zhao Z, Ji H, Jing R, Liu C, Wang M, Zhai
L, Bai X and Xing G: Extracorporeal shock-wave therapy reduces
progression of knee osteoarthritis in rabbits by reducing nitric
oxide level and chondrocyte apoptosis. Arch Orthop Trauma Surg.
132:1547–1553. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yoon SR and Kim JH: Effect of
extracorporeal shock wave therapy on knee osteoarthritis. Ann Phys
Rehabil Med. 57:e37–e38. 2014. View Article : Google Scholar
|
|
11
|
Wang P, Liu C, Yang XT, Wei XF, Zhou YJ,
Yang L and He CQ: Effect of extracorporeal shock wave therapy on
cartilage and subchondral bone remodeling in rabbits with
ACLT-induced osteoarthritis. Sichuan Da Xue Xue Bao Yi Xue Ban.
45:120–125. 2014.(In Chinese). PubMed/NCBI
|
|
12
|
Frisbie DD, Kawcak CE and McIlwraith CW:
Evaluation of the effect of extracorporeal shock wave treatment on
experimentally induced osteoarthritis in middle carpal joints of
horses. Am J Vet Res. 70:449–454. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ochiai N, Ohtori S, Sasho T, Nakagawa K,
Takahashi K, Takahashi N, Murata R, Takahashi K, Moriya H, Wada Y
and Saisu T: Extracorporeal shock wave therapy improves motor
dysfunction and pain originating from knee osteoarthritis in rats.
Osteoarthritis Cartilage. 15:1093–1096. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mueller M, Bockstahler B, Skalicky M,
Mlacnik E and Lorinson D: Effects of radial shockwave therapy on
the limb function of dogs with hip osteoarthritis. Vet Rec.
160:762–765. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Imamura M, Alamino S, Hsing WT, Alfieri
FM, Schmitz C and Battistella LR: Radial extracorporeal shock wave
therapy for disabling pain due to severe primary knee
osteoarthritis. J Rehabil Med. 49:54–62. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wright JG, Swiontkowski MF and Tolo VT:
Meta-analyses and systematic reviews: New guidelines for JBJS. J
Bone Joint Surg Am. 94:15372012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jokstad A: Cochrane collaboration
systematic reviews may be based on trials not approved by a
research ethics committee. Clin Exp Dent Res. 3:179–182. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chen TW, Lin CW, Lee CL, Chen CH, Chen YJ,
Lin TY and Huang MH: The efficacy of shock wave therapy in patients
with knee osteoarthritis and popliteal cyamella. Kaohsiung J Med
Sci. 30:362–370. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cho SJ, Yang JR, Yang HS and Yang HE:
Effects of extracorporeal shockwave therapy in chronic stroke
patients with knee osteoarthritis: A pilot study. Ann Rehabil Med.
40:862–870. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Elerian AE, Ewidea TMA and Ali N: Effect
of shock wave therapy versus corticosteroid injection in management
of knee osteoarthritis. Int J Physiother. 3:246–251. 2016.
View Article : Google Scholar
|
|
21
|
Zhao Z, Jing R, Shi Z, Zhao B, Ai Q and
Xing G: Efficacy of extracorporeal shockwave therapy for knee
osteoarthritis: A randomized controlled trial. J Surg Res.
185:661–666. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lee JH, Lee S, Choi S, Choi YH and Lee K:
The effects of extracorporeal shock wave therapy on the pain and
function of patients with degenerative knee arthritis. J Phys Ther
Sci. 29:536–538. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lizis P, Kobza W and Manko G:
Extracorporeal shockwave therapy vs. kinesiotherapy for
osteoarthritis of the knee: A pilot randomized controlled trial. J
Back Musculoskelet Rehabil. 30:1121–1128. 2017. View Article : Google Scholar : PubMed/NCBI
|