Introduction
The International Association for the Study of Pain,
describes pain as ‘an unpleasant sensory and emotional experience
associated with actual or potential tissue damage or described in
terms of such damage’ (1). A large
majority of patients undergoing surgery experience post-operative
pain, which is not only agonizing and distressing, but may also
contribute to complications and to a delayed recovery (2). Pain exacerbates stress responses, which
lead to increased tissue breakdown, coagulation and fluid
retention, and have deleterious effects on the recuperation of
patients (3).
Abdominal surgery is considered to be one of the
most painful surgical procedures (4). The site's proximity to the diaphragm
and extensive cross-innervations in the area multiply the
post-operative distress experienced by patients (5). Inadequate pain control in such
individuals can lead to impaired respiration, disrupted sleep, loss
of appetite, prolonged hospitalization, patient dissatisfaction and
increased treatment costs (4,6,7).
Pain management has been a subject of intense
research with a number of technological advancements striving to
achieve optimal pain control. Even with the advent of patient-
controlled analgesia, continuous intravenous infusion and the
intraspinal application of opioids, pain control remains a major
challenge (4). Post-operative
patients are under the constant supervision of nurses, who also are
responsible for assessing the need and type of pain relief
(3). While the administration of
analgesics is an important part of nursing practice,
non-pharmacological interventions for the reduction of
post-operative pain are slowly gaining popularity. Patient
education, massages, music, guided imagery and relaxation therapy
are being increasingly used by nurses in the post-operative setting
to achieve more effective pain relief (8).
Relaxation therapy has been shown to provide pain
relief by decreasing anxiety, lowering muscle tension and
distracting attention (9). While a
number of studies (4,7,9) have
described the beneficial effects of relaxation therapy for pain
relief in patients undergoing abdominal surgery, evidence in the
form of a systematic review and meta-analysis is lacking, at least
to the best of our knowledge. Therefore, the aim of this study was
to perform a systematic literature search and critically analyze
available evidence with the objective of assessing the efficacy of
relaxation techniques for pain relief in patients undergoing
abdominal surgery.
Data and methods
This systematic review of the literature was
conducted in line with the Preferred Reporting Items for Systematic
Reviews and Meta-analyses (PRISMA) statement (10) and guidelines of the Cochrane Handbook
for Systematic Reviews of Intervention (11). The study protocol was prepared prior
to the commencement of the study. The issue in question was the
effectiveness of relaxation techniques against post-operative pain
in patients undergoing abdominal surgery.
Eligibility criteria
We searched for studies evaluating the effects of
relaxation therapy in patients undergoing abdominal surgery. No
restrictions were placed on the type of relaxation technique and
the type of abdominal surgery. Controlled clinical trials (CCTs)
and randomized control trials (RCTs) studying the effects of
relaxation therapy on post-operative pain reduction in patients
undergoing abdominal surgery were included in this review. The
participants of the included studies needed to be >18 years of
age, had to have undergone surgery under general anesthesia or
spinal anesthesia and must have been hospitalized during the period
of the surgery for at least 48 h. Participants were not to have any
cognitive impairment and were not to have planned to undergo any
neurosurgery. Intervention had to include relaxation therapy with
muscle relaxation in the post-operative period. Outcome assessment
had to include pain scores measured on any scale, such as the
visual analogue scale (VAS) (3). The
studies excluded were the following: i) Studies combining
relaxation therapy with other psychological pain relief measures,
such as guided imagery; ii) studies in which relaxation therapy was
performed pre-operatively; and iii) studies which did not include
pain as an outcome variable. Additionally, non-English language
studies, studies on healthy volunteers and uncontrolled studies
were also excluded.
Search strategy
We searched the PubMed, Scopus, Cochrane Central
Register of Controlled Trials (CENTRAL) and Google Scholar
databases (first 100 results) electronically for articles published
up to May, 2019. The key words used in various combinations were:
Relaxation therapy [MeSH], relaxation techniques [MeSH],
progressive muscle relaxation [Free text], systematic relaxation
[Free text], Benson's relaxation [Free text], abdominal surgery
[Free text], surgery [MeSH], pain [MeSH], pain relief [MeSH],
abdominal pain [MeSH], nursing [MeSH] and nursing care [MeSH].
References of included studies and review articles were analysed
for the identification of any additional studies.
Collection of data and analysis
Two reviewers examined potentially eligible studies.
Following the removal of duplicates, studies were scrutinized by
their title and abstracts. Full-texts of selected articles were
then scanned for their inclusion in the review. Any differences in
opinion were resolved by discussion. The following data were
extracted from the included trials: Authors, publication year,
sample size, demographic data, relaxation technique, relaxation
protocol and outcomes assessed.
Evaluating risk of bias
The Cochrane Collaboration risk assessment tool for
RCTs was used for assessing the risk of bias (12). Seven criteria were evaluated for each
study: Random sequence generation, allocation concealment, blinding
of participants and personnel, blinding of outcome assessment,
incomplete outcome data, selective outcome reporting and other
biases. Studies were scored for each criteria as follows: Low risk
(score of 2), high risk (score of 0), or unclear risk of bias
(score of 1). Based on the scores awarded, individual studies were
grouped as low- (score 0–5), medium- (score 6–10), or high- (score
11–14) quality trials.
Statistical analysis
Studies were included in the meta-analysis only if
pain scores were reported as the means and standard deviation. The
results of the remaining studies were summarized in a narrative
form. Outcome data extracted were entered into Review Manager
[RevMan, version 5.3; Nordic Cochrane Centre (Cochrane
Collaboration), 2014] for quantitative analysis. the data of
different relaxation techniques were pooled for a sub-group
analysis. Considering the heterogeneity amongst studies, a
random-effects model was used to calculate the pooled effect size.
The standardized mean difference (SMD) with the 95% confidence
interval (CI) was used for combining pain data measured on
different scales. Heterogeneity was calculated using the
I2 statistic. I2 values of 25–50% represented
low, values of 50–75% medium and >75% represented substantial
heterogeneity.
Results
Search outcome
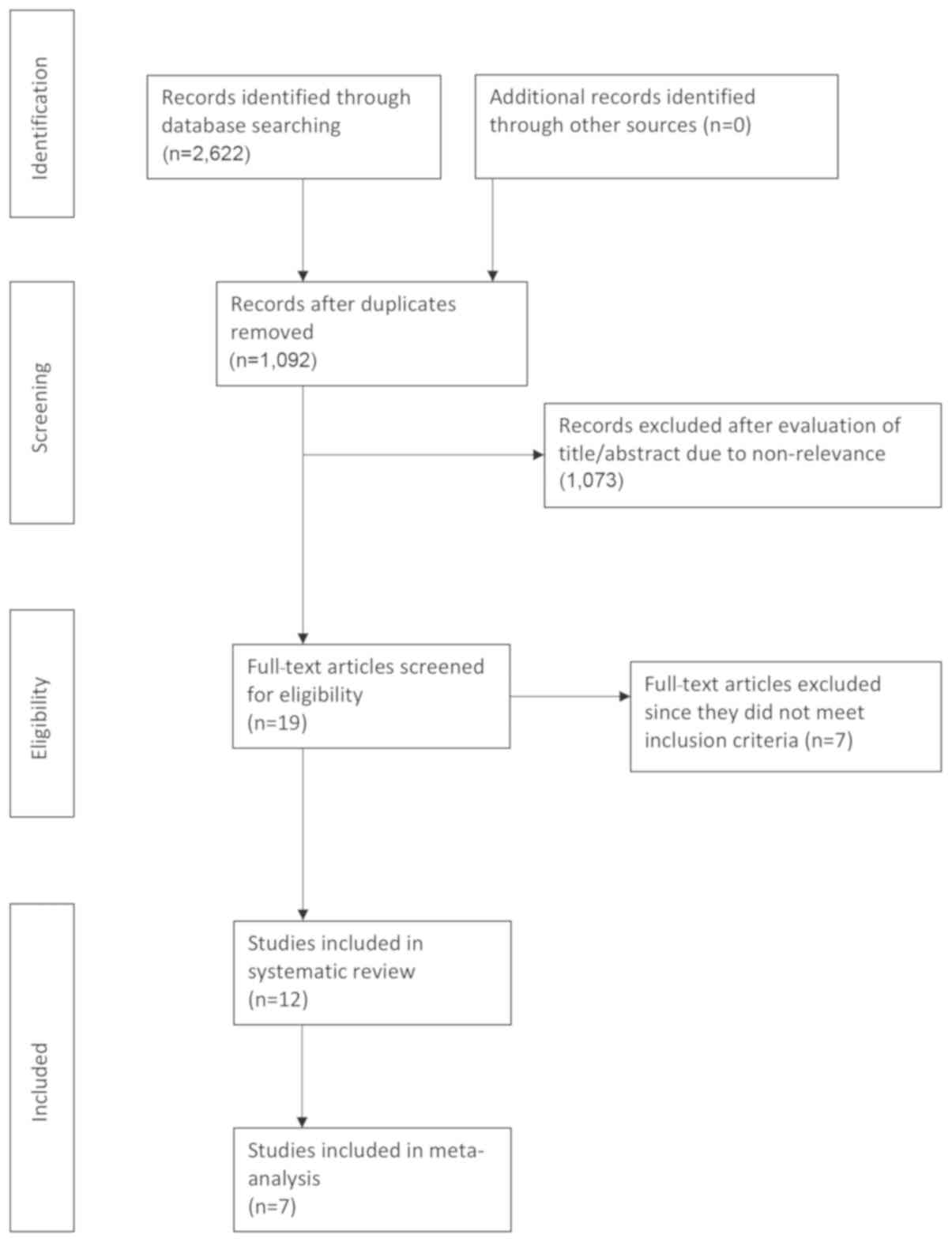
The search outcome of the review is presented in
Fig. 1. A total of 1,092 articles
were examined by their abstracts. We excluded a total of 1,072
studies as they were not relevant to the study. In total, 20
articles were analyzed by their full text. Seven studies were
excluded from the review (13–19). Two
studies did not include pain as an outcome measure (15,18), 1
did not include a control group (19), 1 was a duplicate publication
(13), the relaxation technique did
not include actual muscle relaxation in 1 study (17), 1 combined guided imagery with
relaxation therapy (16) and 1
administered relaxation therapy only pre-operatively (14). A total of 12 studies (2,4,7,9,20–27) were
included in the qualitative review and 7 trials (2,7,9,21,23,24,27)
were included in the meta-analysis.
Relaxation techniques
A total of 4 relaxation techniques were utilized in
the included studies, namely: The jaw relaxation technique,
Benson's relaxation technique, progressive muscle relaxation (PMR)
technique and systematic relaxation technique. The description of
each technique was as follows: i) The jaw relaxation technique was
carried out with patients dropping the lower jaw slightly as though
starting a small yawn. The tongue was kept quiet and resting at the
bottom of the mouth. The lips were to parted slightly, and the
patient was to breath slowly and rhythmically with a 3-rhythm
pattern (inhale, exhale and rest). Word formation was not advised
and the patient was advised to not think of any words (9,27). ii)
Benson's relaxation therapy involved deep relaxation of all
muscles, focusing on breathing and repeating any word to focus on
relaxation, and preventing the wandering of the individual's
attention (20,24). iii) PMR consisted of deep breathing
along with the systemic sequential tensing of the muscles (5–7 sec)
followed by relaxation (10–12 sec). The technique was repeated for
different muscle groups until the entire body was relaxed (21–23,25). iv)
Systematic relaxation differed from PMR as no tensing of the
muscles was carried out in this technique and focus was only placed
on sequentially relaxing individual groups of muscles (2,7,26).
Characteristics of included
studies
The details of the included studies are presented in
Table I. The sample sizes of the
included studies varied from a minimum of 17 patients per group to
a maximum of 130 patients. The studies included a combination of
patients undergoing gastrointestinal or gynecological surgical
procedures. PMR was the most commonly studied relaxation therapy
with 4 trials reporting its use (21–23,25).
Systematic relaxation was studied by 3 trials (2,7,26). There were 2 studies each for jaw
relaxation (9,27) and Benson's relaxation therapy
(20,24), and 1 trial (4) did not specify the type of relaxation
technique used. The relaxation technique were explained to the
interventional group pre-operatively in all studies and practiced
for use in the post-operative period. Considerable variation was
observed in the relaxation protocol used across studies. Relaxation
therapy was practiced at a specific time in all studies apart from
2. In the studies by Wilson (26)
and Levin et al (20),
relaxation was performed by the patients as and when required. Pain
scores were measured just after the completion of the relaxation
therapy in all studies, apart from 2. The study by Devmurari and
Nagrale (22) compared pain scores
after the completion of 5 days of PMR therapy, while the study by
Ismail and Elgzar (21) compared
pain scores after 2 days of therapy. In total, 10 of the 12
included studies demonstrated statistically significant pain relief
in the relaxation group as compared to controls (2,4,7,9,20,21,23,25–27). The
study by Solehati and Rustina (24)
utilizing Benson's relaxation technique found significant pain
relief in both the interventional and control group. The study by
Devmurari and Nagrale (22) reported
greater pain reduction in the PMR group; however, no statistical
analysis was carried out.
 | Table I.Characteristics of the included
studies. |
Table I.
Characteristics of the included
studies.
|
|
|
| No. of
participants |
|
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|---|
| Author/(Ref.),
year | Relaxation
technique | Surgery type | R | C | Age group | Sex | Relaxation
protocol | Time interval
between post-test and relaxation | Study
conclusion |
|---|
| Flaherty and
Fitzpatrick (27), 1978a | Jaw relaxation | Cholecystectomy,
herniorrhaphy, haemorrhoidectomy | 21 | 21 | 18–65 | M: 23 F: 19 | 6–8 h after
surgery, relaxation started just before patient ambulation (30 ft),
continued during and after ambulation. | Immediately | Significantly less
incisional pain, body distress and respiratory rate in relaxation
group. No difference in blood pressure and pulse rates. |
| Wilson (26), 1981 | Systematic
relaxation | Cholecystectomy,
hysterectomy | 17 | 18 | 42.3 10.7 | NS | Relaxation therapy
used by patients as and when desired for post-operative days 1, 2
and 3. | NS | Significantly
better hospital recovery in relaxation group |
|
|
|
|
|
|
|
| Data of 3 days
averaged and compared. | NS | Significantly less
pain in relaxation group. |
| Levin et al
(20), 1987 | Benson's
relaxation |
Cholecystectomy | 9 | 10 | 21–65 | F: 19 | Relaxation therapy
used by patients as and when desired. Data collected evening of
surgery and then twice daily for 2 days. |
| No difference in
number of analgesics consumed and length of hospital stay between 2
groups. |
| Good et al
(9), 1999a | Jaw relaxation | Gastro-intestinal,
gynaecological, exploratory, urinary | 130 | 120 | 20–70 | NS | On 1st
post-operative day, relaxation started 5 min prior to ambulation,
continued during and after ambulation for 10 min. One half tested
after ambulation other half tested at rest. Order reversed on 2nd
day. | 10 min | Significantly less
pain and distress in relaxationgroup. Reduced pulse rates and
respiratory rates in treatment group. |
| Roykulcharoen and
Good (2), 2004a | Systematic
relaxation | Gastrointestinal,
gynaecological, exploratory | 51 | 51 | 21–65 | M:18 F: 84 | Post-ambulation on
1st post-operative day, relaxation therapy given for 15 min. | Immediately | Significantly less
pain sensation and distress of pain in relaxation group. No change
in anxiety levels between the 2 groups and no difference in 6-h
opioid intake |
| Chandrababu
(25), 2012 | Progressive muscle
relaxation | NS | 20 | 20 | 18–60 | NS | On 1st
post-operative day, relaxation therapy performed for 20 min.
Repeated twice daily for 3 days. | 5 min | Significantly less
pain in relaxation group. No difference in respiration rate,
systolic blood pressure and diastolic blood pressure between the 2
groups. |
| Topcu and Findik
(4), 2012 | NS | NS | 60 | 60 | 48.38 NS | NS | On post-operative
days 1–4, relaxation therapy performed for 20 min. | Immediately | Significantly less
pain in relaxation group. |
| Rejeh et al
(7), 2013a | Systematic
relaxation | NS | 62 | 62 | 65–92 | M: 32 F: 92 | Relaxation therapy
repeated 3 times. Post-test measured after 15 min recovery
following ambulation. | 15 min, 1 h and 12
h | Significantly less
pain, anxiety and analgesic use in relaxation group. |
| Solehati and
Rustina (24), 2015 | Benson's
relaxation | Caesarean | 30 | 30 | NS | F: 60 | Relaxation therapy
performed 2 h after the operation, continued twice daily for 4
days. | Immediately | Significant pain
reduction seen in both relaxation and control groups |
| Devi and Saharia
(23), 2017a | Progressive muscle
relaxation | Appendicectomy,
cholecystectomy, hernioplasty, gastrectomy, gastro-jejunostomy | 20 | 20 | 20–40 | M: 20 F: 20 | For 3
post-operative days, relaxation therapy performed for 15 min. | 1h | Significantly less
pain in relaxation group |
| Devmurari and
Nagrale (22), 2018 | Progressive muscle
relaxation | Caesarean | 17 | 17 | 18–30 | F: 34 | Relaxation therapy
performed 10 times per session. One session performed each day from
post-operative days 3–7. | After completing 5
days of therapy | Greater pain
reduction in relaxation group. No statistical analysis done. |
| Ismail and Elgzar
(21), 2018a | Progressive muscle
relaxation | Caesarean | 40 | 40 | 20–35 | F: 80 | Relaxation therapy
performed thrice daily for 30 min on post-operative days 0 and
1. | After completing 2
days of therapy | Significantly less
pain, improved physical activity and better quality of sleep in
relaxation group. |
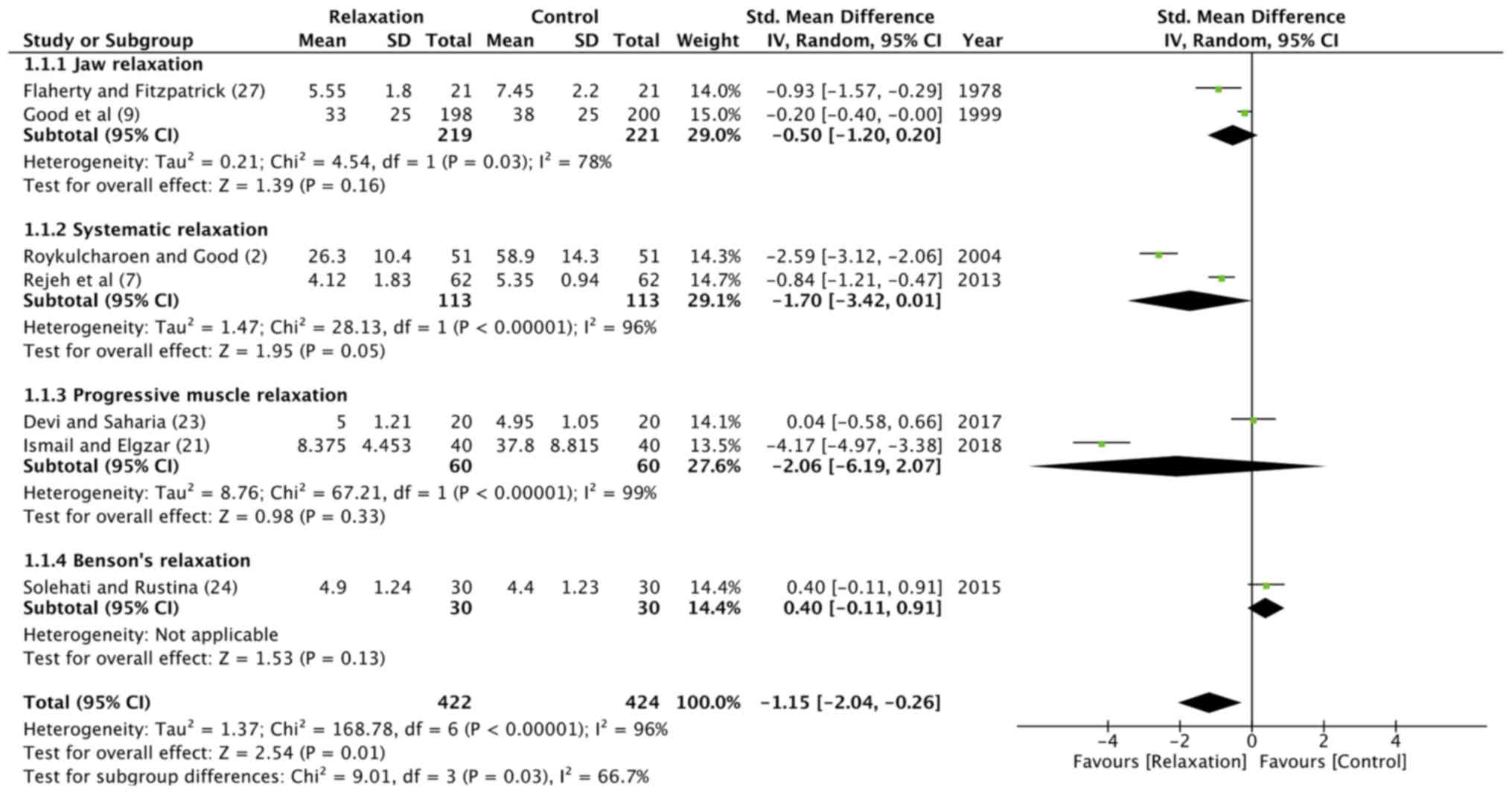
Meta-analysis
Seven of the 12 included studies reported sufficient
data for inclusion in the meta-analysis (2,7,9,21,23,24,27).
The data of 422 patients in the relaxation group and 424 patients
in the control group were pooled for a quantitative analysis. The
results indicated that patients undergoing abdominal surgery
experienced significantly greater pain relief following relaxation
therapy as compared to the controls (random: SMD, −1.15; 95% CI,
−2.04 to −0.26; P<0.00001) (Fig.
2). There was significant heterogeneity amongst studies with
I2=96%. Sub-group analysis demonstrated statistically
significant pain relief in patients undergoing abdominal surgery
and performing jaw relaxation (random: SMD, −0.50; 95% CI, −1.2 to
0.2; P=0.03), systematic relaxation (random: SMD, −1.7; 95% CI,
−3.42 to 0.01; P<0.00001); and PMR (random: SMD, −2.06; 95% CI,
−6.19 to 2.07; P<0.00001).
Outcome variables other than pain
A number of additional outcome variables were
compared between the relaxation and control groups by the included
studies. Systemic measures, such as pulse rate, blood pressure and
respiratory rate were analyzed by 3 studies (9,25,27).
Flaherty and Fitzpatrick (27), in
their study on jaw relaxation, recorded vital signs of the 2 groups
at the point when pain was being measured. There was no significant
difference in pulse rates and blood pressure between the 2 groups.
However, they found a greater post-operative decrease in the
respiratory rate in the relaxation group. Similarly, Good et
al (9), in their study on jaw
relaxation therapy, found significant decrease in pulse rates and
respiratory rates in the interventional group. On the other hand,
Chandrababu (25), in a trial on
PMR, reported no effect of relaxation therapy on respiratory rates
and blood pressure.
Studies on systematic relaxation
reported conflicting results on the effects of relaxation on
post-operative anxiety
While Roykulcharoen and Good (2) demonstrated no difference in
post-operative anxiety between the 2 groups, Rejeh et al
(7) recorded significantly less
anxiety in the relaxation group. Similarly, while the studies by
Levin (20) and Roykulcharoen and
Good (2) found no difference in
analgesic consumption between the relaxation and control groups,
Rejeh et al (7) recorded
significantly less analgesic use in the group practicing systematic
relaxation.
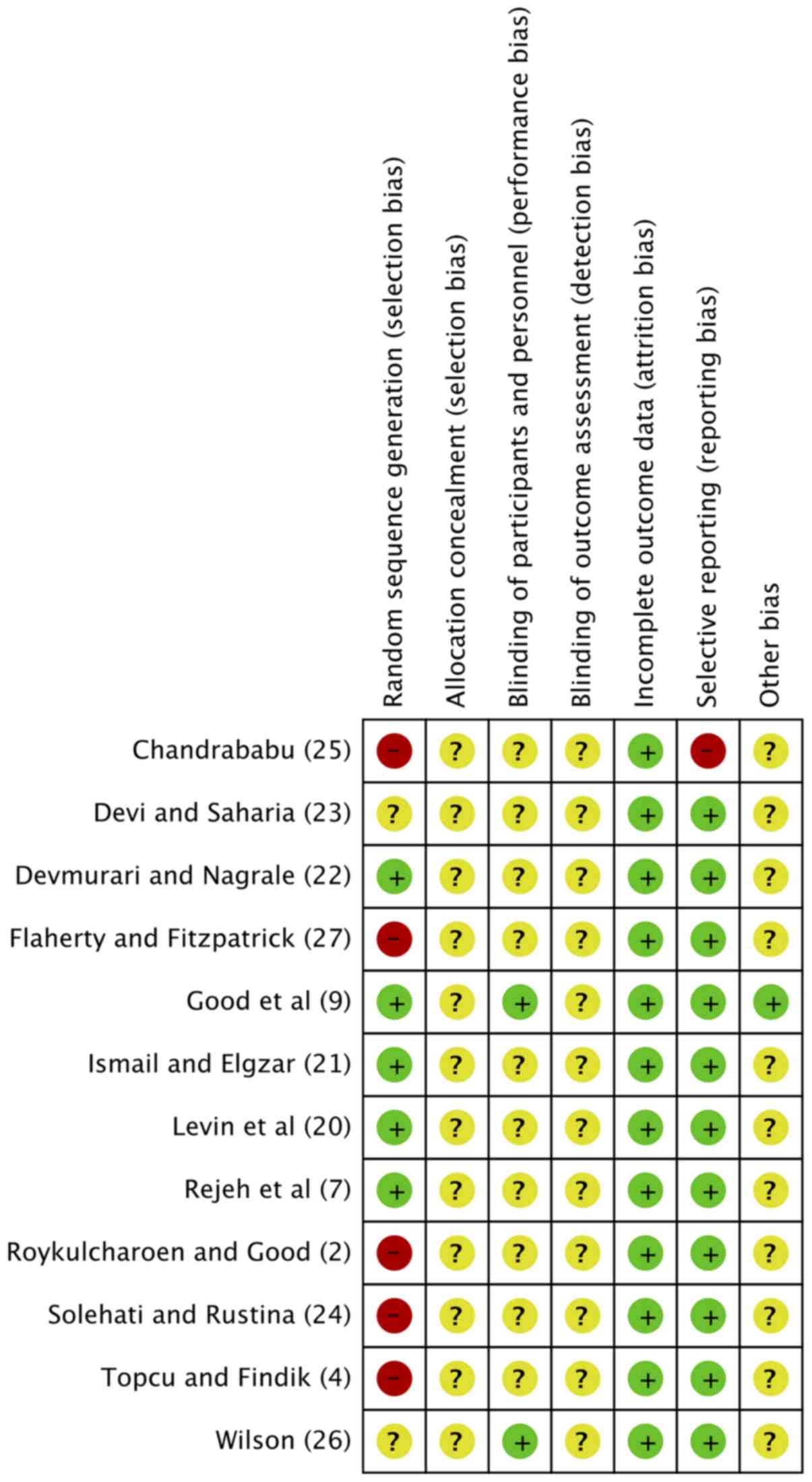
Quality of included studies
The risk of bias summary of the included studies is
presented in Fig. 3. Only 5 trials
reported an adequate information on the randomization method used
(7,9,20–22).
Blinding was reported by only 2 of the 12 studies (9,26). Based
on the scoring criteria, there was only 1 high quality study, while
all others were rated as ‘medium’.
Discussion
As shown by our literature review, relaxation
therapy has been a subject of substantial research in the area of
pain relief after abdominal surgery. Studies have compared 4
different relaxation methods to date. ‘Jaw relaxation’, which
involves the relaxation of the mouth and throat, is a specific
regional approach developed by Jacobson (9,28). He
proposed that as skills in releasing tension in the local parts of
the body are developed, the relaxation of the entire body becomes
easier. This technique was investigated by two of the included
studies in this review. Flaherty and Fitzpatrick (27) and Good et al (9) both demonstrated significant difference
in pain relief between patients practicing jaw relaxation therapy
and controls. Similar results with jaw relaxation have been
replicated by other researchers in the field of orthopedic surgery
(28,29). Ceccio et al (28) studied post-movement pain, in the
first 24 h following hip-surgery in elderly patients. They reported
significantly less pain in the group practicing jaw relaxation.
Seers et al (29) found
statistically significant reduction in pain with both jaw
relaxation and total body relaxation in patients undergoing
elective orthopedic surgery.
Total body relaxation techniques used by studies in
our review included, Benson's relaxation, PMR and systematic
relaxation. Only minor differences separate these 3 techniques
(2). Systematic relaxation differs
from PMR, as there is no muscle contraction involved; which
according to some authors may be painful in a post-operative
surgical patient (2). Benson's
relaxation and systematic relaxation are quite similar apart from
the fact that participants are more focused on breathing and the
repetition of a single word in Benson's technique. Upon the pooled
analysis of all the studies, we found that patients utilizing
relaxation techniques experienced a statistically significant
reduction in pain, as compared to individuals receiving usual
nursing care. These results were also significant for individual
sub-groups of jaw relaxation, PMR and systematic relaxation. While
our review focused only on abdominal surgery patients, relaxation
techniques have been used as a non-pharmacological pain relief
intervention in a number of other disorders. De Paolis et al
(30) found PMR with interactive
imagery to be an effective adjuvant pain relief technique for
terminal cancer patients. Jong et al (31) used PMR as an effective tool for pain
relief in children with primary headaches.
The mechanism of pain relief with relaxation therapy
has been explained in relation to the gate control theory of pain.
The gate control theory of pain postulates that alteration or
modification of pain impulses being transmitted from the peripheral
nerve receptors to the brain can result in little or no pain
perception (32). Substansia
gelatinosa, a group of densely packed cells along the length of the
spinal cord, are considered the site of transmission blockage. When
‘open’, this area allows for the transmission of pain sensation to
reach the dorsal horn of the spinal cord. Emotional and cognitive
factors are thought to influence this sensory transmission
(27,28). Fear, anxiety, attention to pain, past
experiences etc., all influence the pain response by acting on the
gate control system (33).
Relaxation therapy is thought to affect this cognitive and
emotional alteration thereby providing pain relief. Melzack and
Chapman (34) suggested that the
distraction of attention from the painful site, the reduction of
anxiety and the development of a sense of control over pain by
means of relaxation therapy can help diminish the noxious feeling.
Relaxation also helps diminish muscular and mental tension thereby
reducing sympathetic stimulation of the hypothalamus. This
modulates endogenous opioid production in the nervous systems which
in turn decreases propagation of pain impulses (35–37).
The actual effect of relaxation therapy on anxiety,
stress and systemic variables (pulse, blood pressure and
respiratory rate) in abdominal surgery have also been studied.
While some studies (7,18) have report significant reductions in
post-operative anxiety with relaxation therapy, others differ
(2). Similar variable results have
been reported for pulse rate, respiratory rate and blood pressure
(9,15,25,27).
Post-operative stress in patients with colorectal cancer has been
estimated using serum cortisol levels by Kim et al (15). Significant differences were found
between relaxation and control group on the first post-operative
day. The conflicting results amongst studies may be attributed to a
number of factors, such as small sample sizes in trials
demonstrating significant results (18), variable relaxation protocols,
difference in anxiety scales used, errors is timing and measurement
methods for systemic variables etc.
The strength of any meta-analysis to a certain
extent depends on the homogeneity and quality of the studies
included. A number of factors limit our reviews ability to draw
strong conclusions for relaxation therapy. Foremost, there was only
one high quality study (9) available
for inclusion. The methodology of the remaining studies was
questionable with absence of proper randomization and the blinding
of outcome assessment. Secondly, only 1 study included >100
participants per group (9). A number
of trials were underpowered with <20 patients in each group
(20,22,26).
Thirdly, the was a wide variation in the relaxation protocol used,
with studies employing the therapy at different times and for
varying periods of time. There was disparity in the pain scales
used, with both 10-point and 100-mm scales of VAS utilized across
studies. Fourthly, there was no longterm data available on the
effects of relaxation therapy on post-operative pain relief. Seers
et al (29) demonstrated that
pain relief following relaxation was not sustained for a long
period of time. While the majority of studies measured pain
immediately following relaxation therapy and found significant
differences between the intervention and control groups, the study
by Devmurari and Nagrale (22),
while comparing pain scores in post-caesarean females, after 5 days
of relaxation therapy, they found a significant reduction in pain
in both the interventional and control groups.
Despite a number of trials demonstrating benefits of
relaxation therapy for immediate pain relief in patients undergoing
post-abdominal surgery, there is lack of high-quality scientific
evidence substantiating its routine use. There is a need for more
robust RCTs utilizing standardized relaxation protocols to provide
further evidence on this subject. However, in the absence of
harmful effects of relaxation therapy and minimal time required for
training patients, despite weak evidence, it may still be employed
by nurses in the post-operative setting to provide short-term pain
relief.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WJ conceived and designed the study. LR, JC and YD
collected the data and performed the literature search. All authors
were involved in the writing of the manuscript. All authors have
read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
IASP pain terminology: International
Association for the Study of Pain (IASP). 2010.
|
|
2
|
Roykulcharoen V and Good M: Systematic
relaxation to relieve postoperative pain. J Adv Nurs. 48:140–148.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Miaskowski C: Current concepts in the
assessment and management of acute pain. Medsurg nursing: official
journal of the Academy of Medical-Surgical Nurses. 2:28–32, 40.
1993.PubMed/NCBI
|
|
4
|
Topcu SY and Findik UY: Effect of
relaxation exercises on controlling postoperative pain. Pain Manag
Nurs. 13:11–17. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jurf JB and Nirschl AL: Acute
postoperative pain management: A comprehensive review and update.
Crit Care Nurs Q. 16:8–25. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shang AB and Gan TJ: Optimising
postoperative pain management in the ambulatory patient. Drugs.
63:855–867. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rejeh N, Heravi-Karimooi M, Vaismoradi M
and Jasper M: Effect of systematic relaxation techniques on anxiety
and pain in older patients undergoing abdominal surgery. Int J Nurs
Pract. 19:462–470. 2013.PubMed/NCBI
|
|
8
|
Crowe L, Chang A, Fraser JA, Gaskill D,
Nash R and Wallace K: Systematic review of the effectiveness of
nursing interventions in reducing or relieving post-operative pain.
JBI Library Syst Rev. 6:165–224. 2008. View Article : Google Scholar
|
|
9
|
Good M, Stanton-Hicks M, Grass JA,
Cranston Anderson G, Choi C, Schoolmeesters LJ and Salman A: Relief
of postoperative pain with jaw relaxation, music and their
combination. Pain. 81:163–172. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Moher D, Liberati A, Tetzlaff J and Altman
DG; PRISMA Group, : Preferred reporting items for systematic
reviews and meta-analyses: The PRISMA statement. PLoS Med.
6:e10000972009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Higgins JPT and Green S: Cochrane Handbook
for Systemic Reviews of Interventions. Version 5. The Cochrane
Collaboration. 2011.
|
|
12
|
Higgins JPT, Altman D and Sterne J;
Cochrane Statistical Methods Group and the Cochrane Bias Methods
Group, : Chapter 8: Assessing risk of bias in included studies.
Cochrane Handbook for Systemic Reviews of Interventions. Higgins
JPT and Green S: Version 5. The Cochrane Collaboration. 2011
|
|
13
|
Good M, Anderson GC, Ahn S, Cong X and
Stanton-Hicks M: Relaxation and music reduce pain following
intestinal surgery. Res Nurs Health. 28:240–251. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hasanpour-Dehkordi A, Solati K, Tali SS
and Dayani MA: Effect of progressive muscle relaxation with
analgesic on anxiety status and pain in surgical patients. Br J
Nurs. 28:174–178. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kim KJ, Na YK and Hong HS: Effects of
progressive muscle relaxation therapy in colorectal cancer
patients. West J Nurs Res. 38:959–973. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Broadbent E, Kahokehr A, Booth RJ, Thomas
J, Windsor JA, Buchanan CM, Wheeler BR, Sammour T and Hill AG: A
brief relaxation intervention reduces stress and improves surgical
wound healing response: A randomised trial. Brain Behav Immun.
26:212–217. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Haase O, Schwenk W, Hermann C and Müller
JM: Guided imagery and relaxation in conventional colorectal
resections: A randomized, controlled, partially blinded trial. Dis
Colon Rectum. 48:1955–1963. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cheung YL, Molassiotis A and Chang AM: A
pilot study on the effect of progressive muscle relaxation training
of patients after stoma surgery. Eur J Cancer Care (Engl).
10:107–114. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
de Paula AAD, de Carvalho EC and dos
Santos CB: The use of the ‘progressive muscle relaxation’ technique
for pain relief in gynecology and obstetrics. Rev Lat Am
Enfermagem. 10:654–659. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Levin RF, Malloy GB and Hyman RB: Nursing
management of postoperative pain: Use of relaxation techniques with
female cholecystectomy patients. J Adv Nurs. 12:463–472. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Aziz Ismail NIA and Elgzar WTI: The effect
of progressive muscle relaxation on post cesarean section pain,
quality of sleep and physical activities limitation. Int J Stud
Nurs. 3:14–29. 2018. View Article : Google Scholar
|
|
22
|
Devmurari D and Nagrale S: Effectiveness
of Jacobson's progressive muscle relaxation technique for pain
management in post-cesaerean women. Indian J Obstet Gynecol Res.
5:228–232. 2018. View Article : Google Scholar
|
|
23
|
Devi R and Saharia H: Effect of
progressive muscle relaxation on postoperative analgesia. Indian J
Med Res Rev. 5:113–118. 2017.
|
|
24
|
Solehati T and Rustina Y: Benson
relaxation technique in reducing pain intensity in women after
cesarean section. Anesth Pain Med. 5:e222362015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chandrababu R: Effectiveness of
progressive muscle relaxation technique on pain perception among
patients who are subjected to abdominal surgery. Indian J Surg
Nurs. 1:83–88. 2012.
|
|
26
|
Wilson JF: Behavioral preparation for
surgery: Benefit or harm? J Behav Med. 4:79–102. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Flaherty GG and Fitzpatrick JJ: Relaxation
technique to increase comfort level of postoperative patients: A
preliminary study. Nurs Res. 27:352–355. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ceccio CM: Postoperative pain relief
through relaxation in elderly patients with fractured hips. Orthop
Nurs. 3:11–19. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Seers K, Crichton N, Tutton L, Smith L and
Saunders T: Effectiveness of relaxation for postoperative pain and
anxiety: Randomized controlled trial. J Adv Nurs. 62:681–688. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
De Paolis G, Naccarato A, Cibelli F,
D'Alete A, Mastroianni C, Surdo L, Casale G and Magnani C: The
effectiveness of progressive muscle relaxation and interactive
guided imagery as a pain-reducing intervention in advanced cancer
patients: A multicentre randomised controlled non-pharmacological
trial. Complement Ther Clin Pract. 34:280–287. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Jong MC, Boers I, van Wietmarschen HA,
Tromp E, Busari JO, Wennekes R, Snoeck I, Bekhof J and Vlieger AM:
Hypnotherapy or transcendental meditation versus progressive muscle
relaxation exercises in the treatment of children with primary
headaches: A multi-centre, pragmatic, randomised clinical study.
Eur J Pediatr. 178:147–154. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Davis P: Pain: Opening up the gate control
theory. Nurs Stand. 7:25–27. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Casey KL: The neurophysiologic basis of
pain. Postgrad Med. 53:58–63. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Melzack R and Chapman CR: Psychologic
aspects of pain. Postgrad Med. 53:69–75. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Vidal C and Jacob J: The effect of medial
hypothalamus lesions on pain control. Brain Res. 199:89–100. 1980.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Standley JM: Music research in
medical/dental treatment: Meta-analysis and clinical applications.
J Music Ther. 23:56–122. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Turner JA and Chapman CR: Psychological
interventions for chronic pain: A critical review. II. Operant
conditioning, hypnosis, and cognitive-behavioral therapy. Pain.
12:23–46. 1982. View Article : Google Scholar : PubMed/NCBI
|