Introduction
SSc is a connective tissue disease with
insufficiently known etiology, engraving of microvasculopathy and
excessive cutaneous and visceral fibrosis. Studies show that the
underlying pathogenic process is an immunological disorder from
which targeted antibodies develop against ‘self’ structures. These
autoantibodies trigger an excessive activation of the immune system
and mainly of T cells (1) followed
by inflammation at cellular level (2). SSc is part of the rare disease group,
having an increasing incidence over the past two decades.
Statistics show not only an increase in SSc incidence, but in
autoimmune diseases as a whole (3).
Initially, reversible vasospasm of digital arteries
is manifested by the appearance of Raynaud's phenomenon, followed
by a disruption in finger pulp capillary architecture. In
microangiopathy, ischemic disorders determine the appearance of
digital ulcers and pitting scars (4). The disease pathogenesis is complex,
partially known. Under the action of viruses, anti-endothelial
antibodies, cytotoxic T lymphocytes and endothelial cells are
activated early in SSc evolution and proliferation of the innermost
vessels is triggered (5). It has
been observed that microvascular endothelial dysfunction has as
substrate the appearance of anti-endothelial antibodies and,
mainly, the presence of anti-intercellular adhesion molecule
(ICAM)-1 antibodies (6). Activated
endothelial cells release proinflammatory cytokines and connective
tissue growth factors, interleukin (IL)-1, IL-4, tumor necrosis
factor (TNF)-α, IL-6 and IL-8 transforming growth factor (TGF)-β,
which induce aberrant hyperactivated fibroblasts (7-11).
Early endothelial cell involvement in SSc, leads to the destruction
of blood capillaries with reduction in microvasculature through
vascular repair and defective neoangiogenesis simultaneously with
impaired lymphatic circulation followed by exudative accumulation
and edema formation. Associations between lymphatic
microvasculature damage with digital ulcer development and
accentuation of cutaneous induration were observed, an induration
which must be differentiated from that which appears in other
disorders with sclerodermiform skin lesions, occurring in isolation
or in the context of associated autoimmune diseases (12-14).
The presence of Raynaud's phenomenon reflects the
affected vasodilation determined by the endothelial lesion, which
has as substrate apoptosis of endothelial cells most likely under
the action of anti-endothelial antibodies (15). The microvasculopathy lesions are
expressed by the appearance of digital ulcers, telangiectasia, and
at macrovascular level by kidney damage, pulmonary arterial
hypertension and erectile dysfunction (16). Vascular occlusion results in the
occurrence of ischemic-type phenomena, digital ulcers, which are
difficult to treat with conventional treatments (17,18);
they are located on the tip of the fingers and on the extension
surfaces of the joint, can become complicated with infections and
sometimes with gangrene, thus requiring amputations or
sympathectomy (19-21).
Less often, impairment of microvasculature and digital arteries can
produce critical digital ischemia (22). Cutolo et al (23) have described three capillaroscopic
models of microvasculature impairment identified with the
videocapillaroscope at the nailfold level. ‘Early’ pattern
corresponds with the presence of dilated capillaries, ‘giant
capillaries’ and hemorrhages. These changes are more pronounced in
the ‘active’ capillary pattern, and ‘late’ pattern of the advanced
SSc is characterized by alternating areas without capillaries, with
areas where the capillaries are branched - ‘bushy capillaries’.
Considering the multiple yet undetermined issues of
this disease, we evaluated digital ulcers and Raynaud's phenomenon
as an expression of peripheral vasculopathy, as well as
acroosteolysis and microstomia, in order to establish correlations
between vascular impairment and subsequent fibrosis. We noted
personal observations on this group of patients and established
correlations between the identified clinical aspects. These
correlations may be the basis for elucidating the etiopathogenesis
of SSc, incompletely known. Previously, SSc benefitted only from
symptomatic treatment with vasodilators, antifibrotic and
immunosuppressive drugs, all with a modest therapeutic response and
with often unpredictable evolution. Other interesting observations
should be focused on relating to the microbioma changes on or
around the lesional skin in scleroderma as in other diseases and
also the possible adverse reactions that might have occurred after
some topical or internal tratments of the comorbidities (24-34).
Having the above in mind, numerous studies would be useful to
clarify various aspects of the disease.
Patients and methods
An observational study was conducted on a group of
22 patients diagnosed with SSc with the help of the 2013 American
College of Rheumatology (ACR)/European League Against Rheumatism
(EULAR) criteria. For this study, the agreement was obtained from
the Research Ethics Committee of the Faculty of Medicine in Iasi,
as well as from the Ethics Council of the University Clinic in
Bucharest. The patients were admitted between February and July
2019 to the internal medicine and rheumatology wards of a
university clinic in Bucharest. The data was obtained from the
clinical examination of the patients after they signed the informed
consent and from the capillaroscopic examination of the nailfold.
Acrosteolysis was evaluated clinically and radiologically and the
oral opening was measured to quantify the degree of microstomia.
With originality note, we used microstomia as an early indicator of
skin fibrosis of the face observed before the appearance of
tegumental induration in the hands and other segments evaluated by
Rodnan score. The clinical and paraclinical data were observed and
correlated to establish causality between vasculopathy and
fibrosis. The data obtained was entered into an Excel file and
analyzed statistically using Microsoft Excel, SPSS version 24.0,
and the results are reported in the tables and graphs.
Results
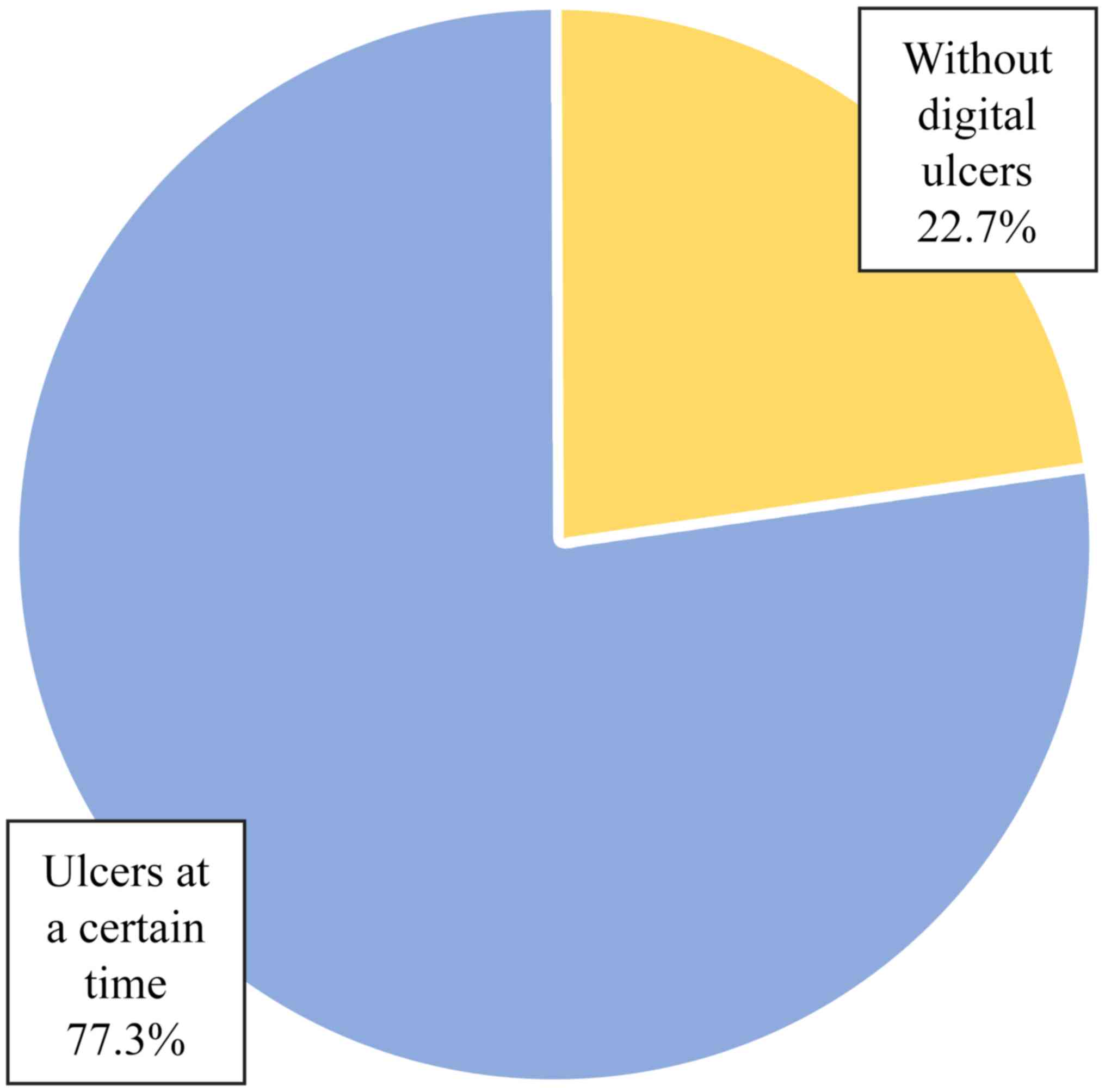
Of the 22 patients, only 17 patients (77.3%) had
ulcers at one moment in time (Table
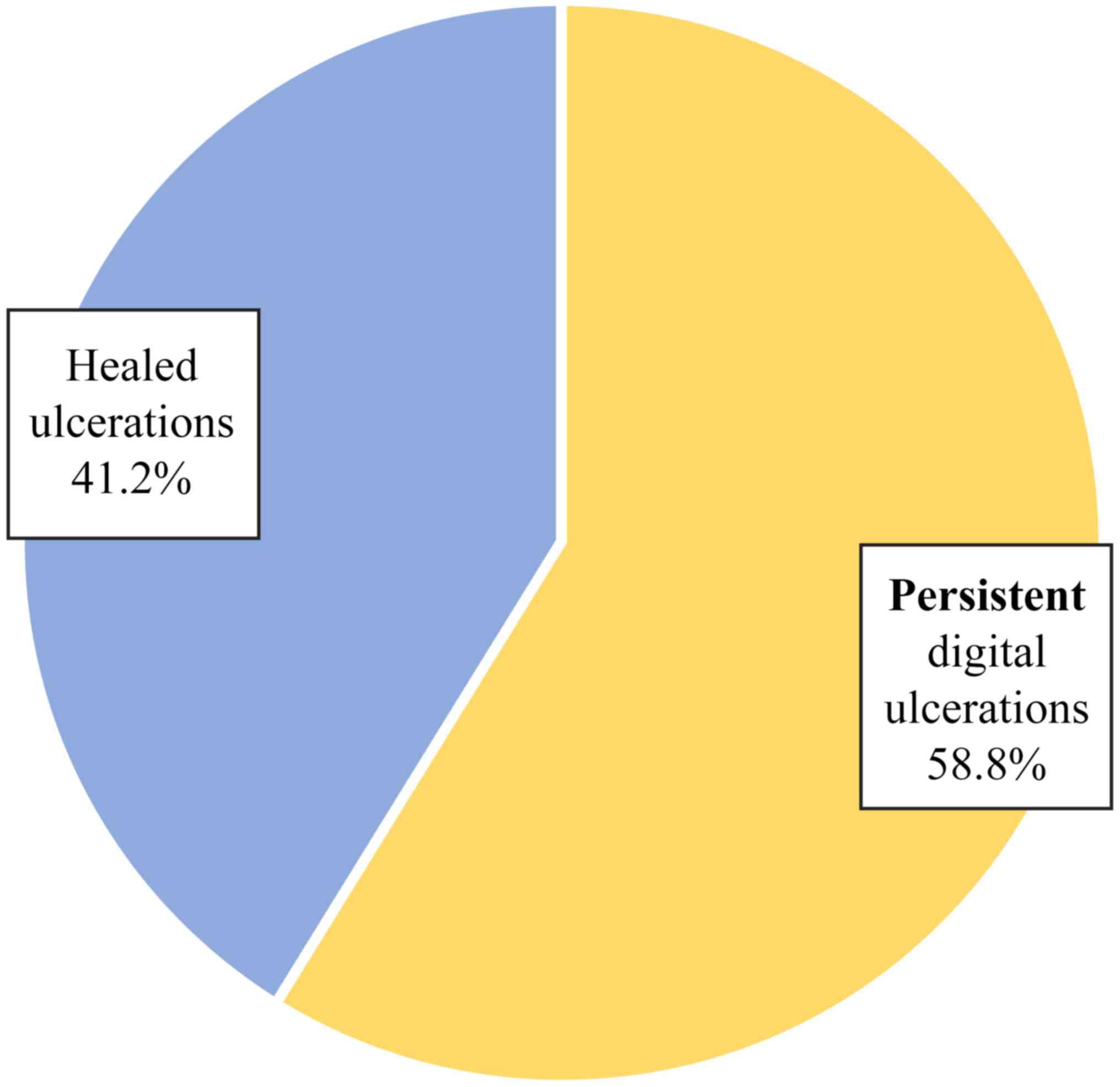
I and Fig. 1). Of the 17
patients who presented with ulcers at one moment in time, 10
patients (58.8%) had persistent digital ulcers despite the correct
treatment and 7 patients (41.2%) had a favorable ulcer evolution -
healing and lack of recurrence (Table
II and Fig. 2). The
heterogeneous evolution of the disease was observed, a fact which
is sometimes difficult to predict.
 | Table IStatus of digital ulcers - frequency
distribution. |
Table I
Status of digital ulcers - frequency
distribution.
| Groups | Absolute
frequency | Percentage
frequency |
|---|
| Valid |
|
Without
digital ulcers | 5 | 22.7 |
|
Ulcers at a
certain time | 17 | 77.3 |
| Total | 22 | 100.0 |
| Table IIDynamics of digital ulcers - frequency
distribution. |
Table II
Dynamics of digital ulcers - frequency
distribution.
| Groups | Absolute
frequency | Percentage
frequency |
|---|
| Valid |
|
Persistent
digital ulcers | 10 | 58.8 |
|
Healed
ulcers | 7 | 41.2 |
| Total | 17 | 100.0 |
Of the 10 patients who had digital ulcers without
healing, only 2 reached gangrene level without requiring
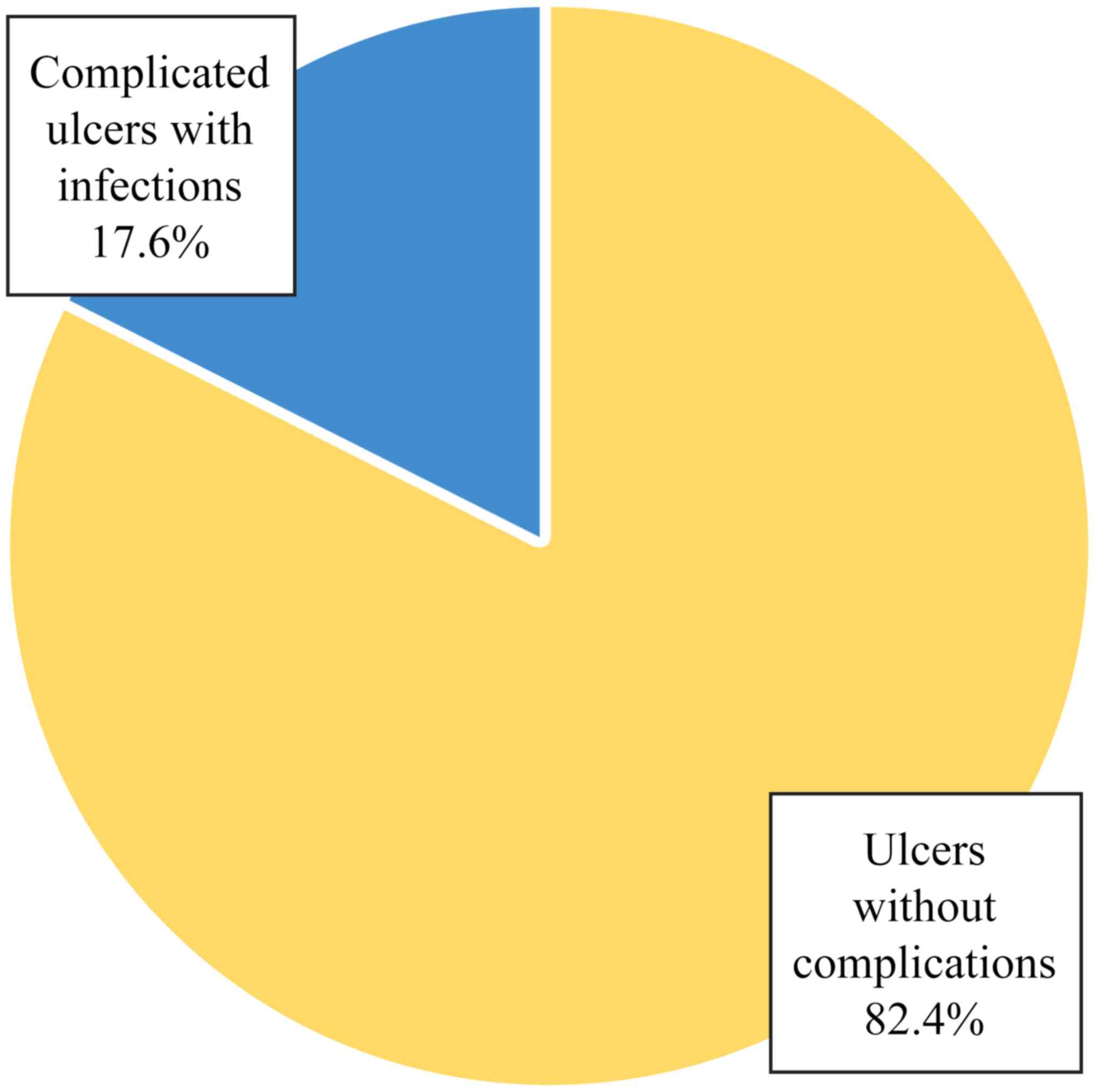
amputation. Of the total 17 patients who presented with ulcers at
one moment in time, 3 cases (17.6%) were complicated with
infections with Staphylococcus aureus identified through
cultures from infected ulcers (Table
III and Fig. 3). Of the 3
patients with infected digital ulcers, 2 patients had persistent
ulcers after the resolution of the infectious process and only one
patient had ulcers which were completely healed.
| Table IIIEvolution of digital ulcers -
frequency distribution. |
Table III
Evolution of digital ulcers -
frequency distribution.
| Groups | Absolute
frequency | Percentage
frequency |
|---|
| Valid |
|
Complicated
ulcers with infections | 3 | 17.6 |
|
Ulcers
without complications | 14 | 82.4 |
| Total | 17 | 100.0 |
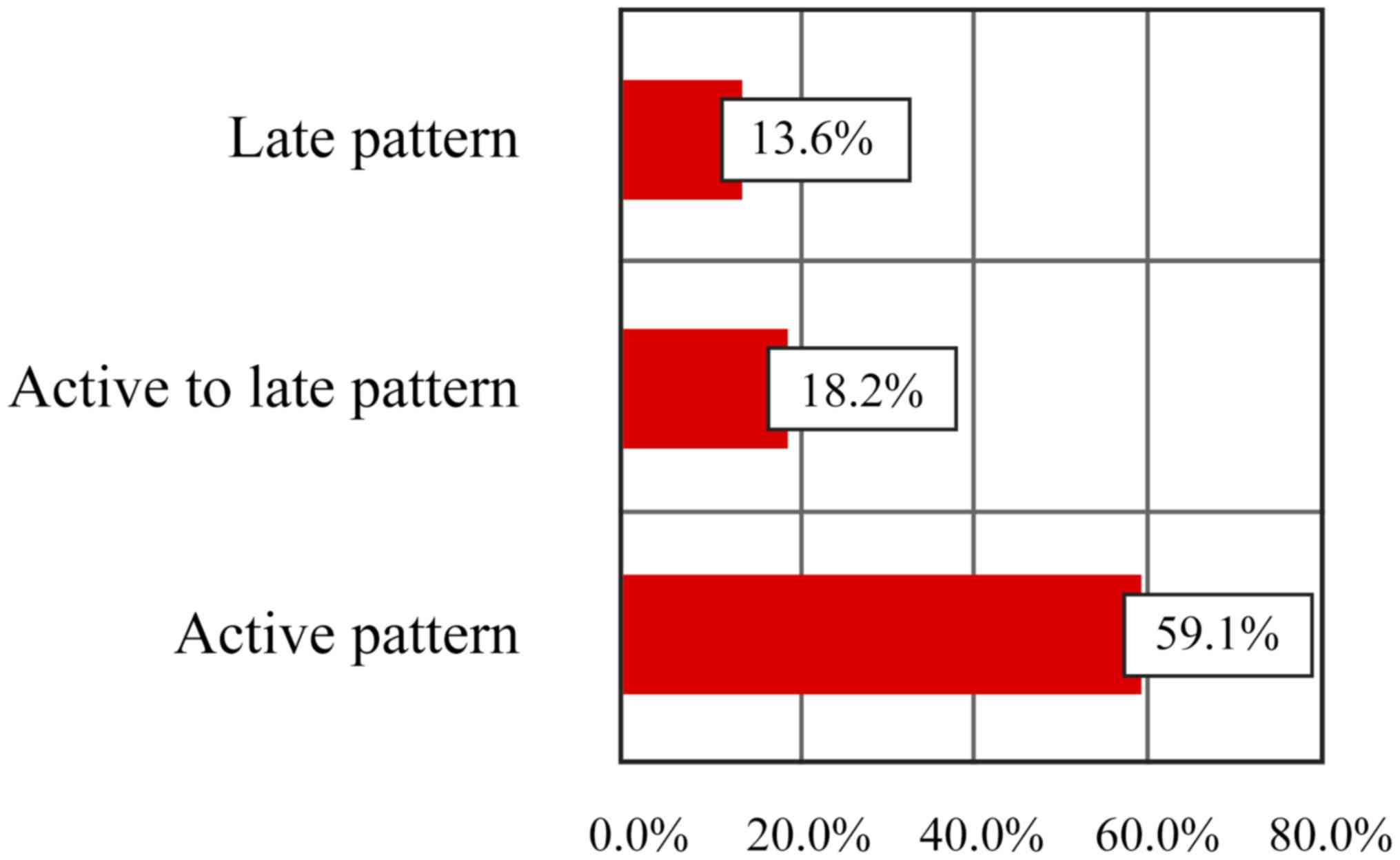
The model of impairment of blood capillaries in the
fingers was studied using capillaroscopy (Table IV and Fig. 4) in order to establish a correlation
with the status of digital ulcerations. Most patients had an active
pattern on capillaroscopic examination (59.1%) or active to late
(18.2%) and only 3 patients (13.6%) were registered with a late
pattern. Furthermore, 2 patients (9.1%) with non-specific ScS
pattern were identified.
| Table IVPattern of blood capillary damage -
frequency distributions. |
Table IV
Pattern of blood capillary damage -
frequency distributions.
| | 0 - absent | 1 - present | Total |
|---|
| Groups | n | % | n | % | n | % |
| Capillary active
pattern | 9 | 40.9 | 13 | 59.1 | 22 | 100.0 |
| Active pattern to
late | 18 | 81.8 | 4 | 18.2 | 22 | 100.0 |
| Late pattern | 19 | 86.4 | 3 | 13.6 | 22 | 100.0 |
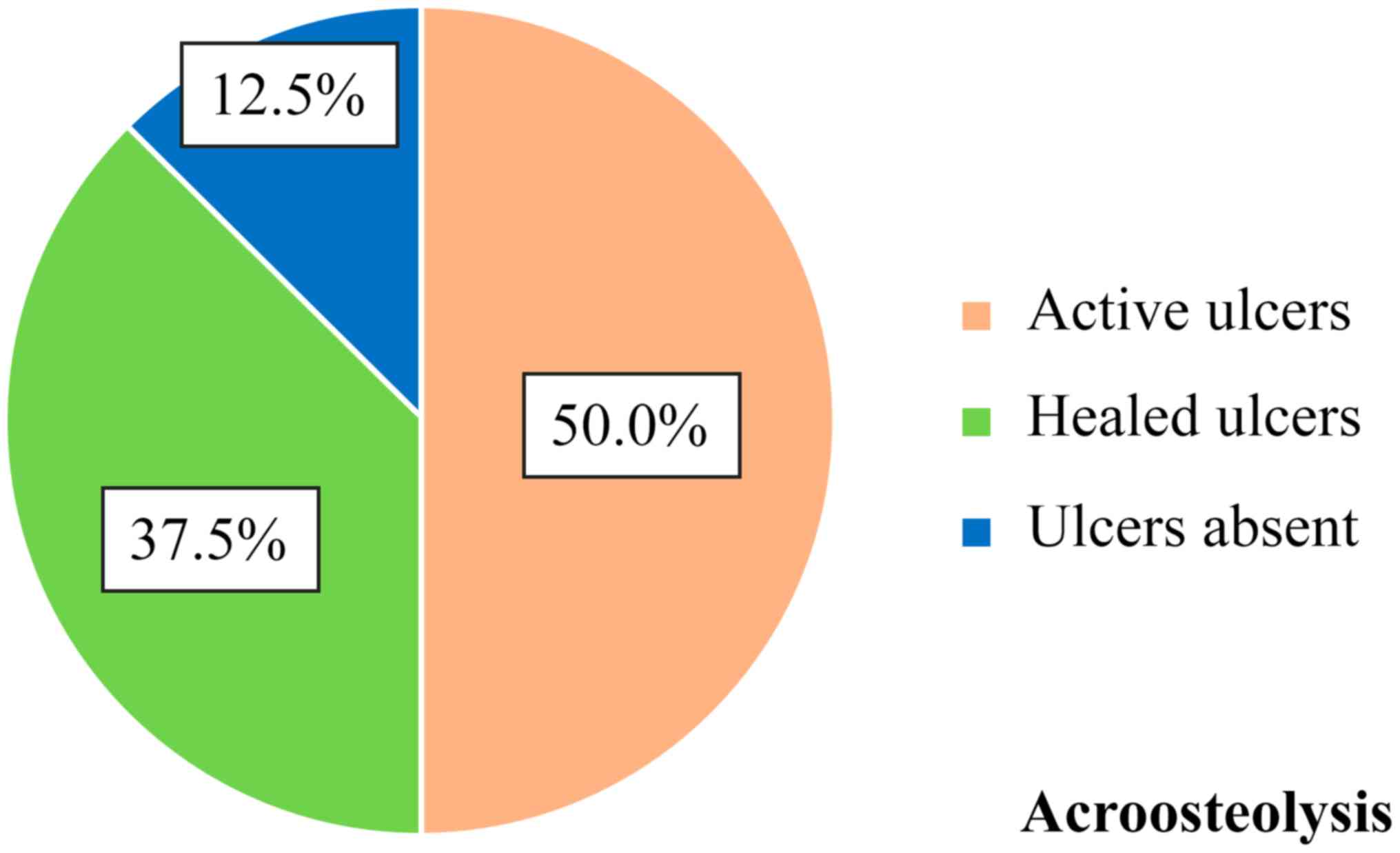
By correlating the presence of acroosteolysis and
digital ulcers (Fig. 5), it was
found that of the 8 patients with acroosteolysis, 4 patients
(50.0%) had ulcers that remained active without healing, 3 patients
(37.5%) had ulcers that healed in time and 1 patient (12.5%) had
never suffered from digital ulcers. No correlation between the
presence of digital ulcers and shortening of the distal phalanx
seemed to exist.
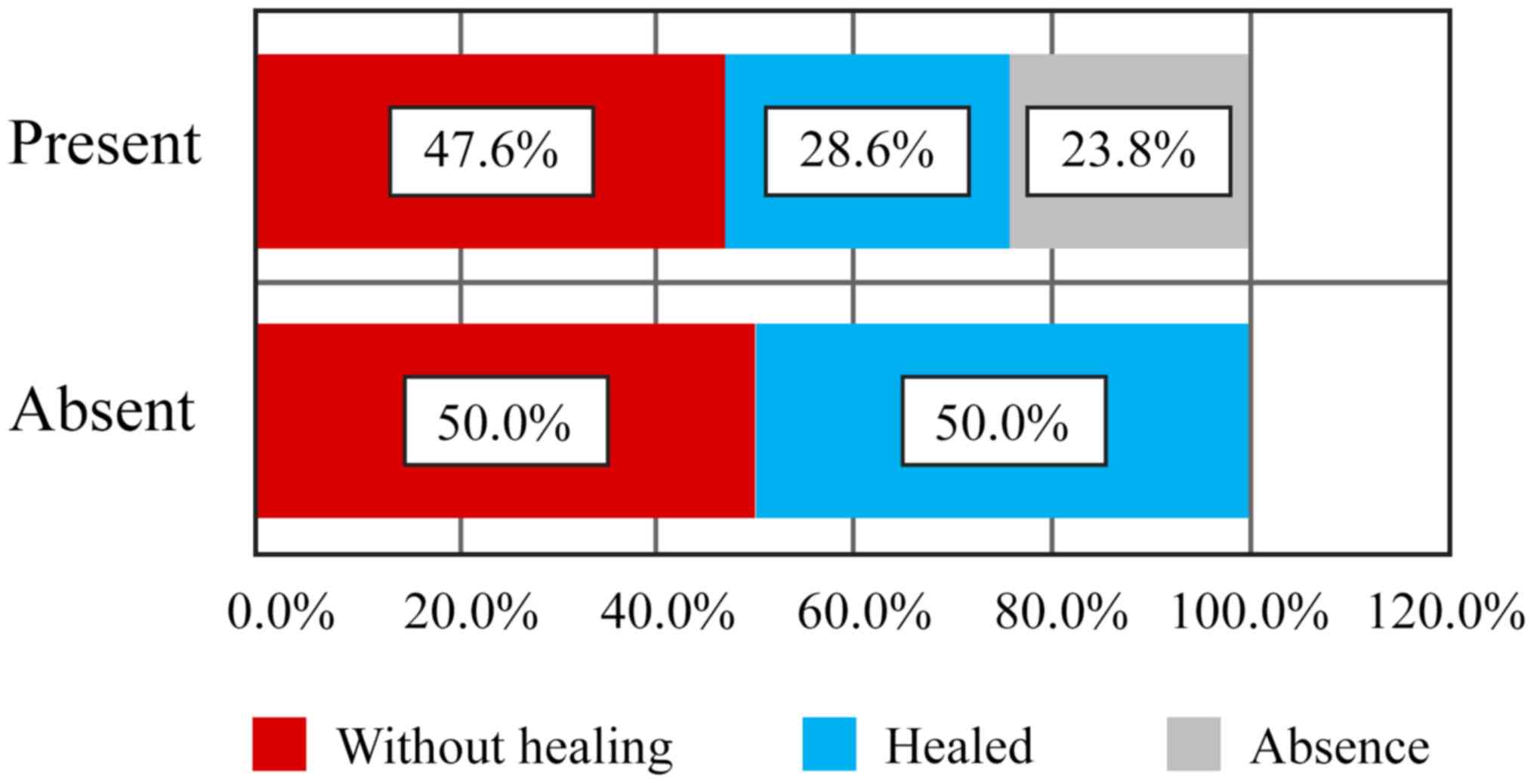
Referring to the correlation between absence or
presence of microstomia as an indicator of cutaneous fibrosis in
association with digital ulcers, we observed that of the 2 patients
who did not present with microstomia, 1 patient (50.0%) had
persistent ulcers without healing with gangrenous transformation,
and 1 patient (50.0%) had ulcers that healed in the course of the
disease. Among those with microstomia, 9 patients (45.0%) suffered
from non-healing ulcers, of which 1 reached gangrene; 6 patients
(30.0%) had healing ulcers and 5 patients (25.0%) never suffered
from ulcers (Table V and Fig. 6). Thus, presence of microstomia as an
indicator of cutaneous fibrosis, known to be subsequent to vascular
impairment, does not correlate with status and evolution of digital
ulcers, which represent a clue for peripheral microvasculopathy
(Pearson χ2=739, P=0.691).
| Table VCorrelation of microstomia with
digital ulcers. |
Table V
Correlation of microstomia with
digital ulcers.
| | Ulcers | |
|---|
| | Without
healing | Healed | Absent | Total |
|---|
| Microstomia | n | % | n | % | n | % | n | % |
|---|
| Absence | 1 | 50.0 | 1 | 50.0 | | | 2 | 100.0 |
| Present | 9 | 45.0 | 6 | 30.0 | 5 | 25.0 | 20 | 100.0 |
| Total | 10 | 45.5 | 7 | 31.8 | 5 | 22.7 | 22 | 100.0 |
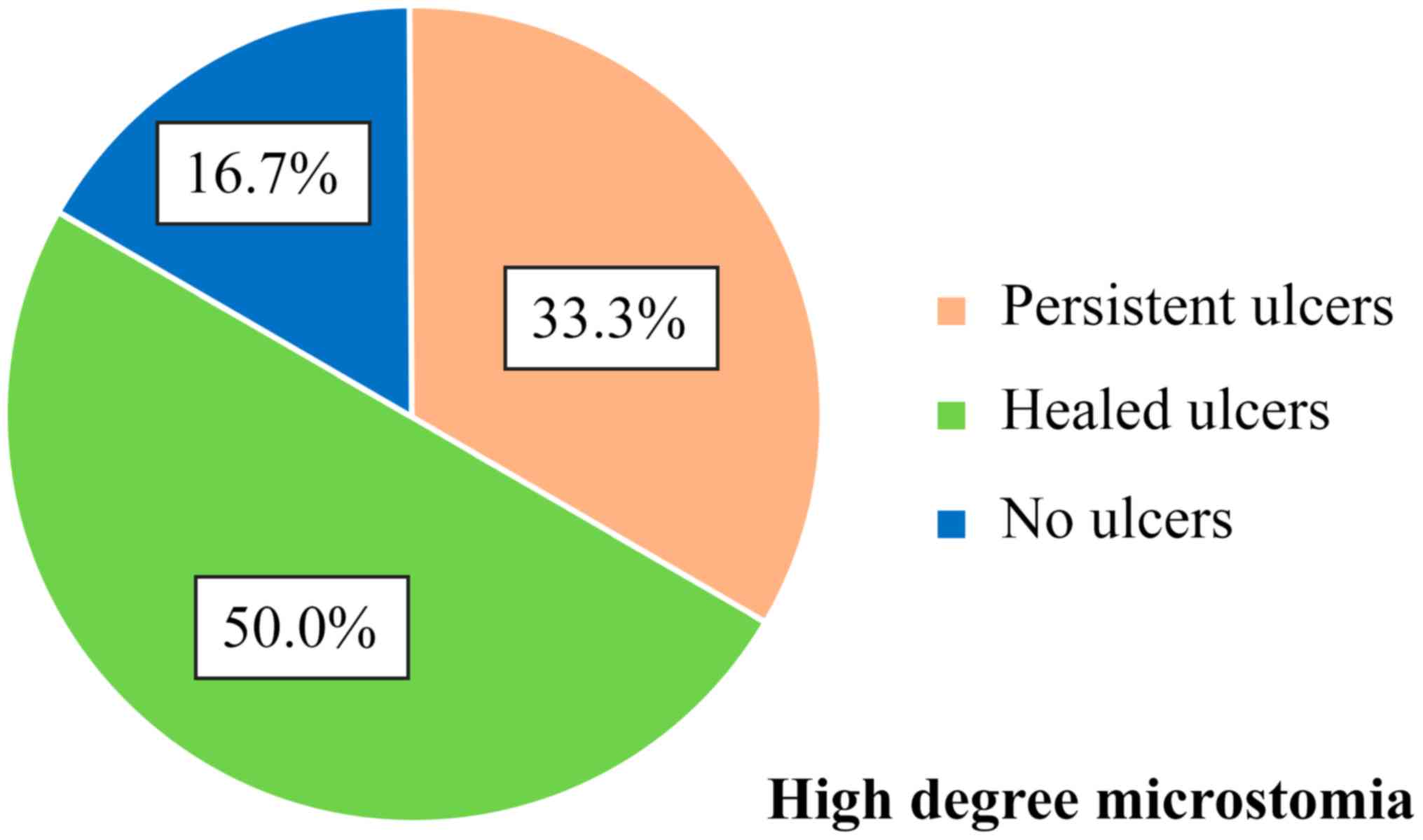
Of the 6 patients with high degree microstomia (4 cm
oral opening), 2 patients (33.3%) presented with persistent ulcers
during the disease course, 3 patients (50.0%) had healed ulcers and
1 patient (16.7%) never presented with ulcers (Fig. 7). No correlation between the
important limitation of oral opening and the status of digital
ulcers was made.
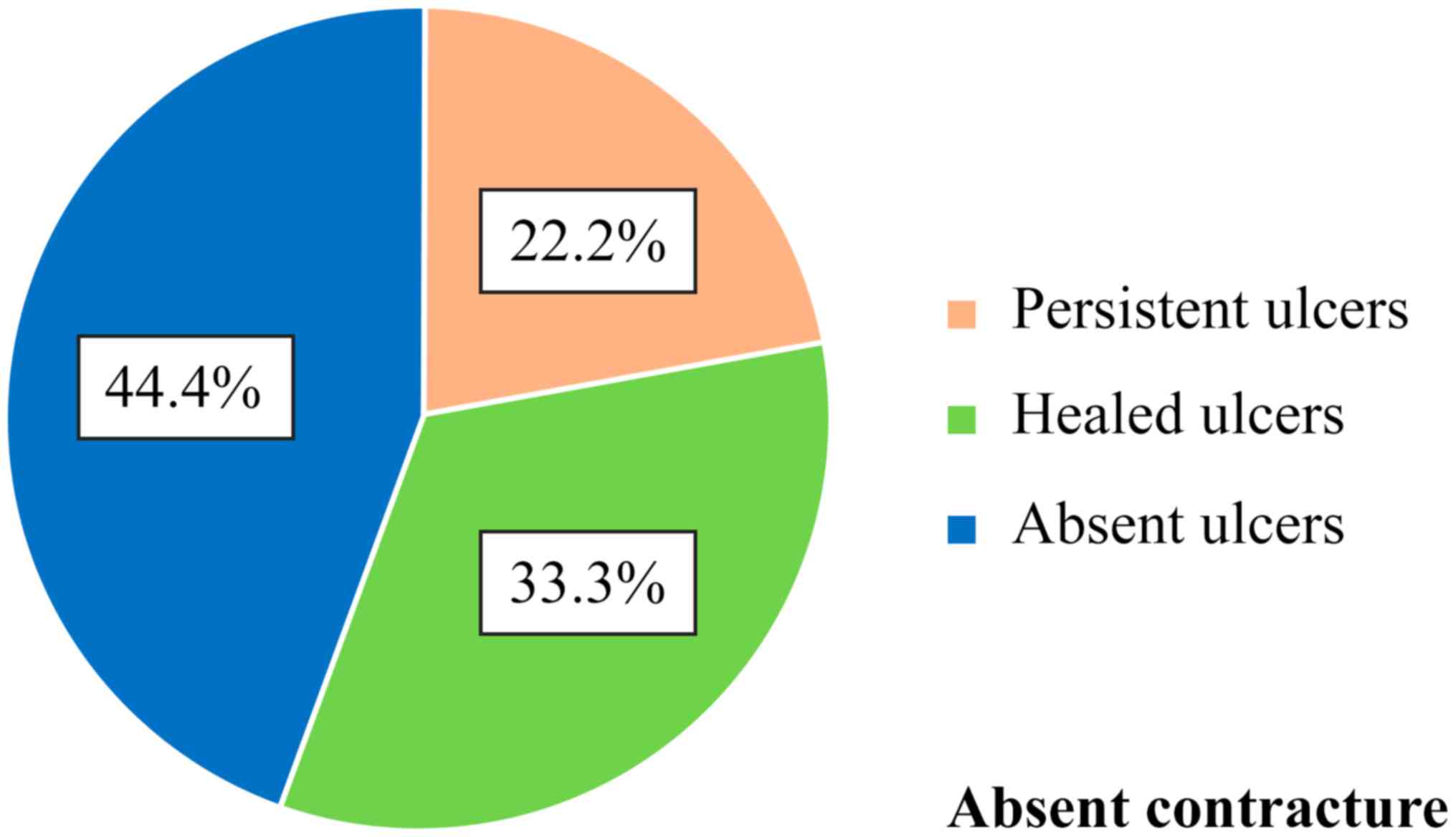
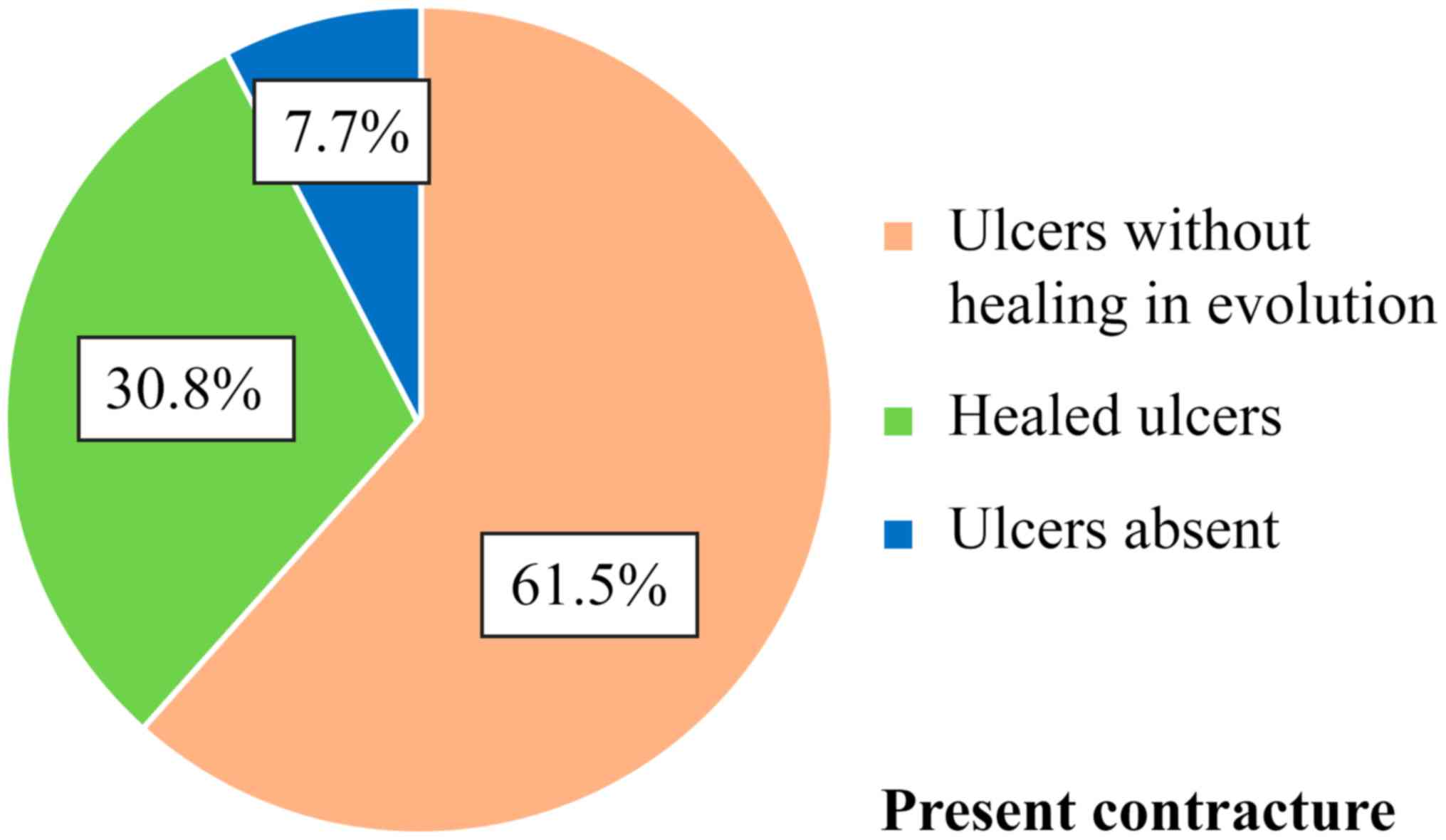
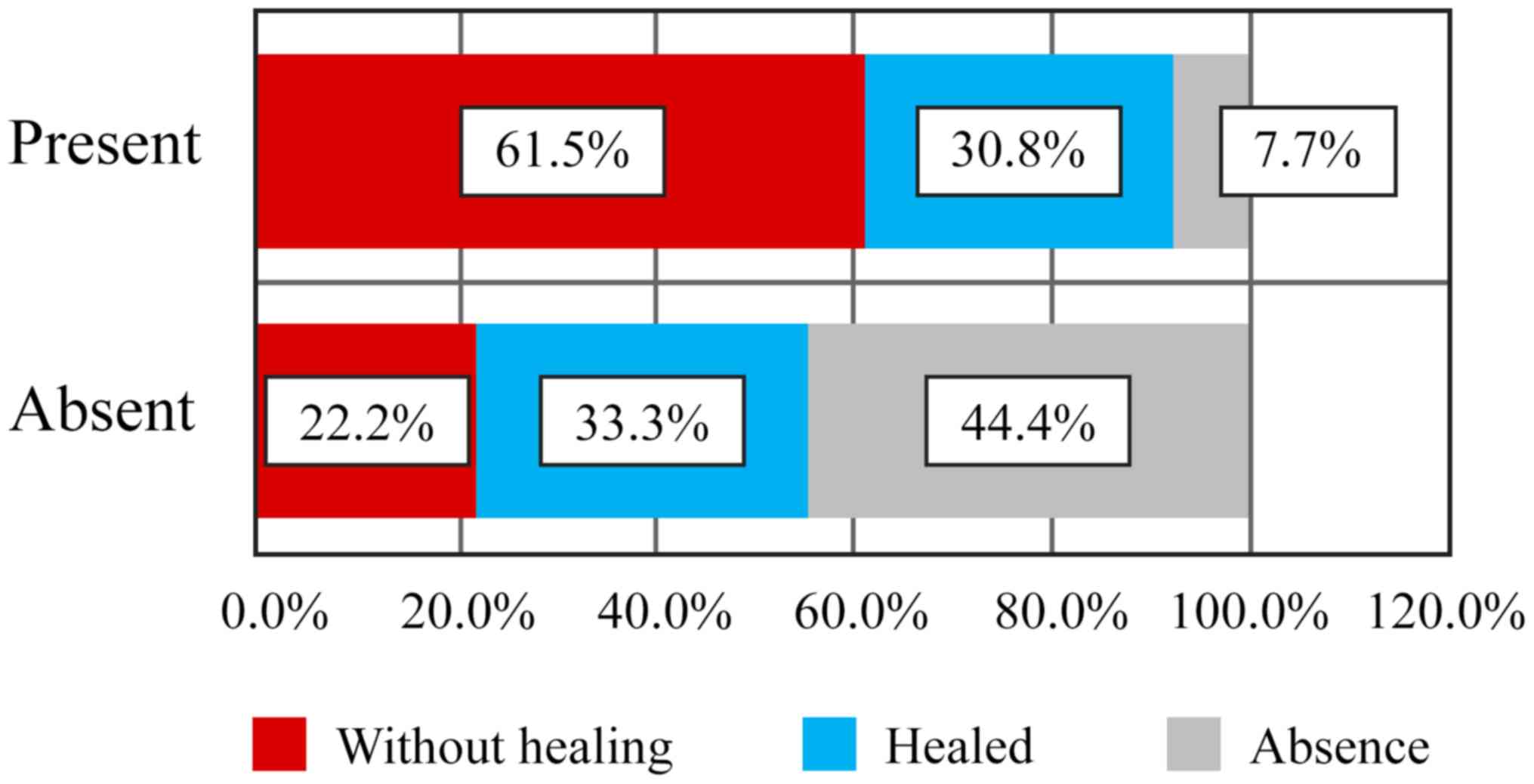
Of the 9 patients who did not have finger
contracture in the hands, and such, no limitations in finger
flexion and extension, 2 patients (22.2%) presented with persistent
ulcers, 3 patients (33.3%) had healed ulcers during the disease
course and 4 patients (44.4%) never had ulcers (Table VI and Fig. 8). Moreover, there was no correlation
between the contracture of the fingers and the status of digital
ulcers. Of the 13 patients who had contracted fingers, 8 patients
(61.5%) had persistent active ulcers, 4 patients (30.8%) had
healing ulcers and 1 patient (7.7%) never had digital ulcers
(Figs. 9 and 10). Although there were clear differences,
they did not reach the statistical significance threshold (Pearson
χ2=4.98, P=0.082).
| Table VICorrelation between the presence of
digital contracture and digital ulcers. |
Table VI
Correlation between the presence of
digital contracture and digital ulcers.
| | Ulcers | |
|---|
| | Without
healing | Healed | Absent | Total |
|---|
| Contracture | n | % | n | % | n | % | n | % |
|---|
| Absence | 2 | 22.2 | 3 | 33.3 | 4 | 44.4 | 9 | 100.0 |
| Present | 8 | 61.5 | 4 | 30.8 | 1 | 7.7 | 13 | 100.0 |
| Total | 10 | 45.5 | 7 | 31.8 | 5 | 22.7 | 22 | 100.0 |
Discussion
We conducted this observational study to create an
overview of the skin condition of an SSc patient group in a
university center; the small number of patients included in the
study suggests the relatively low prevalence of this disease.
Furthermore, SSc has a low incidence and the patients studied had
different stages of disease through recruitment of both new cases
and ones with >10 years of progression. SSc is part of the rare
diseases group, although in the recent years there has been a
slight increase in incidence (3).
By analyzing the status of digital ulcers, we found
that less than a quarter of patients had never suffered from
digital ulcers, and of those with ulcers, more than half had
persistent forms despite the correct treatment (35). Other patients had a favorable outcome
with ulcer healing and no recurrence, a state most often registered
under treatment with a dual endothelin receptor antagonist. The
heterogeneous disease course is sometimes difficult to predict
(36). Regarding the number and
location of digital ulcers, the majority of patients had between 3
and 6 digital ulcers and patients with 1, 2 or >6 ulcers were
rarely identified; the most commonly affected were fingers II and
III, probably due to their more frequent use in prehension. Of the
patients who presented with digital ulcers at one time during the
disease, only 3 cases were complicated by infections with
Staphylococcus aureus and after antibiogram-guided
antibiotic therapy, only one patient had completely healed ulcers,
and the other 2 patients had persistent ulcers even after the
infectious process was resolved. One can notice the low risk of
infection of digital ulcers although they are located in an exposed
area which is not covered and is frequently used. In the context of
a disease with impaired immunity, the natural anti-infectious
defense is preserved. Among patients who suffered from persistent
digital ulcers, only one fifth had an unfavorable disease course
towards gangrene, which was treated with no need for amputation.
Most patients (with one exception) had Raynaud's phenomenon,
reflecting the presence of peripheral microangiopathy; since one
case did not present with digital ulcers. Absence of digital ulcers
was found in the patient without Raynaud's phenomenon, but not all
patients with Raynaud's phenomenon had digital ulcers. By analyzing
the capillaroscopic pattern, only half of the patients with active
pattern had persistent ulcers and only one third was associated
with acroosteolysis (this was present in those with a late
pattern). As in digital ulcers, acroosteolysis predominantly
affected fingers II and III, being more frequently involved in
prehension. I was noted that one of the patients having a
nonspecific capillaroscopic pattern did not show Raynaud's
phenomenon and never suffered from digital ulcers, probably due to
an early disease stage. Studying the presence of microstomia and
that of finger contracture in flexion as indicators of fibrosis,
and the dynamics of digital ulcers as an indicator of digital
microvasculopathy, no correlation between them was found although
the causality between vascular and fibrosis is well known. However,
the presence of a small degree of microstomia was observed as an
early and more faithful indicator for skin fibrosis, which appeared
earlier than the skin induration of the hands. In the early stages
of the disease, before the appearance of tegumentary induration,
Rodnan score being 0, the presence of a small degree of microstomia
already suggests the installation of cutaneous fibrosis based on
our observations.
In conclusion, for now SSc remains an incurable
disease with an etiology and pathogenesis that are not known in
their entirety, with an invalidating course and an unfavorable
psychological impact which diminishes the patient's quality of
life; these reasons are a statement for the imperative need for
future studies and observations on all aspects of the disease which
might be useful for optimal management (1,37,38).
Acknowledgements
Not applicable
Funding
No funding was received.
Availability of data and materials
The analyzed data sets generated during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
CB, ALT, MC and LS conceived and designed the study,
provided the study materials or patient data and were responsible
for the collection and assembly of the data, data analysis and
interpretation, were involved in drafting and editing the
manuscript. All the authors made an equal contribution to the
article. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
For this study, the agreement was obtained from the
Research Ethics Committee of the Faculty of Medicine in Iasi, as
well as from the Ethics Council of the University Clinic in
Bucharest. All patients provided informed consent and approved the
publication of data.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chihara M, Kurita M, Yoshihara Y, Asahina
A and Yanaba K: Clinical significance of serum galectin-9 and
soluble CD155 levels in patients with systemic sclerosis. J Immunol
Res. 2018(9473243)2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Cottin V and Brown KK: Interstitial lung
disease associated with systemic sclerosis (SSc-ILD). Respir Res.
20(13)2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Butt SA, Jeppesen JL, Fuchs C, Mogensen M,
Engelhart M, Torp-Pedersen C, Gislason GH, Jacobsen S and Andersson
C: Trends in incidence, mortality, and causes of death associated
with systemic sclerosis in Denmark between 1995 and 2015: A
nationwide cohort study. BMC Rheumatol. 2(36)2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Friedrich S, Lüders S, Glimm AM, Werner
SG, Schmittat G, Burmester GR, Backhaus M, Riemekasten G and
Ohrndorf S: Association between baseline clinical and imaging
findings and the development of digital ulcers in patients with
systemic sclerosis. Arthritis Res Ther. 21(96)2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
McFarlane IM, Bhamra MS, Kreps A, Iqbal S,
Al-Ani F, Saladini-Aponte C, Grant C, Singh S, Awwal K, Koci K, et
al: Gastrointestinal manifestations of systemic sclerosis.
Rheumatology (Sunnyvale). 8(235)2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Altorok N, Wang Y and Kahaleh B:
Endothelial dysfunction in systemic sclerosis. Curr Opin Rheumatol.
26:615–620. 2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Liakouli V, Elies J, El-Sherbiny YM,
Scarcia M, Grant G, Abignano G, Derrett-Smith EC, Esteves F,
Cipriani P, Emery P, et al: Scleroderma fibroblasts suppress
angiogenesis via TGF-β/caveolin-1 dependent secretion of pigment
epithelium-derived factor. Ann Rheum Dis. 77:431–440.
2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Grigore O, Mihailescu AI, Solomon I, Boda
D and Caruntu C: Role of stress in modulation of skin neurogenic
inflammation. Exp Ther Med. 17:997–1003. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ilie MA, Caruntu C, Lixandru D, Tampa M,
Georgescu SR, Constantin MM, Constantin C, Neagu M, Zurac SA and
Boda D: In vivo confocal laser scanning microscopy imaging
of skin inflammation: Clinical applications and research
directions. Exp Ther Med. 17:1004–1011. 2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Ilie MA, Caruntu C, Tampa M, Georgescu SR,
Matei C, Negrei C, Ion RM, Constantin C, Neagu M and Boda D:
Capsaicin: Physicochemical properties, cutaneous reactions and
potential applications in painful and inflammatory conditions. Exp
Ther Med. 18:916–925. 2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ghiţă MA, Căruntu C, Rosca AE, Căruntu A,
Moraru L, Constantin C, Neagu M and Boda D: Real-time investigation
of skin blood flow changes induced by topical capsaicin. Acta
Dermatovenerol Croat. 25:223–227. 2017.PubMed/NCBI
|
|
12
|
Manetti M, Pratesi S, Romano E, Rosa I,
Bruni C, Bellando-Randone S, Guiducci S, Maggi E, Ibba-Manneschi L
and Matucci-Cerinic M: Decreased circulating lymphatic endothelial
progenitor cells in digital ulcer-complicated systemic sclerosis.
Ann Rheum Dis. 78:575–577. 2019.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Tatu AL and Nwabudike LC: The treatment
options of male genital lichen sclerosus et atrophicus: Treatments
of genital lichen sclerosus. In: 14th National Congress of
Urogynecology (Urogyn), Eforie, Romania, 262-264, 2017.
|
|
14
|
Tatu AL and Ionescu MA: Multiple
autoimmune syndrome type III-thyroiditis, vitiligo and alopecia
areata. Acta Endocrinol (Bucharest). 13:124–125. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kahaleh MB: Raynaud phenomenon and the
vascular disease in scleroderma. Curr Opin Rheumatol. 16:718–722.
2004.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Denton CP: Advances in pathogenesis and
treatment of systemic sclerosis. Clin Med (Lond). 15 (Suppl
6):s58–s63. 2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Codullo V, Distler O and Montecucco C:
Pathophysiology of systemic sclerosis. In: Novel Insights into
Systemic Sclerosis Management. Publisher Future Medicine Ltd.,
London, pp22-35, 2013.
|
|
18
|
Nwabudike LC and Tatu AL: Magistral
prescription with silver nitrate and Peru Balsam in difficult to
heal diabetic foot ulcers. Am J Ther. 25:e679–e680. 2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Guillevin L, Hunsche E, Denton CP, Krieg
T, Schwierin B, Rosenberg D and Matucci-Cerinic M: DUO Registry
Group. Functional impairment of systemic scleroderma patients with
digital ulcerations: Results from the DUO Registry. Clin Exp
Rheumatol. 31 (Suppl 76):71–80. 2013.PubMed/NCBI
|
|
20
|
Gheorghe I, Tatu AL, Lupu I, Thamer O,
Cotar AI, Pircalabioru GG, Popa M, Cristea VC, Lazar V and
Chifiriuc MC: Molecular characterization of virulence and
resistance features in Staphylococcus aureus clinical
strains isolated from cutaneous lesions in patients with drug
adverse reactions. Rom Biotechnol Lett. 22:12321–12327. 2017.
|
|
21
|
Ilie MA, Caruntu C, Lupu M, Lixandru D,
Tampa M, Georgescu SR, Bastian A, Constantin C, Neagu M, Zurac SA,
et al: Current and future applications of confocal laser scanning
microscopy imaging in skin oncology. Oncol Lett. 17:4102–4111.
2019.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Herrick A and Muir L: Raynaud's phenomenon
(secondary). BMJ Clin Evid: pii: 1125, 2014.
|
|
23
|
Cutolo M, Sulli A, Pizzorni C and Accardo
S: Nailfold videocapillaroscopy assessment of microvascular damage
in systemic sclerosis. J Rheumatol. 27:155–160. 2000.PubMed/NCBI
|
|
24
|
Tatu AL and Cristea VC: Pityriasis
folliculorum of the back thoracic area: Pityrosporum, keratin
plugs, or demodex involved? J Cutan Med Surg.
21(441)2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Nwabudike LC and Tatu AL: Response to -
Chronic exposure to tetracyclines and subsequent diagnosis for
non-melanoma skin cancer in a large Mid-Western US population. J
Eur Acad Dermatol Venereol. 32(e 159)2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Tatu AL and Cristea VC: Unilateral
blepharitis with fine follicular scaling. J Cutan Med Surg.
21(442)2017.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Tatu AL and Nwabudike LC: Reply to: Kubiak
K et al: Endosymbiosis and its significance in dermatology.
J Eur Acad Dermatol Venereol. 32:e346–e347. 2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Tatu AL, Clatici VG and Nwabudike LC:
Rosacea-like demodicosis (but not primary demodicosis) and
papulopustular rosacea may be two phenotypes of the same disease -
a microbioma, therapeutic and diagnostic tools perspective. J Eur
Acad Dermatol Venereol. 33:e46–e47. 2019.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Tatu AL, Ionescu MA and Nwabudike LC:
Contact allergy to topical mometasone furoate confirmed by
rechallenge and patch test. Am J Ther. 25:e497–e498.
2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Tatu AL, Ciobotaru OR, Miulescu M, Buzia
OD, Elisei AM, Mardare N, Diaconu C, Robu S and Nwabudike LC:
Hydrochlorothiazide: Chemical structure, therapeutic, phototoxic
and carcinogenetic effects in dermatology. Rev Chim (Bucharest).
69:2110–2114. 2018.
|
|
31
|
Nwabudike LC, Elisei AM, Buzia OD,
Miulescu M and Tatu AL: Statins. A review on structural
perspectives, adverse reactions and relations with non-melanoma
skin cancer. Rev Chim (Bucharest). 69:2557–2562. 2018.
|
|
32
|
Tatu AL, Elisei AM, Chioncel V, Miulescu M
and Nwabudike LC: Immunologic adverse reactions of β-blockers and
the skin (Review). Exp Ther Med. 18:955–959. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Nwabudike LC, Miulescu M and Tatu AL: Case
series of an alternative therapy for generalised lichen planus:
Four case studies. Exp Ther Med. 18:943–948. 2019.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Ciobotaru OR, Lupu MN, Rebegea L,
Ciobotaru OC, Duca OM, Tatu AL, Voinescu CD, Stoleriu G, Earar K
and Miulescu M: Dexamethasone - chemical structure and mechanisms
of action in prophylaxis of postoperative side effects. Rev Chim
Buchar. 70:843–847. 2019.
|
|
35
|
Kanno Y, Shu E, Kanoh H and Seishima M:
The antifibrotic effect of α2AP neutralization in systemic
sclerosis dermal fibroblasts and mouse models of systemic
sclerosis. J Invest. 136:762–769. 2016.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Vikse J, Gøransson LG and Norheim KB:
Systemic capillary leak syndrome following bosentan treatment in a
patient with systemic sclerosis. Scand J Rheumatol. 48:426–427.
2019.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Bobeică C, Crăescu M, Ancuța CI, Coman M
and Nechita A: Experimental models for the study of systemic
scleroderma In: Annals of the University ‘Dunarea de Jos’ of
Galati, Fascicle XVII. Galati University Press. 71–84. 2018.
|
|
38
|
Bobeică C, Vâță D, Stătescu L, Țăranu T,
Popescu IA, Grăjdeanu AI and Gheucă-Solovăstru L: The quality of
life for a patient with an autoimmune disease. Bull Integr
Psychiatry. XXV:27–36. 2019.
|