Introduction
Temporomandibular joint (TMJ) ankylosis refers to
immobility of the joint and is characterized by the formation of an
osseous, fibrous, or fibro-osseous mass fused to the cranial base
(1). A typical ‘bird face’
appearance is noted in cases of bilateral ankylosis with onset
during childhood (2). Restriction of
mandible movement in pediatric patients frequently leads to
physical and psychological impairments, including speech
impairment, difficulty in chewing and swallowing, rampant caries,
poor oral hygiene, facial deformity and airway obstruction.
Furthermore, the condition of micrognathia is thought to cause
obstructive sleep apnea syndrome (OSAS) due to airway obstruction
due to glossoptosis and reduced oropharyngeal space (3).
Several surgical methods have been applied to treat
patients with micrognathia and repair their bone defects. However,
mandibular distraction osteogenesis (MDO) has additional advantages
over other methods (4). MDO is able
to correct the micrognathia and relieve the airway obstruction due
to its ability to stretch the tongue and muscles attached to the
mandible forward (5). The present
study reports on a case of micrognathia and OSAS due to bilateral
TMJ ankylosis in early childhood. TMJ management combined with
simultaneous MDO was used for the treatment of this patient and the
4-year follow-up indicated optimal results.
Case report
Case presentation
A 5-year-old male patient presented with an abnormal
mandible, limited mouth opening and snoring. The cause of the TMJ
ankylosis was condylar fracture resulting from a trauma to the chin
when the patient was 2 years old. The TMJ exhibited no condylar
mobility and the intraoral condition was poor with several teeth
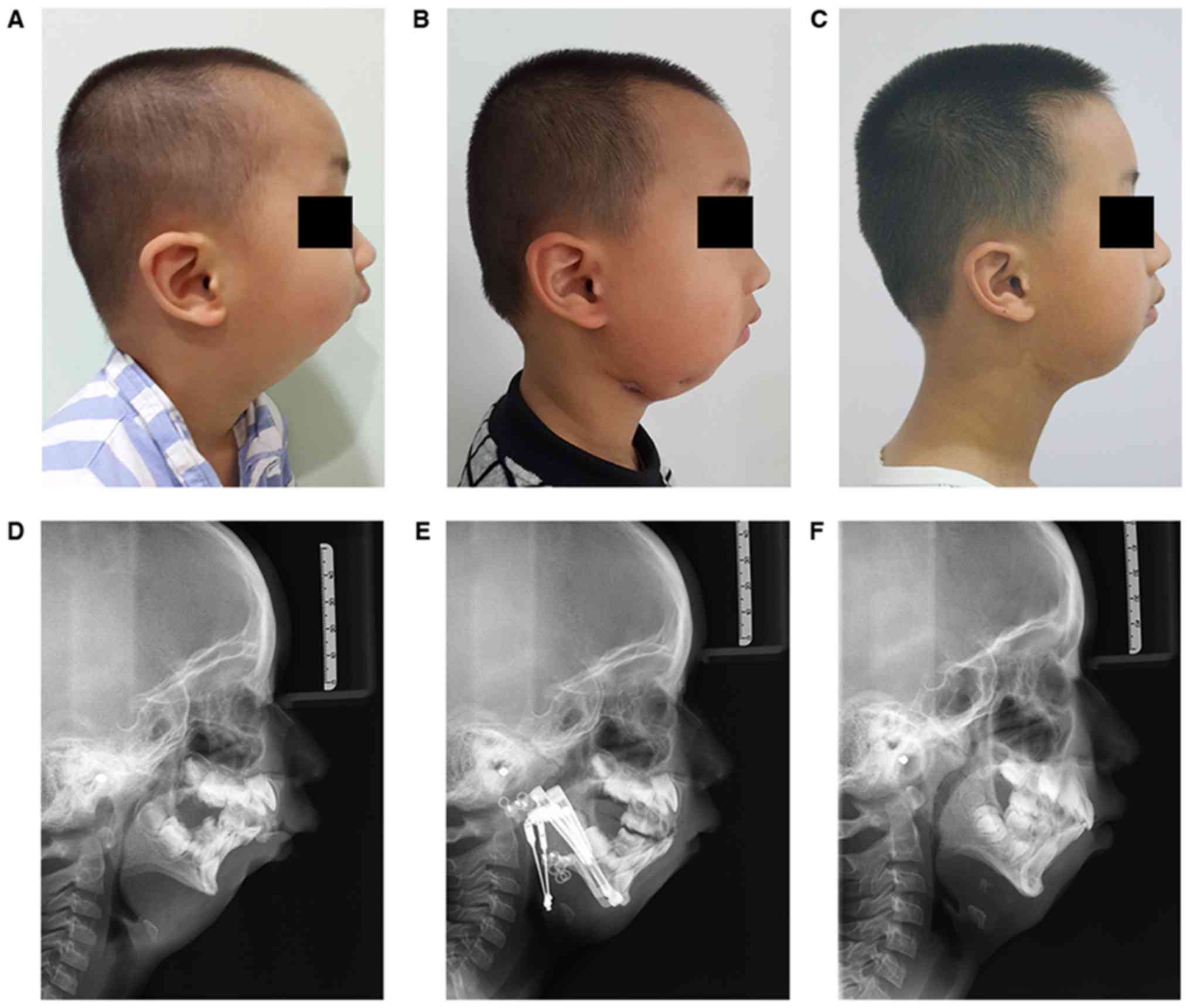
affected by caries and residual roots. A typical ‘bird face’
appearance with serious mandible retrognathism and significant
convex facial profile was noted (Fig.
1). In addition, the patient was unable to lie flat on the bed
at night, resulting in pronounced snoring. Due to poor cooperation
of the patient to perform the polysomnography test and economic
considerations, no oxygen saturation or apnea/hypopnea index data
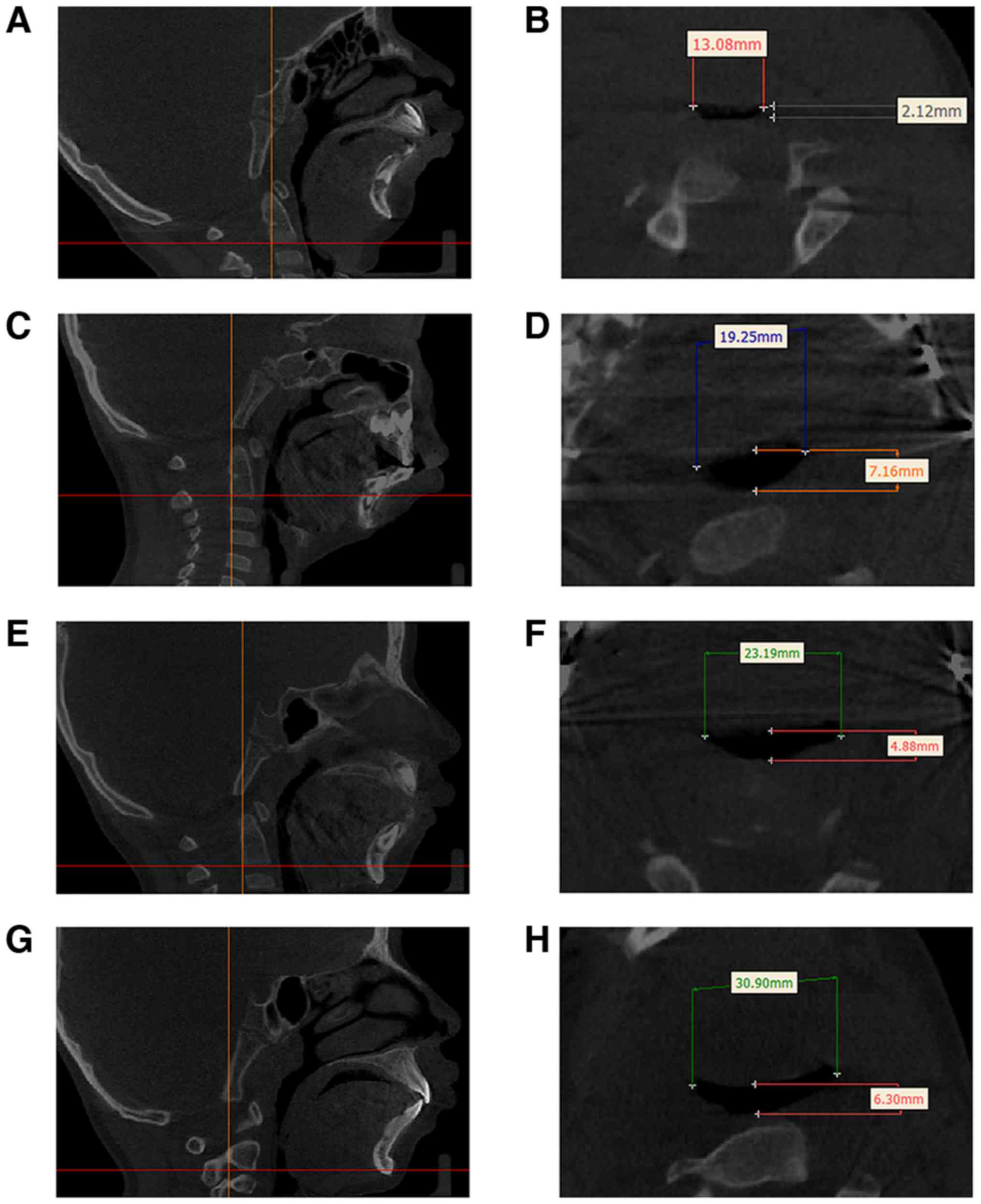
were collected. However, CT measurement was used for pharyngeal
space measurement instead of MRI estimation. On CT, the pharyngeal
space was narrow with a width of 13.08 mm and a length of 2.12 mm
in the retroglossal region (Fig. 2).
Radiological examinations confirmed a condyle deformity and the
mandible was apparently underdeveloped downward and forward.
Cephalometric analysis indicated a severe skeletal Class II
malocclusion with an angle that reflects the maxillary protrusion,
formed by the sella turcica point, nasion point and upper alveolar
point (SNA), of 79.5°; an angle that reflects the mandibular
protrusion, formed by sella turcica point, nasion point and
inferior alveolar point (SNB), of 60.1°; and an angle that reflects
the relative protrusion of maxilla and mandible, formed by the
upper alveolar point, nasion point and inferior point (ANB) of
19.4°. A severely hypoplastic mandible and chin with a facial angle
of 67.8° and a Y-axis angle of 73.1° were also observed (Table I). The diagnosis was TMJ ankylosis,
micrognathia and OSAS. A cephalometric map used for the
measurements is provided in Fig. 3.
Calculation of the pharynx diameters was accomplished by using the
software Mimics Research version 20.0 (Materialise Corp.). The same
slice was identified by the lower border of the second cervical
centrum, which was the middle part of the oropharynx and the
narrowest point of the pharyngeal airway in this patient. Repeated
evaluations were performed for a total of three or four times for
each measure to obtain the average value and statistical analysis
was not applicable to this study.
 | Figure 3.Cephalometric analysis. Landmarks of
the hard tissue: S, sella turcica point; N, nasion point; A, upper
alveolar point; B, inferior alveolar point; Pog, pogonion; Gn,
gnathion; Co, condyle point. Landmarks of the soft tissues: Li,
labium; Pog′, pogonion of the soft tissue; Me′, menton of the soft
tissue; FH, Frankfort horizontal plane; 0-degree meridian, a line
passing through the nasion that is perpendicular to the FH
plane. |
 | Table I.Cephalometric analysis throughout the
distraction process. |
Table I.
Cephalometric analysis throughout the
distraction process.
| Measurement | Pre-treatment: Age, 5
years and 5 months | 3 months after
mandibular DO: Age, 5 years and 8 months | Post-treatment: Age,
9 years and 4 months | Normal value on mixed
dentitiona |
|---|
| Angle (°) |
|
|
|
|
| SNA | 79.5 | 80.1 | 80.3 | 82.3±3.5 |
| SNB | 60.1 | 67.0 | 68.6 | 77.6±2.9 |
| ANB | 19.4 | 13.1 | 11.7 | 4.7±1.4 |
| Facial
angle | 67.8 | 73.6 | 77.8 | 83.1±3.0 |
| Y-axis
angle | 73.1 | 70.4 | 69.9 | 65.5±2.9 |
|
Li-Pog′-throat angle | 175.6 | 161.7 | 159.6 | 110.0±8.0 |
| Linear distance
(mm) |
|
|
|
|
|
Co-Gn | 62.4 | 69.0 | 80.1 | – |
|
Me′-throat length | 24.4 | 27.3 | 30.8 | 42.0±6.0 |
| Chin
projection | −26.9 | −21.0 | −17.4 | 0±2.0 |
Treatment procedure
The protocol by Kaban et al (6) was followed during the initial surgery.
The first step was TMJ arthroplasty by condylectomy and
simultaneous MDO, with bilateral coronoidectomy if required. During
the procedure, the surgeons concluded that the normal TMJ
architecture and intact disc had not been retained and that the
ankylotic mass was fused to the skull base. Subsequently, a
specimen of 15 mm in length of the ankylosed condyle was excised at
the level below the condyle neck. The maximal opening measured 35
mm after completion of the excision. To avoid recurrence of
ankylosis, a Dacron patch (Chester Healthcare Technology Co., Ltd)
was sutured to the soft tissue. The use of a temporalis muscle
fascia flap was avoided following condylectomy.
An individualized 3D-printed model (Cibei Medical
Treatment Appliance Co., Ltd) was constructed prior to the surgery
and the osteotomy line was accurately designed on the mandible
model in order not to injure the teeth buds. The osteotomy line was
designed on the mandible angle to create a transport disc so that
distractors were able to vertically lengthen the ramus height and
sagittal plane, leading to a concomitant extension of the
mandibular body. Cutting guides were also designed to fit on the
mandible model in order to reproduce the planned osteotomy.
Therefore, the parallel placement of the distraction devices was
ensured by the same slots, which were designed on the cutting
guides and devices. During the surgery, the corresponding screw
holes were initially drilled on the bone in order to determine the
positions of the distractors. Subsequently, the corticotomy was
achieved in the mandibular angle. Finally, the internal distractors
(Cibei Medical Treatment Appliance Co., Ltd) were fixed to the
transport disc and mandibular body with screws, lengthening the
ramus height and mandibular body.
After a latency period of 3 days, the distractors
were activated three times daily by a 0.4-mm turn. The duration of
distraction lasted for 13 days until the anterior overjet
disappeared and the anterior teeth exhibited a 2-mm crossbite. The
total extracted length was 15.6 mm. Physical training was initiated
from the day when distractors were applied and a T-shaped opener
was provided to the patient in order to aid with the training of
the mouth opening. The patient's snoring symptoms were relieved
immediately following surgery. Airway enlargement was evident on CT
scans after the distraction period (Fig.
2D). The transverse view of CT scans indicated that the pharynx
diameters were increased to 23.95 mm (width) and 7.70 mm (length).
These were considerably greater than those determined prior to the
operation (13.08×2.12 mm).
Treatment and outcomes at the 1-year
follow-up
No complications of toothache, wound infection or
loosing of devices were reported. During removal at 1 year, it was
noted that the distractors were still fixed in a good position and
the screws were stable. According to the surgery record, the actual
regeneration length was 15.5 mm. The patient reported significant
improvement with sleep problems as a result of the increase in the
oropharyngeal airway. The distractors were removed following the
consolidation period. The ‘bird face’ appearance was improved
(Fig. 1B-E). Cephalometric
measurements demonstrated that the SNB was increased to 67.0°, the
ANB was decreased to 13.1°, the facial angle was increased to 73.6°
and the Y-axis angle was decreased to 70.4°. CT scans indicated
further enlargement of the upper airway diameters that were
estimated at 23.95 mm in width and 7.70 mm in length (Fig. 2F). However, the maximal incisal
opening (MIO) returned to 11 mm at 1 year following condylectomy,
since the patient was unwilling to endure the pain during mouth
opening exercises. In order to obtain a larger opening capacity, a
coronoidectomy was performed and the passive MIO reached to 30 mm
following the completion of the surgery. Mouth-opening exercises
were strongly recommended for the patient.
Outcomes at 4-year follow-up
The patient's lateral view improvement was basically
maintained at 4 years following distraction (Fig. 1C). New articulation was eventually
formed between the glenoid fossa and the transport segment
following remodeling of this structure. The snoring symptom of the
OSAS was resolved to a great extent. Cephalometric evaluation
indicated significant improvements of the mandible atrophy
(Fig. 1F) with an SNA of 80.3°, an
SNB of 68.6° and an ANB of 11.7°. The facial angle increased to
77.8° and the Y-axis angle decreased to 69.9°. CT results indicated
an enlarged pharynx space with a transverse diameter of 30.9 mm in
width and 6.30 mm in length (Fig.
2H). However, the patient's MIO was estimated to 14 mm and 17
mm for the active and passive state, respectively. There was a
certain degree of MIO shrinkage in the patient. The present MIO
result did not reach the optimal expected outcome due to the lack
of physical training and poor compliance. The patient had no
regular follow-up schedule due to the long journey from his
residency to the hospital. Therefore, further physiotherapy with
good compliance were required for the patient.
Discussion
The present study describes a case of pediatric
bilateral TMJ ankylosis and severe secondary micrognathia and OSAS.
In this patient, TMJ ankylosis occurred at a young age as a result
of mandibular trauma and caused severe facial deformity and airway
obstruction. In addition to the growth, the patient was burdened
with severe functional and aesthetic malformations that may
adversely affect his social and psychological development (7). Therefore, it has been proposed that
early treatment of ankylosis is necessary to avoid secondary
deformities (6,7). In the present case, condylectomy was
performed at the age of 5. The patient was of sufficient age to
cooperate with post-operative physiotherapy. However, the patient's
MIO indicated limited improvement following treatment, due to poor
compliance. Therefore, the study suggested that, although early
surgical treatment is essential for pediatric patients with
ankylosis, patient compliance, family support and the financial
burden should also be considered during the selection of the
appropriate time for surgical correction. Early post-operative
exercise, active physiotherapy and stringent follow-up are
essential to prevent post-operative shrinkage and adhesions in TMJ
ankyloses. The motivation to perform active mouth opening training
and tolerance of discomfort are considered key factors in
determining successful maintenance of post-operative mouth opening
(8).
The purpose of MDO in the present case study
included the correction of craniofacial deformities and the
resolution of OSAS. The mandibular lengthening obtained by gradual
distraction may result in expansion of the mandibular bony tissue
and in proportional and harmonic modification of the muscles and
the surrounding soft tissues (9).
However, whether distraction should be performed at the time of TMJ
management remains controversial. Certain surgeons prefer to first
restore the jaw movements and address the secondary facial
deformities afterwards (10),
whereas others perform the distraction first, followed by TMJ
management at the second stage (11). The selection of different surgical
methods is based on specific factors. Lopez and Dogliotti (10) suggested that the MDO should be
performed following arthroplasty, as the growth potential of the
mandible is only realized when the ankylosis has been relieved.
However, Sadakah et al (11)
recommended postponing the release of the ankylosed joint following
bilateral distractions, since it is more advantageous in preventing
rotation and upward movement of the condylar segment during the
course of the distraction. In contrast to this type of treatment,
it has been proposed by surgeons to attempt simultaneous correction
of all deformities by performing distraction during ankylotic mass
removal following the introduction of distraction osteogenesis for
mandibular lengthening (12).
Simultaneous arthroplasty and MDO enable the production of a
neocondyle and allow for concomitant correction of facial
malformations. The treatment outcomes of pre-arthroplastic
distraction and simultaneous arthroplastic distraction have been
previously compared and it was concluded that the two methods were
effective in correcting the aesthetics of the patients and
functional movement of the TMJ (13). Papageorge and Apostolidis (14) were the first to perform simultaneous
gap arthroplasty and MDO for the treatment of micrognathia in
ankyloses of the TMJ in 1999; as a result, mouth opening was
improved and facial deformity was corrected. Eski et al
(15) reported on three patients
with TMJ ankylosis associated with facial asymmetry, who were
treated with gap arthroplasty and simultaneous distraction. As a
result, TMJ ankylosis was released and bone regeneration was
achieved (15). This method used for
TMJ ankylosis resulted in reduced treatment time and economic
burden of the patients, whereas it eliminated the requirement for
additional surgery. However, the shortcomings of this procedure are
that following release of the ankylotic block, the changes in the
mandibular position cannot be completely controlled during the
distraction period (12). It must be
emphasized that the selection of the surgical procedure depends on
the specific condition of the patient, including the type of
ankylosis, the severity of mandible dysplasia, the airway
obstruction, the patient's age and the family's financial status.
Further studies with larger sample sizes are required.
Precision device placement is vital to avoid
iatrogenic deformities or surgical failure. In the present case,
the accurate osteotomy was guaranteed by using a 3-D printed
pre-operative model and a surgical cutting guide. Improvements in
the appearance and airway obstruction were apparent. However, it
has been reported that the distracted mandible exhibits a period of
relapse and usually does not exhibit a ‘catch-up’ growth compared
with the residual somatic growth of the face (16). To achieve optimal appearance and
respiratory function, mandibular distraction may be combined with
other surgical techniques, e.g. instance genoplasty (17). Mandibular distraction may further
correct the 3-D skeletal deficiencies in patients with micrognathia
deformity and achieve an ideal surgical effect.
In conclusion, TMJ management with simultaneous
mandible distraction is an effective method to improve mandibular
movement restrictions, airway obstructions and micrognathia. MDO
has a versatile role in the treatment process. Patients with
childhood onset require early surgical treatments to avoid
secondary malformations. However, poor compliance with
post-surgical physiotherapy is likely to lead to a limited range of
motion following surgery.
Acknowledgements
Not applicable.
Funding
The present study was financially supported by a
grant from the National Natural Science Foundation of China (grant
no. 81070818).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request
Authors' contributions
XY collected, analyzed and interpreted the patient
data and was a major contributor in writing the manuscript. JW
performed the surgical treatment of the patient and drafted the
manuscript. SH contacted the patient and organized return visits
and analyzed the patient data. RZ was responsible for acquisition
of data and drafting and revising the manuscript. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient's parents for publication of this case report and
accompanying data and images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
TMJ
|
temporomandibular joint
|
|
OSAS
|
obstructive sleep apnea syndrome
|
|
MDO
|
mandibular distraction
osteogenesis
|
|
MIO
|
maximal incisal opening
|
References
|
1
|
Elgazzar RF, Abdelhady AI, Saad KA,
Elshaal MA, Hussain MM, Abdelal SE and Sadakah AA: Treatment
modalities of TMJ ankylosis: Experience in Delta Nile, Egypt. Int J
Oral Maxillofac Surg. 39:333–342. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chidzonga MM: Temporomandibular joint
ankylosis: Review of thirty-two cases. Br J Oral Maxillofac Surg.
37:123–126. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bookman LB, Melton KR, Pan BS, Bender PL,
Chini BA, Greenberg JM, Saal HM, Taylor JA and Elluru RG: Neonates
with tongue-based airway obstruction: A systematic review.
Otolaryngol Head Neck Surg. 146:8–18. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Breik O, Tivey D, Umapathysivam K and
Anderson P: Mandibular distraction osteogenesis for the management
of upper airway obstruction in children with micrognathia: A
systematic review. Int J Oral Maxillofac Surg. 45:769–782. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Karp NS, Thorne CH, McCarthy JG and
Sissons HA: Bone lengthening in the craniofacial skeleton. Ann
Plast Surg. 24:231–237. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kaban LB, Bouchard C and Troulis MJ: A
protocol for management of temporomandibular joint ankylosis in
children. J Oral Maxillofac Surg. 67:1966–1978. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Resnick CM: Temporomandibular joint
reconstruction in the growing child. Oral Maxillofac Surg Clin
North Am. 30:109–121. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gupta H, Tandon P, Kumar D, Sinha VP,
Gupta S, Mehra H and Singh J: Role of coronoidectomy in increasing
mouth opening. Natl J Maxillofac Surg. 5:23–30. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yu H, Shen G, Zhang S and Wang X: Gap
arthroplasty combined with distraction osteogenesis in the
treatment of unilateral ankylosis of the temporomandibular joint
and micrognathia. Br J Oral Maxillofac Surg. 47:200–204. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
López EN and Dogliotti PL: Treatment of
temporomandibular joint ankylosis in children: Is it necessary to
perform mandibular distraction simultaneously? J Craniofac Surg.
15:879–884; discussion 884–885. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sadakah AA, Elgazzar RF and Abdelhady AI:
Intraoral distraction osteogenesis for the correction of facial
deformities following temporomandibular joint ankylosis: A modified
technique. Int J Oral Maxillofac Surg. 35:399–406. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sharma A, Paeng JY, Yamada T and Kwon TG:
Simultaneous gap arthroplasty and intraoral distraction and
secondary contouring surgery for unilateral temporomandibular joint
ankylosis. Maxillofac Plast Reconstr Surg. 38:122016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chellappa AL, Mehrotra D, Vishwakarma K,
Mahajan N and Bhutia DP: Pre-arthroplastic and simultaneous
mandibular distraction for correction of facial deformity in
temporomandibular joint ankylosis. J Oral Biol Craniofac Res.
5:153–160. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Papageorge MB and Apostolidis C:
Simultaneous mandibular distraction and arthroplasty in a patient
with temporomandibular joint ankylosis and mandibular hypoplasia. J
Oral Maxillofac Surg. 57:328–333. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Eski M, Deveci M, Zor F and Sengezer M:
Treatment of temporomandibular joint ankylosis and facial asymmetry
with bidirectional transport distraction osteogenesis technique. J
Craniofac Surg. 19:732–739. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Peacock ZS, Salcines A, Troulis MJ and
Kaban LB: Long-term effects of distraction osteogenesis of the
mandible. J Oral Maxillofac Surg. 76:1512–1523. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yin L, Tang X, Shi L, Yin H and Zhang Z:
Mandibular distraction combined with orthognathic techniques for
the correction of severe adult mandibular hypoplasia. J Craniofac
Surg. 25:1947–1952. 2014. View Article : Google Scholar : PubMed/NCBI
|