Introduction
Post-stroke depression (PSD) is one of the most
prevalent psychiatric disorders following strokes, and affects
nearly a third of the survivors during the first 5 years after the
stroke (1). The occurrence of PSD is
associated with negative clinical outcomes, including impaired
cognition and delayed recovery of neurological functions.
Furthermore, PSD acts as a prominent barrier to stroke
rehabilitation and has been related to a reduced quality of life as
well as an increasing risk of stroke recurrence and mortality
(2). Thus, early diagnosis as well
as efficient management of PSD must be a priority in clinical
stroke rehabilitation.
Extensive investigations have suggested that
inflammation plays an important role in acute ischemic stroke and
depression by stimulating various pro-inflammatory markers, where
the subsequent inflammation has been demonstrated to be involved in
the development of PSD (3,4). Acute ischemic stroke has been
demonstrated to induce the inflammatory response accompanied by a
significant increase in the expression levels of inflammatory and
pro-inflammatory cytokines markers, such as interleukin (IL)-1β,
IL-1α, tumor necrosis factor (TNF)-α, IL-6, IL-8 and soluble TNF
receptor 1 in the plasma, which are frequently found in the acute
phase of stroke (5).
Pro-inflammatory cytokines induce an inflammatory cascade reaction
(6) and the expression of
inflammatory related cytokines are strongly related with larger
infarct sizes and a poorer prognosis for stroke patients (7).
Previous studies have shown that low-grade
inflammation plays a critical role in the development of depression
(8). Antidepressants may moderately
improve depressive symptoms by reducing the levels of
pro-inflammatory cytokines and increase the production of
anti-inflammatory cytokines (9).
Inflammatory mediators have been found to interact with key
biological systems in depression (10), including altering neurotransmitter
metabolism, neuroendocrine function, neural plasticity and the
levels of reactive oxygen species. Similarly, a cohort study showed
that the serum levels of IL-6, IL-10, TNF-α and IFN-γ were
significantly higher in the PSD cohort compared to the non-PSD
cohort (11). Furthermore, a recent
study found that the coexistence of higher homocysteine and
C-reactive protein (CRP) expression levels were independent risk
factors for PSD (12).
In recent years, the neutrophil-to-lymphocyte ratio
(NLR) and platelet-to-lymphocyte ratio (PLR) have emerged as
well-accepted biomarkers for the assessment of overall inflammatory
status. The NLR and PLR are simple and cost-effective biomarkers
that can be easily derived from blood during routine examinations
(13). Elevated levels of NLR and
PLR have been found to be related with oxidative stress and
increased cytokine production in patients with depressive disorders
(14). Furthermore, the NLR and PLR
are strongly related to the prognosis of infarction and
thrombo-inflammatory state. The NLR has been used as an indicator
to reflect the prevalence of intracranial atherosclerosis (15) and is considered to be an independent
risk factor for ischemic stroke and a poorer prognosis (16). Similarly, the PLR has been used to
predict poor prognoses, the rate of insufficient recanalization and
the size of infarcted area following stroke (17).
In addition to the inflammation and stroke, the NLR
and PLR are also considered to be related to psychiatric disorders,
especially depression. The NLR has been found to be increased in
patients with major depression without antidepressant therapy;
however, the NLR returned to normal levels after 3 months of
Selective Serotonin Reuptake Inhibitor treatment (18). Moreover, the PLR in patients with
major depression has also been found to be increased (19). Recent studies have suggested that the
NLR or PLR are associated with PSD 1 month following stroke
occurrence (20,21), which highlighted the relationship
between early PSD and the inflammation index. However, there was
not clear association between these indicators and 6-month PSD. To
the best of the our knowledge, the present study is the first to
explore the association between the NLR/PLR and PSD at 6 months.
The aim of the present study was to examine the value of the NLR
and PLR as joint indicators in the diagnosis of PSD. Whether the
joint index has better diagnostic value than independence index is
a valuable question which may improve the diagnosis of PSD.
Materials and methods
Study population.
The present study was approved by the Ethics
Committee of the First Affiliated Yijishan Hospital of Wannan
Medical College. Written informed consents were signed by all
participants or their relatives prior to their inclusion in the
present study.
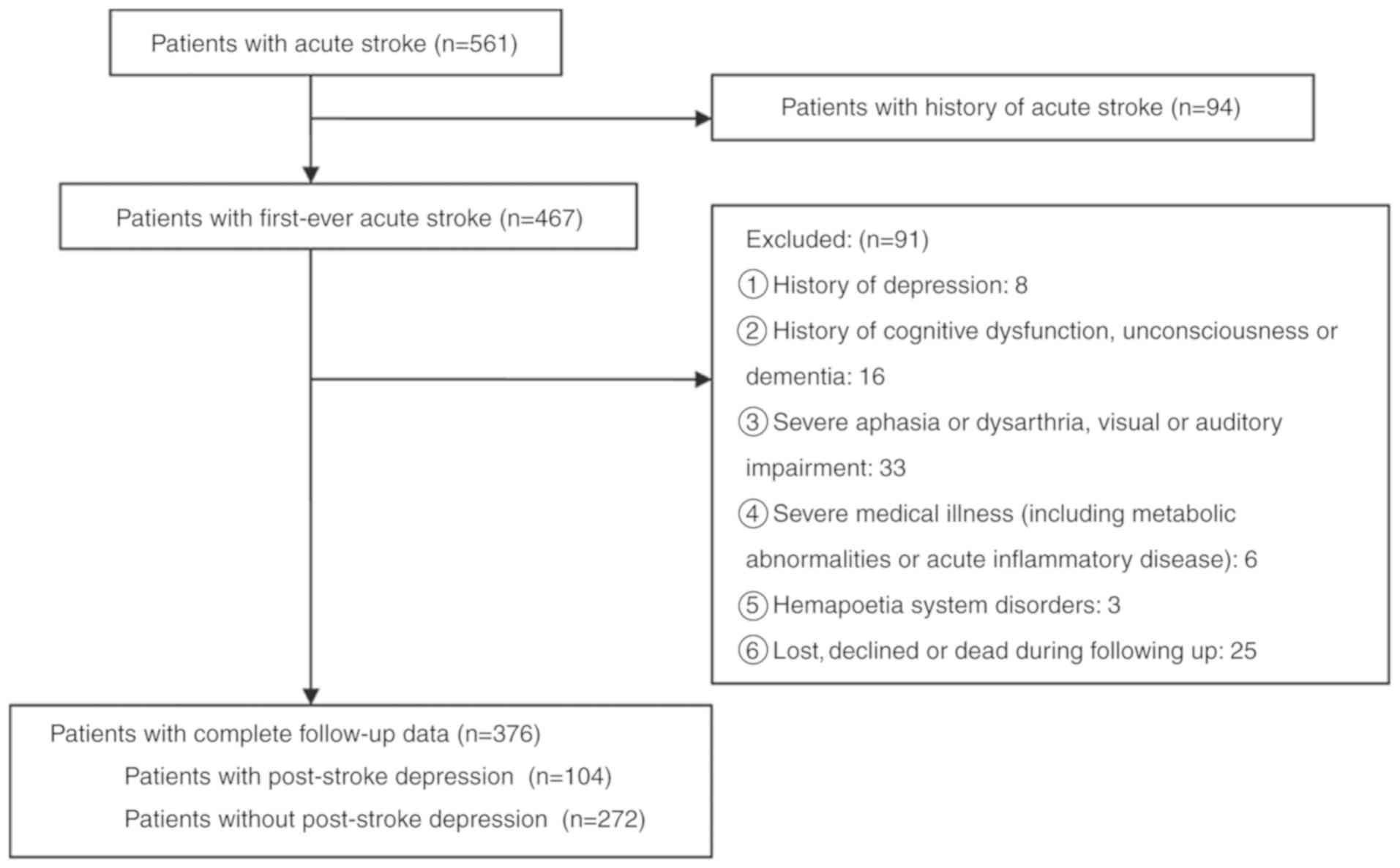
Retrospective analysis was carried out in 376
patients with first-ever acute ischemic stroke in Stroke Ward of
the First Affiliated Yijishan Hospital of Wannan Medical College
between March 2015 and September 2017. All of the enrolled patients
met the World Health Organization Multinational Monitoring of
Trends and Determinants in Cardiovascular Disease criteria defined
for acute ischemic stroke (22), and
the diagnoses were verified by the results from computed tomography
(CT) or magnetic resonance imaging (MRI) within 24 h after
admission. The exclusion criteria for patients were: i) Patients
with psychosis or other psychiatric conditions, including anxiety,
depression and suicidal behavior; ii) patients with central nervous
system diseases including dementia, significant cognitive
impairment or decreased level of consciousness; iii) patients with
severe aphasia or dysarthria as well as visual or auditory
impairments; iv) patients with metabolic abnormalities, tumors,
significant acute inflammatory disease or other medical illness
besides stroke; v) patients with hematological disorders; and vi)
patients who were not followed-up or died during follow-up
(Fig. 1). The diagnosis of
depression was based on the structured clinical interview for the
Structured Clinical Interview For Diagnostic and Statistical Manual
of Mental Disorders-IV technique (23) at 6 months, followed up by telephone
consultation or outpatient clinic. The severity of depressive
symptoms was quantified using the Hamilton Depression Scale (HAM-D)
score (24). Additionally, 120
healthy volunteers from the physical examination center in the
First Affiliated Yijishan Hospital of Wannan Medical College were
recruited between March 2015 and September 2017 as controls
retrospectively.
Clinical measurement.
Relevant clinical data were retrospectively
collected from relevant medical records. Demographic data [such as
age, sex, body mass index (BMI), and education level], history of
conventional vascular risk factor (such as hypertension, diabetes
mellitus, hypercholesterolemia and atrial fibrillation) and medical
history (such smoking, alcohol consumption, previous infarctions
and family history of strokes) were obtained. Stroke subtype was
classified according to the Trial of Org 10172 in Acute Stroke
Treatment criteria (25). Stroke
severity was evaluated by trained neurologists using the National
Institutes of Health Stroke Scale (NIHSS) within 24 h of admission
at baseline. Cognitive function was measured using Mini Mental
State Examination (MMSE) on admission (26). Functional outcomes were obtained
using the modified Rankin Scale (mRS) at a 3-month follow-up. The
data of CT/MRI, performed within 24 h after admission, were
collected retrospectively in order to confirm diagnosis and assess
the site, size and cause of the infarction. The NLR and PLR were
all retrospectively obtained from the blood routine results at
admission by calculating the ratios between neutrophil or platelets
and lymphocytes in peripheral blood samples.
Statistical analyses.
Results are expressed as the mean ± SD or as the
median (quartiles) for the continuous variables depending on
whether the data were normally or not normally distributed,
respectively. Categorical variables are presented as percentages.
Proportions were compared using the χ2 test, and
Student's t-test and two-way ANOVA were employed for the normally
distributed variables, while the Mann-Whitney U test was employed
for the non-normally distributed variables. Spearman's rank
correlation was used for bivariate correlations. The association
between the NLR or PLR and the NIHSS score and HAM-D score were
also assessed using linear regression models with multivariate
adjustments for possible confounders; the NLR and PLR were
dichotomized using a median split. The influence of the NLR/PLR
separately or jointly on PSD was examined using binary logistic
regression analyses, resulting in odds ratios (ORs) and 95% CI.
Multiple-adjusted logistic regression models were also used,
allowing for the adjustment for potential confounding factors. A
receiver operating characteristic curve analysis was used to
identify the cutoff points for the NLR and PLR levels at admission
with the greatest sensitivity and specificity to predict PSD at the
6-month follow-up. All statistical analyses were performed using
SPSS for Windows (version 19.0; IBM Corp.). P<0.05 was
considered to indicate a statistically significant difference.
Results
Clinical characteristics of study
samples.
Among all follow-up patients, 224 (59.57%) patients
were male, and the average age was 61.37±10.34 years. In total, 104
(27.66%) patients were diagnosed with PSD at the end of 6 months
follow-up. The basic characteristics of the 376 patients with and
without PSD are presented in Table
I.
 | Table IBaseline clinical characteristics in
patients with and without post-stroke depression at 6 months. |
Table I
Baseline clinical characteristics in
patients with and without post-stroke depression at 6 months.
| Variant | Non-PSD
(n=272) | PSD (n=104) | Normal control
(n=120) |
P-valuea |
P-valueb |
|---|
| Demographic
characteristics |
|
Age, years
Mean ± SD | 60.64±10.02 | 61.74±10.52 | 60.21±10.37 | 0.348 | 0.275 |
|
Female,
% | 101 (37.13) | 51 (49.04) | 52 (43.33) | 0.035 | 0.393 |
|
Educational,
years | 5 (0-7) | 3 (0-6) | | 0.032 | |
|
BMI,
kg/m2 | 22.24
(20.67-24.58) | 26.73
(22.87-30.12) | | 0.016 | |
|
Widowhood,
% | 28 (10.29) | 36 (34.62) | | <0.001 | |
| Vascular risk
factors, % |
|
Hypertension | 186 (68.38) | 72 (69.23) | | 0.874 | |
|
Hyperlipidemia | 85 (31.25) | 33 (31.73) | | 0.928 | |
|
Diabetes
mellitus | 116 (42.62) | 48 (46.15) | | 0.540 | |
|
Coronary
heart disease | 79 (29.04) | 34 (32.69) | | 0.490 | |
|
Atrial
fibrillation | 81 (29.78) | 35 (33.65) | | 0.467 | |
|
Active
smokers | 101 (37.13) | 43 (41.35) | | 0.452 | |
|
Alcohol
consumption | 91 (33.46) | 36 (34.62) | | 0.832 | |
| Type of stroke
etiology, % | | | | 0.390 | |
|
Atherothrombotic | 156 (57.35) | 63 (60.57) | | | |
|
Lacunar | 73 (26.84) | 15 (14.42) | | | |
|
Cardioembolic | 6 (2.21) | 7 (6.73) | | | |
|
Others | 37 (13.60) | 19 (18.27) | | | |
| Lesion location,
% | | | | 0.459 | |
|
Frontal | 55 (20.22) | 17 (16.35) | | | |
|
Parietal | 31 (11.40) | 13 (12.50) | | | |
|
Temporal | 22 (8.09) | 11 (10.58) | | | |
|
Occipital | 26 (9.56) | 9 (8.65) | | | |
|
Basal
ganglia | 84 (30.88) | 29 (27.88) | | | |
|
Posterior
fossa | 51 (18.75) | 20 (19.23) | | | |
|
Others | 3 (1.10) | 5 (4.81) | | | |
| Hospital stay,
days | 15 (7-23) | 16 (8-27) | | 0.261 | |
| Baseline NIHSS
score | 8 (6-11) | 9 (7-12) | | <0.001 | |
| Baseline MMSE
score | 28 (25-30) | 26 (22-28) | | 0.024 | |
| mRS at 3
months | 2 (1-2) | 2 (1-4) | | 0.072 | |
| NLR | 2.83
(2.31-3.79) | 3.81
(2.52-4.67) | 1.96
(1.54-2.57) | <0.001 | <0.001 |
| PLR | 112.04
(89.25-143.73) | 159.74
(124.87-246.05) | 112.17
(87.36,142.3) | <0.001 | <0.001 |
Relationship between the NLR and PLR,
and the stroke characteristics.
The median value [interquartile range (IQR)] of NLR
or PLR for all patients with stroke was significantly higher than
that of the normal subjects, the NLR in patients and in healthy
subjects was 2.87 (2.39-4.02) and 1.96 (1.54-2.57), respectively
(P<0.001). The PLR in patients and in healthy subjects was
125.31 (103.21-203.74) and 112.17 (87.36,142.3), respectively
(P<0.001). Moreover, the NLR and PLR were observed to increase
with the extent of damage caused by the stroke, as defined by the
NIHSS score. There was a positive correlation observed between the
NLR and the NIHSS score (r=0.289, P<0.001), and a similar
correlation between the PLR and the NIHSS score (r=0.237,
P<0.001). Similarly, Raised HAM-D scores at the 6-month follow
up were also found to correspond with increased NLRs and PLRs
(r=0.206, P=0.003; r=0.201, P=0.001, respectively). Additionally,
when patient MRI data was available (n=261), a positive correlation
was also observed between the infarct volume of patients as well as
the NLRs (r=0.166, P=0.032). No correlation was observed between
the PLR and the infarct volumes (P=0.071). There was a positive
correlation between the lesion volumes and HAM-D scores (r=0.251,
P<0.001).
NLRs, PLRs and PSD.
Patients with PSD showed significantly higher NLR
levels at admission than the ones without PSD [3.81 (2.52-4.67) vs.
2.83 (2.31-3.79), respectively, P<0.001]. Similarly, PLR levels
in patients with PSD were higher than those in patients without PSD
[159.74 (124.87-246.05) vs. 112.04 (89.25-143.73), respectively,
P<0.001]. Patients with PSD were predominantly female compared
to the non-PSD group. The PSD group also had a lower average
education level, higher BMI, a higher proportion of patients living
alone, higher stroke severity and worse cognition. However, there
was no association between lesion location, etiological subtype,
functional outcomes according to mRS as well as vascular risk
factors and PSD.
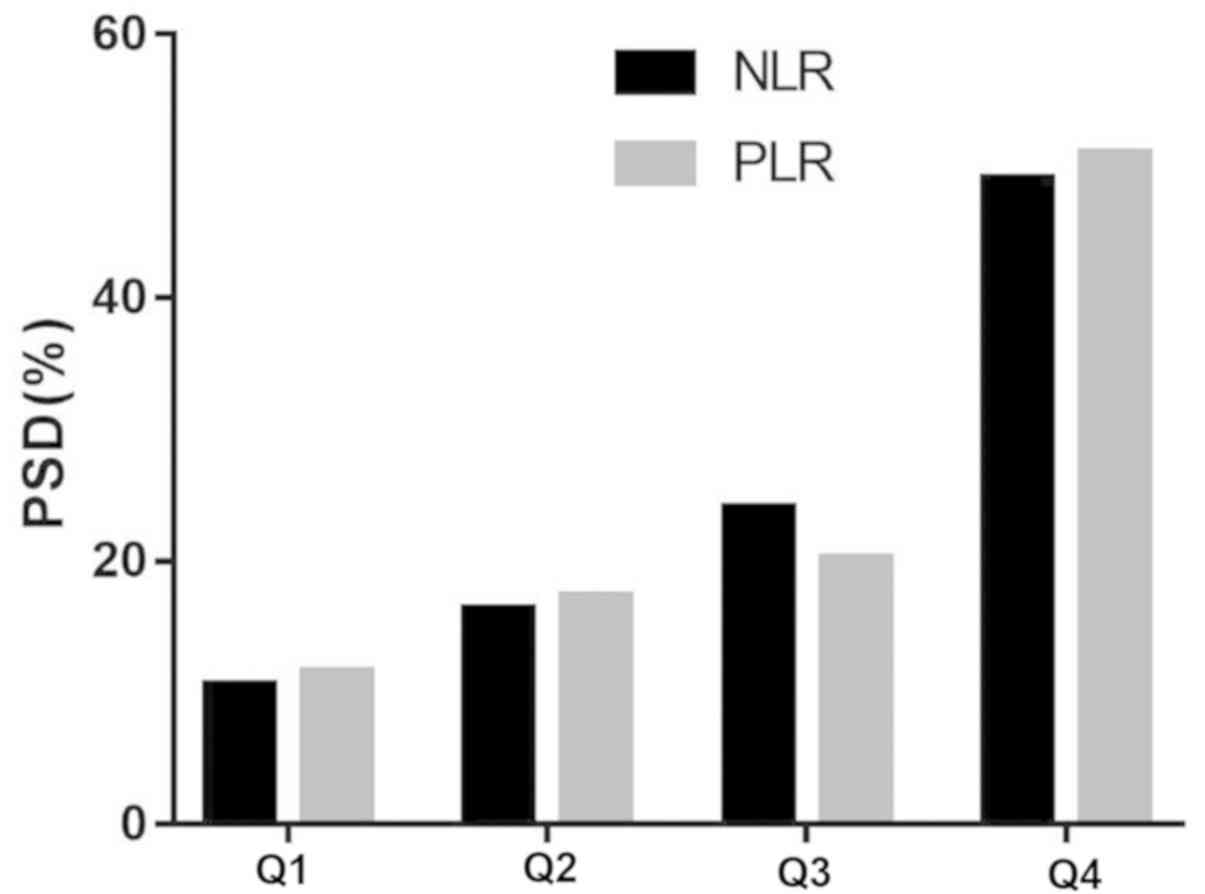
The quartiles of NLR and PLR values in the PSD group
were observed to have a significant difference from those in the
non-PSD group (P<0.0001) (Table
II). The PSD distribution across the NLR quartiles ranged
between 10.58-49.04% between the first and fourth quartile,
respectively (Fig. 2). The
corresponding distribution for PLR was 11.54-50.96% between the
first and fourth quartile, respectively (Fig. 2).
| Table IIThe NLR and PLR quartiles of
patients. |
Table II
The NLR and PLR quartiles of
patients.
| PLR and NLR % | PSD (n=104) | Non-PSD
(n=272) | P-value |
|---|
| NLR, % | | | <0.001 |
|
Quartile
1 | 11 (10.58) | 81 (29.78) | 0.001 |
|
Quartile
2 | 17 (16.35) | 73 (26.84) | 0.033 |
|
Quartile
3 | 25 (24.04) | 71 (26.10) | 0.681 |
|
Quartile
4 | 51 (49.04) | 47 (17.28) | <0.001 |
| PLR, % | | | <0.001 |
|
Quartile
1 | 12 (11.54) | 78 (28.68) | 0.005 |
|
Quartile
2 | 18 (17.31) | 76 (27.94) | 0.033 |
|
Quartile
3 | 21 (20.19) | 70 (25.74) | 0.262 |
|
Quartile
4 | 53 (50.96) | 48 (17.65) | <0.001 |
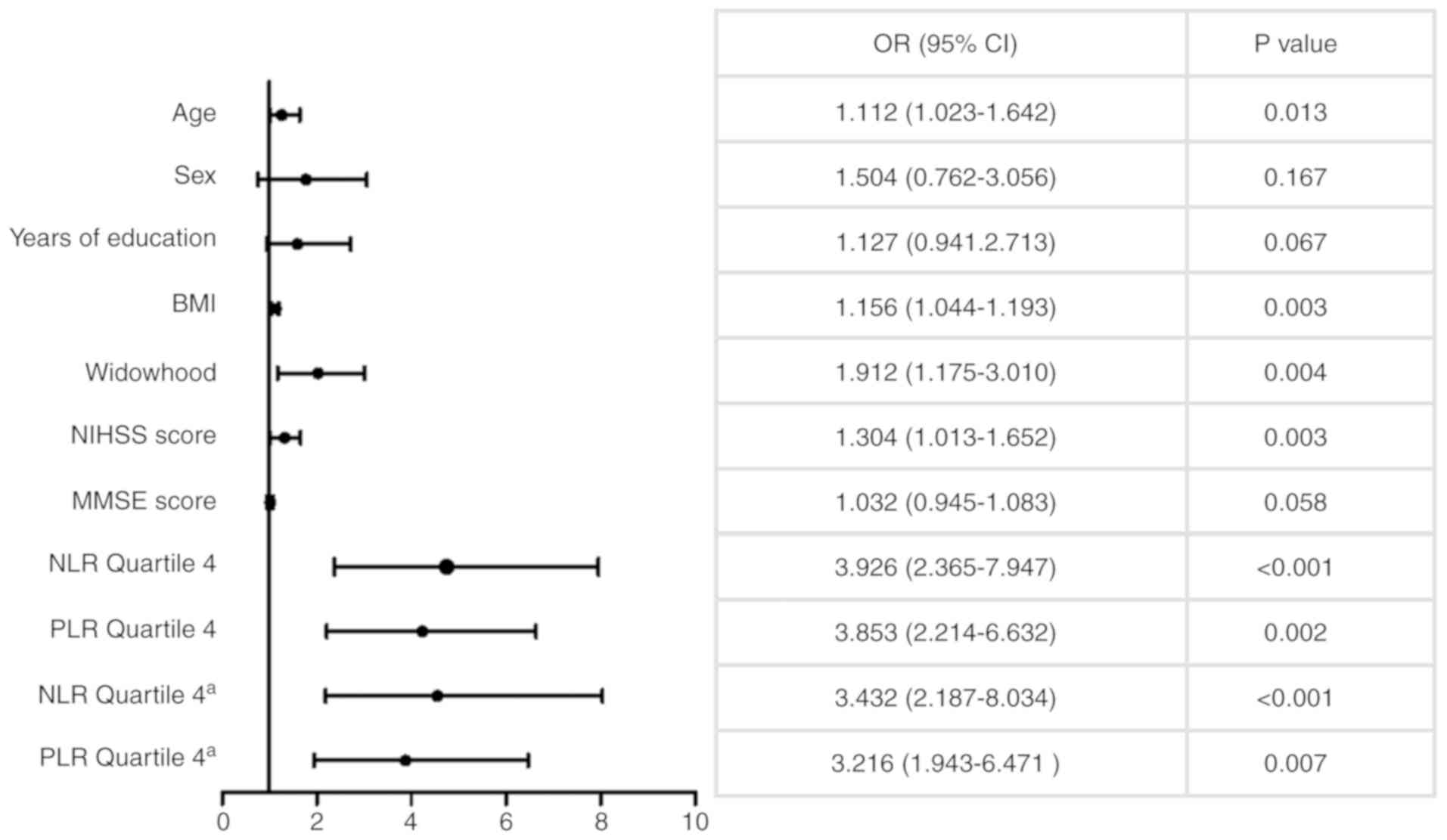
In the multivariate logistic regression analysis,
analyzing quartile 1 to quartile 3 of the NLR data [upper quartile,
<4.02; median, 2.87 (2.39-4.02)] and the PLR data [upper
quartile, <203.74; median, 121.31 (103.21-203.74)], using all
stroke patients as a reference respectively, after adjusting for
other multiple confounding factors, the fourth quartile of the NLR
data [OR 3.926, 95% CI (2.365-7.947), P<0.001] and the PLR [OR
3.853, 95% CI (2.214-6.632), P=0.002] were significantly associated
with PSD (Fig. 3). Moreover, age,
BMI, widowhood and NIHSS score were associated with PSD.
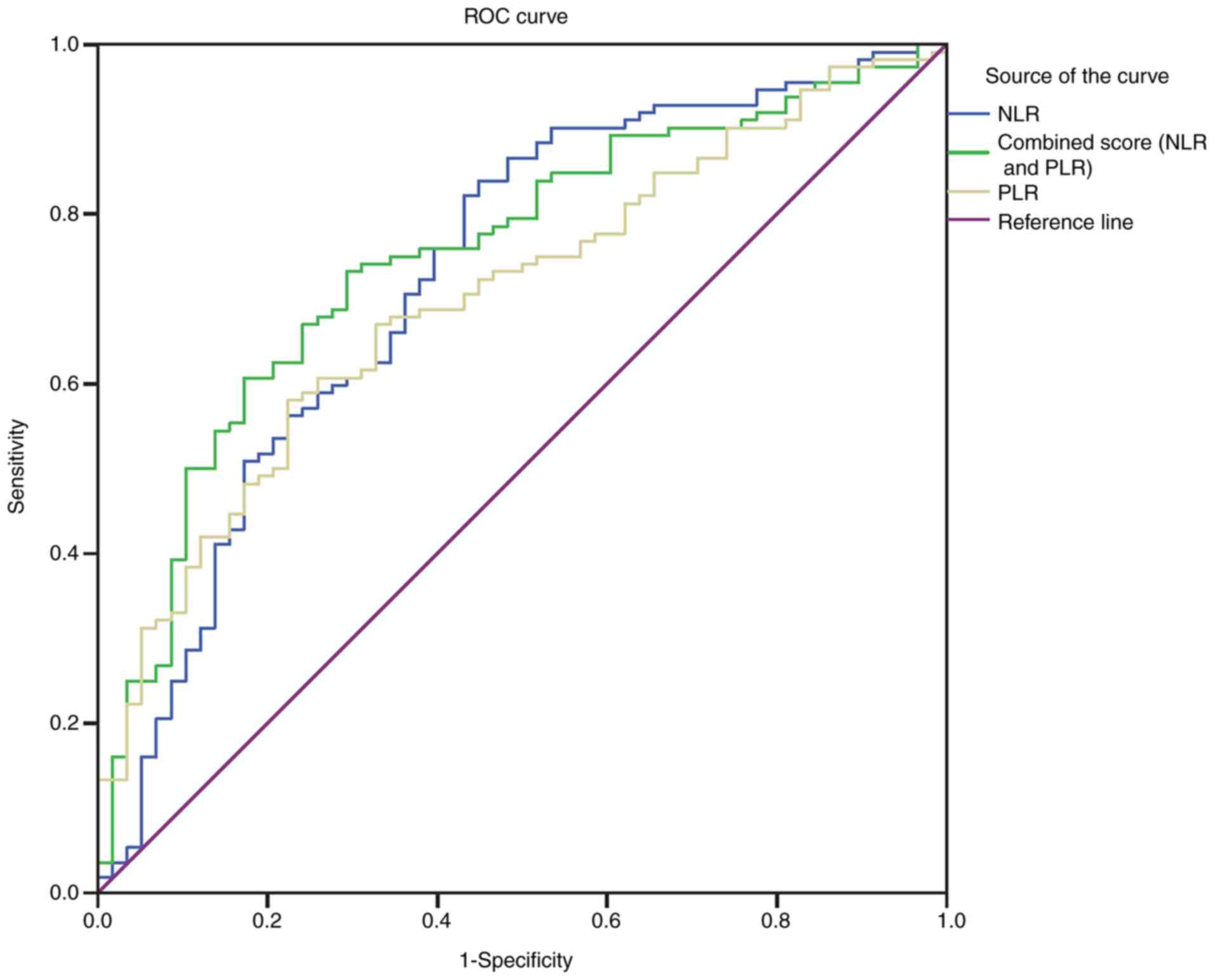
With an area under the curve (AUC) of 0.726 (95% CI,
0.643-0.809), the NLR showed a greater discriminatory ability to
predict PSD than the PLR [AUC 0.701, 95% CI (0.622-0.780);
P<0.001] (Fig. 4). Furthermore,
the PLR improved the ability of NLR to diagnose PSD [AUC of the
combined model 0.751, 95% CI (0.675-0.827); P<0.001] (Fig. 4).
The lower level of both the NLR and the PLR (both
<quartile 4) were used as a reference, and the group with higher
levels of both NLR and PLR (≥quartile 4; NLR ≥4.02 and PLR ≥203.74)
was used to predict PSD with an OR of 5.79 (95% CI, 3.03-9.45;
P<0.001) compared with the group with lower levels of both
factors (<quartile 4) after adjustment for multiple confounding
factors (age, BMI, widowhood, NIHSS score, MMSE score, vascular
risk factors and the type of stroke etiology). This showed that
higher levels of both NLR and PLR (≥quartile 4; NLR ≥4.02 and PLR
≥203.74) exhibited superior predictive value in evaluating the risk
of PSD compared with lower levels of both factors.
Discussion
Although previous studies have analyzed the
significance of the NLR or the PLR in predicting 1 month PSD, the
current study paper included these two common inflammatory
indicators and analyzed their respective and combined abilities to
predict PSD 6 months after stroke. It was found that high NLRs and
PLRs were strongly associated with the risk of PSD at 6 months
after the adjustment by variables, and it was also found that the
ability of the combined index to diagnose PSD was greater than that
of either of the inflammatory indicators alone. Higher NLRs and
PLRs, ≥quartile 4, was associated with PSD at a 5.79-fold
(P<0.001) increase compared with the lower levels of both
ratios. The combined index was much more meaningful than the
independent indexes in the early clinical detection of PSD. This
present study combined the two common indicators and found that the
combined forecasting ability was stronger than the single
forecasting ability. It is believed that the NLR and PLR may be
readily available prognostic markers for PSD.
A number of studies have reported that NLR is
associated with the poor prognosis for ischemic diseases (27). Previous studies have demonstrated
that increased neutrophils, a high number of which have been found
atherosclerotic plaques at various stages of atherosclerosis, may
damage endothelial cells, and they. Chronic inflammation
represented by NLR was also reported to be associated with a number
of vascular risk factors, including hypertension, diabetes and
hyperlipidemia (28,29). During infarction progression,
neutrophils appear to be the first leukocytes to reach the ischemic
brain, and in turn activate the inflammatory process (30). Furthermore, once they have reached
the site of injury, the highest levels of pro-inflammatory
cytokines and biomarkers of inflammation coincide with the largest
recruitment and activation of neutrophils (31). The release of these inflammatory
cytokines further amplifies the immune cascade, leading to cellular
dysfunction and the production of reactive oxygen species.
Inflammation changes the function of the intracranial
neuroendocrine, and at the same time reduces the synthesis and
secretion of monoamine neurotransmitters, leading to the
development of PSD (32). Meanwhile,
Lymphocytes are an immune cell related to regulation and
protection. The decrease of lymphocyte numbers, reflects the
pathological stress state of the body, thus a low count indicates a
poor prognosis (33).
Increasing evidence has shown that inflammation is
involved in the etiology of depression. There are a number of
cytokines which are believed to have a large impact on the
development and progression of depression, including inflammatory
and pro-inflammatory cytokines as well as cytokines produced by the
hypothalamic-pituitary-adrenal (HPA) axis (34). The excess production of these
cytokines in patients with depression, may affect neurotransmission
through the overactivation of the HPA axis (35). It has also been shown that major
depressive disorder is affected by excessive oxidative stress. Both
the NLR and PLR have been shown to demonstrate the degree of
inflammation, and are also relatively inexpensive and easy to
measure in the clinic (36-39).
As such, raised NLRs and PLRs have also been shown to be associated
with increased cytokine production and oxidative stress and have
been used to measure the systemic inflammatory response.
Furthermore, an increased NLR and dysfunctional platelets have also
been linked to patients with psychiatric disorders including
depression (18,40-42).
Platelets can act as an inflammatory indicator, and
higher platelet activation serves as a predictor of inflammation.
Activated platelets play an important role in psychiatric
disorders, including depression (43,44), and
high levels are considered to be a risk factor for an increased
incidence of cardiovascular and cerebrovascular diseases (45). The activation of platelets, mediated
by a number of inflammatory factors, including cytokines,
serotonin, glutamate, dopamine and P-selectin, serves an important
role in psychiatric disorders (46).
In particular, serotonin has been previously reported to be
involved in the activation of plasma platelets and accelerate
aggregation (47). Meanwhile,
activated platelets participate in the regulation of the
permeability of endothelial cells and recruitment of mononuclear
cell through the release of pro-inflammatory factors. Depression is
a result of platelet activation, which is potentiated by elevated
serotonin and epinephrine levels (48). There are high levels of serotonin and
glutamate in platelet dense granules, and serotonin receptors
(5HT2A) and serotonin transporter (SERT) on the surface of
platelets (49). Inflammation
induces platelet activation which is accompanied by the release of
serotonin and glutamate. Pro-inflammatory factors which derive from
activated platelets, take part in regulating and maintaining the
inflammatory reaction, and are thought to play an important role in
depression (50).
The activation of platelets is not only considered
to be a reciprocal causation of inflammation, but also closely
related to infarction and mental disorders, especially depression
(51). Previous studies have shown
that there is a significant correlation between inflammatory
responses and the development of atherosclerosis, platelet
aggregation, plaque rupture and intravascular thrombosis (52). Nemeroff and Musselmanl
(53) demonstrated that platelet
dysnfunction may increase the risk of a patient developing
depression. Activated platelets may induce the formation of a
thrombus in patients suffering from depression, and increased
serotonin levels may further alter the functions of platelets in
these patients (54). It has
previously been shown that an increased PLR is associated with
severe major depression and that it may lead to psychotic symptoms
(51). Raised PLRs have also been
associated with acute ishemic stroke patients (55). Both of these results are consistent
with the findings of the current study, further highlighting that
PSD patients have raised PLR levels when compared to non-PSD
patients. Therefore, as a stable inflammatory indicator, PLR, which
reflects the inflammatory state of stroke and depression, can also
be considered as an available prognostic marker for PSD.
There are some limitations with the present study.
Firstly, this was a single-center retrospective study. Due to the
limitations of the retrospective study, it was not possible to
collect psychosocial factors associated with PSD. Secondly, some
patients with severe aphasia or severe disease were unable to
complete the follow-up were examinations and were thus excluded
from the study, which may have introduced bias to the results.
Thirdly, the NLR and PLR values were collected only once within 24
h on admission; however, there may be a dynamic change during the
development of PSD. As such, it is necessary to pay attention to
the correlation between the NLR and PLR changes at various time
points after stroke and the prediction of PSD in prospective
study.
Although the study had some limitations, the present
study demonstrated the important relationship between the NLRPLR on
admission and PSD 6 months after stroke in south China in a Han
population, which may be involved in the pathophysiological
mechanisms behind PSD depression. Further multicenter prospective
studies are needed to confirm the relationship between NLRPLR and
PSD, and to predict whether inhibiting the inflammatory response
could prevent the occurrence of PSD.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WD was involved in all aspects of the study,
including study design, data analysis and the revision of the
article. JHu analyzed the data and prepared the manuscript. WZ
collected and analyzed general patient data. ZZ and JHan
interpreted the images and evaluated the clinical data of stroke
patients. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the ethics committee of
the First Affiliated Yijishan Hospital of Wannan Medical College.
All subjects gave written informed consent in accordance with the
Declaration of Helsinki.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Towfighi A, Ovbiagele B, El Husseini N,
Hackett ML, Jorge RE, Kissela BM, Mitchell PH, Skolarus LE, Whooley
MA and Williams LS: American Heart Association Stroke Council;
Council on Cardiovascular and Stroke Nursing; and Council on
Quality of Care and Outcomes Research: Poststroke depression: A
scientific statement for healthcare professionals from the American
heart association/American stroke association. Stroke.
48(e30-e43)2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Guajardo VD, Terroni L, Sobreiro Mde F,
Zerbini MI, Tinone G, Scaff M, Iosifescu DV, de Lucia MC and
Fráguas R: The influence of depressive symptoms on quality of life
after stroke: A prospective study. J Stroke Cerebrovasc Dis.
24:201–209. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ferrari F and Villa RF: The neurobiology
of depression: An integrated overview from biological theories to
clinical evidence. Mol Neurobiol. 54:4847–4865. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Becker KJ: Inflammation and the silent
sequelae of stroke. Neurotherapeutics. 13:801–810. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Zeng L, Wang Y, Liu J, Wang L, Weng S,
Chen K, Domino EF and Yang GY: Pro-inflammatory cytokine network in
peripheral inflammation response to cerebral ischemia. Neurosci
Lett. 548:4–9. 2013.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Waisman A, Hauptmann J and Regen T: The
role of IL-17 in CNS diseases. Acta Neuropathol. 129:625–637.
2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Bodhankar S, Chen Y, Vandenbark AA, Murphy
SJ and Offner H: Treatment of experimental stroke with
IL-10-producing B-cells reduces infarct size and peripheral and CNS
inflammation in wild-type B-cell-sufficient mice. Metab Brain Dis.
29:59–73. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Patel A: Review: The role of inflammation
in depression. Psychiatr Danub. 25 (Suppl
2)(S216-S223)2013.PubMed/NCBI
|
|
9
|
Hannestad J, DellaGioia N and Bloch M: The
effect of antidepressant medication treatment on serum levels of
inflammatory cytokines: A meta-analysis. Neuropsychopharmacology.
36:2452–2459. 2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Maes M: Depression is an inflammatory
disease, but cell-mediated immune activation is the key component
of depression. Prog Neuropsychopharmacol Biol Psychiatry.
35:664–675. 2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Su JA, Chou SY, Tsai CS and Hung TH:
Cytokine changes in the pathophysiology of poststroke depression.
Gen Hosp Psychiatry. 34:35–39. 2012.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Yin J, Zhong C, Zhu Z, Bu X, Xu T, Guo L,
Wang X, Zhang J, Cui Y, Li D, et al: Elevated circulating
homocysteine and high-sensitivity C-reactive protein jointly
predicts post-stroke depression among Chinese patients with acute
ischemic stroke. Clin Chim Acta. 479:132–137. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Arbel Y, Finkelstein A, Halkin A, Birati
EY, Revivo M, Zuzut M, Shevach A, Berliner S, Herz I, Keren G and
Banai S: Neutrophil/lymphocyte ratio is related to the severity of
coronary artery disease and clinical outcome in patients undergoing
angiography. Atherosclerosis. 225:456–460. 2012.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kasama T, Miwa Y, Isozaki T, Odai T,
Adachi M and Kunkel SL: Neutrophil-derived cytokines: Potential
therapeutic targets in inflammation. Curr Drug Targets Inflamm
Allergy. 4:273–279. 2005.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Nam KW, Kwon HM, Jeong HY, Park JH, Kim SH
and Jeong SM: High neutrophil to lymphocyte ratios predict
intracranial atherosclerosis in a healthy population.
Atherosclerosis. 269:117–121. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Goyal N, Tsivgoulis G, Chang JJ, Malhotra
K, Pandhi A, Ishfaq MF, Alsbrook D, Arthur AS, Elijovich L and
Alexandrov AV: Admission neutrophil-to-lymphocyte ratio as a
prognostic biomarker of outcomes in large vessel occlusion strokes.
Stroke. 49:1985–1987. 2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Tekesin A and Tunç A: Inflammatory markers
are beneficial in the early stages of cerebral venous thrombosis.
Arq Neuropsiquiatr. 77:101–105. 2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Demircan F, Gözel N, Kılınç F, Ulu R and
Atmaca M: The impact of red blood cell distribution width and
neutrophil/lymphocyte ratio on the diagnosis of major depressive
disorder. Neurol Ther. 5:27–33. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Cai L, Xu L, Wei L and Chen W:
Relationship of mean platelet volume To MDD: A retrospective study.
Shanghai Arch Psychiatry. 29:21–29. 2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Huang G, Chen H, Wang Q, Hong X, Hu P,
Xiao M, Shu M and He J: High platelet-to-lymphocyte ratio are
associated with post-stroke depression. J Affect Disord.
246:105–111. 2019.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Chen H, Luan X, Zhao K, Qiu H, Liu Y, Tu
X, Tang W and He J: The association between
neutrophil-to-lymphocyte ratio and post-stroke depression. Clin
Chim Acta. 486:298–302. 2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Huang H, Zheng T, Wang S, Wei L, Wang Q
and Sun Z: Serum 25-hydroxyvitamin D predicts early recurrent
stroke in ischemic stroke patients. Nutr Metab Cardiovasc Dis.
26:908–914. 2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
First MB and Gibbon M: The structured
clinical interview for DSM-IV Axis I disorders (SCID-I) and the
structured clinical interview for DSM-IV Axis II disorders
(SCID-II) In: Comprehensive Handbook of Psychological Assessment,
Vol. 2. Personality assessment. Hilsenroth MJ and Segal DL (eds.).
John Wiley & Sons Inc., Hoboken NJ, 134-143, 2004.
|
|
24
|
Hamilton M: A rating scale for depression.
J Neurol Neurosurg Psychiatry. 23:56–62. 1960.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Brott T, Adams HP Jr, Olinger CP, Marler
JR, Barsan WG, Biller J, Spilker J, Holleran R, Eberle R and
Hertzberg V: Measurements of acute cerebral infarction: A clinical
examination scale. Stroke. 20:864–870. 1989.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Folstein MF, Folstein SE and McHugh PR:
‘Mini-mental state’. A practical method for grading the cognitive
state of patients for the clinician. J Psychiatr Res. 12:189–198.
1975.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Qun S, Tang Y, Sun J, Liu Z, Wu J, Zhang
J, Guo J, Xu Z, Zhang D, Chen Z, et al: Neutrophil-to-lymphocyte
ratio predicts 3-month outcome of acute ischemic stroke. Neurotox
Res. 31:444–452. 2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Buyukkaya E, Karakas MF, Karakas E, Akcay
AB, Tanboga IH, Kurt M and Sen N: Correlation of neutrophil to
lymphocyte ratio with the presence and severity of metabolic
syndrome. Clin Appl Thromb Hemost. 20:159–163. 2014.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Balta S, Celik T, Mikhailidis DP, Ozturk
C, Demirkol S, Aparci M and Iyisoy A: The relation between
atherosclerosis and the neutrophil-lymphocyte ratio. Clin Appl
Thromb Hemost. 22:405–411. 2016.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Zhang RL, Chopp M, Chen H and Garcia JH:
Temporal profile of ischemic tissue damage, neutrophil response,
and vascular plugging following permanent and transient (2H) middle
cerebral artery occlusion in the rat. J Neurol Sci. 125:3–10.
1994.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Ciree A, Michel L, Camilleri-Broet S, Jean
Louis F, Oster M, Flageul B, Senet P, Fossiez F, Fridman WH,
Bachelez H and Tartour E: Expression and activity of IL-17 in
cutaneous T-cell lymphomas (mycosis fungoides and Sezary syndrome).
Int J Cancer. 112:113–120. 2004.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Celikbilek A, Ismailogullari S and
Zararsiz G: Neutrophil to lymphocyte ratio predicts poor prognosis
in ischemic cerebrovascular disease. J Clin Lab Anal. 28:27–31.
2014.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Gibson PH, Cuthbertson BH, Croal BL, Rae
D, El-Shafei H, Gibson G, Jeffrey RR, Buchan KG and Hillis GS:
Usefulness of neutrophil/lymphocyte ratio as predictor of new-onset
atrial fibrillation after coronary artery bypass grafting. Am J
Cardiol. 105:186–191. 2010.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Furtado M and Katzman MA: Examining the
role of neuroinflammation in major depression. Psychiatry Res.
229:27–36. 2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Li W, Ling S, Yang Y, Hu Z, Davies H and
Fang M: Systematic hypothesis for post-stroke depression caused
inflammation and neurotransmission and resultant on possible
treatments. Neuro Endocrinol Lett. 35:104–109. 2014.PubMed/NCBI
|
|
36
|
Afari ME and Bhat T: Neutrophil to
lymphocyte ratio (NLR) and cardiovascular diseases: An update.
Expert Rev Cardiovasc Ther. 14:573–577. 2016.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Li H, Zhou Y, Ma Y, Han S and Zhou L: The
prognostic value of the platelet-to-lymphocyte ratio in acute
coronary syndrome: A systematic review and meta-analysis. Kardiol
Pol. 75:666–673. 2017.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Li DY, Hao XY, Ma TM, Dai HX and Song YS:
The prognostic value of platelet-to-lymphocyte ratio in urological
cancers: A meta-analysis. Sci Rep. 7(15387)2017.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Chandrashekara S, Mukhtar Ahmad M, Renuka
P, Anupama KR and Renuka K: Characterization of
neutrophil-to-lymphocyte ratio as a measure of inflammation in
rheumatoid arthritis. Int J Rheum Dis. 20:1457–1467.
2017.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Demir S, Atli A, Bulut M, İbiloğlu AO,
Güneş M, Kaya MC, Demirpençe Ö and Sır A: Neutrophil-lymphocyte
ratio in patients with major depressive disorder undergoing no
pharmacological therapy. Neuropsychiatr Dis Treat. 11:2253–2258.
2015.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Ivković M, Pantović-Stefanović M,
Dunjić-Kostić B, Jurišić V, Lačković M, Totić-Poznanović S,
Jovanović AA and Damjanović A: Neutrophil-to-lymphocyte ratio
predicting suicide risk in euthymic patients with bipolar disorder:
Moderatory effect of family history. Compr Psychiatry. 66:87–95.
2016.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Mayda H, Ahsen A, Bağcioğlu E, Öztürk A,
Bahçeci B, Soyuçok E, Başpinar E and Ulu MS: Effect of increased
neutrophil-to-lymphocyte ratio (NLR) and decreased mean platelet
volume (MPV) values on inflammation in acute mania. Noro Psikiyatr
Ars. 53:317–320. 2016.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Morel-Kopp MC, McLean L, Chen Q, Tofler
GH, Tennant C, Maddison V and Ward CM: The association of
depression with platelet activation: Evidence for a treatment
effect. J Thromb Haemost. 7:573–581. 2009.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Ormonde do Carmo MB, Mendes-Ribeiro AC,
Matsuura C, Pinto VL, Mury WV, Pinto NO, Moss MB, Ferraz MR and
Brunini TM: Major depression induces oxidative stress and platelet
hyperaggregability. J Psychiatric Res. 61:19–24. 2015.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Gokdemir MT, Karakilcik AZ and Gokdemir
GS: Prognostic importance of paraoxonase, arylesterase and mean
platelet volume efficiency in acute ischaemic stroke. J Pak Med
Assoc. 67:1679–1683. 2017.PubMed/NCBI
|
|
46
|
Dietrich-Muszalska A and Wachowicz B:
Platelet haemostatic function in psychiatric disorders: Effects of
antidepressants and antipsychotic drugs. World J Biol Psychiatry.
18:564–574. 2017.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Zafar MU, Paz-Yepes M, Shimbo D, Vilahur
G, Burg MM, Chaplin W, Fuster V, Davidson KW and Badimon JJ:
Anxiety is a better predictor of platelet reactivity in coronary
artery disease patients than depression. Eur Heart J. 31:1573–1582.
2010.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Mazza MG, Lucchi S, Tringali AGM, Rossetti
A, Botti ER and Clerici M: Neutrophil/lymphocyte ratio and
platelet/lymphocyte ratio in mood disorders: A meta-analysis. Prog
Neuropsychopharmacol Boil Psychiatry. 84:229–236. 2018.PubMed/NCBI View Article : Google Scholar
|
|
49
|
McCorvy JD, Wacker D, Wang S, Agegnehu B,
Liu J, Lansu K, Tribo AR, Olsen RHJ, Che T, Jin J and Roth BL:
Structural determinants of 5-HT2B receptor activation and biased
agonism. Nat Struct Mol Biol. 25:787–796. 2018.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Liu CS, Adibfar A, Herrmann N, Gallagher D
and Lanctot KL: Evidence for inflammation-associated depression.
Curr Top Behav Neurosci. 31:3–30. 2017.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Kayhan F, Gündüz Ş, Ersoy SA, Kandeğer A
and Annagür BB: Relationships of neutrophil-lymphocyte and
platelet-lymphocyte ratios with the severity of major depression.
Psychiatry Res. 247:332–335. 2017.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Esenwa CC and Elkind MS: Inflammatory risk
factors, biomarkers and associated therapy in ischaemic stroke. Nat
Rev Neurol. 12:594–604. 2016.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Nemeroff CB and Musselman DL: Are
platelets the link between depression and ischemic heart disease?
Am Heart J. 140 (4 Suppl)(S57-S62)2000.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Musselman DL, Tomer A, Manatunga AK,
Knight BT, Porter MR, Kasey S, Marzec U, Harker LA and Nemeroff CB:
Exaggerated platelet reactivity in major depression. Am J
Psychiatry. 153:1313–1317. 1996.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Altintas O, Altintas MO, Tasal A,
Kucukdagli OT and Asil T: The relationship of
platelet-to-lymphocyte ratio with clinical outcome and final
infarct core in acute ischemic stroke patients who have undergone
endovascular therapy. Neurol Res. 38:759–765. 2016.PubMed/NCBI View Article : Google Scholar
|