Introduction
Bladder cancer (BC) is a common urological
malignancy; it is the 4th most common malignancy in males worldwide
(1) and one of the most expensive
cancers to manage (2). In the US,
>79,030 new cases of urothelial carcinoma (UC) were diagnosed in
2017 (3). Approximately 75% of UC
cases are initially identified as non-muscle invasive BC (NMIBC)
(4–6). However, NMIBC is a major challenge in
urological practice due to its high recurrence rate (60–70% of
patients) and rapid progression (20–30% of patients) (5,7). In
particular, T1 high-grade (T1HG) BC accounts for 25% of NMIBC cases
and is characterized by rapid progression and a high mortality rate
(5,8,9). T1HG BC
is a highly malignant tumor type with variable and unpredictable
biological potential (10). Babjuk
et al (11) suggested that
patients with T1HG cancers may undergo a range of treatments from
conservative therapy to early radical cystectomy, as these are
currently the optimal treatment strategies. However, the potential
risk of morbidity and negative impact on quality of life should be
considered when selecting the treatment strategy. It is important
to identify prognostic factors for patients with T1HG BC.
Identification of clinicopathological factors associated with
cancer recurrence and progression is crucial to the prognosis and
management of patients with T1HG BC.
Previous studies have demonstrated that tumor
multiplicity, tumor size, the T stage, the tumor grade and female
sex are risk factors for poor prognoses of patients with BC
(5,12). Previous studies also indicated that
independent prognostic factors for patients with T1HG BC include
female sex, the presence of carcinoma in situ in the
prostatic urethra and recurrence within 3 months (5). However, single prognostic factors exert
limited influence in certain patients with T1HG BC, while precise
individualized predictions may be required. A prognostic nomogram
is an efficient statistical tool that has been suggested as a novel
standard to predict an individual patient's survival. Nomograms,
which are graphic calculating scales, have been indicated to be a
useful tool in the management of several cancer types (13–15).
There are several advantages to prognostic nomograms, including
strong robustness and improved predictive accuracy, which enhance
their potential in maximizing the predictive accuracy of an
individual prognosis (15). However,
the use of prognostic nomograms for patients with T1HG BC, which
may be applied to predict the overall survival (OS) and
cancer-specific survival (CSS), has not been previously reported,
to the best of our knowledge.
In the present study, the clinical information of
cases with T1HG BC from 2004 to 2014 in the SEER dataset was
collected and analyzed. Surveillance Epidemiology and End Results
(SEER) is a US population-based cancer database containing ~28% of
the overall population of the US (15) and collects clinical information of
patients with tumors in 18 registries. The present study aimed to
develop validated prognostic nomograms that are able to predict the
OS and CSS of patients with T1HG BC.
Materials and methods
Patient eligibility and variables
Patient information was collected from the SEER
database. The SEER database is a public database comprising 18
cancer registries and covers ~28% of the US population. For the
present study, the data of patients with T1HG BC (2004–2014) were
downloaded from the SEER database using SEER*Stat software (version
8.3.5; National Cancer Institute).
The inclusion criteria for patients with T1HG BC
were as follows: i) Patients diagnosed with clinical T1HG BC
without evidence of lymph node involvement or metastasis (T1N0M0)
as the primary malignancy between 2004 and 2014 according to the
reclassification of stages in the 8th Edition of the Cancer Staging
Manual from the American Joint Committee on Cancer (16); ii) patients with tumor grades III
(poorly differentiated) and IV (undifferentiated); iii) patients
with known survival time following diagnosis and cause of death;
iv) patients with documentation of tumor size and age at diagnosis;
and v) patients with only primary tumors so that analyses of CSS
were more feasible. Survival time was defined as the time from the
date of disease diagnosis to the date of OS and CSS. Patients with
histological confirmation of urothelial carcinoma (International
Classification of Diseases for Oncology, 3rd: 8120 and 8130) and
missing data were excluded from the present analysis.
The clinicopathological features of patients with
T1HG BC included in the present analysis were sex, age, ethnicity,
tumor size, marital status, surgical status, use of radiation, use
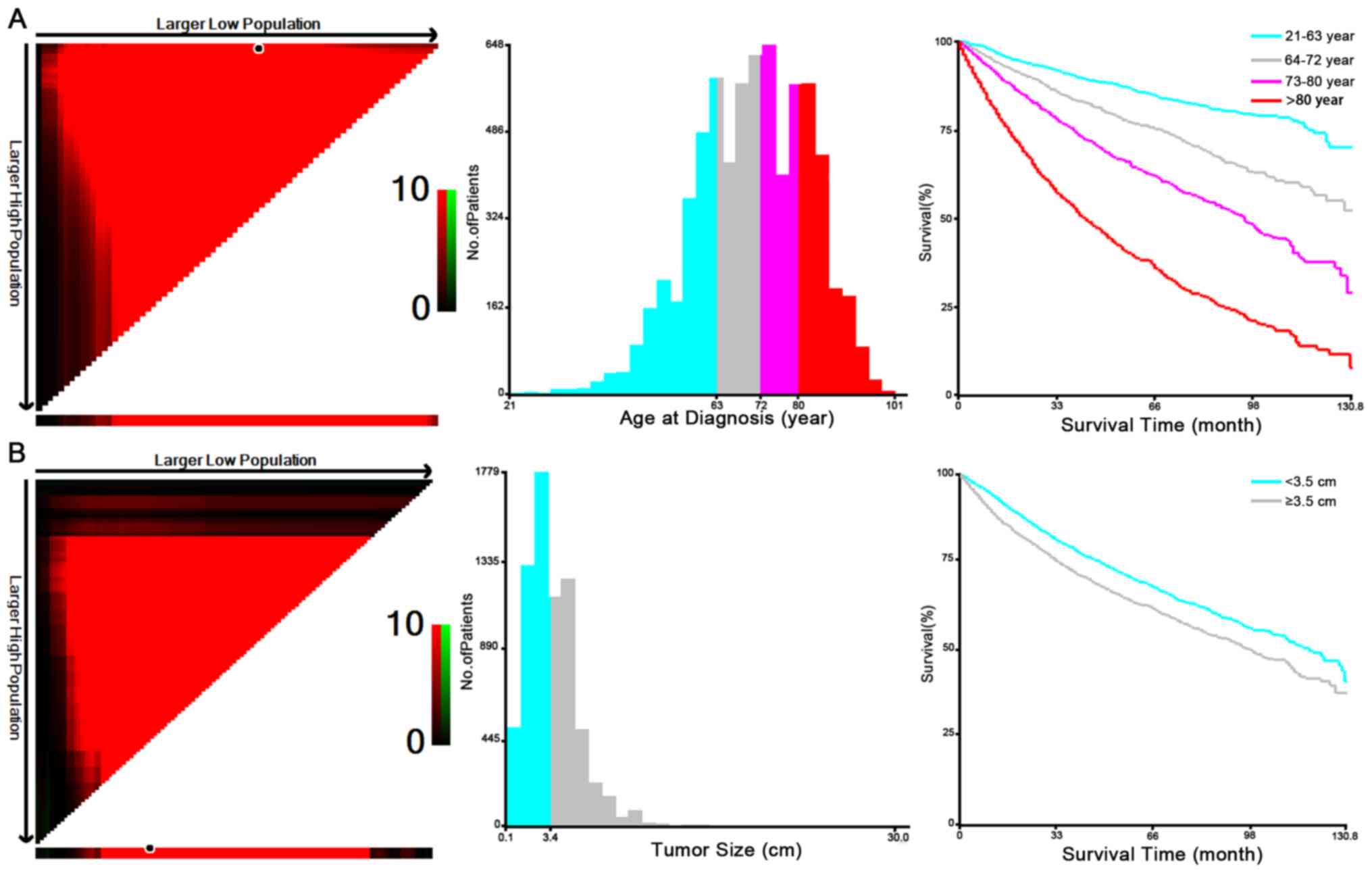
of chemotherapy and survival time. Cutoff values for the age at
diagnosis and tumor size were calculated using X-tile software
(Version 3.6.1; Copyright Yale University). It was applied to
stratify the patients by age and tumor size according to survival
time and status. X-tile software is a novel tool, which was
initially developed to determine the best cutoff values of
variables in cohorts with breast malignancies (17). The optimal cutoff value for the tumor
size of the T1HG BC lesions in the present study was identified as
3.4 cm (Fig. 1). The optimal cutoff
values for age in the cohort of T1HG BC patients were 63, 72 and 80
years. Regarding ethnicity, the cohort was divided into black,
white and other. Marital status was divided into married and
single/other. In terms of surgical resection, patients were divided
into those who underwent local tumor destruction/excision, partial
cystectomy, complete/radical cystectomy and those who did not
undergo any surgical resection. Regarding radiation, the cohort was
divided into those who were treated with radiation and those who
did not receive any radiation treatment. Nuances including
radiation type and fractionation were not available from the SEER
database. In terms of chemotherapy, the patients were divided into
those who received chemotherapy and those who did not receive
chemotherapy.
Statistical analysis
All of the patients with T1HG BC identified
according to the above-mentioned inclusion and exclusion criteria
(n=6,980) were randomly divided into the training cohort (n=4,886)
to construct and validate the prognostic nomograms, and the
validation cohort (n=2,094) to validate the nomograms. Chi-square
tests were applied to compare clinical characteristics between the
training and validation cohort.
Categorical variables were presented as the number
of patients with T1HG BC and the respective percentages. Cutoff
values for tumor size and age at diagnosis were calculated using
X-tile software based on OS (Fig.
1). The prognostic factors (sex, age, race, tumor size, marital
status, surgical status, use of radiation and use of chemotherapy)
were all incorporated in the univariate and multivariate Cox
proportional hazards model analysis for OS and CSS, respectively.
Hazard ratios and corresponding 95% confidence intervals (95% CIs)
of variables were listed. Variables determined to be significant in
the univariate and multivariate Cox proportional hazards regression
analyses were used to generate nomograms to predict 3- and 5-year
OS and CSS. The training cohort was used to establish the
nomograms. Internal and external validation of the prognostic
nomograms were based on the training cohort and the validation
cohort, respectively. Harrell's concordance-index (C-index)
(17) was applied to evaluate the
performances of the prognostic nomograms. The C-index value ranges
from 0.5 to 1.0, where 0.5 indicates total chance and 1.0 indicates
perfect matching. Consistency between the predicted probability and
the observed probability were assessed using calibration curves of
the nomograms. Chi-square test, and univariate and multivariate Cox
proportional hazards regression analysis, were performed in SPSS
22.0 (IBM Corp.). The rms package (version 3.3.3) in R was applied
to construct and validate the nomograms. Statistical significance
was defined as a two-sided P<0.05.
Results
Patient characteristics at
baseline
A total of 6,980 patients with T1HG BC were divided
into the training cohort (n=4,886) and the validation cohort
(n=2,094). The characteristics of all the patients with T1HG BC are
summarized in Table I. The total
cohort comprised 5,452 (78.1%) male patients and 1,528 (21.9%)
female patients. A total of 361 (5.2%) patients were black, 6,212
(89.0%) were white and 407 (5.8%) were designated as other. A total
of 4,538 (65.0%) patients were married and 2,442 (35%) patients
were single or other. Among the patients with T1HG BC, 6,472
(92.7%) patients underwent local tumor destruction/excision, 83
(1.2%) underwent a partial cystectomy, 338 (4.8%) underwent
complete/radical cystectomy and 87 (1.2%) patients did not undergo
surgical resection. A total of 858 (12.3%) deaths were attributed
to T1HG BC and 1,054 (15.1%) patients died from other causes. There
were no significant differences in sex, age, ethnicity, tumor size,
marital status, surgical status, use of chemotherapy and use of
radiation between the training and validation cohorts.
 | Table I.Demographics and clinicopathological
characteristics of patients with T1 high-grade bladder cancer. |
Table I.
Demographics and clinicopathological
characteristics of patients with T1 high-grade bladder cancer.
| Variable | Training cohort
(n=4,886) | Validation cohort
(n=2,094) | Total
(n=6,980) | P-value |
|---|
| Sex |
|
|
| 0.426 |
|
Male | 3,829 (78.4) | 1,623 (77.5) | 5,452 (78.1) |
|
|
Female | 1,057 (21.6) | 471 (22.5) | 1,528 (21.9) |
|
| Age (years) |
|
|
| 0.203 |
|
21–63 | 1,281 (26.2) | 501 (23.9) | 1,782 (25.5) |
|
|
64–72 | 1,275 (26.1) | 547 (26.1) | 1,822 (26.1) |
|
|
73–80 | 1,151 (23.6) | 520 (24.8) | 1,671 (23.9) |
|
|
>80 | 1,179 (24.1) | 526 (25.1) | 1,705 (24.4) |
|
| Ethnicity |
|
|
| 0.271 |
|
Black | 239 (4.9) | 122 (5.8) | 361 (5.2) |
|
|
White | 4,361 (89.3) | 1,851 (88.4) | 6,212 (89.0) |
|
|
Other | 286 (5.9) | 121 (5.8) | 407 (5.8) |
|
| Marital status |
|
|
| 0.107 |
|
Single/other | 1,680 (34.4) | 762 (36.4) | 2,442 (35.0) |
|
|
Married | 3,206 (65.6) | 1,332 (63.6) | 4,538 (65.0) |
|
| Surgery |
|
|
| 0.927 |
|
None | 63 (1.3) | 24 (1.1) | 87 (1.2) |
|
| Local
tumor destruction/excision | 4,527 (92.7) | 1,945 (92.9) | 6,472 (92.7) |
|
| Partial
cystectomy | 60 (1.2) | 23 (1.1) | 83 (1.2) |
|
|
Complete/radical
cystectomy | 236 (4.8) | 102 (4.9) | 338 (4.8) |
|
| Tumor size
(cm) |
|
|
| 0.773 |
|
<3.5 | 2,592 (53.0) | 1,103 (52.7) | 3,695 (52.9) |
|
|
≥3.5 | 2,294 (47.0) | 991 (47.3) | 3,285 (47.1) |
|
| Radiation |
|
|
| 0.381 |
|
Yes | 107 (2.2) | 39 (1.9) | 146 (2.1) |
|
| No | 4,779 (97.8) | 2,055 (98.1) | 6,834 (97.9) |
|
| Chemotherapy |
|
|
| 0.155 |
|
Yes | 1,045 (21.4) | 480 (22.9) | 1,525 (21.8) |
|
| No | 3,841 (78.6) | 1,614 (77.1) | 5,455 (78.2) |
|
OS of the training cohort
Sex, age, ethnicity, tumor size, marital status,
surgical status, use of chemotherapy and use of radiation in the
training cohort were selected as variables for the univariate Cox
analyses (Table II). The results of
the analysis revealed that all of the above-mentioned variables
were associated with OS (P<0.05;). Furthermore, all of these
variables except for the use of chemotherapy were associated with
CSS (P<0.05). Multivariate Cox analyses were then performed to
control for the confounding variables (Table III). According to the multivariate
analysis, age, ethnicity, tumor size, marital status, surgical
status and use of radiation were identified as significant
prognostic factors for OS and CSS (P<0.05).
| Table II.Univariate Cox regression analysis of
prognostic factors in patients with T1 high-grade bladder
cancer. |
Table II.
Univariate Cox regression analysis of
prognostic factors in patients with T1 high-grade bladder
cancer.
|
| Cancer-specific
survival | Overall
survival |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Sex (female vs.
male) | 1.502 | 1.272–1.774 | <0.001 | 1.302 | 1.158–1.465 | <0.001 |
| Age (years) |
|
|
|
|
|
|
|
21–63 | Reference |
|
| Reference |
|
|
|
64–72 | 1.358 | 1.053–1.751 | 0.019 | 1.770 | 1.459–2.147 | <0.001 |
|
73–80 | 1.933 | 1.514–2.469 | <0.001 | 3.092 | 2.508–3.705 | <0.001 |
|
>80 | 4.079 | 3.259–5.105 | <0.001 | 6.426 | 5.414–7.627 | <0.001 |
| Ethnicity |
|
|
|
|
|
|
|
Black | Reference |
|
| Reference |
|
|
|
White | 0.521 | 0.393–0.690 | <0.001 | 0.606 | 0.493–0.744 | <0.001 |
|
Other | 0.460 | 0.300–0.705 | <0.001 | 0.415 | 0.302–0.572 | <0.001 |
| Marital status
(married vs. single/other) | 0.623 | 0.535–0.725 | <0.001 | 1.033 | 0.453–2.355 | <0.001 |
| Surgery | 14.476 | 3.391–61.792 | <0.001 | 9.955 | 2.376–41.720 | 0.002 |
|
None | Reference |
|
| Reference |
|
|
| Local
tumor destruction/excision | 0.429 | 0.257–0.716 | 0.001 | 0.493 | 0.341–0.712 | <0.001 |
| Partial
cystectomy | 0.673 | 0.329–1.377 | 0.278 | 0.506 | 0.290–0.880 | 0.016 |
|
Complete/radical
cystectomy | 0.447 | 0.245–0.815 | 0.005 | 0.346 | 0.221–0.541 | <0.001 |
| Tumor
size (≥3.5 vs. <3.5 cm) | 1.451 | 1.247–1.688 | <0.001 | 1.329 | 1.199–1.473 | <0.001 |
|
Radiation (yes vs. no) | 5.070 | 3.809–6.749 | <0.001 | 3.413 | 2.696–14.321 | <0.001 |
| Chemotherapy (yes
vs. no) | 0.315 | 0.738–1.103 | 0.315 | 0.859 | 0.745–0.990 | 0.035 |
| Table III.Multivariate Cox regression analysis
for prognosis factors in patients with T1 high-grade bladder
cancer. |
Table III.
Multivariate Cox regression analysis
for prognosis factors in patients with T1 high-grade bladder
cancer.
|
| Cancer-specific
survival | Overall
survival |
|---|
|
|
|
|
|---|
| Covariates | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Sex (female vs.
male) | 1.114 | 0.931–1.332 | 0.237 | 0.969 | 0.854–1.100 | 0.629 |
| Age (years) |
|
|
|
|
|
|
|
21–63 | Reference |
|
| Reference |
|
|
|
64–72 | 1.409 | 1.091–1.819 | <0.001 | 1.808 | 1.490–2.195 | <0.001 |
|
73–80 | 1.941 | 1.518–2.483 | <0.001 | 3.106 | 2.590–3.725 | <0.001 |
|
>80 | 3.854 | 3.063–4.848 | <0.001 | 6.203 | 5.210–7.384 | <0.001 |
| Ethnicity |
|
|
|
|
|
|
|
Black | Reference |
|
| Reference |
|
|
|
White | 0.526 | 0.394–0.701 | <0.001 | 0.552 | 0.477–0.680 | <0.001 |
|
Other | 0.473 | 0.306–0.730 | 0.001 | 0.402 | 0.291–0.556 | <0.001 |
| Marital status
(married vs. single/other) | 0.792 | 0.672–0.933 | 0.005 | 0.856 | 0.764–0.959 | 0.007 |
| Surgery |
|
|
|
|
|
|
|
None | Reference |
|
| Reference |
|
|
| Local
tumor destruction/excision | 0.521 | 0.311–0.873 | 0.013 | 0.561 | 0.387–0.811 | 0.002 |
| Partial
cystectomy | 0.588 | 0.286–1.210 | 0.149 | 0.438 | 0.251–0.765 | 0.004 |
|
Complete/radical
cystectomy | 0.703 | 0.383–1.290 | 0.255 | 0.547 | 0.348–0.859 | 0.009 |
| Tumor size (≥3.5
vs. <3.5 cm) | 1.323 | 1.135–1.541 | <0.001 | 1.237 | 1.115–1.372 | <0.001 |
|
Radiation (yes vs. no) | 3.906 | 2.911–5.241 | <0.001 | 2.766 | 2.169–3.526 | <0.001 |
|
Chemotherapy (yes vs. no) |
|
|
| 0.884 | 0.765–1.022 | 0.095 |
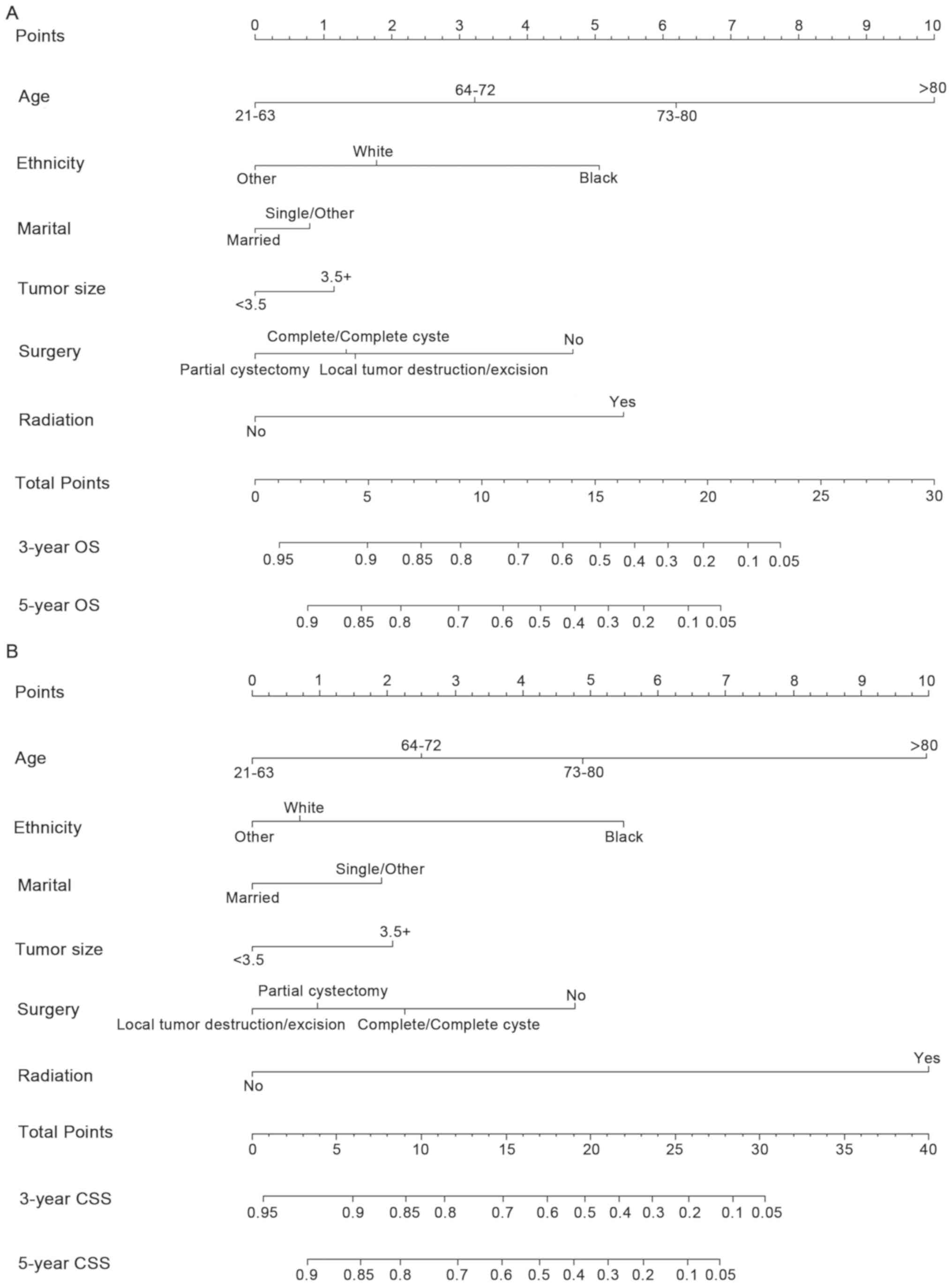
Construction and validation of OS and
CSS nomograms
The six aforementioned variables were used to
construct prognostic nomograms to predict 3- and 5- year OS and CSS
of patients with T1HG BC (Fig. 2;
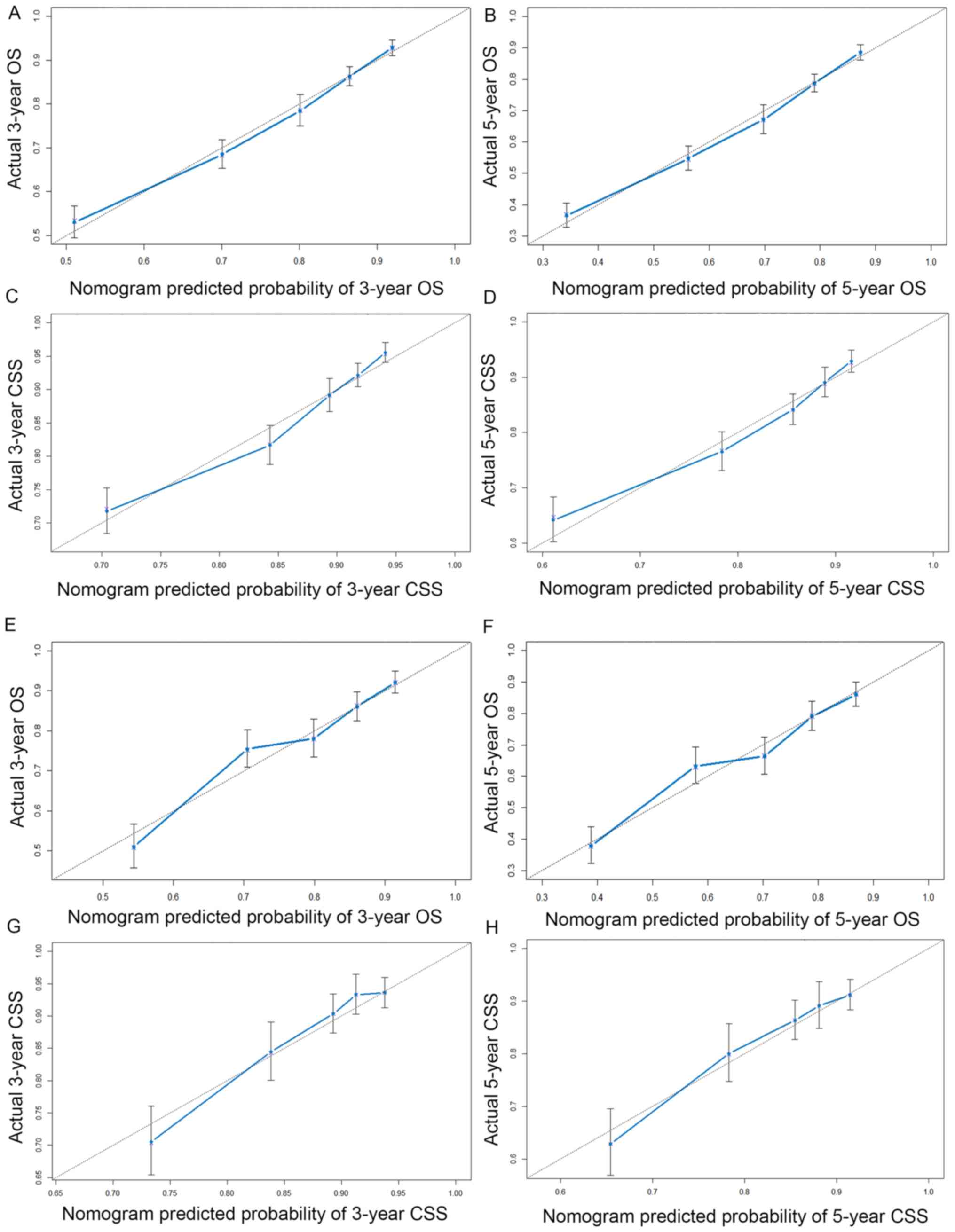
Table IV). Internal and external
validation of prognostic nomograms were performed. The predictive
accuracy of the final prognostic nomogram models was evaluated by
the C-index. The C-indices for the internal validation of the OS
and CSS nomograms were 0.707 (95% CI, 0.693–0.721) and 0.700 (95%
CI, 0.679–0.721), respectively. In the external validation, the
C-indices for the OS and CSS nomograms were 0.700 (95% CI,
0.677–0.723) and 0.698 (95% CI, 0.666–0.730), respectively.
Calibration plots revealed a good agreement between actual survival
and the nomogram prediction (Fig.
3). These prognostic nomograms are easy to use by surgeons for
the prognostication of patients with T1HG BC.
| Table IV.Specific scores of prognosis factors
in prognostic nomograms in patients with T1 high-grade bladder
cancer. |
Table IV.
Specific scores of prognosis factors
in prognostic nomograms in patients with T1 high-grade bladder
cancer.
| Characteristic | OS nomogram | CSS nomogram |
|---|
| Age (years) |
|
|
|
21–63 | 0 | 0 |
|
64–72 | 3.2 | 2.5 |
|
73–80 | 6.2 | 4.9 |
|
>80 | 10.0 | 10.0 |
| Ethnicity |
| 0 |
|
Black | 5.1 | 5.5 |
|
White | 1.8 | 0.7 |
|
Other | 0 | 0 |
| Marital status |
|
|
|
Single/other | 0.8 | 1.9 |
|
Married | 0 | 0 |
| Surgery |
|
|
|
None | 4.7 | 4.8 |
| Local
tumor destruction/excision | 1.5 | 0 |
| Partial
cystectomy | 0 | 1.0 |
|
Complete/radical
cystectomy | 1.3 | 2.2 |
| Tumor size
(cm) |
|
|
|
<3.5 | 0 | 0 |
|
≥3.5 | 1.2 | 6.5 |
| Radiation |
|
|
| No | 0 | 0 |
|
Yes | 5.4 | 10.0 |
Discussion
Due to heterogeneity of T1HG cancers, it is
difficult to predict the behavior of T1HG BC and the prognosis of
affected patients (18,19). Various prognostic factors may
influence the survival rate of patients with cancer. Therefore,
understanding the role of prognostic factors in the evaluation of
patients with T1HG BC is important. However, a single prognostic
factor may only have limited utility in individual survival
prediction. Nomograms, a tool commonly used for estimating the
survival of individual patients, are capable of considering the
accumulated effect of all prognostic factors, thus being able to
predict 3- and 5-year survival probabilities (20–22). To
date, several nomograms have been established for patients with BC
(23–25).
However, to the best of our knowledge, prognostic
nomograms have not been constructed for patients with T1HG BC, and
the present study was the first to establish comprehensive
prognostic nomograms to predict 3- and 5-year OS and CSS for
patients with T1HG BC using the SEER database. These validated
nomograms may be used in the clinical setting based on specific
clinicopathological information, which is most likely available to
the surgeon to evaluate a patient's prognosis. Several clinical
characteristics were determined to be independent prognostic
factors for OS or CSS, including patient age, ethnicity, tumor
size, marital status, status of surgery and use of radiation.
By using the optimal cutoff values for age in the
present study, it was revealed that the survival rates of patients
with T1HG BC worsened with increasing age, and it was suggested
that age is a strong and independent risk factor for T1HG BC
patient survival. The present study indicated that a larger tumor
size (>3.5 cm) was an independent prognostic factor in patients
with T1HG BC. A previous study indicated that recurrence,
progression and poorer survival rates were more common in patients
with larger tumors (26). In the
present study, the marital status had a significant prognostic
value. In a previous study, the mean relative survival was
significantly increased among married patients with BC (27). It may be hypothesized that support
from a spouse is key to increasing the OS of patients with T1HG BC
and this may include complex mechanisms. Ethnicity was also an
independent prognostic factor for survival, as white and black
patients with T1HG BC had poorer survival compared with other
ethnicities with T1HG BC, particularly black patients. The results
were similar to those of previous studies that suggest that
ethnicity influence prognosis (28,29). The
differential rates may reflect underlying sociodemographic and
economic factors. These factors may affect access to care and
lifestyle characteristics, including obesity and smoking, as well
as education (30–32).
The goal in the treatment of patients with T1HG BC
is to minimize the recurrence and progression of the disease, as
well as patient mortality, while maximizing the patient's quality
of life. This particularly applies to patients newly diagnosed with
T1HG BC or those with recurrent T1HG BC. In the present study,
surgical status and use of radiation were also identified as
independent prognostic factors. The proposed nomograms included
four treatment strategies: Local tumor destruction/excision,
partial cystectomy, complete/radical cystectomy and radiation,
which are significant predictors of survival outcomes for patients
with T1HG BC. It is noteworthy that adjuvant radiotherapy was
associated with poorer survival rates. Although radiotherapy has
improved or preserved organ function in patients with T1HG BC, a
recent phase-III trial indicated that radiotherapy alone was not
superior to other conservative treatment strategies (33). However, the ultimate value of
radiotherapy should be determined in a randomized trial using a
multicenter approach to recruit a sufficient amount of patients.
Among these treatment strategies, surgical therapy remains the most
frequently used therapeutic method for patients with T1HG BC.
T1HG BC is heterogeneous in nature and challenging
to treat. Bladder cystectomy is the current standard treatment
modality for patients with T1HG BC. A recent study reported that
patients with T1HG BC have a considerable risk of progression and
strongly advocated for immediate/early cystectomy for patients with
T1HG BC who have a long life expectancy (34). However, whether patients with T1HG BC
should undergo immediate radical cystectomy or bladder preservation
remains a much-debated issue (35).
Certain studies have indicated that immediate or early cystectomy
for patients with T1HG BC reduced the risk of recurrence,
progression and metastasis (36,37).
However, cystectomy may severely affect the quality of life of
patients with T1HG BC. Transurethral resection with intravesical
therapy is the first-line therapy for patients with NMIBC (11). However, recurrence or progression
occurs in more than half of all patients, which requires a second
resection or cystectomy (38–40).
Therefore, the overall situation and the prognosis of the patient
must be taken into account when selecting the most appropriate
surgical treatment.
Significant prognostic factors identified in the
present study were used to construct nomograms to estimate the 3-
and 5-year OS and CSS of patients with T1HG BC. Individual survival
rates of patients with T1HG BC may be precisely evaluated via these
nomograms. A practicable nomogram may help surgeons estimate the
precise likelihood of survival at different time-points. Such
prognostic nomograms may increase the surgeon's ability to identify
patients with T1HG BC with an elevated risk of progression and
mortality.
As an example for the application of the nomogram, a
75-year-old single white patient diagnosed with conventional T1HG
BC with a primary tumor size of 5.0 cm is discussed. The patient
would not have undergone surgery or received radiation therapy.
Corresponding points may be acquired from the vertical line of each
significant prognostic factor in the nomogram point scale. This
patient receives 14.7 and 18.8 points in the OS and CSS prognostic
nomograms, respectively. Therefore, the estimated 3- and 5-year OS
probability of this patient would be 52.5 and 35%, respectively,
from the OS nomogram scale. The 3- and 5-year CSS probability of
this patient would be 54 and 41%, respectively, from the CSS
nomogram scale.
Several potential limitations of the present study
should still be considered. First, the only 3- and 5-year survival
were considered as the end-points, but did not local recurrence, as
it was not available from the SEER database. Furthermore, the
information used to construct and validate the nomograms was from
the same SEER database, which may reduce the reliability of the
nomogram. The prognostic nomograms provided by the present study
may be more credible if they were validated by another dataset.
In summary, nomograms for predicting 3- and 5-year
OS and CSS of patients with T1HG BC were constructed and validated
in the present study. The nomograms were based on the patients'
age, ethnicity, tumor size, marital status, status of surgery and
use of radiation. They may serve as effective and convenient
evaluation tools to help surgeons perform personalized survival
prediction and mortality risk identification in patients with T1HG
BC.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Science and
Technology Planning Project of Guangdong Province (grant no.
2017B030314108) and the research start-up fee for the Eighth
Affiliated Hospital, Sun Yat-sen University (grant no.
zdbykyqdf005).
Availability of data and materials
The datasets analyzed during the present study were
downloaded from the SEER database (https://seer.cancer.gov/).
Authors' contributions
ZH, FT and ZL conceived the study. FT, ZL, WW and YC
performed the experiments. GW and YL analyzed the data. ZH, FT and
ZL wrote the paper. All the authors read and approved the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
T1HG
|
T1 high-grade
|
|
BC
|
bladder cancer
|
|
SEER
|
Surveillance Epidemiology and End
Results
|
|
OS
|
overall survival
|
|
CSS
|
cancer-specific survival
|
|
UC
|
urothelial carcinoma
|
|
NMIBC
|
non-muscle invasive bladder cancer
|
References
|
1
|
Chavan S, Bray F, Lortet-Tieulent J,
Goodman M and Jemal A: International variations in bladder cancer
incidence and mortality. Eur Urol. 66:59–73. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sievert KD, Amend B, Nagele U, Schilling
D, Bedke J, Horstmann M, Hennenlotter J, Kruck S and Stenzl A:
Economic aspects of bladder cancer: What are the benefits and
costs? World J Urol. 27:295–300. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Colombo R, Hurle R, Moschini M, Freschi M,
Colombo P, Colecchia M, Ferrari L, Lucianò R, Conti G, Magnani T,
et al: Feasibility and clinical roles of different substaging
systems at first and second transurethral resection in patients
with T1 high-grade bladder cancer. Eur Urol Focus. 4:87–93. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Babjuk M, Burger M, Zigeuner R, Shariat
SF, van Rhijn BW, Compérat E, Sylvester RJ, Kaasinen E, Böhle A,
Palou Redorta J, et al: EAU guidelines on non-muscle-invasive
urothelial carcinoma of bladder: Update 2013. Eur Urol. 64:639–653.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Proctor I, Stoeber K and Williams GH:
Biomarkers in bladder cancer. Histopathology. 57:1–13. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Goodison S, Rosser CJ and Urquidi V:
Bladder cancer detection and monitoring: Assessment of urine- and
blood-based marker tests. Mol Diagn Ther. 17:71–84. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
van Rhijn BW, Burger M, Lotan Y, Solsona
E, Stief CG, Sylvester RJ, Witjes JA and Zlotta AR: Recurrence and
progression of disease in non-muscle-invasive bladder cancer: From
epidemiology to treatment strategy. Eur Urol. 56:430–442. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fransen van de Putte EE, Behrendt MA,
Pigot GL, van der Kwast TH and van Rhijn BW: Prognostic
significance of substage and WHO classification systems in T1
urothelial carcinoma of the bladder. Curr Opin Urol. 25:427–435.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kitamura H and kakehi Y: Treatment and
management of high-grade T1 bladder cancer: What should we do after
second TUR? Jpn J Clin Oncol. 45:315–322. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Babjuk M, Böhle A, Burger M, Capoun O,
Cohen D, Compérat EM, Hernández V, Kaasinen E, Palou J, Rouprêt M,
et al: EAU guidelines on non-muscle-invasive urothelial carcinoma
of the bladder: Update 2016. Eur Urol. 71:447–461. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Fernandez-Gomez J, Madero R, Solsona E,
Unda M, Martinez-Piñeiro L, Gonzalez M, Portillo J, Ojea A, Pertusa
C, Rodriguez-Molina J, et al: Predicting non-muscle invasive
bladder cancer recurrence and progression in patients treated with
bacillus Calmette-Guerin: The CUETO scoring model. J Urol.
182:2195–2203. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Song K, Shi X, Wang H, Zou F, Lu F, Ma X,
Xia X and Jiang J: Can a nomogram help to predict the overall and
cancer-specific survival of patients with chondrosarcoma? Clin
Orthop Relat Res. 476:987–996. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fang C, Wang W, Feng X, Sun J, Zhang Y,
Zeng Y, Wang J, Chen H, Cai M, Lin J, et al: Nomogram individually
predicts the overall survival of patients with
gastroenteropancreatic neuroendocrine neoplasms. Br J Cancer.
117:1544–1550. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dong F, Shen Y, Gao F, Shi X, Xu T, Wang
X, Zhang X, Zhong S, Zhang M, Chen S and Shen Z: Nomograms to
predict individual prognosis of patients with primary small cell
carcinoma of the bladder. J Cancer. 9:1152–1164. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Amin MB, Edge SB, Greene FL, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR,
Sullivan DC, et al: AJCC cancer staging manual. 8th. New York:
Springer; 2017, View Article : Google Scholar
|
|
17
|
Camp RL, Dolled-Filhart M and Rimm DL:
X-tile: A new bio-informatics tool for biomarker assessment and
outcome-based cut-point optimization. Clin Cancer Res.
10:7252–7259. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang LC, Xylinas E, Kent MT, Kluth LA,
Rink M, Jamzadeh A, Rieken M, Al Hussein Al Awamlh B, Trinh QD, Sun
M, et al: Combining smoking information and molecular markers
improves prognostication in patients with urothelial carcinoma of
the bladder. Urol Oncol. 32:433–440. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Xylinas E, Kluth LA, Lotan Y, Daneshmand
S, Rieken M, Karakiewicz PI and Shariat SF: Blood- and tissue-based
biomarkers for prediction of outcomes in urothelial carcinoma of
the bladder. Urol Oncol. 32:230–242. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Valentini V, van Stiphout RG, Lammering G,
Gambacorta MA, Barba MC, Bebenek M, Bonnetain F, Bosset JF, Bujko
K, Cionini L, et al: Nomograms for predicting local recurrence,
distant metastases, and overall survival for patients with locally
advanced rectal cancer on the basis of European randomized clinical
trials. J Clin Oncol. 29:3163–3172. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Balachandran VP, Gonen M, Smith JJ and
DeMatteo RP: Nomograms in oncology: More than meets the eye. Lancet
Oncol. 16:e173–e80. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kim MS, Lee SY, Lee TR, Cho WH, Song WS,
Koh JS, Lee JA, Yoo JY and Jeon DG: Prognostic nomogram for
predicting the 5-year probability of developing metastasis after
neo-adjuvant chemotherapy and definitive surgery for AJCC stage II
extremity osteosarcoma. Ann Oncol. 20:955–960. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Al-Daghmin A, English S, Kauffman EC, Din
R, Khan A, Syed JR, Sztorc J, Mehedint D, Sharif M, Shi Y, et al:
External validation of preoperative and postoperative nomograms for
prediction of cancer-specific survival, overall survival and
recurrence after robot-assisted radical cystectomy for urothelial
carcinoma of the bladder. BJU Int. 114:253–260. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Brooks M, Godoy G, Sun M, Shariat SF,
Amiel GE and Lerner SP: External validation of bladder cancer
predictive nomograms for recurrence, cancer-free survival and
overall survival following radical cystectomy. J Urol. 195:283–289.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ishioka J, Saito K, Sakura M, Yokoyama M,
Matsuoka Y, Numao N, Koga F, Masuda H, Fujii Y, Kawakami S and
Kihara K: Development of a nomogram incorporating serum C-reactive
protein level to predict overall survival of patients with advanced
urothelial carcinoma and its evaluation by decision curve analysis.
Br J Cancer. 107:1031–1036. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fujii N, Hoshii Y, Hirata H, Mori J,
Shimizu K, Kobayashi K, Kawai Y, Inoue R, Yamamoto Y, Matsumoto H,
et al: Impact of divergent differentiation in urothelial carcinoma
on oncological outcome in patients with T1 high-grade bladder
cancer. Jpn J Clin Oncol. 47:560–567. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Merrill RM and Johnson E: Benefits of
marriage on relative and conditional relative cancer survival
differ between males and females in the USA. J Cancer Surviv.
11:578–589. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chamie K, Litwin MS, Bassett JC, Daskivich
TJ, Lai J, Hanley JM, Konety BR and Saigal CS; Urologic Diseases in
America Project, : Recurrence of high-risk bladder cancer: A
population-based analysis. Cancer. 119:3219–3227. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Abdollah F, Gandaglia G, Thuret R,
Schmitges J, Tian Z, Jeldres C, Passoni NM, Briganti A, Shariat SF,
Perrotte P, et al: Incidence, survival and mortality rates of
stage-specific bladder cancer in United States: A trend analysis.
Cancer Epidemiol. 37:219–225. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Brookfield KF, Cheung MC, Gomez C, Yang R,
Nieder AM, Lee DJ and Koniaris LG: Survival disparities among
African American women with invasive bladder cancer in Florida.
Cancer. 115:4196–4209. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Mallin K, David KA, Carroll PR, Milowsky
MI and Nanus DM: Transitional cell carcinoma of the bladder: Racial
and gender disparities in survival (1993 to 2002), stage and grade
(1993 to 2007). J Urol. 185:1631–1636. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ward EM, Fedewa SA, Cokkinides V and Virgo
K: The association of insurance and stage at diagnosis among
patients aged 55 to 74 years in the national cancer database.
Cancer J. 16:614–621. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Weiss C, Ott OJ, Wittlinger M, Krause SF,
Fietkau R, Sauer R and Rödel C: Treatment options for high-risk T1
bladder cancer: Status quo and future perspectives of
radiochemotherapy. Strahlenther Onkol. 184:443–449. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Vartolomei MD, Ferro M, Cantiello F,
Lucarelli G, Di Stasi S, Hurle R, Guazzoni G, Busetto GM, De
Berardinis E, Damiano R, et al: Validation of
neutrophil-to-lymphocyte ratio in a multi-institutional cohort of
patients with T1G3 non-muscle-invasive bladder cancer. Clin
Genitourin Cancer. 16:445–452. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Canter D, Egleston B, Wong YN, Smaldone
MC, Simhan J, Greenberg RE, Uzzo RG and Kutikov A: Use of radical
cystectomy as initial therapy for the treatment of high-grade T1
urothelial carcinoma of the bladder: A SEER database analysis. Urol
Oncol. 31:866–870. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Aziz A, May M, Burger M, Palisaar RJ,
Trinh QD, Fritsche HM, Rink M, Chun F, Martini T, Bolenz C, et al:
Prediction of 90-day mortality after radical cystectomy for bladder
cancer in a prospective European multicenter cohort. Eur Urol.
66:156–163. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Shabsigh A, Korets R, Vora KC, Brooks CM,
Cronin AM, Savage C, Raj G, Bochner BH, Dalbagni G, Herr HW and
Donat SM: Defining early morbidity of radical cystectomy for
patients with bladder cancer using a standardized reporting
methodology. Eur Urol. 55:164–174. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Gontero P, Sylvester R, Pisano F, Joniau
S, Oderda M, Serretta V, Larré S, Di Stasi S, Van Rhijn B, Witjes
AJ, et al: The impact of re-transurethral resection on clinical
outcomes in a large multicentre cohort of patients with T1
high-grade/Grade 3 bladder cancer treated with bacille
Calmette-Guérin. BJU Int. 118:44–52. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Fritsche HM, Burger M, Svatek RS, Jeldres
C, Karakiewicz PI, Novara G, Skinner E, Denzinger S, Fradet Y,
Isbarn H, et al: Characteristics and outcomes of patients with
clinical T1 grade 3 urothelial carcinoma treated with radical
cystectomy: Results from an international cohort. Eur Urol.
57:300–309. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Soria F, Marra G, D'Andrea D, Gontero P
and Shariat SF: The rational and benefits of the second look
transurethral resection of the bladder for T1 high grade bladder
cancer. Transl Androl Urol. 8:46–53. 2019. View Article : Google Scholar : PubMed/NCBI
|