Introduction
As one of the serious and end-point events of
various common heart diseases (1),
chronic heart failure (CHF) is the leading cause of death among the
elderly worldwide. Studies have shown that 915,000 patients with
first-episode heart failure (HF) were diagnosed in the United
States in 2012 (2,3), and ~20% of people >40 years of age
will develop HF (4). An Italian
study (5) has shown that 81.1% of
1,623 subjects aged 65–84 years had preclinical HF. The high cost
of health care brought by HF is a heavy burden on patients and
society (6). The above research data
indicate that the high incidence, high prevalence and high
mortality of HF is still a social problem, and its diagnosis and
treatment are increasingly valued by society.
Galectin-3 (Gal-3) and microRNA (miR) have attracted
increasing attention in recent years. Studies have found that Gal-3
can cause myocardial fibrosis (7),
and the higher the concentration of Gal-3, the more severe the
myocardial fibrosis (8). Cardiac
fibrosis is a decisive factor in the progression of cardiovascular
disease to HF. In 2012, the American College of Cardiology
Foundation recommended Gal-3 as a fibrosis biomarker (9). However, Gal-3 also has limitations in
the diagnosis of CHF. The pathophysiological mechanism and
biological half-life in the human body are not fully understood,
and they are also expressed in various immune diseases or
inflammation (10). Moreover, the
specificity is low leading to different diagnostic results.
Therefore, seeking a new diagnostic marker has attracted increasing
attention. As a short non-coding RNA with a length of ~22
nucleotides, miR's main function is to affect the stability or
inhibit the translation of mRNA by binding all or part of the
non-translation region of its downstream target gene mRNA 3′
terminal, and participates in the physiological and pathological
processes of cells in the body. Recent studies have found that
numerous heart diseases are regulated by miRs (11,12).
Circulating miR is expected to be used for the diagnosis and
prognosis in HF, and several miRs are involved in important
mechanisms that lead to HF, such as hypertrophy and fibrosis
(13). In 2008, Lawrie et al
(14) presented for the first time
that miR could stably exist in human serum, and circulating miR has
great potential in being a biochemical marker of cardiovascular
diseases (15). miR-214 is a member
of miR family. The study by van Rooij et al (16) showed that the level of miR-214 in
patients with dilated cardiomyopathy with HF was significantly
higher than that in healthy subjects, suggesting that its clinical
significance could be studied according to its expression in the
peripheral blood serum of patients with CHF.
In the present study, the expression of miR-214 and
Gal-3 in the peripheral blood of patients with CHF was detected and
their diagnostic and efficacy prediction values were studied,
providing new clinical diagnostic indicators for CHF.
Patients and methods
General data
A total of 50 cases of CHF patients, diagnosed and
treated in Shanghai Xuhui Central Hospital (Shanghai, China) from
January 2017 to March 2018, were assigned in the study group, and
30 cases of healthy subjects who underwent physical examination
during the same period were assigned in the control group. All test
indexes of the healthy subjects were normal. The study was approved
by the Ethics Committee of Shanghai Xuhui Central Hospital. Signed
informed consents were obtained from the patients or the
guardians.
Inclusion and exclusion criteria
Inclusion criteria
Patients diagnosed with heart failure for more than
half a year, according to the diagnostic criteria of the ESC
Guidelines for the diagnosis and treatment of acute and chronic
heart failure 2012 (17); patients
treated in the specific hospital; patients with complete clinical
data; and patients who were informed and signed an informed consent
form.
Exclusion criteria
Patients >80 years of age or <50 years of age;
patients with partial absence of clinical data; and patients with
myocardial infarction within 3 months, communication disorder,
malignant tumor, impaired liver and kidney function, severe
infection or mental dysfunction.
Therapy of patients in the observation
group
Patients received conventional treatment and were
given Enalapril maleate tablets orally, 10 mg/time, 1 time/day;
Metoprolol sustained-release tablet (Southwest Pharmaceutical Co.,
Ltd.) orally, with initial dose of 6.25 mg/time, 2 times/day, and
then the weekly dose was doubled, not exceeding, however, the dose
of 400 mg/day; Spironolactone tablet (Beijing zhongxin
pharmaceutical factory) orally, 20 mg/time, 1 time/day.
Sample collection and determination
Sample collection
A total of 3 ml of venous blood were taken from the
enrolled CHF patients on an empty stomach, on the second day of
admission in the morning, and then after 6 months of treatment.
Similar blood samples were collected from the patients of the
control group, and were left at room temperature for 30 min and
centrifuged at 2,800 × g for 10 min. The supernatant was absorbed
and stored in a refrigerator at −80°C for centralized
detection.
RT-qPCR detection of miR-214
expression in serum
Total RNA of the collected serum was extracted with
TRIzol kit (15596018; Invitrogen; Thermo Fisher Scientific, Inc.).
The purity, concentration and integrity of total RNA were detected
by UV spectrophotometry and agarose gel electrophoresis. TaqMan
Reverse Transcription kit (N8080234; Invitrogen; Thermo Fisher
Scientific, Inc.) was used for reverse transcription according to
the manufacturer's instructions. The reaction volume was 15 µl, and
the temperature protocol was 16°C for 30 min, 42°C for 30 min, 85°C
for 5 min, and 4°C until the end. cDNA was collected for PCR
amplification. miR-214 forward, 5′-GATACTCACTTTTTGCGGTCT-3′ and
reverse, 5′-GTGCAGGGTCCGAGGT-3′; U6 forward,
5′-CGCTTCGGCAGCACATATAC-3′ and reverse, 5′-CAGGGGCCATGCTAATCTT-3′.
The amplification system of qPCR was as follows: cDNA 1 µl, forward
primer 0.4 µl, reverse primer 0.4 µl, 2X TransStart®
Green qPCR SuperMix UDG (AQ111-01, Transgen Biotech Co., Ltd.) 10
µl, Passive Reference Dye (50X) (optional) 0.4 µl, and
nuclease-free water was added for a final volume of 20 µl. qPCR
amplification conditions were as follows: Incubation at 94°C for 10
min, pre-denaturation at 94°C for 5 sec, annealing and extension at
60°C for 30 sec, with a total of 40 cycles. Each sample was set
with 3 duplicate wells, and the experiment was carried out 3 times.
In this study, U6 was used as the internal reference gene and
2−∆∆Cq method was used to analyze the data (18).
ELISA in detection of Gal-3 expression
in serum
Serum Gal-3 was detected by Human Galectin-3
enzyme-linked immunosorbent assay (ELISA) kit (cat no. KE00126;
ProteinTech Group, Inc.). Specific Gal-3 antibodies were pre-coated
on a 96-well microplate adding standard and test samples to the
micropores, respectively, and setting up a blank well at the same
time. Biotinylated Gal-3 antibody was added to the micropores, and
then the micropores were washed thoroughly to remove unbound
biotinylated antibody. HRP-labeled avidin was added, the micropores
were washed again, and TMB substrate (ProteinTech Group, Inc.) was
added for color development. TMB turned blue under catalysis and
turned yellow under the action of acid. The absorbance (OD value)
was measured by ELISA at a wavelength of 450 nm, and the
corresponding concentration was converted using a standard
curve.
Observational indexes
Main observational indexes
The expression levels of miR-214 and Gal-3 in the
peripheral blood of patients with CHF were compared between the
observation and control group. Their correlation and diagnostic
value for CHF were also studied.
Secondary observational indexes
miR-214 and Gal-3 expression levels were compared
before and after treatment, and regarding the clinical curative
effect. Patients were divided into a good curative effect group
(significant effect) and a poor curative effect (effective +
invalid effect) according to the clinical efficacy. The expression
levels of Gal-3 and miR-214 in the two groups after treatment were
compared. ROC curve analysis was performed to observe their
predictive value in curative effect, and Pearson's correlation
analysis was carried out to detect the correlation between miR-214
and Gal-3 expression levels.
Efficacy assessment criteria
After 6 months of treatment, the curative effect of
50 patients was evaluated according to the classification of the
New York Heart Association (NYHA), as shown in Table I.
 | Table I.NYHA classification. |
Table I.
NYHA classification.
| Curative effect | Efficacy assessment
criteria |
|---|
| Significantly
effective | Main clinical
symptoms and signs of HF disappeared and cardiac functions improved
≥2 levels |
| Effective | Heart functions
improved 1 level |
| Invalid | Heart functions
improved <1 level |
Statistical analysis
SPSS 20.0 software package (Cabit Information
Technology Co., Ltd.) was used for the statistical analysis of the
collected data. GraphPad Prism 7 (Softhead, Inc.) was used to
generate the graphs. Measurement data were expressed as the mean ±
SD. Independent samples t-test was used for their comparisons
between two groups, and paired t-test for comparisons between two
groups before and after treatment. Chi-square test was used for the
comparison of nominal data between two groups. ROC curves were
drawn to evaluate the diagnostic and efficacy prediction value of
miR-214 and Gal-3 in CHF. Pearson's correlation analysis was
carried out for the correlation of miR-214 and Gal-3 expression
levels. P<0.05 was considered to indicate a statistically
significant difference.
Results
Comparison of clinical data
The results revealed that there was no statistical
difference in the basic clinical data between the two groups
(P>0.05). Details are shown in Table
II.
| Table II.Baseline data. |
Table II.
Baseline data.
| Factors | Observation group
(n=50) | Control group
(n=30) | t/χ2
value | P-value |
|---|
| Age (years) |
62.8±8.5 |
60.8±8.4 | 1.023 | 0.309 |
| Gender |
|
|
|
|
| Male | 27 (54.00) | 16 (53.33) | 0.003 | 0.954 |
|
Female | 23 (46.00) | 14 (46.67) |
|
|
| Smoking
history |
|
|
|
|
|
Yes | 24 (48.00) | 13 (43.33) | 0.164 | 0.685 |
| No | 26 (52.00) | 17 (56.67) |
|
|
| BMI
(kg/m2) | 23.94±1.99 | 24.38±2.03 | 0.950 | 0.345 |
| Fasting blood
glucose (mmol/l) |
5.91±1.33 |
5.60±1.74 | 1.157 | 0.250 |
| ALT (U/l) | 18.71±5.81 | 18.32±5.87 | 0.400 | 0.690 |
| AST (U/l) | 21.47±6.20 | 20.13±5.62 | 1.315 | 0.191 |
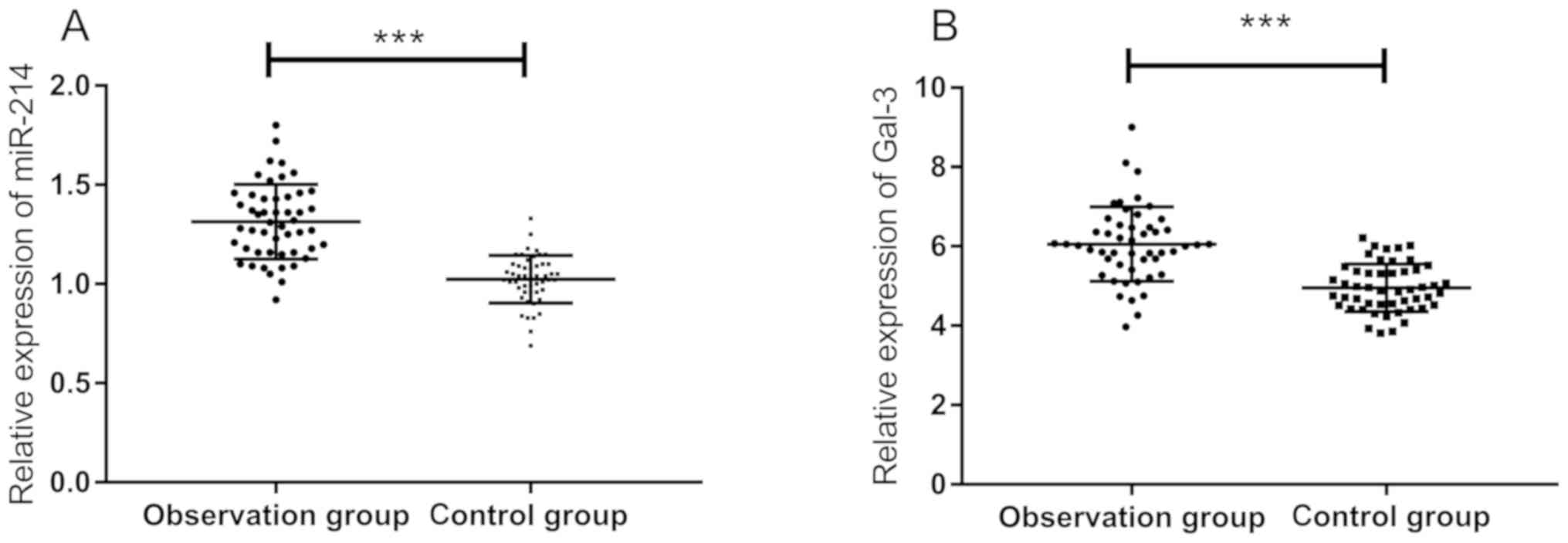
Expression of miR-214 and Gal-3 in the
serum of patients in the two groups
By comparing the relative expression of miR-214 and
Gal-3 in the serum of patients in the two groups before treatment,
it was found that the serum expression of miR-214 in the
observation group (1.32±0.18) was significantly higher than that in
the control group (1.03±0.12), and the expression of Gal-3 in the
observation group (6.15±0.78 ng/ml) was significantly higher than
that in the control group (4.78±0.63 ng/ml) (P<0.001) (Fig. 1).
Diagnostic value of miR-214 and Gal-3
in CHF patients
The expression of the two indexes before treatment
was used to draw the ROC curves. The results revealed that the area
under curve (AUC) of miR-214 was 0.916 (95% CI, 0.861–0.971), the
sensitivity was 92%, the specificity was 74%, Youden index was 72%,
and the cut-off value was <1.165. The AUC of Gal-3 was 0.852
(95% CI, 0.776–0.927), the sensitivity was 88%, the specificity was
72%, Youden index was 62%, and the cut-off value was <5.68
(Fig. 2).
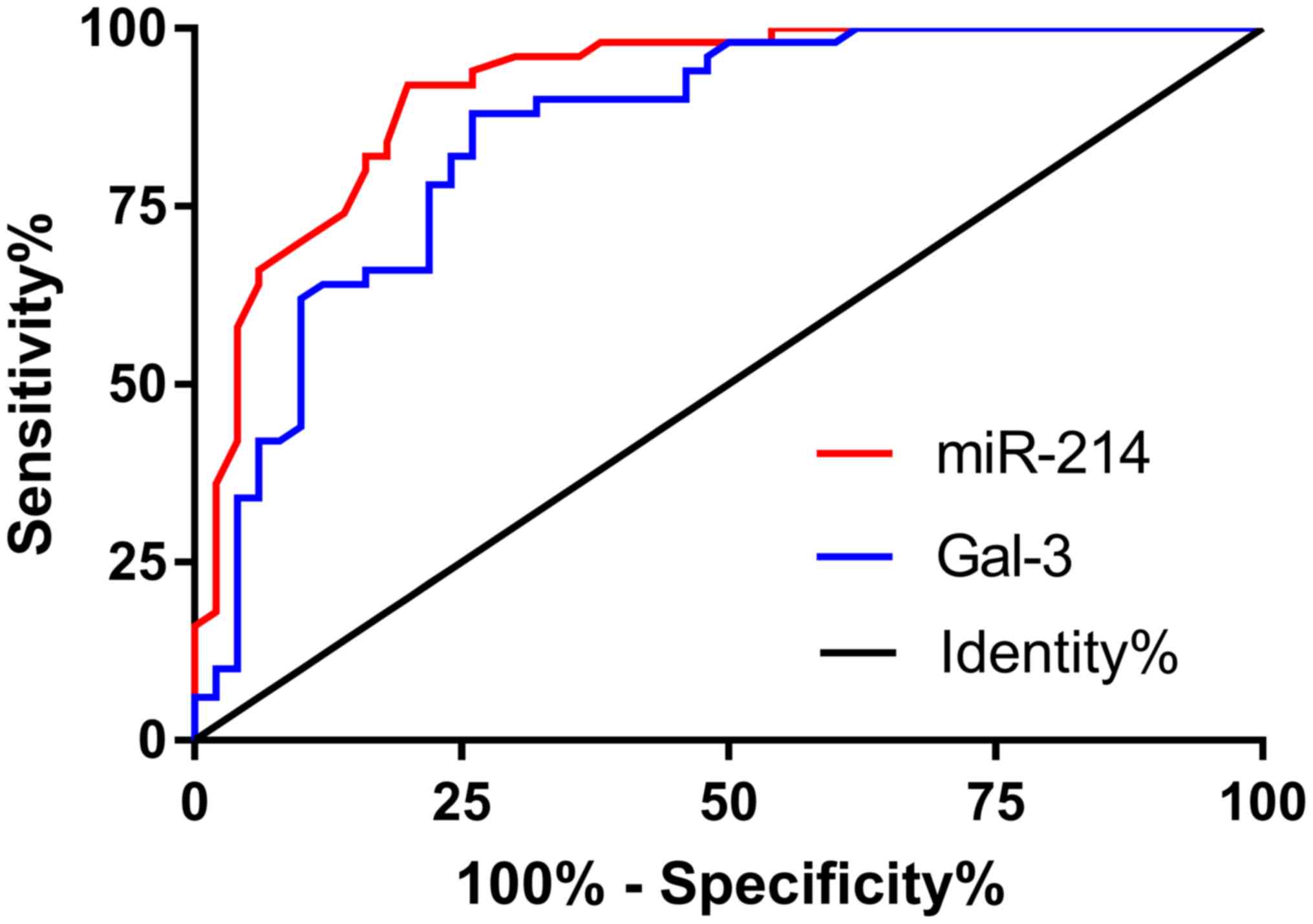 | Figure 2.ROC curves of miR-214 and Gal-3 in CHF
diagnosis. Red line is the ROC curve of miR-214. AUC, 0.916 (95%
CI, 0.861–0.971); sensitivity, 92%; specificity, 74%; Youden index,
72%; cut-off value, <1.165. Blue line is the ROC curve of Gal-3.
AUC, 0.852 (95% CI, 0.776–0.927); sensitivity, 88%; specificity,
72%; Youden index, 62%; cut-off value, <5.68. miR-214,
microRNA-214; Gal-3, galectin-3; CHF, chronic heart failure; AUC,
area under curve. |
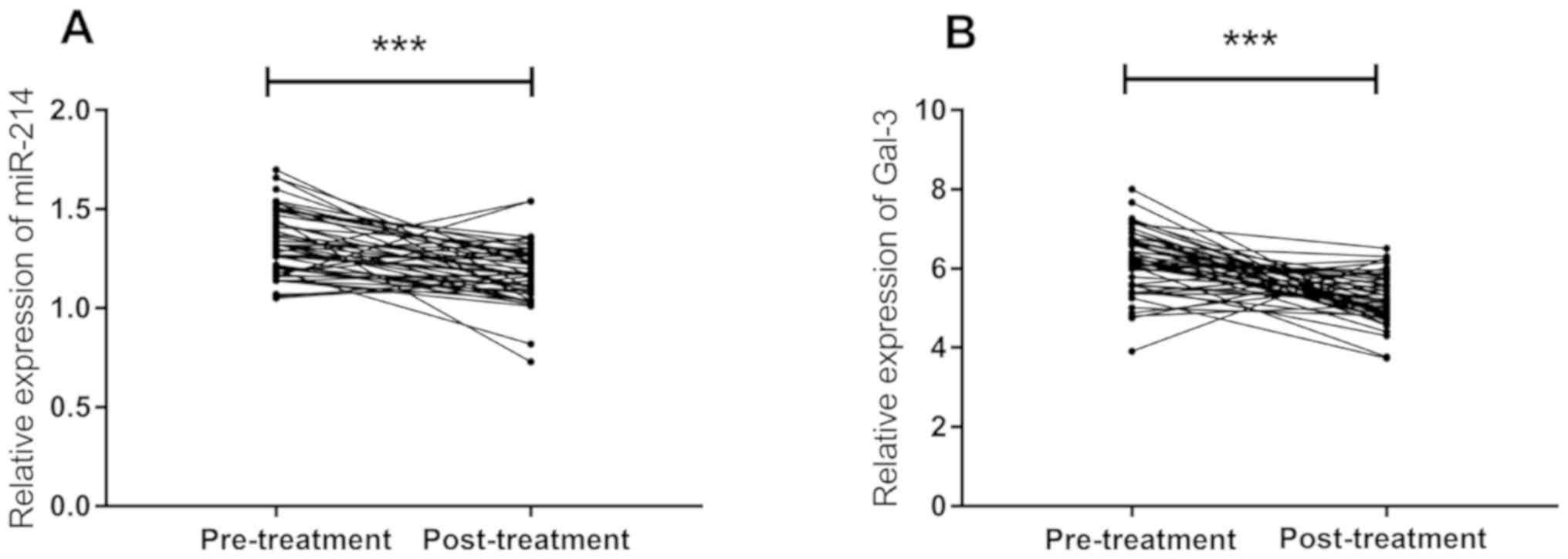
Relative expression of miR-214 and
Gal-3 before and after treatment
The changes in the relative expression of miR-214
and Gal-3 in the observation group, before and after treatment were
compared. The results revealed that the expression of miR-214
(1.17±0.14) and Gal-3 (5.31±0.54 ng/ml) in the serum of patients in
the observation group was significantly decreased after treatment,
and there was a significant difference compared with that before
treatment (P<0.001) (Fig. 3).
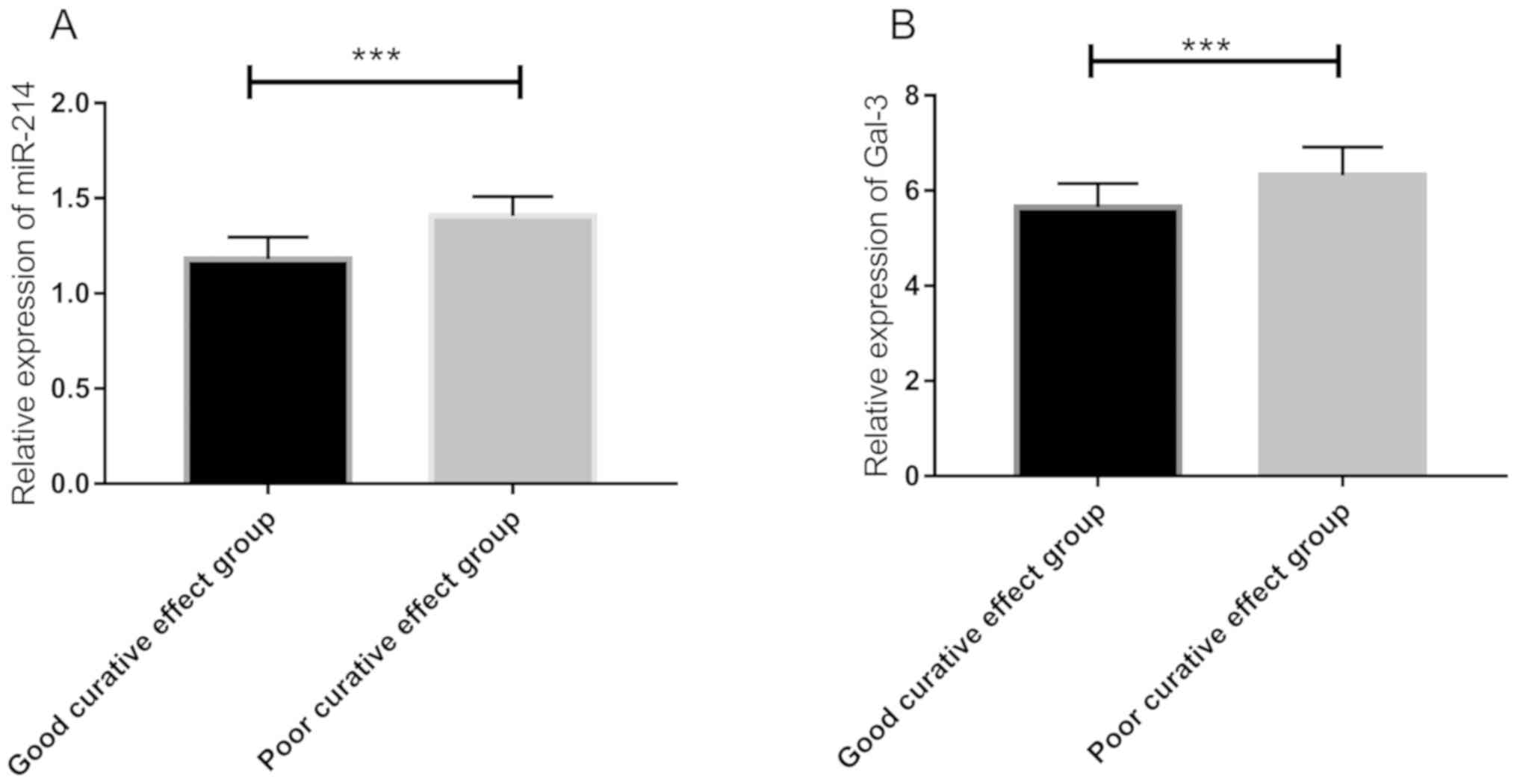
Association of the expression of
miR-214 and Gal-3 with clinical efficacy
The recent clinical efficacy was assessed. After
treatment, there were 19 patients with significantly effective, 27
patients with effective, and 4 patients with invalid effect.
According to clinical efficacy, the patients were divided into a
group with good efficacy (significant effect, 19 patients) and a
group with poor efficacy (effective + invalid effect, 31 patients).
By comparing the expression of miR-214 and Gal-3 after treatment,
it was found that the expression of miR-214 in the group with good
efficacy (1.173±0.097) was significantly lower than that in the
group with poor efficacy (1.400±0.179) after treatment, and the
expression of Gal-3 in the group with good efficacy (5.352±0.608
ng/ml) was significantly lower than that in the group with poor
efficacy (6.487±0.839 ng/ml) after treatment (P<0.001) (Fig. 4). Subsequently, ROC curve analysis of
miR-214 and Gal-3 expression after treatment in the group with good
efficacy and the group with poor efficacy showed that the AUC of
miR-214 was 0.874 (95% CI, 0.771–0.976), with sensitivity of
77.42%, specificity of 100%, Youden index of 77.42%, and cut-off
value of >1.315. The AUC of Gal-3 was 0.897 (95% CI,
0.812–0.982), with sensitivity of 77.42%, specificity of 94.74%,
Youden index of 72.16%, and cut-off value of >6.03 (Fig. 5).
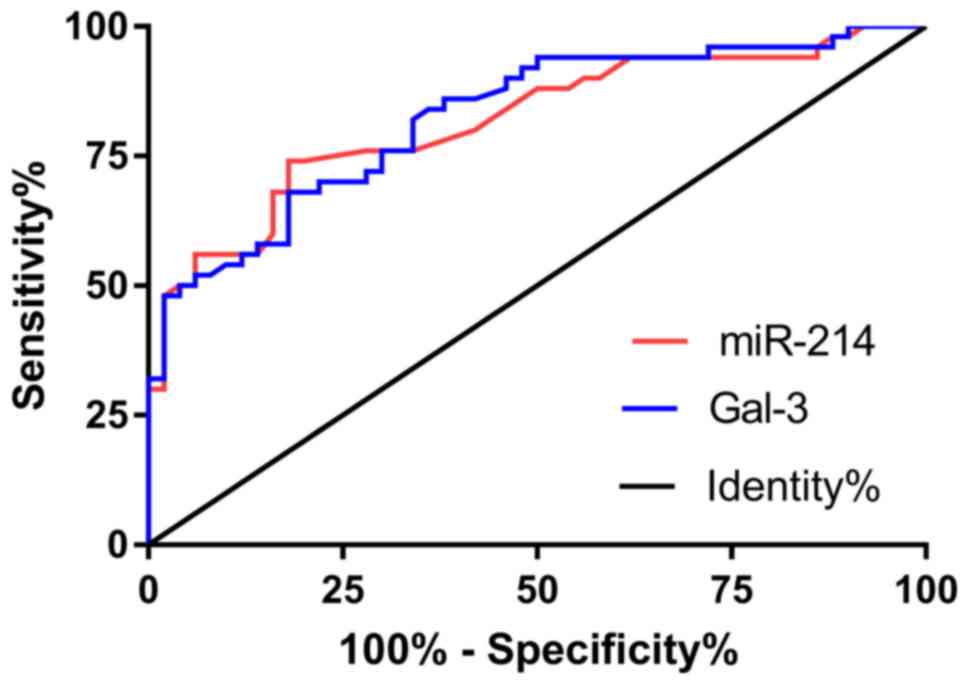 | Figure 5.ROC curves of efficacy prediction
value of miR-214 and Gal-3. Red line is the ROC curve of miR-214.
AUC, 0.874 (95% CI, 0.771–0.976); sensitivity, 77.42%; specificity,
100%; Youden index, 77.42%; cut-off value, >1.315. Blue line is
the ROC curve of Gal-3. AUC, 0.897 (95% CI, 0.812–0.982);
sensitivity, 77.42%; specificity, 94.74%; Youden index, 72.16%;
cut-off value, >6.03. miR-214, microRNA-214; Gal-3, galectin-3;
AUC, area under curve. |
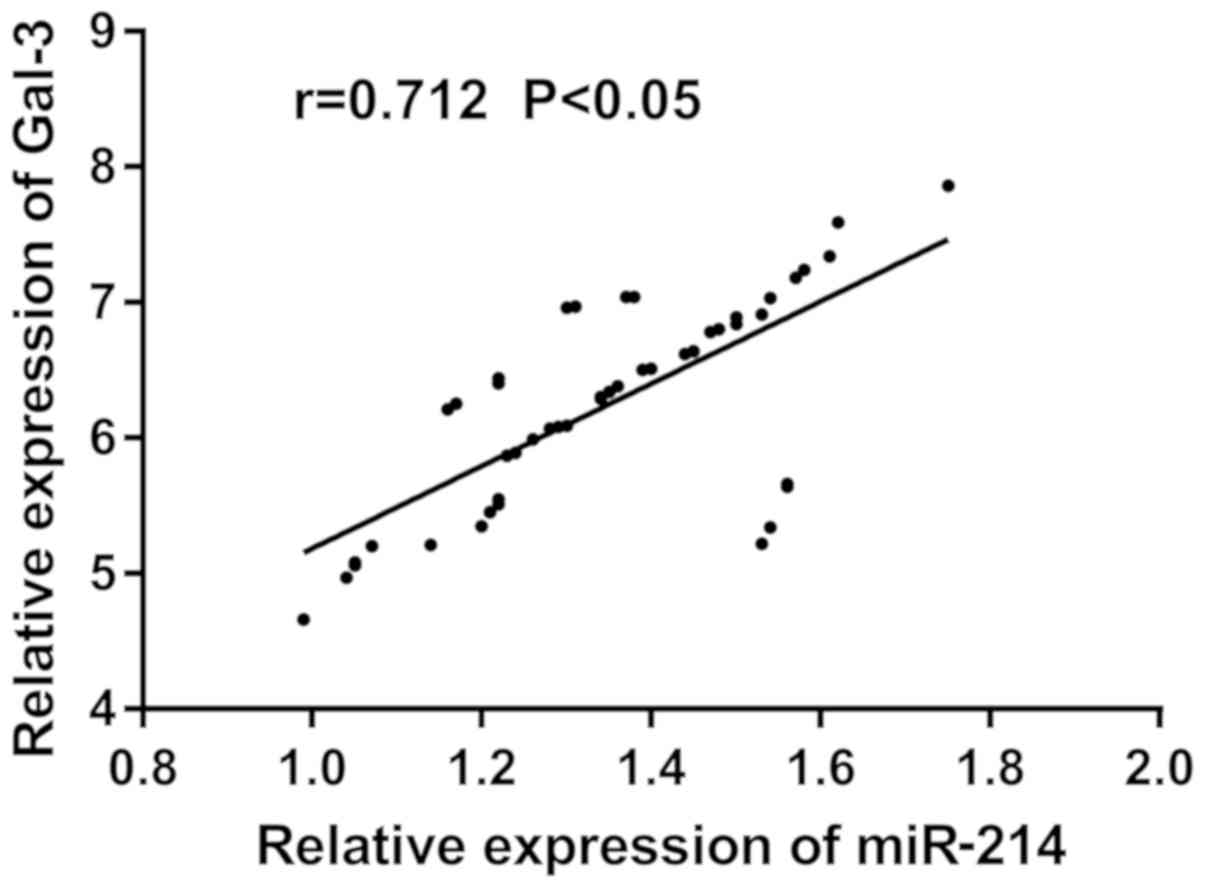
Correlation between miR-214 and Gal-3
expression
Pearson's correlation analysis was used to analyze
the correlation between miR-214 and Gal-3 in serum of patients
before treatment, and it was found that miR-214 and Gal-3
expression levels were positively correlated (r=0.712, P<0.05).
The scatter plot in Fig. 6 shows
that serum miR-214 level increased significantly with the increase
of Gal-3.
Discussion
CHF has a high incidence and mortality. In recent
years, studies have shown that, although the survival rate has
improved, the mortality rate of HF remains ~50% within 5 years
after diagnosis, and the prognosis is even worse (19). Therefore, it is of great significance
to improve diagnosis, treatment guidance and curative effect
prediction of CHF. Gal-3 is currently recognized as an inflammatory
factor that promotes cardiac fibrosis. With the further research on
the inflammatory mechanism of HF, it has been confirmed that
inflammatory factors play a crucial role in the occurrence and
development of HF (20). Relevant
studies have supported that miR-214 and Gal-3 are upregulated in
patients with CHF (16,21), which is closely related to the
pathophysiological process of HF and is expected to be a new
biomarker for HF.
As a hot research field in recent years, miR has
attracted the attention of numerous scholars. The main role of miR
is to bind to the downstream target gene 3′-UTR, leading to
degradation of mRNA, to inhibit its translation and transcription
(22,23), so as to change the expression of the
target gene. Normally, Gal-3 is expressed in a small amount in
cardiac tissue. In the case of myocardial injury, however, the
concentration of Gal-3 increases rapidly, leading to cardiac
fibrosis (24), which can provide
short- or long-term independent prognostic information for patients
with HF (25). The study of Dong
et al (26) showed that the
expression of miR-214 in the infarcted part of rats after 6 h of
acute myocardial infarction increased, which could protect
cardiomyocytes (27). miR-214 and
Gal-3 are involved in the occurrence and development of CHF;
however, their clinical efficacy indexes after treatment have not
been studied. Therefore, this study further verified the
correlation between miR-214 and Gal-3, and their clinical
diagnostic and efficacy prediction value for CHF.
In the present study, we collected serum of CHF
patients and healthy subjects and detected the expression of
miR-214 and Gal-3 in the serum of the two groups. It was found that
the serum levels of miR-214 and Gal-3 in the observation group were
higher than those in the control group, with significant
difference. Studies on mice by Yu et al (28) and Martínez-Martínez et al
(29) have found that myocardial
fibrosis would not occur in the absence of Gal-3. In addition, the
upregulation of miR-214 could reduce endothelial cell proliferation
and angiogenesis during the transition from hypertrophic heart
rhythm to HF (30). This suggested
that these two indexes are expected to be potential diagnostic
indexes for CHF. Therefore, ROC curve analysis was performed on the
expression of miR-214 and Gal-3 in the observation and control
groups. The results revealed that the AUC of the expression of
miR-214 and Gal-3 was 0.874 and 0.897, respectively. This indicates
that CHF patients and healthy subjects can be well distinguished by
detecting the expression of miR-214 and Gal-3, and therefore can be
used as potential diagnostic indicators for patients with CHF.
Although the above studies revealed that miR-214 and Gal-3 could be
used as clinical diagnostic indexes of CHF, there was no further
study conducted on the clinical efficacy assessment after treatment
of CHF patients. According to the clinical efficacy in the
observation group, patients were divided into a group with good
efficacy and a group with poor efficacy, and the association of
miR-214 and Gal-3 expression with efficacy was investigated. The
results revealed that the relative expression of miR-214 and Gal-3
in the group with good efficacy were significantly lower than those
in the group with poor efficacy, which suggests that the expression
of miR-214 and Gal-3 before treatment may be a potential predictive
index of the clinical efficacy of patients after treatment. For
this reason, ROC curves were drawn, and it was found that the AUC
of miR-214 and Gal-3 was 0.818 and 0.825, respectively, which
indicates that the expression of the two indexes before treatment
could be used as a predictor of the clinical efficacy of patients
after treatment.
Pearson's correlation analysis was used to analyze
the correlation between miR-214 and Gal-3 expression in serum of
patients, and it was found that the expression level of miR-214 was
positively correlated with the expression level of Gal-3 (r=0.712,
P<0.05). The scatter plot revealed that the expression level of
Gal-3 increased with the increase of miR-214 expression, suggesting
that both of them participate in the development of CHF and may be
considered prognostic indexes of CHF. Gal-3 has the effect of
promoting cardiac fibrosis. Furthermore, studies have found that
miR-214 could regulate the proliferation of fibroblasts (31). Combined with the results of this
study, it is suggested that the two indexes have a synergistic
effect on promoting cardiac fibrosis. However, as this study did
not investigate the patient's survival, whether miR-214 and Gal-3
can become prognostic indicators of CHF needs further
investigation.
Although the clinical significance of miR-214 in the
occurrence and development of a variety of heart diseases has been
recognized, the mechanism of its abnormal expression has not been
clarified. In addition, miR is very sensitive to temperature, and
therefore will be inevitably partially decomposed due to changes in
the surrounding environment, causing deviations in experimental
data. The pathophysiological mechanism and biological half-life of
Gal-3 in the human body are not fully understood, which along with
the low specificity, are responsible for deviations in the
diagnostic results. At present, this study is still in the initial
stage, and further exploration is needed to apply these results
into practice. The stability and durability of miR-214 and Gal-3
expression need further investigation.
In conclusion, it is speculated that miR-214 and
Gal-3 are involved in the occurrence and development of CHF and are
expected to be potential indicators for the diagnosis and efficacy
prediction of CHF.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
RH, KL, LL and LZ conceived and designed the study,
and drafted the manuscript. RH, KL, LZ and HZ collected, analyzed
and interpreted the experimental data. RH revised the manuscript
for important intellectual content. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Shanghai Xuhui Central Hospital (Shanghai, China). Signed informed
consents were obtained from the patients or the guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ahmed A: DEFi - Heart Failure: A guide to
management of geriatric heart failure by generalist physicians.
Minerva Med. 100:39–50. 2009.PubMed/NCBI
|
|
2
|
Mozaffarian D, Benjamin EJ, Go AS, Arnett
DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després JP,
Fullerton HJ, et al Writing Group Members; American Heart
Association Statistics Committee; Stroke Statistics Subcommittee, :
Heart disease and stroke statistics- 2016 update: A report from the
American Heart Association. Circulation. 133:e38–e360. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Heidenreich PA, Albert NM, Allen LA,
Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam
MA, Maddox TM, et al: American Heart Association Advocacy
Coordinating Committee; Council on Arteriosclerosis, Thrombosis and
Vascular Biology; Council on Cardiovascular Radiology and
Intervention; Council on Clinical Cardiology; Council on
Epidemiology and Prevention; Stroke Council: Forecasting the impact
of heart failure in the United States: A policy statement from the
American Heart Association. Circ Heart Fail. 6:606–619. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lloyd-Jones DM, Larson MG, Leip EP, Beiser
A, D'Agostino RB, Kannel WB, Murabito JM, Vasan RS, Benjamin EJ and
Levy D; Framingham Heart Study, : Lifetime risk for developing
congestive heart failure: The Framingham Heart Study. Circulation.
106:3068–3072. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mureddu GF, Agabiti N, Rizzello V,
Forastiere F, Latini R, Cesaroni G, Masson S, Cacciatore G,
Colivicchi F, Uguccioni M, et al PREDICTOR Study Group, :
Prevalence of preclinical and clinical heart failure in the
elderly. A population-based study in Central Italy. Eur J Heart
Fail. 14:718–729. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Schocken DD, Benjamin EJ, Fonarow GC,
Krumholz HM, Levy D, Mensah GA, Narula J, Shor ES, Young JB and
Hong Y; American Heart Association Council on Epidemiology and
Prevention; American Heart Association Council on Clinical
Cardiology; American Heart Association Council on Cardiovascular
Nursing; American Heart Association Council on High Blood Pressure
Research; Quality of Care and Outcomes Research Interdisciplinary
Working Group and Functional Genomics and Translational Biology
Interdisciplinary Working Group, : Prevention of heart failure: A
scientific statement from the American Heart Association Councils
on Epidemiology and Prevention, Clinical Cardiology, Cardiovascular
Nursing, and High Blood Pressure Research; Quality of Care and
Outcomes Research Interdisciplinary Working Group; and Functional
Genomics and Translational Biology Interdisciplinary Working Group.
Circulation. 117:2544–2565. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Morrow DA and O'Donoghue ML: Galectin-3 in
cardiovascular disease: A possible window into early myocardial
fibrosis. J Am Coll Cardiol. 60:1257–1258. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sharma UC, Pokharel S, van Brakel TJ, van
Berlo JH, Cleutjens JP, Schroen B, André S, Crijns HJ, Gabius HJ,
Maessen J, et al: Galectin-3 marks activated macrophages in
failure-prone hypertrophied hearts and contributes to cardiac
dysfunction. Circulation. 110:3121–3128. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ho JE, Liu C, Lyass A, Courchesne P,
Pencina MJ, Vasan RS, Larson MG and Levy D: Galectin-3, a marker of
cardiac fibrosis, predicts incident heart failure in the community.
J Am Coll Cardiol. 60:1249–1256. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rabinovich GA, Liu FT, Hirashima M and
Anderson A: An emerging role for galectins in tuning the immune
response: Lessons from experimental models of inflammatory disease,
autoimmunity and cancer. Scand J Immunol. 66:143–158. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
van Almen GC, Verhesen W, van Leeuwen RE,
van de Vrie M, Eurlings C, Schellings MW, Swinnen M, Cleutjens JP,
van Zandvoort MA, Heymans S, et al: MicroRNA-18 and microRNA-19
regulate CTGF and TSP-1 expression in age-related heart failure.
Aging Cell. 10:769–779. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yang B, Lin H, Xiao J, Lu Y, Luo X, Li B,
Zhang Y, Xu C, Bai Y, Wang H, et al: The muscle-specific microRNA
miR-1 regulates cardiac arrhythmogenic potential by targeting GJA1
and KCNJ2. Nat Med. 13:486–491. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Vegter EL, van der Meer P, de Windt LJ,
Pinto YM and Voors AA: MicroRNAs in heart failure: From biomarker
to target for therapy. Eur J Heart Fail. 18:457–468. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lawrie CH, Gal S, Dunlop HM, Pushkaran B,
Liggins AP, Pulford K, Banham AH, Pezzella F, Boultwood J,
Wainscoat JS, et al: Detection of elevated levels of
tumour-associated microRNAs in serum of patients with diffuse large
B-cell lymphoma. Br J Haematol. 141:672–675. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tijsen AJ, Creemers EE, Moerland PD, de
Windt LJ, van der Wal AC, Kok WE and Pinto YM: MiR423-5p as a
circulating biomarker for heart failure. Circ Res. 106:1035–1039.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
van Rooij E, Sutherland LB, Liu N,
Williams AH, McAnally J, Gerard RD, Richardson JA and Olson EN: A
signature pattern of stress-responsive microRNAs that can evoke
cardiac hypertrophy and heart failure. Proc Natl Acad Sci USA.
103:18255–18260. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Anguita M, Comin J, Almenar L, Crespo M,
Delgado J, Gonzalez-Costello J, Hernandez-Madrid A, Manito N, Perez
de la Sota E, Segovia J, et al: Comments on the ESC Guidelines for
the diagnosis and treatment of acute and chronic heart failure
2012. A report of the Task Force of the Clinical Practice
Guidelines Committee of the Spanish Society of Cardiology. Rev Esp
Cardiol (Engl Ed). 65:874–878. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yancy CW, Jessup M, Bozkurt B, Butler J,
casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi
JL, et al: 2013 ACCF/AHA guideline for the management of heart
failure: A report of the American College of Cardiology
Foundation/American Heart Association Task Force on practice
guidelines. Circulation. 128:240–327. 2013. View Article : Google Scholar
|
|
20
|
Oikonomou E, Tousoulis D, Siasos G,
Zaromitidou M, Papavassiliou AG and Stefanadis C: The role of
inflammation in heart failure: New therapeutic approaches. Hellenic
J Cardiol. 52:30–40. 2011.PubMed/NCBI
|
|
21
|
Bagnall RD, Tsoutsman T, Shephard RE,
Ritchie W and Semsarian C: Global microRNA profiling of the mouse
ventricles during development of severe hypertrophic cardiomyopathy
and heart failure. PLoS One. 7:e447442012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bartel DP: MicroRNAs: Genomics,
biogenesis, mechanism, and function. Cell. 116:281–297. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ambros V: The functions of animal
microRNAs. Nature. 431:350–355. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hrynchyshyn N, Jourdain P, Desnos M,
Diebold B and Funck F: Galectin-3: A new biomarker for the
diagnosis, analysis and prognosis of acute and chronic heart
failure. Arch Cardiovasc Dis. 106:541–546. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
de Boer RA, Lok DJ, Jaarsma T, van der
Meer P, Voors AA, Hillege HL and van Veldhuisen DJ: Predictive
value of plasma galectin-3 levels in heart failure with reduced and
preserved ejection fraction. Ann Med. 43:60–68. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Dong S, Cheng Y, Yang J, Li J, Liu X, Wang
X, Wang D, Krall TJ, Delphin ES and Zhang C: MicroRNA expression
signature and the role of microRNA-21 in the early phase of acute
myocardial infarction. J Biol Chem. 284:29514–29525. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lv G, Shao S, Dong H, Bian X, Yang X and
Dong S: MicroRNA-214 protects cardiac myocytes against
H2O2-induced injury. J Cell Biochem.
115:93–101. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yu L, Ruifrok WP, Meissner M, Bos EM, van
Goor H, Sanjabi B, van der Harst P, Pitt B, Goldstein IJ, Koerts
JA, et al: Genetic and pharmacological inhibition of galectin-3
prevents cardiac remodeling by interfering with myocardial
fibrogenesis. Circ Heartai1. 6:107–117. 2013.
|
|
29
|
Martínez-Martínez E, Calvier L,
Fernández-Celis A, Rousseau E, Jurado-López R, Rossoni LV, Jaisser
F, Zannad F, Rossignol P, Cachofeiro V, et al: Galectin-3 blockade
inhibits cardiac inflammation and fibrosis in experimental
hyperaldosteronism and hypertension. Hypertension. 66:767–775.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Duan Q, Yang L, Gong W, Chaugai S, Wang F,
Chen C, Wang P, Zou MH and Wang DW: MicroRNA-214 is upregulated in
heart failure patients and suppresses XBP1-mediated endothelial
cells angiogenesis. J Cell Physiol. 230:1964–1973. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sun M, Yu H, Zhang Y, Li Z and Gao W:
MicroRNA-214 mediates isoproterenol-induced proliferation and
collagen synthesis in cardiac fibroblasts. Sci Rep. 5:183512015.
View Article : Google Scholar : PubMed/NCBI
|