Introduction
Hepatocyte growth factor (HGF) was originally
discovered as a mitogen of hepatocytes in adult rats and exhibits a
cytotoxic effect in certain tumor cells, such as those in hematoma
(1-2). HGF is a
paracrine factor that is secreted by mesenchymal cells, such as
fibroblasts, bronchial epithelial cells, alveolar macrophages and
neutrophils, and plays an important role in lung development,
inflammation and tissue repair (3-5).
The biological effect of HGF is mediated by the cell membrane
receptor MET (6). HGF synthesis is
regulated by prostaglandins, cytokines and hormones, while its
cellular secretion is stimulated by acute phase proteins, such as
tumor necrosis factor-α (TNF-α), interleukin (IL)-1α, IL-1β, IL-6,
platelet derived growth factor and fibroblast growth factor β, as
well as cyclic adenosine monophosphate (7-10).
HGF can be detected in edema fluid during acute lung injury, where
it is produced locally by fibroblasts and inflammatory cells
(11-14).
HGF is therefore used to assess progression of Legionella pneumonia
(15), solitary pulmonary nodules
(16) and bacterial pneumonia
(17).
Mycoplasma pneumoniae pneumonia (MP), which
is unresponsive to commonly used antibiotics such as penicillin, is
caused by a microorganism associated with atypical pneumonia
(18). Mycoplasma pneumoniae
infections vary dramatically in clinical presentation, ranging from
mild and self-limiting upper respiratory symptoms to
radiographically confirmed pneumonia that requires hospitalization
(19). In some cases, Mycoplasma
pneumoniae infection may result in severe clinical consequences
that involve organs other than lungs, such as encephalitis and
acute hepatitis, which is known as extrapulmonary complications
(20, 21). As the Mycoplasma pneumoniae
incubation period can last as long as 3 weeks, and prolonged
shedding follows infection, outbreaks often go unnoticed and the
course of infection can extend for long periods of time (22). The clinical detection of
Mycoplasma pneumoniae relies on serological IgM testing or
PCR assay; culture is rarely used because the microorganism grows
very slowly (23, 24). Macrolides are the treatment of choice
for MP, while tetracyclines and fluoroquinolones also prove to be
effective (25).
Pneumonia treatment is particularly important in
children, as it remains the most common cause of mortality and
morbidity in children <5 years of age globally (26). Although preventable, pneumonia can
lead to chronic lung conditions, such as pulmonary fibrosis, if it
is recurrent or untreated (27). A
study among a Finnish population reported that MP was detected in
30% of pediatric community-acquired pneumonia patients and in
>50% children aged 5 years or older (28).
In the present study, serum HGF levels were assessed
in MP as well as in bacterial pneumonia.
Materials and methods
Patient enrollment
Children (n=137; age range, 3-14 years; mean age,
6.7±3.5) who visited the Pediatric Department of Tianjin Nankai
Hospital between January 2014 and June 2015 were enrolled in the
study, including 65 cases of MP, 42 cases of bacterial pneumonia
and 30 healthy children who visited the department for health
examinations. This study was approved by The Ethics Committee of
Tianjin Nankai Hospital (approval no. 2017-018P), which waived
written consent, because the study was observational and residual
blood after completing the routine follow-up was used. Oral consent
for participation in the study was obtained from each patient and
their parent.
Diagnosis of MP and bacterial
pneumonia
The inclusion criteria were a combination of: i)
Fever; ii) cough; iii) breathing crackles; iv) lung consolidation,
and v) serum IgM against Mycoplasma pneumoniae ≥1:160 at the
first day of admission or an increase in IgG against Mycoplasma
pneumoniae at least 4 times by the 7th day following admission
(29). Patients were also not
responsive to penicillin, cephalosporins or sulfonamide.
Severe MP (n=27) was defined as in the guidelines of
community-acquired pneumonia management in children in China
(30). It was diagnosed if a patient
met at least two of criteria i-iii or either of criteria iv and v.
The criteria were: i) Obvious tachycardia or tachypnea (respiratory
rate ≥40 breaths per minute or heart rate ≥140 beats per minutes in
children aged 1-5 years; respiratory rate ≥30 breaths per minute or
heart rate ≥120 beats per minutes in children aged over 5 years);
ii) unresponsive to β-Lactam antibiotics; iii) lung consolidation
that involved more than one lobe of the lung confirmed by chest
x-ray; iv) complicated with pleural effusion or pulmonary
necrosis/abscess, and v) partial pressure of oxygen less than 60
mmHg (7.98Ka) or involvement of other organs.
Cases of bacterial pneumonia were diagnosed by blood
culture and culture of the expectorated sputa with no
contamination, as indicated by scanty squamous epithelium but
dominant with columnar epithelium (31).
Exclusion criteria
The exclusion criteria were any of the following: i)
Patients were infected by another pathogen within 7 days of
hospital stay; ii) patients were in the recovery stage of pneumonia
since their admission, as shown by stable body temperature and
resolved chest x-ray; iii) patients with a past history of
bronchial asthma or recurrent pulmonary infection; iv) primary or
secondary immune-compromised patients; v) patients with complicated
renal, pulmonary, liver, cardiovascular or connective tissue
diseases, and vi) patients with incomplete medical history.
Determination of HGF, WBC, LDH,
alanine aminotransferase (ALT), aspartate aminotransferase (AST)
and CRP levels
Serum levels of HGF in each sample were determined
by ELISA (cat. no. E01H0208; Blue Gene) according to the
manufacturer's instructions while WBC, LDH, ALT, AST and CRP levels
were assessed using ADVIA 2400 Clinical Chemistry System (Siemens
Healthineers). HGF and CRP lebels were examined on the day of
admission and at 2 days after admission.
Azithromycin administration
All patients who suffered from MP were administered
azithromycin (10 mg/kg/day) intravenously on the day of admission
for 2 days. Readings were then taken on the third day to confirm
whether patients have responded to treatment. Patients were
evaluated and further divided into two groups according to the
effectiveness of azithromycin. Treatment was determined to be
effective if systemic symptoms such as fever, myalgia and headache
were resolved and respiratory symptoms improved. This was based on
the recommendations of the guidelines of community-acquired
pneumonia management in children in China (30).
Statistical analysis
All statistical analyses were performed using SPSS
v17.0 (SPSS, Inc.). Continuous variables are presented as the mean
± standard deviation (SD) or median values with interquartile range
(IQR). Normally distributed parameters between multiple groups were
tested using one-way ANOVA followed by Tukey's multiple comparison
test. Normally distributed parameters between two groups were
examined with unpaired t-tests. The Mann-Whitney U test was used to
compare serum CRP levels, which were not normally distributed.
Discrete variables between multiple groups were analyzed using the
χ2 test. Receiver operating characteristic (ROC) curve
analysis was used to analyze the discriminative power of laboratory
markers to predict the efficacy of macrolides in MP. P<0.05 was
considered to indicate a statistically significant difference.
Results
There were no significant differences between age
and sex of the subjects in the control, bacterial pneumonia and MP
groups. Additionally, there were no significant differences between
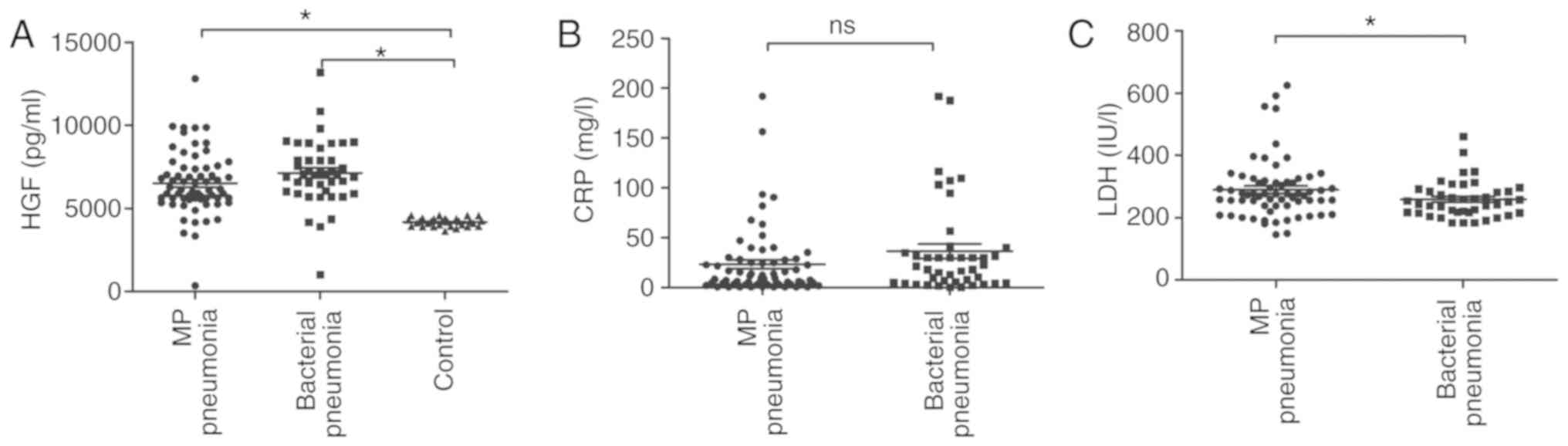
ALT and AST levels among the three groups (Table I). CRP levels significantly differed
among bacterial pneumonia, MP pneumonia and control subjects
(P<0.001; Table I). As indicated
in Fig. 1A, serum HGF levels were
significantly higher in the MP and bacterial pneumonia groups
compared to levels in control subjects on the day of admission
before treatment (P<0.05). HGF levels did not vary significantly
between MP and bacterial pneumonia (Fig.
1A). Similarly, CRP levels did not vary significantly between
MP and bacterial pneumonia (Fig.
1B), while LDH levels are significantly higher in MP pneumonia
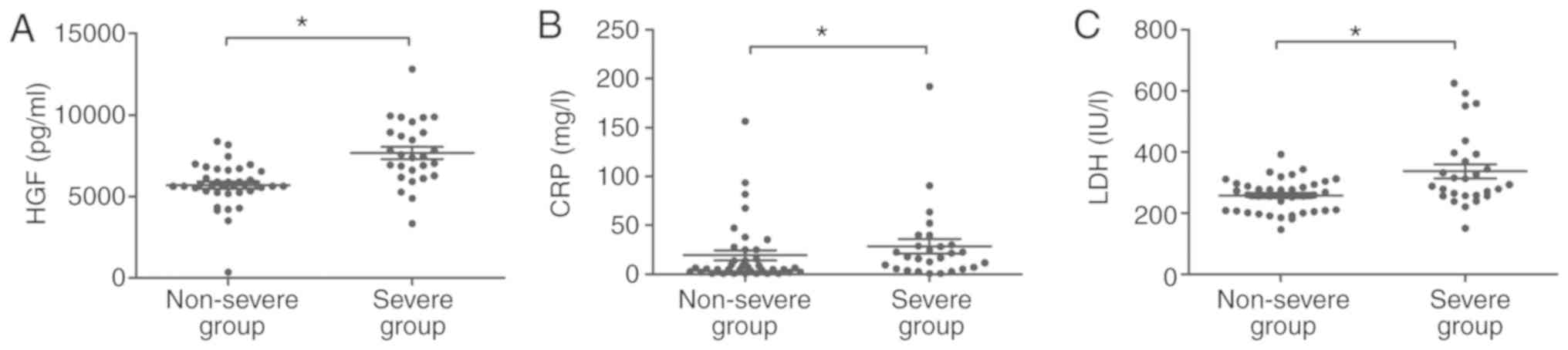
compared with bacterial pneumonia (P<0.05; Fig. 1C). Patients who suffered from MP were
divided into severe MP (n=27) and non-severe MP (n=38), according
to the guidelines of community-acquired pneumonia management in
children in China (30). HGF was
significantly higher in severe MP than in non-severe MP on the day
of admission (P<0.05; Fig. 2A).
In addition, CRP was significantly higher in severe MP [17.8
(5.5-30.1) mg/l] than in non-severe MP [5.9 (2.4-25.0) mg/l;
Table II; Fig. 2B] as was LDH (337.0±120.3 vs.
256.9±54.4 IU/l; Table II; Fig. 2C). There were no obvious differences
in sex, WBC count and liver function (as indicated by ALT and AST)
between severe cases and non-severe cases. However, the average age
of severe MP patients was significantly older than that of
non-severe patients (Table II).
 | Table IClinical characteristics of patients
in all three groups. |
Table I
Clinical characteristics of patients
in all three groups.
| | Patient group | |
|---|
| Variables | MP | Bacterial
pneumonia | Healthy
control | P-value |
|---|
| No. of cases | 65 | 42 | 30 | |
| Mean age
(years) | 7.2±3.2 | 5.8±3.7 | 6.9±3.4 | 0.089 |
| Sex
(male/female) | 36/29 | 18/24 | 14/16 | 0.406 |
| WBC count
(x/µl) |
8,585.2±3,985.9 |
9,992.4±4,819.2 |
6,283.3±1,394.8 | 0.001 |
| LDH (IU/l) | 290.2±95.7 | 259.0±59.1 | 130.1±29.5 | <0.001 |
| ALT (IU/l) | 18.5±6.7 | 18.1±6.5 | 20.3±5.6 | 0.349 |
| AST (IU/l) | 28.0±9.3 | 30.1±8.1 | 27.2±5.2 | 0.275 |
| CRP (mg/l) | 9.5 (3.6-28.0) | 20.1
(5.2-36.3) | <0.8 | <0.001 |
| Table IIComparison of clinical
characteristics of patients with differing severities of MP. |
Table II
Comparison of clinical
characteristics of patients with differing severities of MP.
| | MP severity | |
|---|
| Variables | Non-severe | Severe | P-value |
|---|
| No. of cases | 38 | 27 | |
| Mean age
(years) | 6.3±3.1 | 8.5±3.1 | 0.004 |
| Sex
(male/female) | 19/19 | 17/10 | 0.324 |
| WBC count
(x/µl) |
9,028.2±4,258.9 |
7,961.9±3,550.1 | 0.291 |
| LDH (IU/l) | 256.9±54.4 | 337.0±120.3 | 0.003 |
| ALT (IU/l) | 17.5±4.1 | 19.9±9.2 | 0.201 |
| AST (IU/l) | 27.8±9.0 | 28.4±9.8 | 0.768 |
| CRP (mg/l) | 5.9 (2.4-25.0) | 17.8
(5.5-30.1) | 0.038 |
In those 42 patients who responded to 2 days of
azithromycin treatment, serum HGF levels dropped significantly
(P<0.05; Fig. 3A) as did CRP
levels (P<0.05; Fig. 3B). In
addition, LDH was also significantly reduced (P<0.05; Fig. 3C). There was no evident change in
HGF, CRP or LDH (P>0.05) in the 23 patients who were not
responsive to azithromycin treatment (Fig. 3).
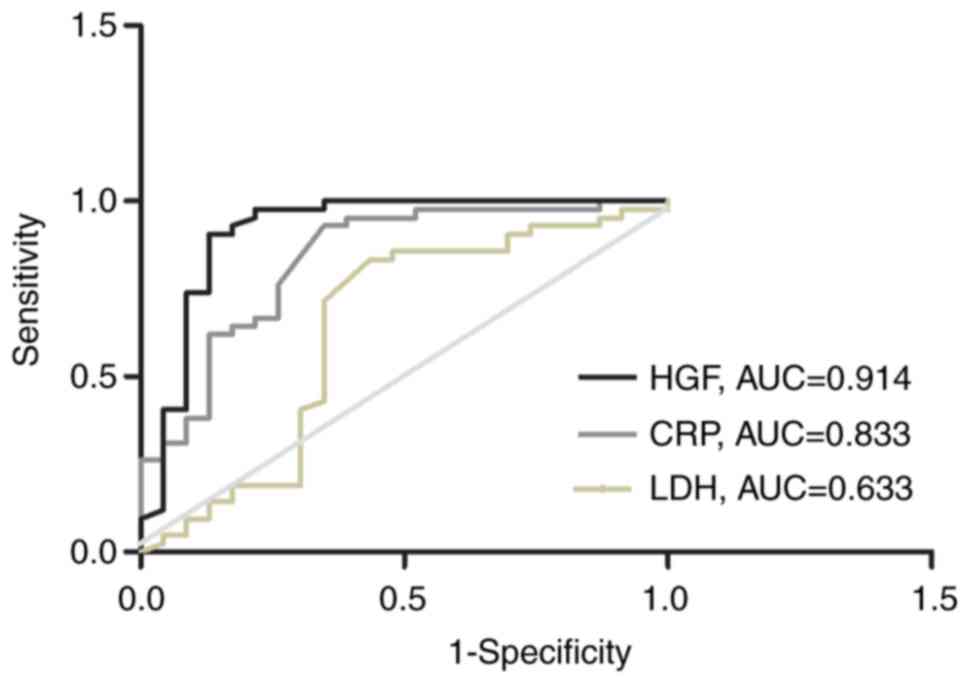
Finally, the sensitivity and specificity of CRP, LDH
and HGF in assessing effectiveness of azithromycin treatment were
compared. As indicated in Fig. 4,
HGF showed advantage over CRP and LDH in evaluating azithromycin
treatment with higher sensitivity or specificity (P<0.05). The
sensitivity (97.6%) and specificity (78.3%) levels of HGF were both
higher than those of CRP (91.2% sensitivity; 69.1% for specificity)
and LDH (85.1% sensitivity; 70.2% specificity), respectively
(Table III).
| Table IIIA comparison of sensitivity and
specificity of LDH, CRP and HGF. |
Table III
A comparison of sensitivity and
specificity of LDH, CRP and HGF.
| Parameter | Sensitivity
(%) | Specificity
(%) | 95% CI |
|---|
| HGF | 97.6 | 78.3 | 0.817-1.000 |
| CRP | 91.2 | 69.1 | 0.725-0.942 |
| LDH | 85.1 | 70.2 | 0.473-0.792 |
Discussion
HGF is known to be elevated in Legionella pneumonia
(15) and bacterial pneumonia
(17), which led to the hypothesis
that it may be elevated in MP. When children are infected with
Mycoplasma pneumoniae IL-2, IL-6 and TNF-α are released into
the peripheral blood (32), which
can stimulate secretion of HGF (10). HGF is also known to be secreted at
high levels in viral pneumonia and HGF/MET signaling enhances the
innate immune response, by stimulating the secretion of IL-8 and
granulocyte macrophage colony-stimulating factor (33). Additionally, both HGF and CRP levels
correlated with the severity of MP, as shown in the present study.
HGF has been used to assess the severity of avian origin influenza
A (H7N9) virus and worked as an independent outcome predictor
(34). Therefore, HGF has been
suggested to act as a general indicator of activity of the innate
immune response, rather than as a specific marker for MP. However,
this does not impede its application in assessing MP.
Interestingly, the present study showed that LDH was also
upregulated in severe MP. In the present study LDH was used as a
biomarker to predict refractory MP, which is characterized by
prolonged fever and hospital stay as well as more severe pulmonary
symptoms in children (35) as an
alternative to erythrocyte sedimentation rate and CRP (36). LDH may be an indicator of severity of
MP. In the present study, the mean age of severe MP patients was
higher than non-severe ones, which may be due to the more mature
immune system in older children causing longer duration of fever,
higher CRP, and more severe pulmonary lesions compared to younger
patients.
Determining the severity of pneumonia is not always
straightforward. The World Health Organization criteria divide the
severity of pneumonia into 2 grades: Severe pneumonia and very
severe pneumonia (37). Although
there is an association between these classifications and clinical
outcome (38,39), it is still a relatively coarse
classification system and does not consider population variation
due to geography. As all subjects in the present study were Chinese
children, Chinese national guidance was applied to divide pediatric
pneumonia into severe and non-severe cases (30). Identifying severe cases of MP is
important, because the use of steroids is advocated alongside
antibiotics for such cases (30).
Macrolides have been shown to be effective in severe cases of
Mycoplasma pneumoniae infection (25). The results of the present study
suggest that HGF levels could be assessed to determine whether
children with MP require early steroid treatment.
β-lactam antibiotics, including penicillin and
cephalosporins, are considered to be the drugs of choice for
treating respiratory diseases, as they are active against most
respiratory bacterial pathogens (40). However, they are ineffective against
Mycoplasma pneumoniae because they target the cell wall,
while Mycoplasma pneumoniae lacks a cell wall (41). Macrolides and tetracyclines, which
act as protein synthesis inhibitors, and fluoroquinolones, which
act against topoisomerases to inhibit DNA synthesis and
replication, are usually highly effective against Mycoplasma
pneumoniae and are the drugs of choice (25). However, only macrolides are
recommended for children, as tetracycline and fluoroquinolone
administration can lead to a number of age-related adverse events,
such as cardiotoxicity and inhibition of bone growth (42,43).
Thus, in the present study azithromycin, a macrolide, was used to
treat pediatric patients. However, approximately one third (23/65)
of patients did not respond to this treatment. Since the first
report of macrolide resistance in 2001, it has increased rapidly,
with the highest prevalence in East Asia (44,45). The
mechanism underlying macrolide resistance is related to point
mutations in domain V of the 23S ribosomal RNA gene of
Mycoplasma pneumoniae and can usually be detected with the
onset of the disease (46). CRP is
the only factor demonstrated to significantly predict the efficacy
of macrolides in MP patients (47).
The results of the present study suggest that HGF may also be
useful to assess the efficacy of azithromycin administration to MP
patients. HGF has previously been used to evaluate the
effectiveness of treatment in patients with acute brucellosis and
acute myocardial infarction (48,49).
Though this suggests that HGF is a general indicator for
inflammation or the immune response the results of the present
study indicated that HRP had a higher sensitivity and specificity
than CRP in assessing efficacy of azithromycin treatment of MP.
Acknowledgements
Not applicable.
Funding
The present study was funded by a grant from The
Municipal Bureau of Health project (grant no. 2014KZ049).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
LQL administered the medication, assessed clinical
parameters and performed statistical analysis. ZHW collected
patient samples, assessed clinical parameters and performed
statistical analysis. HYY designed the study and drafted the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Local Ethics
Committee of Tianjin Nankai Hospital (approval no. 2017-018P),
which waived written consent, as the study was observational and
residual blood after completing the routine follow-up was used.
Oral consent from each patient and their parent was obtained.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Nakamura T, Nawa K and Ichihara A: Partial
purification and characterization of hepatocyte growth factor from
serum of hepatectomized rats. Biochem Biophys Res Commun.
122:1450–1459. 1984.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Tajima H, Matsumoto K and Nakamura T:
Hepatocyte growth factor has potent anti-proliferative activity in
various tumor cell lines. FEBS Lett. 291:229–232. 1991.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Panganiban RA and Day RM: Hepatocyte
growth factor in lung repair and pulmonary fibrosis. Acta Pharmacol
Sin. 32:12–20. 2011.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Ware LB and Matthay MA: Keratinocyte and
hepatocyte growth factors in the lung: Roles in lung development,
inflammation, and repair. Am J Physiol Lung Cell Mol Physiol.
282:L924–L940. 2002.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Morimoto K, Amano H, Sonoda F, Baba M,
Senba M, Yoshimine H, Yamamoto H, Ii T, Oishi K and Nagatake T:
Alveolar macrophages that phagocytose apoptotic neutrophils produce
hepatocyte growth factor during bacterial pneumonia in mice. Am J
Respir Cell Mol Biol. 24:608–615. 2001.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Nagahori T, Dohi M, Matsumoto K, Saitoh K,
Honda ZI, Nakamura T and Yamamoto K: Interferon-γ upregulates the
c-Met/hepatocyte growth factor receptor expression in alveolar
epithelial cells. Am J Respir Cell Mol Biol. 21:490–497.
1999.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Matsumoto K, Okazaki H and Nakamura T:
Novel function of prostaglandins as inducers of gene expression of
HGF and putative mediators of tissue regeneration. J Biochem.
117:458–464. 1995.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Zarnegar R: Regulation of HGF and HGFR
gene expression. EXS. 74:33–49. 1995.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Matsuo R, Ohkohchi N, Murata S, Ikeda O,
Nakano Y, Watanabe M, Hisakura K, Myronovych A, Kubota T, Narimatsu
H, et al: Platelets Strongly Induce Hepatocyte Proliferation with
IGF-1 and HGF In Vitro. J Surg Res. 145:279–286. 2008.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Marchand-Adam S, Fabre A, Mailleux AA,
Marchal J, Quesnel C, Kataoka H, Aubier M, Dehoux M, Soler P and
Crestani B: Defect of pro-hepatocyte growth factor activation by
fibroblasts in idiopathic pulmonary fibrosis. Am J Respir Crit Care
Med. 174:58–66. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Grenier A, Chollet-Martin S, Crestani B,
Delarche C, El Benna J, Boutten A, Andrieu V, Durand G,
Gougerot-Pocidalo MA, Aubier M, et al: Presence of a mobilizable
intracellular pool of hepatocyte growth factor in human
polymorphonuclear neutrophils. Blood. 99:2997–3004. 2002.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Verghese GM, McCormick-Shannon K, Mason RJ
and Matthay MA: Hepatocyte growth factor and keratinocyte growth
factor in the pulmonary edema fluid of patients with acute lung
injury. Biologic and clinical significance. Am J Respir Crit Care
Med. 158:386–394. 1998.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Yanagita K, Matsumoto K, Sekiguchi K,
Ishibashi H, Niho Y and Nakamura T: Hepatocyte growth factor may
act as a pulmotrophic factor on lung regeneration after acute lung
injury. J Biol Chem. 268:21212–21217. 1993.PubMed/NCBI
|
|
14
|
Yanagita K, Nagaike M, Ishibashi H, Niho
Y, Matsumoto K and Nakamura T: Lung may have an endocrine function
producing hepatocyte growth factor in response to injury of distal
organs. Biochem Biophys Res Commun. 182:802–809. 1992.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Higa F, Akamine M, Furugen M, Hibiya K,
Koide M, Tamayose M, Tamaki Y, Haranaga S, Arakaki N, Yara S, et
al: Hepatocyte growth factor levels in Legionella pneumonia: A
retrospective study. BMC Infect Dis. 11(74)2011.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Yu H, Wang Y, Yu Q, Zhang H, Ma W, Shang S
and Wang D: Significance of plasma hepatocyte growth factor in
diagnosis of benign and malignant solitary pulmonary nodules. Int J
Clin Exp Pathol. 8:2063–2067. 2015.PubMed/NCBI
|
|
17
|
Abednazari H, Xu J, Millinger E, Brudin L,
Forsberg P and Nayeri F: Hepatocyte growth factor is a better
indicator of therapeutic response than C-reactive protein within
the first day of treatment in pneumonia. Chemotherapy. 52:260–263.
2006.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Atkinson TP, Balish MF and Waites KB:
Epidemiology, clinical manifestations, pathogenesis and laboratory
detection of Mycoplasma pneumoniae infections. FEMS Microbiol Rev.
32:956–973. 2008.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Bajantri B, Venkatram S and Diaz-Fuentes
G: Mycoplasma pneumoniae: A potentially severe infection. J Clin
Med Res. 10:535–544. 2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Decaux G, Szyper M, Ectors M, Cornil A and
Franken L: Central nervous system complications of Mycoplasma
pneumoniae. J Neurol Neurosurg Psychiatry. 43:883–887.
1980.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Squadrini F, Lami G, Pellegrino F, Pinelli
G, Bavieri M, Fontana A and Bisetti A: Acute hepatitis complicating
Mycoplasma pneumoniae infection. J Infect. 16:201–202.
1988.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Gdalevich M, Haas EJ, Dukhan L, Katz M,
Zelenski V and Moran-Gilad J: Control of a Mycoplasma pneumoniae
outbreak in an institutional setting using azithromycin
prophylaxis. Front Public Health. 5(366)2017.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Nilsson AC, Björkman P and Persson K:
Polymerase chain reaction is superior to serology for the diagnosis
of acute Mycoplasma pneumoniae infection and reveals a high rate of
persistent infection. BMC Microbiol. 8(93)2008.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Zhang L, Zong ZY, Liu YB, Ye H and Lv XJ:
PCR versus serology for diagnosing Mycoplasma pneumoniae infection:
A systematic review & meta-analysis. Indian J Med Res.
134:270–280. 2011.PubMed/NCBI
|
|
25
|
Lee H, Yun KW, Lee HJ and Choi EH:
Antimicrobial therapy of macrolide-resistant Mycoplasma pneumoniae
pneumonia in children. Expert Rev Anti Infect Ther. 16:23–34.
2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Bénet T, Picot VS, Awasthi S, Pandey N,
Bavdekar A, Kawade A, Robinson A, Rakoto-Andrianarivelo M, Sylla M,
Diallo S, et al: For The Gabriel Network: Severity of Pneumonia in
Under 5-Year-Old Children from Developing Countries: A Multicenter,
Prospective, Observational Study. Am J Trop Med Hyg. 97:68–76.
2017.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Tablan OC and Reyes MP: Chronic
interstitial pulmonary fibrosis following Mycoplasma pneumoniae
pneumonia. Am J Med. 79:268–270. 1985.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Korppi M, Heiskanen-Kosma T and Kleemola
M: Incidence of community-acquired pneumonia in children caused by
Mycoplasma pneumoniae: Serological results of a prospective,
population-based study in primary health care. Respirology.
9:109–114. 2004.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Lee WJ, Huang EY, Tsai CM, Kuo KC, Huang
YC, Hsieh KS, Niu CK and Yu HR: Role of serum Mycoplasma pneumoniae
IgA, IgM, and IgG in the diagnosis of Mycoplasma pneumoniae-related
pneumonia in school-age children and adolescents. Clin Vaccine
Immunol. 24(e00471-16)2017.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Chinese Medial Association pediatric
branch respiratory group. Editor Committee of Chinese Journal of
Pediatrics: Management guidance of community acquired pneumonia.
Chinese Journal of Pediatrics 51: 745-752, 856-862, 2013.
|
|
31
|
Joyce SM: Sputum analysis and culture. Ann
Emerg Med. 15:325–328. 1986.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Kazachkov MY, Hu PC, Carson JL, Murphy PC,
Henderson FW and Noah TL: Release of cytokines by human nasal
epithelial cells and peripheral blood mononuclear cells infected
with Mycoplasma pneumoniae. Exp Biol Med (Maywood). 227:330–335.
2002.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Ito Y, Correll K, Zemans RL, Leslie CC,
Murphy RC and Mason RJ: Influenza induces IL-8 and GM-CSF secretion
by human alveolar epithelial cells through HGF/c-Met and TGF-α/EGFR
signaling. Am J Physiol Lung Cell Mol Physiol. 308:L1178–L1188.
2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Guo J, Huang F, Liu J, Chen Y, Wang W, Cao
B, Zou Z, Liu S, Pan J, Bao C, et al: The Serum Profile of
Hypercytokinemia Factors Identified in H7N9-Infected Patients can
Predict Fatal Outcomes. Sci Rep. 5(10942)2015.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Lu A, Wang C, Zhang X, Wang L and Qian L:
Lactate Dehydrogenase as a Biomarker for Prediction of Refractory
Mycoplasma pneumoniae Pneumonia in Children. Respir Care.
60:1469–1475. 2015.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Wang M, Wang Y, Yan Y, Zhu C, Huang L,
Shao X, Xu J, Zhu H, Sun X, Ji W, et al: Clinical and laboratory
profiles of refractory Mycoplasma pneumoniae pneumonia in children.
Int J Infect Dis. 29:18–23. 2014.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Scott JA, Wonodi C, Moïsi JC,
Deloria-Knoll M, DeLuca AN, Karron RA, Bhat N, Murdoch DR, Crawley
J, Levine OS, et al: Pneumonia Methods Working Group: The
definition of pneumonia, the assessment of severity, and clinical
standardization in the Pneumonia Etiology Research for Child Health
study. Clin Infect Dis. 54 (Suppl 2):S109–S116. 2012.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Pépin J, Demers AM, Mberyo-Yaah F, Jaffar
S, Blais C, Somsé P, Bobossi G and Morency P: Acute lower
respiratory infections among children hospitalized in Bangui,
Central African Republic: Toward a new case-management algorithm.
Trans R Soc Trop Med Hyg. 95:410–417. 2001.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Sehgal V, Sethi GR, Sachdev HP and
Satyanarayana L: Predictors of mortality in subjects hospitalized
with acute lower respiratory tract infections. Indian Pediatr.
34:213–219. 1997.PubMed/NCBI
|
|
40
|
Garau J: Role of beta-lactam agents in the
treatment of community-acquired pneumonia. Eur J Clin Microbiol
Infect Dis. 24:83–99. 2005.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Huong PL, Thi NT, Nguyet NT, Van TK Hang
DT, Huong VT, Anh DD and Sasaki T: First report on clinical
features of Mycoplasma pneumoniae infections in Vietnamese
children. Jpn J Infect Dis. 60:370–373. 2007.PubMed/NCBI
|
|
42
|
Guo D, Cai Y, Chai D, Liang B, Bai N and
Wang R: The cardiotoxicity of macrolides: A systematic review.
Pharmazie. 65:631–640. 2010.PubMed/NCBI
|
|
43
|
Demers P, Fraser D, Goldbloom RB, Haworth
JC, LaRochelle J, MacLean R and Murray TK: Effects of tetracyclines
on skeletal growth and dentition. A report by the Nutrition
Committee of the Canadian Paediatric Society. Can Med Assoc J.
99:849–854. 1968.PubMed/NCBI
|
|
44
|
Okazaki N, Narita M, Yamada S, Izumikawa
K, Umetsu M, Kenri T, Sasaki Y, Arakawa Y and Sasaki T:
Characteristics of macrolide-resistant Mycoplasma pneumoniae
strains isolated from patients and induced with erythromycin in
vitro. Microbiol Immunol. 45:617–620. 2001.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Liu Y, Ye X, Zhang H, Xu X, Li W, Zhu D
and Wang M: Antimicrobial susceptibility of Mycoplasma pneumoniae
isolates and molecular analysis of macrolide-resistant strains from
Shanghai, China. Antimicrob Agents Chemother. 53:2160–2162.
2009.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Cao B, Zhao CJ, Yin YD, Zhao F, Song SF,
Bai L, Zhang JZ, Liu YM, Zhang YY, Wang H, et al: High prevalence
of macrolide resistance in Mycoplasma pneumoniae isolates from
adult and adolescent patients with respiratory tract infection in
China. Clin Infect Dis. 51:189–194. 2010.PubMed/NCBI View
Article : Google Scholar
|
|
47
|
Seo YH, Kim JS, Seo SC, Seo WH, Yoo Y,
Song DJ and Choung JT: Predictive value of C-reactive protein in
response to macrolides in children with macrolide-resistant
Mycoplasma pneumoniae pneumonia. Korean J Pediatr. 57:186–192.
2014.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Ozden M, Kalkan A, Demirdag K, Kilic SS,
Denk A and Yuce P: Hepatocyte growth factor (HGF) in patients with
acute brucellosis. Scand J Infect Dis. 36:109–113. 2004.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Soeki T, Tamura Y, Shinohara H, Tanaka H,
Bando K and Fukuda N: Serial changes in serum VEGF and HGF in
patients with acute myocardial infarction. Cardiology. 93:168–174.
2000.PubMed/NCBI View Article : Google Scholar
|