Introduction
Laparoscopic total hysterectomy is a major abdominal
surgery with an operating time of several hours. It is performed
using CO2 insufflation and mechanical ventilation on
patients in the Trendelenburg position under general anesthesia.
Inappropriate mechanical ventilation settings during general
anesthesia may aggravate and even initiate lung damage in patients
with normal lungs, which may theoretically lead to
ventilator-induced lung injury (VILI) (1,2). The
expression of interleukin-8 (IL-8) is stimulated by the classic
pro-inflammatory cytokines tumor necrosis factor and IL-1, which
are released early in the inflammatory response. In particular,
IL-8 is known to participate in the development of lung injury in
adults with acute respiratory distress syndrome (ARDS) (3-5).
Clara cell protein 16 (CC16) is a lung secretory protein (6) with anti-oxidant and anti-inflammatory
properties that is regarded as a sensitive biomarker to potentially
identify lung injury in surgical patients within hours (7,8).
Multiple review articles suggested that lung-protective mechanical
ventilation (LPV) is beneficial during anesthesia in patients with
healthy lungs (9,10), and in individuals with ARDS in
intensive care units (ICU) (11).
Decades of study have demonstrated that LPV may also reduce VILI
(12), via the production of low
tidal volumes (TV) (13) and higher
positive end-expiratory pressure (PEEP) (14), as well as the performance of regular
alveolar recruitment maneuvers (ARM) (15). The effects of different components of
ventilation on improving post-operative outcomes in patients with
normal lungs following surgery have been broadly explored (16). Relevant studies have concluded that
only low TV ventilation reduces post-operative pulmonary
complications (PPCs) effectively and the efficacy afforded by other
components, including the level of PEEP, remains controversial
(17-19).
Moderate fixed PEEP may not suit each patient and it is critical to
determine individualized PEEP to stabilize the lung and maximize
lung protection thereby reducing the risk of VILI. Properly
adjusted PEEP may have a significant protective effect, whereas
inadequate PEEP values may promote pulmonary atelectasis and/or
hyperinflation of dependent lung tissue (20-23).
Therefore, in order for PEEP to be effective, it must be
personalized to suit the individual lung physiology of each
patient. However, the efficacy of using individualized PEEP values
has not been studied thoroughly in laparoscopic total
hysterectomy.
Multiple methods of personalizing PEEP have been
investigated, including inflection points on the pressure/volume
curve, dead space (VD) to TV ratio (VD/TV) or static lung
compliance (Cstat)-directed techniques (24). In the present clinical trial, optimal
PEEP values were determined during a Cstat-directed PEEP titration
procedure to protect from hyperdistention and regular ARM was
performed by volume-controlled ventilation to prevent
atelectasis.
The aim of the present study was to evaluate the
benefit of intra-operative individualized LPV on pulmonary
oxygenation function and the incidence of PPCs in patients
scheduled for laparoscopic total hysterectomy surgery. It was
hypothesized that intra-operative individualized LPV may improve
pulmonary oxygenation function and decrease the total occurrence of
PPCs compared to conventional ventilation during anesthesia in
patients undergoing laparoscopic total hysterectomy surgery.
Materials and methods
Study design
All patients provided written informed consent prior
to inclusion in the study. The present study was a randomized,
double-blinded, controlled, investigator-initiated clinical trial
and was approved by the Ethical Committee of Huzhou Maternal and
Child Healthcare Hospital (approval no. 20180206-9; Huzhou, China).
Investigators randomly assigned participants to the PV group or the
CV group at a ratio of 1:1. Concealed randomization was performed
using Random Allocation Software (Windows software, version 1.0;
Microsoft Corp.). The group-identification information was stored
in sealed and numbered envelopes. Participants were included and
allocated in numerical order.
The anesthetist was responsible for the collection
of patient data during surgery. Ventilator settings recorded during
anesthesia were concealed in the case report form. The surgeon
responsible for the patient was not informed of the ventilator
settings. Physicians that were not involved in the care of the
patient during anesthesia and surgery performed post-operative
evaluation. Anesthesia recordings and ventilator settings during
surgery were concealed from the post-operative physicians and
nurses.
Inclusion and exclusion criteria
Patients who were scheduled for elective
laparoscopic total hysterectomy surgery under general anesthesia
between January 2017 and January 2019 at Huzhou Maternal and Child
Healthcare Hospital were included in the present study. Patients
were eligible for participation if they conformed to the following
criteria: American Society of Anesthesiologists (ASA) physical
status I-III; age of ≥18 years; body mass index (BMI) <30
kg/m2; candidates for elective laparoscopic total
hysterectomy surgery under general anesthesia with an expected
duration of >2 h. The exclusion criteria were as follows:
Individuals who refused or were unable to provide informed consent,
or were participating in another interventional study; neuropathy
or any neuromuscular disease; thoracic deformity and intrathoracic
diseases (e.g. mediastinal tumor or chest tumor); severe cardiac
disease defined as New York Heart Association grade III or IV,
acute coronary syndrome or persistent ventricular tachyarrhythmias;
any previous lung surgery or history of pulmonary disease; use of
positive pressure ventilation prior to surgery [e.g. continuous
positive airway pressure for sleep obstructive apnea syndrome
(CPAP)]; liver cirrhosis (Child-Pugh score B or C); chronic renal
failure with dialysis; allergy to local anesthetic; emergency
surgery; or the requirement for the patient to be transferred to
the ICU after surgery.
Standard procedures
All patients accepted a standard procedure of
general anesthesia induction comprising intravenous midazolam
hydrochloride (0.05 mg/kg; Jiangsu Enhua Medical Co.), sufentanyl
(0.6 µg/kg; Yichang Renfu Medical Co.), propofol (2 mg/kg; Xi An Li
Bang Medical Co.) and rocuronium bromide (0.6 mg/kg; Zhe Jiang Xian
Ju Medical Co.). After 3 min, patients were intubated with a
tracheal tube (internal diameter, 7 mm for females), and the tube
cuff pressure was adjusted between 20 and 25 cmH2O.
Maintenance anesthesia was provided by continuous intravenous
propofol infusion (4-12 mg/kg/h), remifentanil infusion (0.05-0.3
µg/kg/min) and sevoflurane inhalation (concentration, 1-3%) based
on the BiSpectral index of the patient, which was maintained at
40-60. As continuous intravenous propofol and remifentanil infusion
were provided to maintain anesthesia and inhibit respiration,
additional cisatracurium besilate (5 mg) was prescribed when
clinically indicated to produce further muscle relaxation. Routine
intra-operative monitoring was performed continuously using a
dedicated monitor, including invasive blood pressure, pulse
oximetry, heart rate, end-tidal fractions of carbon dioxide
(ETCO2) and electrocardiogram. Immediately prior to the
end of the operation, tolane setron (5 mg) was administered to
prevent post-operative nausea and vomiting. After the surgery,
patients were directly transported to the post-anesthesia care
unit. After tracheal extubation, patients were oxygenated with an
inspired oxygen fraction (FiO2) of 0.33 through a
venturi face mask (Tian Jin Shuang Li Medical Device Co., Ltd).
Following surgery, the patients received intravenous
continuous analgesia in the form of sufentanyl (50 µg) and
dexmedetomidine (200 µg), combined with 100 ml normal saline to
control pain. The background dose was 2 ml/h and the bolus dose was
2 ml. Post-operative analgesia was provided for at least 48 h to
achieve a visual analogue scale (VAS) score of <3(25). If the VAS score was ≥3, intravenous
tramadol (50 mg) was to be administered for remedial analgesia, but
none of the patients was given tramadol in the present study as the
VAS scores were ≥3. All patients received routine physiotherapy
(26) during the post-operative
period according to the standard of care at Huzhou Maternal and
Child Healthcare Hospital (Huzhou, China).
Ventilation protocol
In the two groups, the surgery was performed under
pneumoperitoneum induced and held using an intra-abdominal pressure
of 13-15 mmHg with room-temperature CO2 insufflation.
The mechanical ventilation protocol consisted of a
volume-controlled mode with an FiO2 of 0.40 and an
inspiratory to expiratory ratio of 1:2 in the two groups, which was
performed using an S/5 Avance anesthesia machine (Datex Ohmeda; GE
Healthcare). The respiratory rate (RR) was regulated to obtain an
ETCO2 of 35-45 mmHg.
Patients were randomly assigned to the CV group or
the PV group. In the CV group, the ventilation protocol was TV of 9
ml/kg of ideal body weight (IBW), without PEEP or ARM throughout
the surgery. The IBW was calculated according to the following
pre-defined formula for females (27): IBW (kg)=45.5 + 0.91 (height in
cm-152.4).
In the PV group, the ventilation protocol settings
were the same as those in the CV group immediately after induction
of anesthesia and orotracheal intubation. However, once a steady
state had been reached, all patients were submitted to an ARM using
sustained airway pressure via the CPAP method, applying TV of 7
ml/kg IBW and 30 cm H2O PEEP for 30 sec based on a study
by Ruszkai et al (28),
followed by a decremental PEEP titration (DPT) procedure directed
by Cstat. The depth of anesthesia was regulated to ensure the
patients were haemodynamically stable and a
PaO2/FiO2 of ≥300 mmHg was also guaranteed to
assure that the pulmonary oxygenation function was normal. If so,
the ARM was considered successful.
The method of DPT was as follows (28): During the PEEP titration procedure,
PEEP was decreased from 14 cm H2O by 2 cm H2O
every 4 min, until a final PEEP of 6 cm H2O was reached.
On each level of PEEP, Cstat was measured by the ventilator.
Optimal PEEP was considered as the PEEP value resulting in the
highest possible Cstat measurement. After the PEEP titration
procedure, an ARM was implemented and lung-protective mechanical
ventilation was then performed using the optimal PEEP and TV of 7
ml/kg.
Data source and collection
The following demographic parameters were recorded
for the 87 patients enrolled: Age, BMI, ASA physical status and
post-operative length of stay (PLOS). The intra-operative data,
including operation time, mechanical ventilation time, TV, RR and
arousal time (time from the end of the operation to the time the
patients woke up) were recorded for the two groups. Breathing
mechanics [pulmonary dynamic compliance (Cdyn)] were calculated as
TV (peak-PEEP) (24) in the
operative period at time-point 1 (T1; after endotracheal
intubation), T2 (10 min after pneumoperitoneum), T3 (60 min after
pneumoperitoneum) and T4 (10 min after pneumoperitoneum was
stopped). Arterial blood gas (ABG) was recorded at T1, T3, T5 (30
min after tracheal extubation) and T6 (the day after the surgery).
The lung oxygenation ability was assessed by determining the oxygen
index (OI) calculated from the pressure of arterial oxygen
(PaO2) and FiO2 as
OI=PaO2/FiO2 (29). Alveolar-arterial differences for
oxygen (A-aO2) were calculated from the atmospheric
pressure (PB), saturated vapor pressure at room temperature
(PH2O), pressure of arterial carbon dioxide
(PaCO2) and respiration quotient (R), PaO2
and FiO2 as A-aO2=(PB-PH2O) x
FiO2-PaCO2/R-PaO2 (30), with PB set at 760 mmHg,
PH2O at 47 mmHg and R at 0.8. Saturation of pulse
oxygenation (SPO2) was recorded on the second day after
surgery (D2) and D5. SPO2 was measured in the ward. If
the patient was using a nasal oxygen catheter, the catheter was
removed for 10 min and SPO2 was then measured after
adaptation on D2 and D5. If SPO2 dropped <90% during
the adaptive time, the manipulation was stopped and SPO2
was immediately obtained. Venous blood samples were taken at T1,
T3, T5 and T6 to assess the systemic inflammatory response. Venous
blood samples of the patients were centrifuged at 5,000 x g for 10
min at 4˚C, and supernatants were separated immediately after
collection. All supernatants were stored at -80˚C until biochemical
measurements were performed. eBioscience Platinum ELISA (Bender
MedSystems GmbH) was used to measure the serum levels of IL-8 and
CC16. Post-operative follow-up was performed and the total
incidence rate of PPCs in the two groups during the first 7
post-operative days was recorded. PPCs were defined as the
development of one of seven complications: Atelectasis, pleural
effusion, respiratory infection, pneumothorax, bronchospasm,
respiratory failure and aspiration pneumonitis during the period of
post-operative hospitalization, as reported by Jammer et al
(31) and Gallart and Canet
(32).
Primary and secondary endpoints
The primary endpoint was the change in pulmonary
oxygenation function including OI during the pre-and post-operative
period. The secondary endpoints were Cdyn during the operation and
the total incidence of PPCs in the first 7 days after surgery.
Post-operative pneumonia was diagnosed based on 3 criteria: i)
Presence of new pulmonary infiltrates from chest X-ray images; ii)
leukocytosis and iii) fever (ear temperature, ≥38.0˚C) (33,34).
Statistical analysis
The formula for calculation of the sample size was
as follows: n=[(Zα/2 + Zβ) 2x2 (SD) 2/(µ1-µ2) 2] (35), where n represents the sample size
required in each group, µ1 is the mean of the OI in the PV group,
µ2 is the mean of the OI in the CV group; µ1-µ2 is the clinically
significant difference; Zα/2 represents a 5% level of significance
(1.96); Zβ represents 95% statistical power (1.96) and SD
represents the standard deviation, which was 1.195. A pilot study
was performed on 16 patients (8 in each group) to detect a
significant difference in OI between groups, during which µ1 was
measured as 1.05 and µ2 as 1.25. The OI was obtained during the
pilot study at T3 (60 min after pneumoperitoneum) and T4 (10 min
after pneumoperitoneum was stopped). Therefore, n was equal to 35
for each group, requiring a total sample size of 70. Considering a
20% attrition rate, the total sample size was increased to 86
patients (43 patients in each group). Statistical analysis was
performed using SPSS version 17 (SPSS Inc.). The normality of
distribution of continuous variables was tested using one-sample
Kolmogorov-Smirnov test. Continuous data were analyzed using
one-way ANOVA to assess the significance of differences in means
between and within the groups. If the variance was not homogeneous,
a non-parametric test (Kruskal-Wallis H-test for multiple
independent samples) was used. Categorical variables were compared
using the RxC χ2 test or Fisher's exact test. In all
cases, P-values were two-sided and P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient enrolment and follow-up
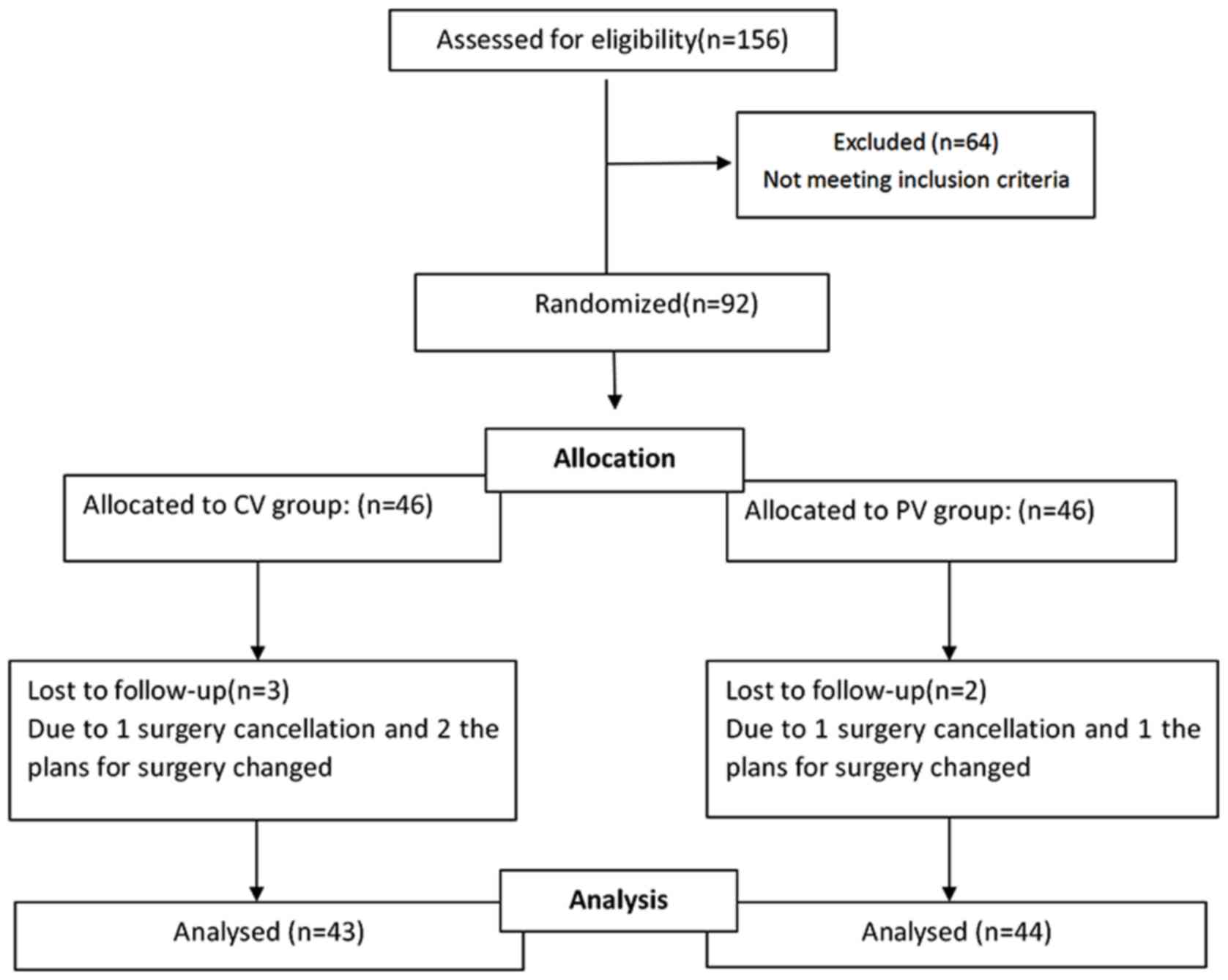
A flow chart of the enrolment and follow-up of the
patients is provided in Fig. 1. A
total of 156 consecutive patients who were scheduled to undergo
laparoscopic total hysterectomy surgery were assessed for
eligibility. Of these, 64 patients were excluded, as they did not
meet the inclusion criteria. The remaining 92 patients were
included in the study and were divided into 2 groups with 46
patients each in the CV group and the PV group. The surgery was
cancelled for 2 patients assigned to the CV group and 1 patient
assigned to the PV group. In addition, 2 patients assigned to the
CV group and 1 patient assigned to the PV group were excluded, as
the plans for surgery changed. Finally, 87 patients were enrolled
and included in the final analysis, comprising 43 in the CV group
and 44 in the PV group. In terms of the baseline characteristics,
there were no significant differences between the two groups
(Table I).
 | Table IBaseline characteristics of the
patients. |
Table I
Baseline characteristics of the
patients.
| Parameter | CV group
(n=43) | PV group
(n=44) | P-value |
|---|
| Age (years) | 50.32±9.83 | 51.08±8.86 | 0.72 |
| BMI
(kg/m2) | 22.58±3.05 | 23.31±3.98 | 0.34 |
| ASA score |
|
I | 8 (18.60) | 6 (13.64) | 0.53 |
|
II | 30 (69.77) | 34 (77.27) | 0.43 |
|
III | 5 (11.63) | 4 (9.09) | 0.70 |
| History of
hypertension | 10 (23.26) | 9 (20.45) | 0.75 |
| History of
cardiopathy | 5 (11.63) | 3 (5.82) | 0.44 |
| History of
smoking | 3 (6.98) | 4 (9.09) | 0.72 |
| PLOS (days) | 6.56±1.23 | 7.02±2.16 | 0.23 |
Intra-operative data of the two
groups
Compared with those in the CV group, the TV was
lower and the RR was higher in the PV group; however, there were no
statistically significant differences between the two groups with
regard to intra-operative mechanical ventilation time, operation
time and arousal time (Table
II).
| Table IIIntra-operative data. |
Table II
Intra-operative data.
| Parameter | CV group
(n=43) | PV group
(n=44) | P-value |
|---|
| Mechanical
ventilation time (min) | 145.97±60.02 | 156.15±50.43 | 0.41 |
| Operation time
(min) | 125.03±34.23 | 127.21±44.26 | 0.82 |
| Tidal volume
(ml) | 535.64±59.18 | 440.64±55.37 | 0.00 |
| RR
(breaths/min) | 12.59±1.67 | 13.54±1.43 | 0.01 |
| Arousal time
(min) | 15.68±9.34 | 14.73±8.69 | 0.33 |
| Crystalloid volume
(ml/kg) | 18.26±3.41 | 18.55±4.17 | 0.72 |
| Colloid volume
(ml/kg | 9.29±2.00 | 9.14±1.79 | 0.71 |
| Urine output
(ml/kg) | 1.38±0.57 | 1.41±0.65 | 0.79 |
| Blood loss
(ml) | 83.82±27.38 | 89.25±34.87 | 0.42 |
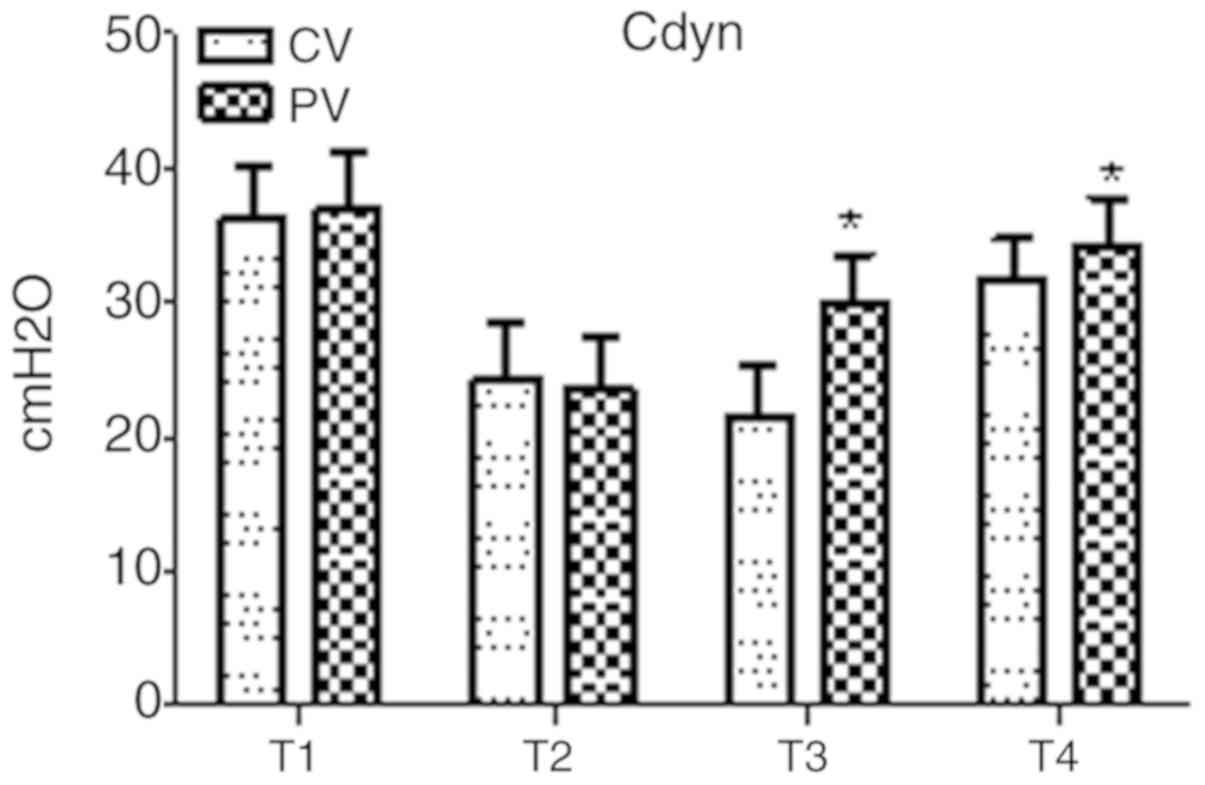
Breathing mechanics during the operative period in
the two groups are presented in Fig.
2. In the two groups, Cdyn exhibited a marked decline at T2 as
compared with that at T1, but no statistical significance was
found. Compared with that in the CV group, Cdyn was significantly
elevated in the PV group at T3 and T4 (P<0.05).
Pulmonary oxygenation
The pulmonary oxygenation during the operative and
post-operative period for the two groups is presented in Figs.
3-5. In the PV group, the OI value was higher and the
A-aO2 was lower compared with those in the CV group at
T3, T5 and T6 (P<0.05). Furthermore, in the PV group,
SPO2 was higher compared with that in the CV group on D2
and D5 (P<0.05).
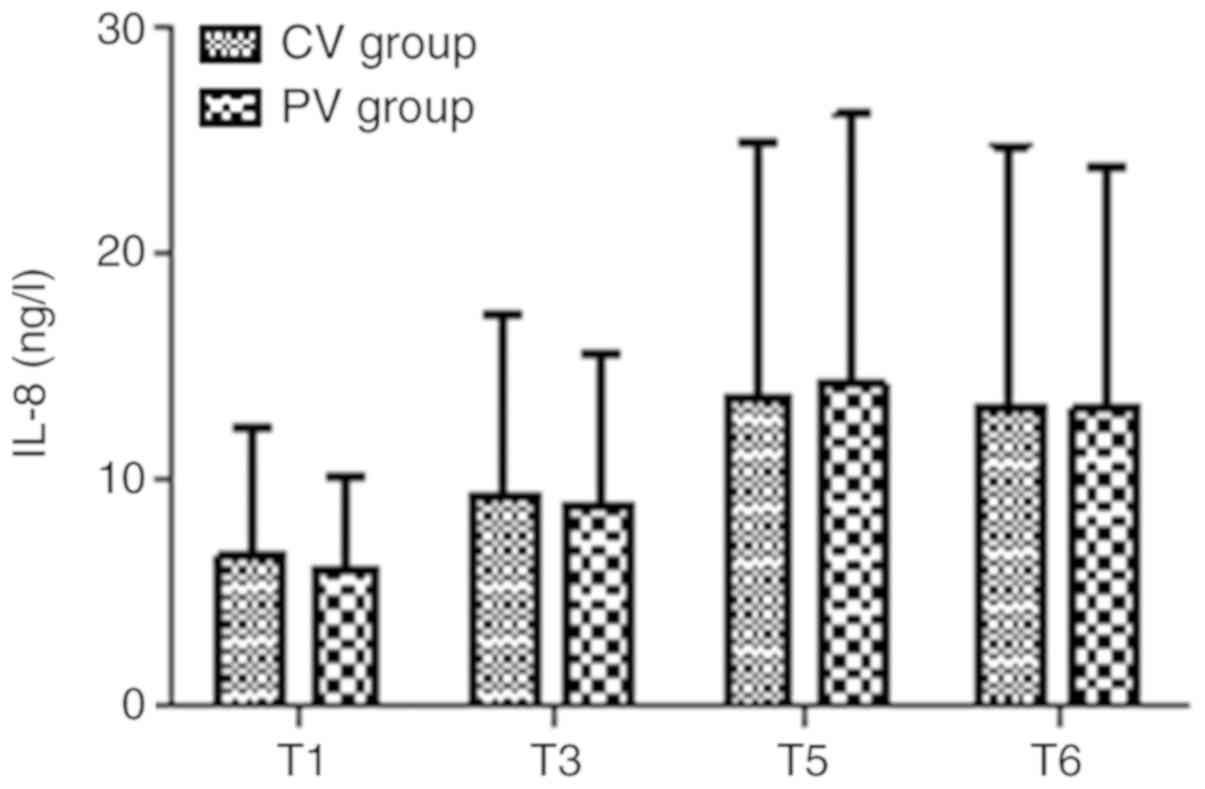
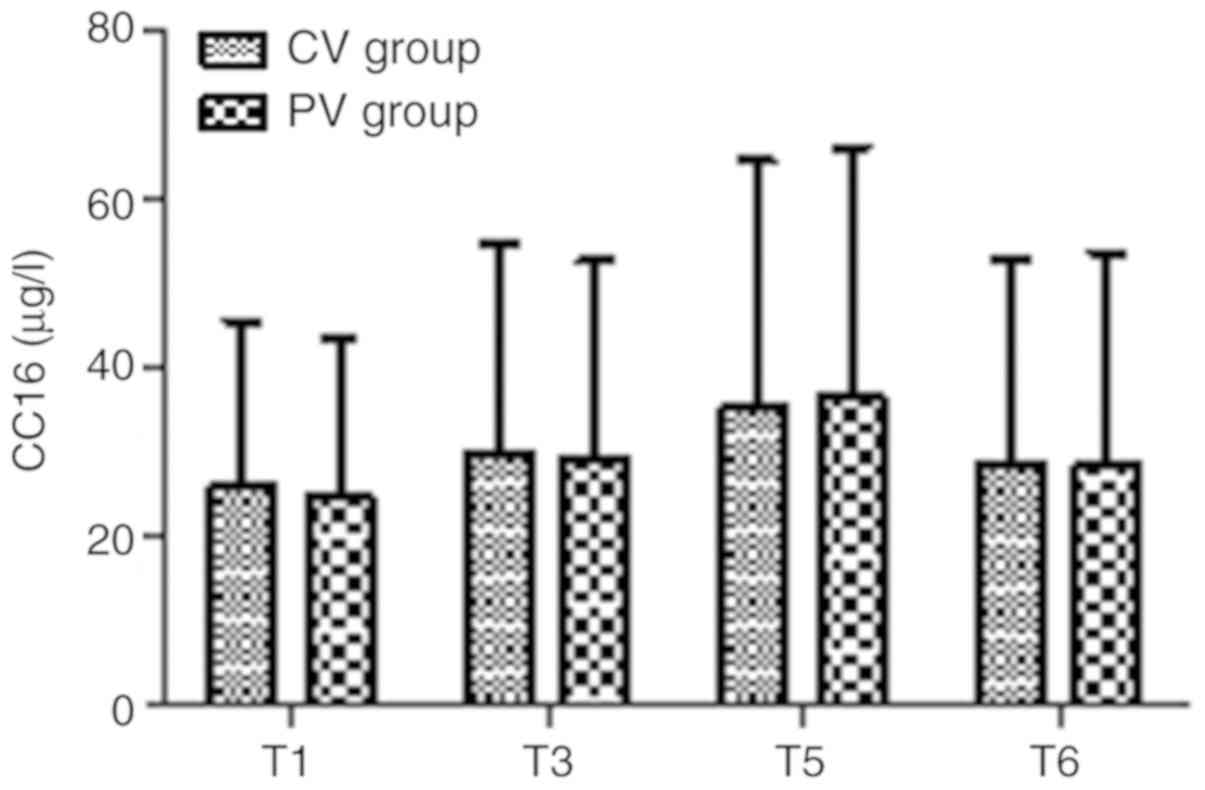
Inflammatory factors
The inflammatory factors IL-8 and CC16 in the two
groups at T1, T3, T5 and T6 are presented in Figs. 6 and 7. There were no significant differences in
IL-8 and CC16 in the two groups at any time-point (P>0.05).
Incidence of PPCs
The total incidence of PPCs was compared
post-operatively in the two groups during the first 7 days after
surgery (Table III). Pneumothorax,
bronchospasm, respiratory failure and aspiration pneumonitis did
not occur in either group. Compared with the CV group, there was no
difference in the incidence of respiratory infection and pleural
effusion in the PV group (P>0.05). However, the total incidence
of PPCs and atelectasis in the CV group was higher compared with
that in the PV group (P<0.05).
| Table IIIOccurrence of PPCs during the first 7
days after surgery in the two groups. |
Table III
Occurrence of PPCs during the first 7
days after surgery in the two groups.
| Item | CV group
(n=43) | PV group
(n=44) | P-value |
|---|
| Atelectasis | 4 (9.3) | 0 (0) | 0.04 |
| Pleural
effusion | 2 (4.65) | 1 (2.27) | 0.54 |
| Respiratory
infection | 5 (11.63) | 3 (6.82) | 0.44 |
| Total incidence of
PPCs | 11 (25.58) | 4 (9.09) | 0.04 |
Discussion
In the present study, pulmonary dynamic Cdyn,
pulmonary oxygenation, serum inflammatory factors and the total
incidence of PPCs were compared between a CV and a PV group. It was
observed that, compared with conventional mechanical ventilation
without PEEP, individualized lung PV performed by applying
personalized PEEP and regular ARM was associated with improved
pulmonary dynamic Cdyn and pulmonary oxygenation function, as well
as a reduced incidence of PPCs during the first 7 days following
surgery in patients undergoing laparoscopic total hysterectomy.
However, during the peri-operative period, no significant
differences were observed in terms of PLOS and inflammatory factors
between patients managed using the different ventilatory
strategies.
Laparoscopic total hysterectomy is widely used and
its advantages are generally accepted to include less invasive
surgery, better cosmetic results and reduced duration of hospital
stay on the basis of the surgical technique in most advanced
facilities. Despite this, certain features of laparoscopic
techniques, including the Trendelenburg position and induction of
pneumoperitoneum with CO2, have been reported to be
potential risk factors for an increased incidence of PPC (36).
The beneficial effects of LPV have been demonstrated
in patients with healthy lungs during general anesthesia (10,37). LPV
has also been indicated to be superior in patients with severe lung
injury and ARDS in ICU settings. Application of PEEP, as an
important component of LPV, is currently the primary strategy by
which to minimize dynamic strain for established ARDS. However, the
continued high mortality rate of ARDS indicates that the current
PEEP strategies are not always effective (20).
Therefore, the aims of the current study were to
incorporate personalized PEEP into laparoscopic total hysterectomy
surgery and to evaluate the effects of intra-operative
individualized LPV on clinical outcomes compared with those of
conventional mechanical ventilation. It was hypothesized that
individualized LPV may improve lung oxygenation function compared
to conventional mechanical ventilation, and may therefore reduce
the incidence of PPCs in patients undergoing laparoscopic total
hysterectomy.
In the present study, individualized PEEP values
were determined during a Cstat-directed PEEP titration procedure to
protect from hyperdistention, and regular ARM was performed using
sustained airway pressure by the CPAP method to prevent atelectasis
(22,38,39). In
the PV group, ARM did not cause any hemodynamic instability or
life-threatening events, including a decrease in systolic blood
pressure or heart rate. During the course of mechanical
ventilation, LPV is preferred to reduce regional end-inspiratory
stretch, which also maintains the lung open to improve gas
exchange, obtain better pulmonary oxygenation function and
pulmonary Cdyn in healthy adult lungs. The patients in the PV group
exhibited improved arterial oxygenation and peripheral oxygen
saturation in the peri-operative period, which is in line with the
results of a study by Severgnini et al (40), implying that a low TV with adequate
PEEP is beneficial for avoiding deoxygenation.
In the present study, individualized LPV strategy
was beneficial in the early post-operative period. Certain adverse
effects, including atelectasis, pleural effusion and respiratory
infection, are linked to mechanical ventilation. Atelectasis and
pleural effusion are diagnosed by chest X-ray or CT. In the present
study, pneumothorax, bronchospasm, respiratory failure and
aspiration pneumonitis were not observed in the two groups.
Atelectasis, pleural effusion and respiratory infection occurred in
the two groups; however, no significant difference was present in
the incidence of pleural effusion and respiratory infection. The
rate of post-operative atelectasis was higher in the CV group
compared with that in the PV group (9.3 vs. 0%; P<0.05), as
evaluated using chest X-ray or CT, and the total incidence rate of
PPCs during the early period after the operation in the CV group
was also higher compared with that in the PV group (25.58 vs.
9.09%; P<0.05). These results suggest that LPV with
individualized PEEP and regular RM during surgery may contribute to
the prevention of ventilation-induced atelectasis and to improve
pulmonary oxygenation function.
The results of the present study are consistent with
those of previous studies (41).
However, as the sample size was small, it was not possible to
demonstrate a notable decrease in the incidence of long-term major
PPCs.
Although LPV was indicated to be associated with
reduced PPCs in the present study, no significant difference was
obtained in the serum levels of the inflammatory factors IL-8 and
CC16 during and after surgery, and the PLOS was similar between the
groups. Previous studies demonstrated that invasive mechanical
ventilation may change the course of existing inflammation in
patients with ARDS. The results of the present study suggest that
the difference in ventilatory strategy during surgery alone does
not change the inflammatory process in patients without a history
of pulmonary disease. It is possible that the ventilation period
may have been too short to produce changes in certain inflammatory
mediators due to the long duration of transcriptional and
translational processes. In the present study, the same
intra-operative infusion was adopted in the two groups to exclude
any differences in inflammatory markers. Even though
intra-operative infusion may have affected the serum levels of IL-8
and CC16, the influence was identical in the two groups.
Laparoscopic total hysterectomy is considered to be
a minimally invasive surgical procedure and the increased
inflammatory biomarkers in the two groups in the post-operative
period (T3, T5 and T6) may have been due to the surgery itself.
Ventilatory strategy alterations during surgery alone are not
considered to be sufficient to change the inflammatory processes in
patients without a history of pulmonary disease. All patients
received routine physiotherapy and antibiotics according to the
standard care at our hospital at the post-operative stage,
including encouragement to cough, pats on the back and turning
over. The inflammatory factors increased slightly, and there was no
significant difference between the two groups. The results of the
present study are similar to those of previous studies with regard
to inflammatory mediators (42,43) and
PLOS (44).
The present study had certain potential limitations.
First, the effects of ventilation strategies on major PPCs are not
a major focus of the present study, as the sample size was too
small. Furthermore, the study included only female patients, as a
gynecological disease was being treated. In addition, the patients
were only followed up for the first 7 days after surgery. Hence,
longitudinal studies are required to demonstrate the long-term
clinical impact on the incidence rates of PPCs.
In conclusion, the results of the present study
demonstrated that protective ventilation strategies in laparoscopic
total hysterectomy with low TV, intra-operative individualized PEEP
and regular ARM during surgery are able to significantly improve
pulmonary oxygenation function and reduce the total incidence of
PPCs and atelectasis. However, larger prospective randomized trials
on different types of surgery, including mixed-gender populations
and long-term evaluation after surgery, are recommended in the
future to determine the benefit of low TV together with
individualized optimal PEEP for the patient.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Public
Welfare Technology Research Project of the Huzhou Science and
Technology Bureau (grant no. 2019GYB55) and the Zhejiang Province
Medical Science and Technology Plan (grant no. 2020KY932).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JL contributed to the study conception and design,
data acquisition, statistical analysis, data interpretation and
drafting of the manuscript. XH contributed to the statistical
analysis and data interpretation and revised the manuscript. SH
contributed to the study design and data acquisition and revised
the manuscript. ZM contributed to the study conception and design,
performed data interpretation and revised the manuscript. HH
contributed to data acquisition and revised the manuscript. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Institutional Ethics
Committee of Huzhou Maternal and Child Healthcare Hospital (Huzhou,
China) and was performed in accordance with the ethical standards
set by the 1964 Declaration of Helsinki and its later amendments.
Written informed consent was obtained from all patients or their
legal representative prior to enrollment in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Slutsky AS and Ranieri VM:
Ventilator-induced lung injury. N Engl J Med. 369:2126–2136.
2013.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ricard JD, Dreyfuss D and Saumon G:
Ventilator-induced lung injury. Eur Respir J. Suppl 42(2s-9s)2003.
View Article : Google Scholar
|
|
3
|
Ware LB, Koyama T, Zhao Z, Janz DR,
Wickersham N, Bernard GR, May AK, Calfee CS and Matthay MA:
Biomarkers of lung epithelial injury and inflammation distinguish
severe sepsis patients with acute respiratory distress syndrome.
Crit Care. 17(R253)2013.PubMed/NCBI View
Article : Google Scholar
|
|
4
|
Famous KR, Delucchi K, Ware LB, Kangelaris
KN, Liu KD, Thompson BT and Calfee CS: ARDS Network: Acute
respiratory distress syndrome subphenotypes respond differently to
randomized fluid management strategy. Am J Respir Crit Care Med.
195:331–338. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Bos LD, Schouten LR, van Vught LA, Wiewel
MA, Ong DSY, Cremer O, Artigas A, Martin-Loeches I, Hoogendijk AJ,
van der Poll T, et al: Identification and validation of distinct
biological phenotypes in patients with acute respiratory distress
syndrome by cluster analysis. Thorax. 72:876–883. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Broeckaert F and Bernard A: Clara cell
secretory protein (CC16): Characteristics and perspectives as lung
peripheral biomarker. Clin Exp Allergy. 30:469–475. 2000.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Fernandez-Bustamante A, Klawitter J,
Repine JE, Agazio A, Janocha AJ, Shah C, Moss M, Douglas IS, Tran
ZV, Erzurum SC, et al: Early effect of tidal volume on lung injury
biomarkers in surgical patients with healthy lungs. Anesthesiology.
121:469–481. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wutzler S, Lehnea T, Laurer H, Lehnert M,
Becker M, Henrich D, Vogl T and Marzi I: Circulating levels of
clara cell protein 16 but not surfactant protein D identify and
quantify lung damage in patients with multiple injuries. J Tranma.
71(E31-E36)2011.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Futier E, Constantin JM, Paugam-Burtz C,
Pascal J, Eurin M, Neuschwander A, Marret E, Beaussier M, Gutton C,
Lefrant JY, et al: A trial of intraoperative low-tidal-volume
ventilation in abdominal surgery. N Engl J Med. 369:428–437.
2013.PubMed/NCBI View Article : Google Scholar
|
|
10
|
PROVE Network Investigators for the
Clinical Trial Network of the European Society of Anaesthesiology
, Hemmes SN, Gama de Abreu M, Pelosi P and Schultz MJ: High
versus low positive end-expiratory pressure during general
anaesthesia for open abdominal surgery (PROVHILO trial): A
multicentre randomised controlled trial. Lancet. 384:495–503.
2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Brower RG, Lanken PN, MacIntyre N, Matthay
MA, Morris A, Ancukiewicz M, Schoenfeld D and Thompson BT: National
Heart Lung and Blood Institute ARDS Clinical Trials Network: Higher
versus lower positive end-expiratory pressures in patients with the
acute respiratory distress syndrome. N Engl J Med. 351:327–336.
2004. View Article : Google Scholar
|
|
12
|
Jaber S, Coisel Y, Chanques G, Futier E,
Constantin J, Michelet P, Beaussier M, Lefrant JY, Allaouchiche B,
Capdevila X and Marret E: A multicentre observational study of
intra-operative ventilatory management during general anaesthesia:
Tidal volumes and relation to body weight. Anaesthesia.
67:999–1008. 2012.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Haliloglu M, Bilgili B, Ozdemir M,
Umuroglu T and Bakan N: Low tidal volume positive end-expiratory
pressure versus high tidal volume zero-positive end-expiratory
pressure and postoperative pulmonary functions in robot-assisted
laparoscopic radical prostatectomy. Med Princ Pract. 26:573–578.
2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Hansen JK, Anthony DG, Li L, Wheeler D,
Sessler DI and Bashour CA: Comparison of positive end-expiratory
pressure of 8 versus 5 cm H2O on outcome after cardiac
operations. J Intensive Care Med. 6:338–343. 2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Reis Miranda D, Gommers D, Struijs A,
Dekker R, Mekel J, Feelders R, Lachmann B and Bogers AJ:
Ventilation according to the open lung concept attenuates pulmonary
inflammatory response in cardiac surgery. Eur J Cardiothorac Surg.
28:889–895. 2005.PubMed/NCBI View Article : Google Scholar
|
|
16
|
García-Delgado M, Navarrete-Sánchez I and
Colmenero M: Preventing and managing perioperative pulmonary
complications following cardiac surgery. Curr Opin Anaesthesiol.
27:146–152. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Serpa Neto A, Hemmes SN, Barbas CS,
Beiderlinden M, Biehl M, Binnekade JM, Canet J,
Fernandez-Bustamante A, Futier E, Gajic O, et al: Protective versus
conventional ventilation for surgery. A systematic review and
individual patient data meta-analysis. Anesthesiology. 123:66–78.
2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Zhang Z, Hu X, Zhang X, Zhu X, Chen L, Zhu
L, Hu C and Du B: China Critical Care Clinical Trials Group
(CCCCTG): Lung protective ventilation in patients undergoing major
surgery: A systematic review incorporating a Bayesian approach. BMJ
Open. 5(e007473)2015.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Yang D, Grant MC, Stone A, Wu CL and Wick
EC: A meta-analysis of intraoperative ventilation strategies to
prevent pulmonary complications: Is tidal volume alone sufficient
to protect healthy lungs? Ann Surg. 263:881–887. 2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Villar J, Blanco J and Kacmarek RM:
Current incidence and outcome of the acute respiratory distress
syndrome. Curr Opin Crit Care. 22:1–6. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Levin MA, McCormick PJ, Lin HM, Hosseinian
L and Fischer GW: Low intraoperative tidal volume ventilation with
minimal PEEP is associated with increased mortality. Br J Anaesth.
113:97–108. 2014.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Vargas M, Sutherasan Y, Gregoretti C and
Pelosi P: PEEP role in ICU and operating room: From pathophysiology
to clinical practice. ScientificWorldJournal.
2014(852356)2014.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Menendez C, Martinez-Caro L, Moreno L, Nin
N, Moral-Sanz J, Morales D, Cogolludo A, Esteban A, Lorente JA and
Perez-Vizcaino F: Pulmonary vascular dysfunction induced by high
tidal volume mechanical ventilation. Crit Care Med.
41(e149-e155)2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Nieman GF, Satalin J, Andrews P, Aiash H,
Habashi NM and Gatto LA: Personalizing mechanical ventilation
according to physiologic parameters to stabilize alveoli and
minimize ventilator induced lung injury (VILI). Intensive Care Med
Exp. 5(8)2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kishida M, Yamada Y, Inayama E, Kitamura
M, Nishino T, Ota K, Shintani A and Ikenoue T: Effectiveness of
music therapy for alleviating pain during haemodialysis access
cannulation for patients undergoing haemodialysis: A
multi-facility, single-blind, randomised controlled trial. Trials.
20(631)2019.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lawrence VA, Cornell JE and Smetana GW:
American College of Physicians: Strategies to reduce postoperative
pulmonary complications after noncardiothoracic surgery: Systematic
review for the American college of physicians. Ann Intern Med.
144:596–608. 2006.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Güldner A, Kiss T, Serpa Neto A, Hemmes
SN, Canet J, Spieth PM, Rocco PR, Schultz MJ, Pelosi P and Gama de
Abreu M: Intraoperative protective mechanical ventilation for
prevention of postoperative pulmonary complications: A
comprehensive review of the role of tidal volume, positive
end-expiratory pressure, and lung recruitment maneuvers.
Anesthesiology. 123:692–713. 2015.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Ruszkai Z, Kiss E, László I, Gyura F,
Surány E, Bartha PT, Bokrétás GP, Rácz E, Buzogány I, Bajory Z, et
al: Effects of intraoperative PEEP optimization on postoperative
pulmonary complications and the inflammatory response: Study
protocol for a randomized controlled trial. Trials.
18(375)2017.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Marret E, Cinotti R, Berard L, Piriou V,
Jobard J, Barrucand B, Radu D, Jaber S, Bonnet F and the PPV study
group : Protective ventilation during anaesthesia reduces
major postoperative complications after lung cancer surgery: A
double-blind randomised controlled trial. Eur J Anaesthesiol.
35:727–735. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Okada S, Ito K, Shimada J, Kato D,
Shimomura M, Tsunezuka H, Miyata N, Ishihara S, Furuya T and Inoue
M: Clinical application of postoperative non-invasive positive
pressure ventilation after lung cancer surgery. Gen Thorac
Cardiovasc Surg. 66:565–572. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Jammer I, Wickboldt N, Sander M, Smith A,
Schultz MJ, Pelosi P, Leva B, Rhodes A, Hoeft A, Walder B, et al:
Standards for definitions and use of outcome measures for clinical
effectiveness research in perioperative medicine: European
perioperative clinical outcome (EPCO) definitions: A statement from
the ESA-ESICM joint taskforce on perioperative outcome measures.
Eur J Anaesthesiol. 32:88–105. 2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Gallart L and Canet J: Post-operative
pulmonary complications: Understanding definitions and risk
assessment. Best Pract Res Clin Anaesthesiol. 29:315–330.
2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Arslantas MK, Kara HV, Tuncer BB,
Yildizeli B, Yuksel M, Bostanci K, Bekiroglu N, Kararmaz A, Cinel I
and Batirel HF: Effect of the amount of intraoperative fluid
administration on postoperative pulmonary complications following
anatomic lung resections. J Thorac Cardiovasc Surg. 149314–320.
(321.e1)2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Mommers EHH, Wegdam JA, van der Wolk S,
Nienhuijs SW and de Vries Reilingh TS: Impact of hernia volume on
pulmonary complications following complex hernia repair. J Surg
Res. 211:8–13. 2017.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Faul F, Erdfelder E, Buchner A and Lang
AG: Statistical power analyses using G* Power 3.1: Tests
for correlation and regression analyses. Behav Res Methods.
41:1149–1160. 2009.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Smetana GW, Lawrence VA and Cornell JE:
American College of Physicians: Preoperative pulmonary risk
stratification for noncardiothoracic surgery: Systematic review for
the American college of physicians. Ann Intern Med. 144:581–595.
2006.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Futier E and Jaber S: Lung-protective
ventilation in abdominal surgery. Curr Opin Crit Care. 20:426–430.
2014.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Sutherasan Y, Vargas M and Pelosi P:
Protective mechanical ventilation in the non-injured lung: Review
and meta-analysis. Crit Care. 18(211)2014.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Pelosi P, Gama de Abreu M and Rocco PR:
New and conventional strategies for lung recruitment in acute
respiratory distress syndrome. Crit Care. 14(210)2010.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Severgnini P, Selmo G, Lanza C, Chiesa A,
Frigerio A, Bacuzzi A, Dionigi G, Novario R, Gregoretti C, de Abreu
MG, et al: Protective mechanical ventilation during general
anesthesia for open abdominal surgery improves postoperative
pulmonary function. Anesthesiology. 118:1307–1321. 2013.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Serpa Neto A, Cardoso SO, Manetta JA,
Pereira VG, Espósito DC, Pasqualucci Mde O, Damasceno MC and
Schultz MJ: Association between use of lung-protective ventilation
with lower tidal volumes and clinical outcomes among patients
without acute respiratory distress syndrome: A meta-analysis. JAMA.
308:1651–1659. 2012.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Lee JH, Bae JI, Jang YE, Kim EH, Kim HS
and Kim JT: Lung protective ventilation during pulmonary resection
in children: A prospective, single-centre, randomised controlled
trial. Br J Anaesth. 122:692–701. 2019.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Kokulu S, Günay E, Baki ED, Ulasli SS,
Yilmazer M, Koca B, Arıöz DT, Ela Y and Sivaci RG: Impact of a
lung-protective ventilatory strategy on systemic and pulmonary
inflammatory responses during laparoscopic surgery: Is it really
helpful? Inflammation. 38:361–367. 2014.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Memtsoudis SG, Bombardieri AM, Ma Y and
Girardi FP: The effect of low versus high tidal volume ventilation
on inflammatory markers in healthy individuals undergoing posterior
spine fusion in the prone position: A randomized controlled trial.
J Clin Anesth. 24:263–269. 2012.PubMed/NCBI View Article : Google Scholar
|