Introduction
Approximately 20-40% of females of reproductive age
are diagnosed with leiomyomas, which consist of striated muscle
fibers arranged in a spiral pattern separated from the natural
uterine stroma by connective tissue (1,2). The
symptoms of leiomyomas and adenomyosis, the pathology of which
includes the endometrium breaking through the myometrium, include
bleeding abnormalities, mainly menorrhagia (50%) (3). These symptoms require treatment, which
may be conservative or surgical (3).
Treatment is personalized and based on the symptoms, the location
and size of the leiomyomas and the patient's preferences regarding
preservation of fertility. Surgical resection includes total
hysterectomy, open or laparoscopic myomectomy or, in cases with
submucosal tumors, hysteroscopic resection (4). Alternative methods for the treatment of
uterine leiomyomas include myolysis, interstitial thermotherapy and
pharmaceutical hormone therapy with the administration of
gonadotropin-releasing hormone agonists, aromatase inhibitors, oral
contraceptives (estrogen-progestogen combination or progestogen
alone) or placement of hormone-releasing intrauterine devices
(5,6). Anti-progestin agents, among which
mifepristone is the most extensively investigated, act at the level
of progesterone receptors, which are abundant in uterine leiomyomas
(7).
Uterine artery embolization (UAE) has been used as
an effective alternative method in the treatment of leiomyomas and
adenomyosis and is performed by percutaneous puncture of a common
femoral artery, selective catheterization of both uterine arteries
and injection of agents, such as polyvinyl alcohol (PVA) particles
or acrylic microspheres, for permanent embolization (8,9). The
procedure achieves vascular hypoxia followed by degeneration and
size reduction of the leiomyomas or adenomyomas/adenomyosis. Pain
and inflammation are the most common post-UAE complications
(10). To estimate the degree of
inflammation caused by UAE, the levels of the patients'
inflammatory markers were recorded immediately after the UAE and on
a weekly basis during their hospital stay and following discharge.
The aim of the present study was to evaluate the course of changes
in inflammatory parameters and pain post-UAE, in order to evaluate
the effect of UAE on the quality of life of the patients and to
determine whether UAE may be recommended as a safe alternative
treatment option, as compared with hysterectomy, in pre-menopausal
females with uterine leiomyomas and adenomyosis. It was
hypothesized that inflammation was the major reason for the
occurrence of post-interventional pain [the inflammatory parameters
that were investigated were white blood cell count (WBC) and
C-reactive protein (CRP)] and that WBC count and CRP levels are
crucial in acute-phase reactions and in the inflammatory process
triggered by UAE.
Patients and methods
Patients and pre-operative
examinations
A total of 270 pre-menopausal females with a mean
age of 42 years and 6 months ±5 years and 7 months-(range, 38-50
years) underwent UAE for uterine leiomyomas and/or adenomyosis.
Patients were examined between November 2013 and December 2017. CRP
and WBC count measurements were performed prior to and following
UAE. All patients provided written informed consent prior to the
UAE and underwent MRI, either on a 1 Tesla scanner (GE Healthcare)
or on a 1.5 Tesla magnet (Philips Multiva) up to 60 days prior to
the procedure. MRI included at least sagittal, coronal and axial
T2-weighted images (with and without fat saturation), transverse
T1-weighted images, and transverse, sagittal and coronal fat
saturated T1-weighted images after contrast administration.
Diffusion imaging was applied to the majority of the patients from
2014 onwards. Ethical approval for this procedure was confirmed by
the ethics committee of the University Hospital in Alexandroupolis,
Democritus University of Thrace (Alexandroupolis, Greece; reference
no. 8/37 10/10/13).
Exclusion criteria
Post-menopausal females, patients with serious
comorbidities, patients wishing to preserve their fertility,
patients with known allergy to the contrast agent utilized during
the procedure and patients with a suspected malignant condition
were excluded from the present study.
Procedure
The relevant symptoms noted when recording the
patient history included menometrorrhagia, dysmenorrhea,
dyspareunia and symptoms attributed to bulky disease or pressure on
pelvic organs. Two patients who had undergone fibromyectomy
followed by leiomyoma recurrence were also included. In all cases,
bilateral UAE was performed in one session, with percutaneous
puncture of the right common femoral artery and insertion of a 4F
catheter into the uterine arteries. The left uterine artery was
initially selectively accessed with the crossover technique and,
when the catheter bypassed the arteries supplying the vagina and
cervix, administration of the embolizing particles was initiated.
In the same manner, catheterization and embolization of the right
uterine artery was then performed. In the majority of the patients,
a 2.7 or 2.8 microcatheter was used to access the uterus following
selective catheterization of the uterine artery. Hydrogel-coated
acrylic microspheres (Embozene™; Celonova/Boston
Scientific) sized 500 or 700 µm were used as an embolic agent in
cases of adenomyosis, and the same microspheres, sized 700 and 900
µm, were administered slowly in cases with myomas. The criterion
for stopping particle administration was the fluoroscopic
identification of ‘almost complete stasis’ in the cases of
adenomyosis and ‘complete stasis’ in myomas.
Post-operative care and follow-up
Regarding pain management, 50 mg pethidine was
intramuscularly administered post-intervention and after 4 h and
then every 4 h as required for the first 24 h. Tramadol (50 mg) was
administered every 6 h and non-steroidal anti-inflammatory drug
tablets were administered every 12 h for 1 week. Pain assessment
was performed based on a visual analogue scale (from 0 to 10)
(10) using the numbering pain
rating scale (NPRS). After 1 day, the patients were discharged from
the hospital and administered broad-spectrum third-generation
cephalosporin antibiotics for 2 weeks. Antibiotics were also
administered during the intervention, by intravenous injection in
all cases. Clinical, laboratory and imaging follow-up examinations
by transvaginal ultrasonography and MRI scans were performed at 1,
3, 6 and 12 months after the procedure.
Leiomyoma size exhibited a mean reduction of 75%
over a follow-up period of 1 year post-UAE compared with the size
prior to treatment.
The present study included only pre-menopausal
females, particularly those who had completed their family
planning. However, two unplanned pregnancies were reported, both of
which were terminated. There were no cases with indications for
emergency hysterectomy.
Statistical analysis
Statistical analysis of the data was performed using
SPSS version 19.0 (IBM, Corp.). The normality of quantitative
variables was determined using a Kolmogorov-Smirnov test. Body
temperature and WBC counts were expressed as mean ± SD, while CRP
values and pain scores were expressed as median value and
interquartile range (25th to 75th percentile). Within group
differences of normally distributed quantitative variables (body
temperature and WBC) were examined by one-way repeated measures
ANOVA while post hoc analysis was performed using the
paired-samples t-test, with adjusted level of significance at
a=0.005 according to Bonferroni's correction. Within-group
differences of CRP values and pain scores were examined by Friedman
test; post hoc analysis was performed using Wilcoxon signed ranks
test, with adjusted level of significance at α=0.01. P<0.05 was
considered to indicate a statistically significant difference.
Results
Description of the procedure and
technical details
The procedure was performed without any technical
restrictions in all patients, as punctured and catheterized
arteries were always visible on display when imaged using
angiography (the first step for the UAE procedure) and
super-selective embolization was feasible. In 265 of the 270
patients included in the present study, the post-interventional
course was free of procedure-associated complications. In 4
patients, embolization resulted in necrosis and liquefaction of
submucosal lesions. The MRI performed during the 1st month after
UAE revealed dilation of the internal cervical orifice by
protrusion of the necrotic element. Antibiotic coverage and
therapeutic curettage were performed without any further
complications. In 1 patient, undesired embolization was reported
due to unattended backflow of particles or spread of particles
during the removal of the embolization catheter. The clinical
examination revealed a small area of skin necrosis on the right
buttock 15 days after the intervention, which was successfully
treated by local application of gauzes with fucidic acid of fucidin
compresses with antibiotics and healed 2 weeks later. After a
period of 14 months, the same patient reported a pregnancy
termination due to personal wishes. Based on the laboratory
results, hormonal changes were confirmed only during the early
post-interventional period. No differences were observed between
anti-Müllerian hormone and follicle-stimulating hormone levels at
12 months post-treatment compared with the pre-treatment levels and
there were no cases of permanent amenorrhea.
Statistically significant changes in CRP, body
temperature and WBC were observed (all P<0.001). Post hoc
analysis revealed that all markers exhibited a significant increase
on the second post-operative day, reaching peak values on the third
day (from the initial levels; and the WBC count, 17.71±2.53 Κ/µl,
increased by 143.3%). Subsequently, all markers returned to the
initial levels on the fourth day. The levels of all three markers
were significantly higher in patients compared with healthy
controls at the second and third day (Figs.
1-3).
Changes in inflammatory
parameters
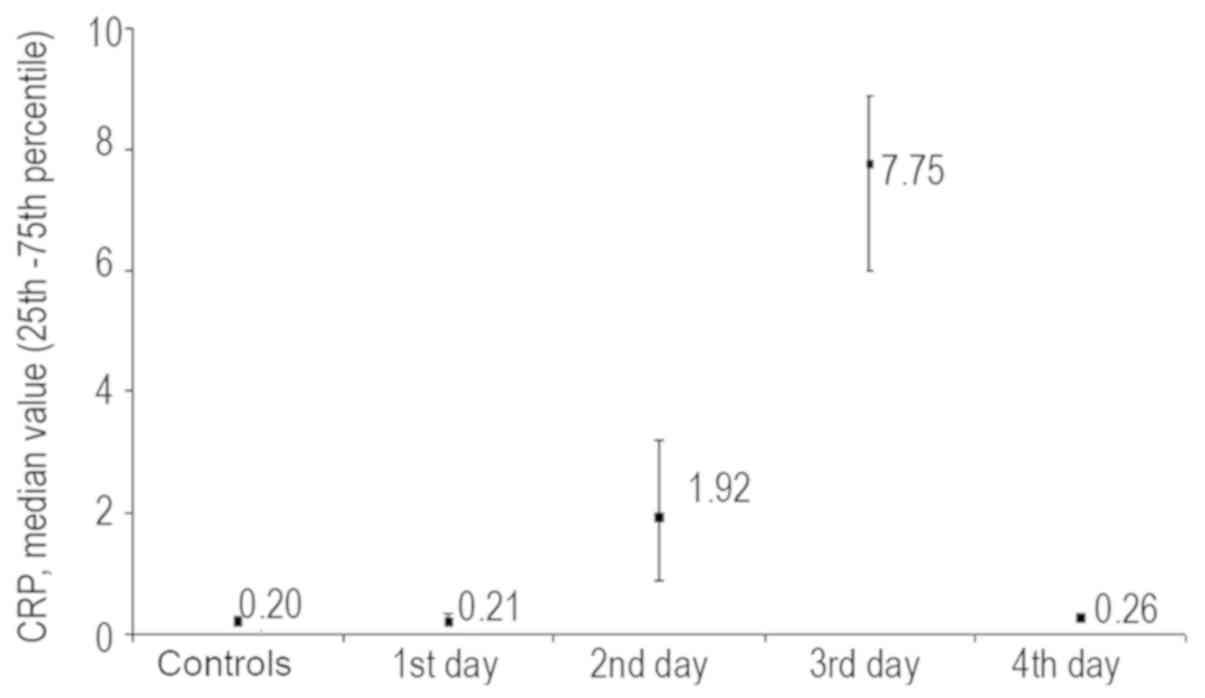
The chronological course of alterations in the CRP
levels was clearer compared with that of the WBC count. A value of
6.0 mg/dl was set as the point of reference based on
recommendations from the Department of Microbiology and
Biopathology of Democritus University of Thrace for non-surgical
procedures. None of the patients had an increased CRP value prior
to the procedure. Post-UAE, an increase in the CRP levels to
7.75±3.5 mg/dl was observed, with level alterations ranging between
8.3 and 11.9 mg/dl (Fig. 1). The
patient who developed buttock skin necrosis exhibited a value
increase of up to 7.75 mg/dl, whilst the other 4 patients with
leiomyoma necrosis exhibited an increase of 6.4 mg/l. The CRP level
appeared to rise mainly between post-operative days 2 and 4,
followed by normalization. The chronological course of CRP levels
is depicted in Fig. 1. A
normalization in CRP levels was noted within the first 4 days,
after reaching a maximum level increase on post-interventional day
3, due the time needed for the leiomyoma to be necrotized in
aseptic conditions.
Regarding the association of CRP with other
parameters, the maximum CRP level values are known to depend on the
quantity of microsphere UAE material used (11), inferring that the embolization of the
leiomyoma mass may affect the CRP value increase, no such
association was observed in the present study. The same conclusion
was reached when assessing the association between CRP levels and
uterine size. In the current study the same quantity of embolic
agent was always used, contrary to other published studies that
have investigated various embolic agents (11-14).
An increase in the CRP value to 6.0 mg/dl was observed, while it
reached 8.0 mg/dl or higher in certain cases. These CRP changes
occurred with a relative delay on post-operative days 2-4. In the
majority of cases, the values subsequently returned to the normal
range (Fig. 1).
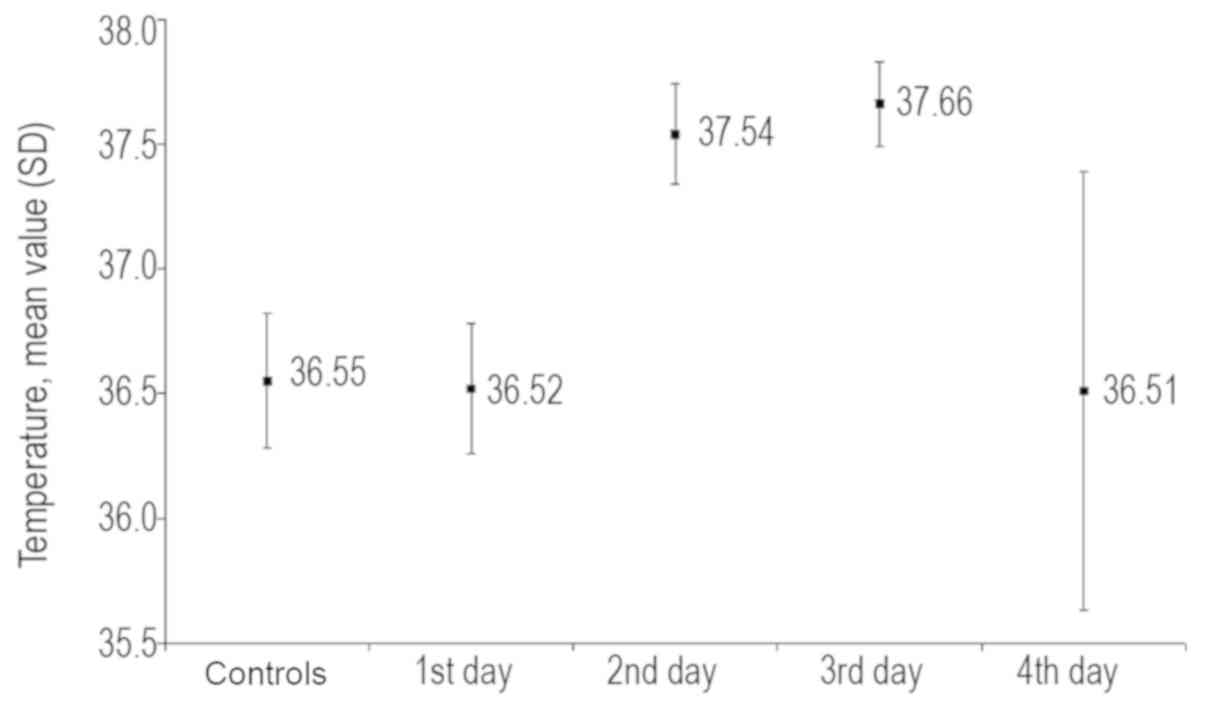
Post-interventional body temperature changes are
provided in Fig. 2. No cases showed
an increased temperature of >38˚C.
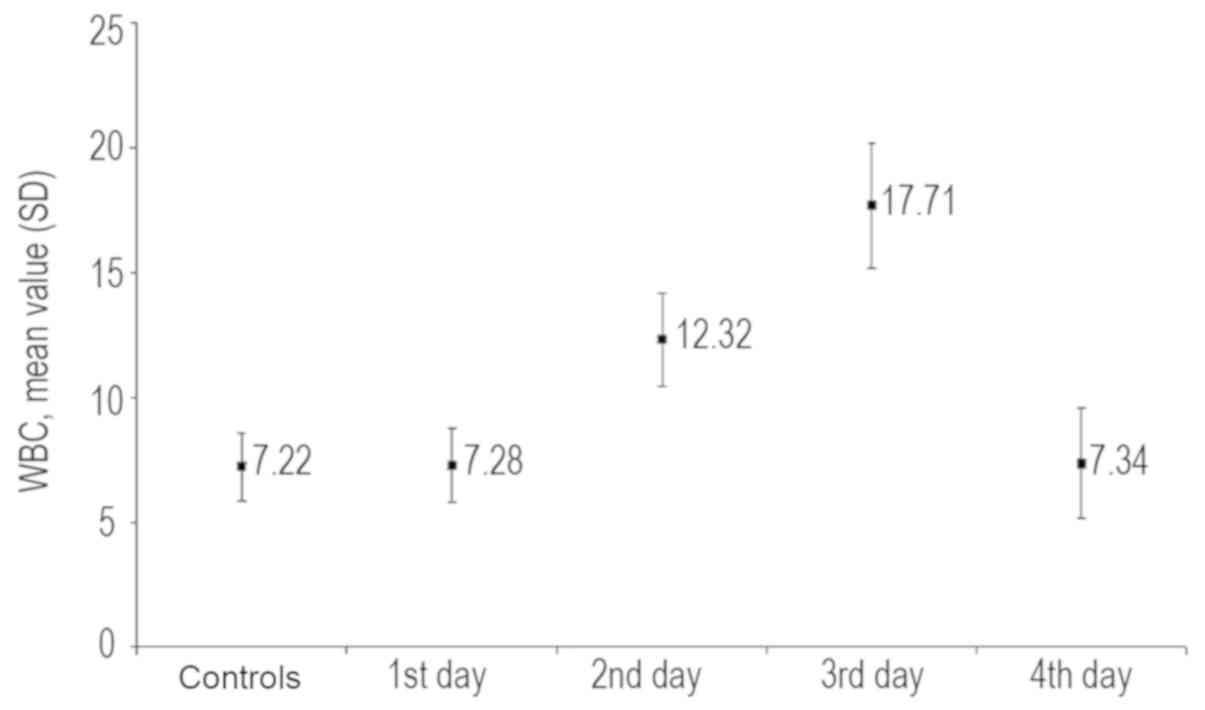
Following UAE, a mild increase in the WBC count was
observed with the value remaining at the upper limit of the normal
range (3.5-10.80 Κ/µl) suggested by the Department of Microbiology
and Biopathology of Democritus University of Thrace).
Association between leukocytosis and
time
Following UAE, an increase in the WBC count was
noted from 7.22±1.75x109/l prior to UAE to a mean
maximum WBC count of 10.8±3.5 Κ/µl (range, 5.9-18.6 Κ/µl). In 2
patients, the WBC count appeared slightly elevated at 11 K/µl prior
to UAE (the upper limit of the normal value is 10 Κ/µl based on
reference values from the Department of Microbiology and
Biopathology of Democritus University of Thrace).
Post-UAE, leukocytosis was observed in the majority
of the patients on days 2 and 3 (10.6 Κ/µl). An elevation was
observed on day 2, with a peak reached at day 3, which returned to
baseline levels on day 4 (Fig. 3),
as well as days 8-10, with a further increase on day 11 (11.5 Κ/µl)
post-intervention. In patients with leiomyoma necrosis,
leukocytosis of up to 15 Κ/µl was observed (Fig. 3).
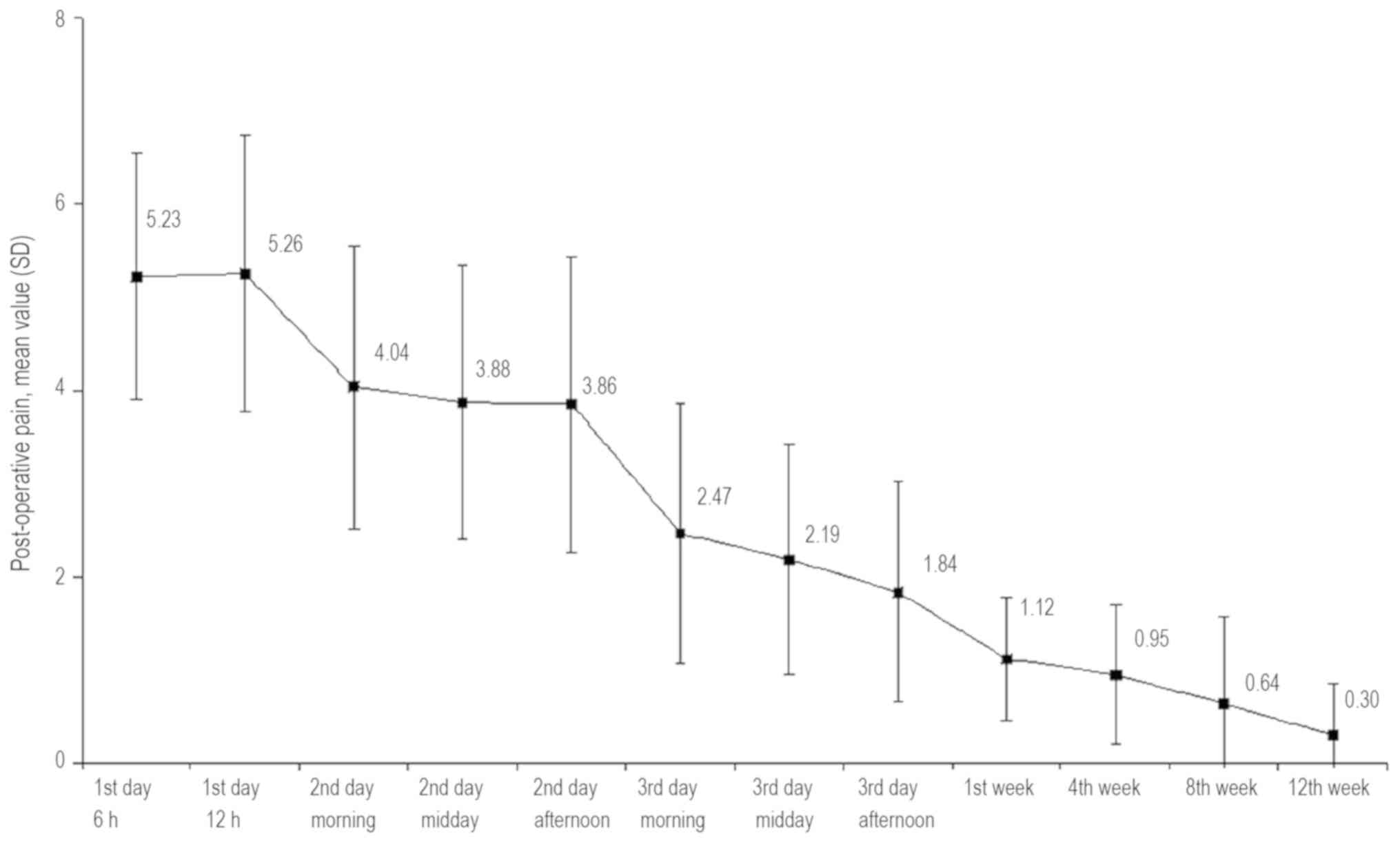
Pain score
A statistically significant reduction of
post-operative pain was observed over time (χ2=913.494;
degrees of freedom=11; P<0.001). Post-hoc analysis using
Wilcoxon's signed-ranks test, with an adjusted level of
significance at α=0.01, was then performed. At 6 h after UAE, the
pain score ranged from 3 to 8, with a median score of 5
(interquartile range, 4-6; mean score, 5.23±1.32); it remained
unchanged during the 1st post-interventional day (12th vs. 6th
post-interventional hour; P=0.752). A significantly lower pain
score was observed in the morning of the 2nd post-interventional
day (P<0.001), remaining at the same level throughout the day.
Post-intervention the patients received an anti-pain medication (50
mg Tramadol) that was prescribed for 1-4 times per day for 4-7 days
after the procedure, which positively influenced the pain course
after the procedure.
The pain score exhibited a statistically significant
reduction in the morning of the 3rd post-interventional day
(P<0.001) and continued to decrease until the afternoon of the
same day. The pain score continued to decline significantly
throughout the follow-up period, reaching its lowest point at the
12th week (range, 0-3; median, 0; mean, 0.30±0.55). The mean pain
score is shown in Fig. 4.
Summary
The major results of the present study on UAE in
were as follows: No significant changes in inflammatory parameters,
specifically the CRP values and WBC counts; no marked fluctuation
in pain levels and no life-threatening complication
post-interventional UAE occurred. No case of permanent amenorrhea
was encountered. The second, third and fourth measurements of the
inflammatory parameters were performed at 3, 6 and 12 months
post-intervention.
Discussion
A number of molecular and cytogenetic studies have
indicated that leiomyomas are tumors that originate from a single
cell (monoclonal origin) and that multiple uterine leiomyomas in
the same uterus are of completely independent origin (15-18).
Although the majority of uterine leiomyomas appear to have a normal
karyotype, ~40% display chromosomal abnormalities, which may be
divided into 7 major cytogenetic subcategories: i) Reciprocal
translocation of the 12th and 14th chromosomes [t (12;14)]; ii)
chromosome 6 (6p21) short-arm rearrangement; iii) deletions in the
long arm of chromosome 7 [del (7)
q22q32)]; iv) deletions in the long arm of chromosome 3; v)
long-arm rearrangements in chromosome 10; vi) trisomy12; and vii)
rearrangements in chromosome X.
The various mutation types in leiomyomas indicate
that genetic mechanisms underlie their development. A different
expression profile of miRNAs has been identified in uterine
leiomyomas compared with that in the normal myometrium (15-18).
Leiomyomas display intense mitotic activity in the smooth muscle
cell component and reduced apoptosis (programmed cell death). These
two factors are considered to be a result of progesterone activity
and lead to an increase in tumor size (15-18).
Progesterone increases the protein expression of Bcl-2, which
prevents cell apoptosis, and at the same time, it inhibits the
expression of tumor necrosis factor-α, a factor promoting
apoptosis. Estrogens are considered to promote leiomyoma
development by increasing the levels of the growth factors
insulin-like growth factor-1, epidermal growth factor receptor,
transforming growth factor (TGF)-β1, TGF-β3 and platelet-derived
growth factor, and contribute to the abnormal survival of uterine
leiomyoma cells by reducing factor p53, increasing anti-apoptotic
factor purkinje cell protein 4 expression and antagonizing
peroxisome proliferator-activated receptor-γ signaling (15-18).
UAE is a minimally invasive procedure that aims to
improve symptoms by interrupting the blood flow to leiomyomas and
reduce blood flow to the muscles at the arteriolar level, using
bilateral hyperselective catheterization of the myometrial feeder
arteries and release of embolizing particles (particles 500-900 µm
in diameter, usually beads of acrylic polymers or PVA particles) to
induce irreversible ischemic damage and degeneration/shrinkage of
the leiomyomas (19-22).
According to previous studies, the treatment success rate for
menometrorrhagia is 80-100% and for pressure phenomena, it is
60-100% (23-26).
In these studies a decrease in leiomyoma size of 40-70% was
observed in the first 6 months, followed by 50-80% in the months
that ensued (23-26,27).
A number of studies include uterine size in the success criteria,
whilst others use the number of leiomyomas as well as uterus size
to assess treatment success (23-26).
Adenomyosis may be diffuse or focal (adenomyoma),
and it may be pure or, more commonly, mixed (coexistent with
leiomyomas), asymmetrically affecting the uterine wall of
pre-menopausal females (12,26,28). The
disease is common in clinical practice, manifesting with
non-specific symptoms and signs, including bleeding/anemia,
dysmenorrhea, dyspareunia, bulk symptoms/sensitive uterus or a
combination of the above caused by leiomyomas (12,26,28);
therefore, it is difficult to diagnose based on the clinical
criteria alone. Adenomyosis occurs predominantly in multiparous
females with an incidence of 5-70%. In 80% of females, adenomyosis
coexists with another uterine condition: Leiomyoma (up to 53% of
females with adenomyosis), pelvic endometriosis and endometrial
polyps (2-20%), endometrial hyperplasia and adenocarcinoma
(12,26,28,29).
Approximately 35% of females with adenomyosis are asymptomatic and
the diagnosis is based on routine gynecological transvaginal
ultrasound; MRI contributes decisively to the diagnosis. For the
differential diagnosis and staging of the disease, MRI is clearly
the examination of choice due to its sensitivity (88-93%) and
specificity (66-91%) (12,26,28-30).
However, clinical diagnosis of adenomyosis is only hypothetical and
the disease is definitively diagnosed based on histological
examination following hysterectomy (12,26,28-30).
Inflammation appears at a rate of 1-2% and is based
on tissue reaction to post-interventional ischemia; inflammation is
an interaction between cells and cytokines and should be diagnosed
at an early stage in order to prevent sepsis, emergency
hysterectomy and death (11,13,14,31). The
inflammatory reactions resulting from UAE intervention in
combination with post-ischemic and post-necrotic reactions is the
major explanation for the occurrence of pain. Serious complications
may appear even at 6 months post-treatment (11,13,14,31). Any
alterations in inflammatory parameters, body temperature or
leukocytosis, along with CRP levels and pain evaluation, should be
monitored until 6 months post-embolization (11,13,14,31-36).
CRP is an acute-phase pro-inflammatory cytokine, which is crucial
in the acute phase of inflammation and increases progressively in
association with the inflammatory process (11,13,14,31-36).
In the present study, leukocytosis of up to 16.0
K/µl and an increase in CRP levels of up to 8.0 mg/l were not
considered alarming based on the recommendations of the Departments
of Microbiology and Biopathology, Democritus University of Thrace,
Greece. It is recommended that patients should be informed in
detail in case of abdominal pain, heavy vaginal bleeding and an
increased temperature, and advised to contact their doctor. To
date, ~100,000 successful UAEs have been performed in total
worldwide (20). In our institution,
(the Department of Interventional Radiology and Medical Imaging,
Democritus University of Thrace) approximately 400 embolizations
have been performed. It is evident that leiomyoma embolization,
similarly to laparoscopic or endoscopic myolysis, should be
performed following strict criteria and parameters. A gynecologist
and an interventional radiologist must confirm therapeutic
indications. The frequency of complications among the participants
in the present study was low. Necrosis and liquefaction of
submucosal leiomyomas were reported in 4 cases and a small area of
skin necrosis on the right buttock developed in 1 case; these were
successfully treated either by fractional curettage or, in the
latter case, by conservative local therapy. Various retrospective
and prospective studies on UAE, as well as case reports on
associated complications, have been published in the international
literature (37,38).
Complications are generally caused by either the
catheterization procedure or the effects of uterine ischemia, which
may cause necrosis, pain and sepsis. The ovaries may also be
affected. Deaths following UAE are rare (1:1,600) and are mainly
attributed to pulmonary embolism, which may be due to the effect of
the necrotic tissue on activation of the coagulation cascade and on
inflammation (37,38).
The complications of catheterization, including
hematoma, allergy to contrast media and pseudo-aneurysm or vascular
separation, are rare (<1%) (37,38).
Elimination of uterine leiomyomas occurs in 5% of cases and may
cause inflammation requiring a repeat uterine embolization or
hysterectomy. Necrotic tissue, if not removed in a timely manner,
may become infected and the condition may be severe (37,38).
Cases with submucosal leiomyomas should be treated
hysteroscopically. Ischemia may lead to the development of
endometritis, pelvic inflammation and pyometra, with poor outcome
unless hysterectomy is performed (37,38).
It has been reported that in 11% of the cases, an
additional circulatory network is present between the ovaries and
the uterus, while in 5% of cases the ovaries are supplied
exclusively by uterine vessels (27). The rates of transient or permanent
amenorrhea may vary according to the age of the patient. While
among young females, the rates range from 0 to 5%, they may reach
43% in females aged >45 years (27). It has been estimated that, if a
patient experiences amenorrhea for a period of 3-11 months,
menopause is likely to occur (~95%) within the next 4 years
(27). On the other hand, females
who have amenorrhea for 1 year have a 10.5% chance of having a
normal menstrual cycle in the future if their age is between 45-49
years (27).
The rate of post-UAE complications is markedly lower
compared with that after hysterectomy, as reported in previous
studies. In retrospective studies comparing myomectomy with UAE,
there was a requirement for transfusion in 12% of cases and the
incidence of complications was 19-25% after fibromyomectomy vs. 0
and 4.2% after UAE, respectively (39,40). The
duration of hospitalization and the time until patients returned to
work after UAE were ~1 and 10 days, respectively, which were
significantly shorter compared with those for surgical methods
(39,40).
The present results are consistent with those of
other studies (27,37,39,40) that
stated that inflammatory parameters are not important prognostic
factors following UAE. Ιt is crucial to develop an objective method
for assessing bleeding during menstruation in order to select the
most suitable candidates to undergo effective therapeutic
approaches other than invasive surgery, including UAE.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
VS participated in the review process, prepared the
manuscript, performed all procedures and described the techniques.
DD collected data and relevant literature. XA contributed to
manuscript corrections and collected data and relevant literature.
AC, AB and FG collected data and literature. GT performed the
statistical analysis. GI, SZ and GG corrected and modified the
manuscript. DS and SM corrected the figures. TV was responsible for
the pain protocol. NN contributed to study design. PT participated
in the review process, prepared the manuscript and made substantive
intellectual contributions to the published study. All authors read
and approved the final version of the manuscript.
Ethics approval and consent to
participate
Approval for this procedure was confirmed by The
Ethics Committee of the University Hospital in Alexandroupolis,
Democritus University of Thrace (Alexandroupolis, Greece; reference
no. 8/37 10/10/13) and patients provided written informed consent
to their participation in the study.
Patient consent for publication
All patients provided written informed consent to
publication of their data for a scientific purpose before the
procedure.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Calaf J, Arqué M, Porta O and D'Angelo E:
The fibroid as clinical problem. Med Clin (Barc). 141 (Suppl
1):S1–S6. 2013.(In Spanish). PubMed/NCBI View Article : Google Scholar
|
|
2
|
O'Sullivan M and Overton C: Tailor
management to the patient with fibroids. Practitioner. 261:19–22.
2017.PubMed/NCBI
|
|
3
|
Donnez J and Dolmans MM: Uterine fibroid
management: From the present to the future. Hum Reprod Update.
22:665–686. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Falcone T and Parker WH: Surgical
management of leiomyomas for fertility or uterine preservation.
Obstet Gynecol. 121:856–868. 2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Stovall DW: Alternatives to hysterectomy:
Focus on global endometrial ablation, uterine fibroid embolization,
and magnetic resonance-guided focused ultrasound. Menopause.
18:437–444. 2011.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sabry M and Al-Hendy A: Medical treatment
of uterine leiomyoma. Reprod Sci. 19:339–353. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Carbonell Esteve JL, Riverón AM, Cano M,
Ortiz AI, Valle A, Texidó CS and Tomasi G: Mifepristone 2.5 mg
versus 5 mg daily in the treatment of leiomyoma before surgery. Int
J Womens Health. 4:75–84. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wang S, Meng X and Dong Y: The evaluation
of uterine artery embolization as a nonsurgical treatment option
for adenomyosis. Int J Gynaecol Obstet. 133:202–205.
2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Tomislav S, Josip M, Liana CS, Marko V,
Marko J, Ante R, Dzenis J, Leo G, Ivica S, Marijan T and Situm K:
Uterine artery embolization as nonsurgical treatment of uterine
myomas. ISRN Obstet Gynecol. 2011(489281)2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Tropeano G, Amoroso S and Scambia G:
Non-surgical management of uterine fibroids. Hum Reprod Update.
14:259–274. 2008.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Stampfl S, Stampfl U, Bellemann N, Sommer
CM, Thierjung H, Radeleff B, Lopez-Benitez R, Berger I, Kauffmann
GW and Richter GM: Biocompatibility and recanalization
characteristics of hydrogel microspheres with polyzene-F as polymer
coating. Cardiovasc Intervent Radiol. 31:799–806. 2008.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Lohle PN, De Vries J, Klazen CA, Boekkooi
PF, Vervest HA, Smeets AJ, Lampmann LE and Kroencke TJ: Uterine
artery embolization for symptomatic adenomyosis with or without
uterine leiomyomas with the use of calibrated tris-acryl gelatin
microspheres: Midterm clinical and MR imaging follow-up. J Vasc
Interv Radiol. 18:835–841. 2007.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Stampfl S, Bellemann N, Stampfl U, Sommer
CM, Thierjung H, Lopez-Benitez R, Radeleff B, Berger I and Richter
GM: Arterial distribution characteristics of Embozene particles and
comparison with other spherical embolic agents in the porcine acute
embolization model. J Vasc Interv Radiol. 20:1597–1607.
2009.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Joffre F, Tubiana JM and Pelage JP: Groupe
FEMIC: FEMIC (Fibromes Embolisés aux MICrosphères calibrées):
Uterine fibroid embolization using tris-acryl microspheres. A
French multicenter study. Cardiovasc Intervent Radiol. 27:600–606.
2004.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Gross KL and Morton CC: Genetics and the
development of fibroids. Clin Obstet Gynecol. 44:335–349.
2001.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Meloni AM, Surti U, Contento AM, Davare J
and Sandberg AA: Uterine leiomyomas: Cytogenetic and histologic
profile. Obstet Gynecol. 80:209–217. 1992.PubMed/NCBI
|
|
17
|
Ligon AH and Morton CC: Genetics of
uterine leiomyomata. Genes Chromosomes Cancer. 28:235–245.
2000.PubMed/NCBI
|
|
18
|
Marsh EE, Lin Z, Yin P, Milad M,
Chakravarti D and Bulun SE: Differential expression of microRNA
species in human uterine leiomyoma versus normal myometrium. Fertil
Steril. 89:1771–1776. 2008.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Raikhlin A, Baerlocher MO and Asch MR:
Uterine fibroid embolization: CME update for family physicians. Can
Fam Physician. 53:25025–25026. 2007.PubMed/NCBI
|
|
20
|
Marshburn PB, Matthews ML and Hurst BS:
Uterine artery embolization as a treatment option for uterine
myomas. Obstet Gynecol Clin North Am. 33:125–144. 2006.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Szkodziak P, Szkodziak F, Trzeciak K and
Czuczwar P: Minimally invasive procedures in the management of
uterine fibroids. Prz Menopauzalny. 16:122–125. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Vilos GA, Allaire C, Laberge PY and
Leyland N: SPECIAL CONTRIBUTORS: The management of uterine
leiomyomas. J Obstet Gynaecol Can. 37:157–178. 2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Kubik-Huch RA, Weston M, Nougaret S,
Leonhardt H, Thomassin-Naggara I, Horta M, Cunha TM, Maciel C,
Rockall A and Forstner R: European society of urogenital radiology
(ESUR) guidelines: MR imaging of leiomyomas. Eur Radiol.
28:3125–3137. 2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Cura M, Cura A and Bugnone A: Role of
magnetic resonance imaging in patient selection for uterine artery
embolization. Acta Radiol. 47:1105–1114. 2006.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Early HM, McGahan JP, Scoutt LM, Revzin M,
Lamba R, Corwin M, Fananapazir G and Sekhon S: Pitfalls of
sonographic imaging of uterine leiomyoma. Ultrasound Q. 32:164–174.
2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Tamai K, Koyama T, Umeoka S, Saga T, Fujii
S and Togashi K: Spectrum of MR features in adenomyosis. Best Pract
Res Clin Obstet Gynaecol. 20:583–602. 2006.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Tsikouras P, Manav B, Koukouli Z,
Trypsiannis G, Galazios G, Souftas D and Souftas V: Ovarian reserve
after fibroid embolization in premenopausal women. Minim Invasive
Ther Allied Technol. 26:284–291. 2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Kim MD, Kim S, Kim NK, Lee MH, Ahn EH, Kim
HJ, Cho JH and Cha SH: Long-term results of uterine artery
embolization for symptomatic adenomyosis. AJR Am J Roentgenol.
188:176–181. 2007.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Levgur M: Therapeutic options for
adenomyosis: A review. Arch Gynecol Obstet. 276:1–15.
2007.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Alvi FA, Glaser LM, Chaudhari A, Tsai S
and Milad MP: New paradigms in the conservative surgical and
interventional management of adenomyosis. Curr Opin Obstet Gynecol.
29:240–248. 2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Stampfl S, Stampfl U, Bellemann N,
Radeleff B, Lopez-Benitez R, Sommer CM, Thierjung H, Berger I and
Richter GM: Immunohistochemical characterization of specific
inflammatory tissue reactions following embolization with four
different spherical agents in the minipig kidney model. J Vasc
Interv Radiol. 20:936–945. 2009.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Kim HS, Czuczman GJ, Nicholson WK, Pham LD
and Richman JM: Pain levels within 24 hours after UFE: A comparison
of morphine and fentanyl patient-controlled analgesia. Cardiovasc
Intervent Radiol. 31:1100–1107. 2008.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Lampmann LE, Lohle PN, Smeets A, Boekkooi
PF, Vervest H, van Oirschot CM and Bremer RC: Pain management
during uterine artery embolization for symptomatic uterine
fibroids. Cardiovasc Intervent Radiol. 30:809–811. 2007.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Jensen LL, Handberg G, Helbo-Hansen HS,
Skaarup I, Lohse T, Munk T and Lund N: No morphine sparing effect
of ketamine added to morphine for patient-controlled intravenous
analgesia after uterine artery embolization. Acta Anaesthesiol
Scand. 52:479–486. 2008.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Roth AR, Spies JB, Walsh SM, Wood BJ,
Gomez-Jorge J and Levy EB: Pain after uterine artery embolization
for leiomyomata: Can its severity be predicted and does severity
predict outcome? J Vasc Interv Radiol. 11:1047–1052.
2000.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Valdes-Devesa V, Jimenez MDM, Sanz-Rosa D,
Espada Vaquero M, Alvarez Moreno E and Sainz de la Cuesta Abbad R:
Preoperative diagnosis of atypical pelvic leiomyoma and sarcoma:
The potential role of diffusion-weighted imaging. J Obstet
Gynaecol. 39:98–104. 2019.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Margau R, Simons ME, Rajan DK, Hayeems EB,
Sniderman KW, Tan K, Beecroft JR and Kachura JR: Outcomes after
uterine artery embolization for pedunculated subserosal leiomyomas.
J Vasc Interv Radiol. 19:657–661. 2008.PubMed/NCBI View Article : Google Scholar
|
|
38
|
McLucas B, Chespak L and Kaminsky D: Myoma
necrosis following Gelfoam embolization of uterine myomata. Minim
Invasive Ther Allied Technol. 17:200–204. 2008.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Choi HJ, Jeon GS, Kim MD, Lee JT and Yoon
JH: Is uterine artery embolization for patients with large myomas
safe and effective? A retrospective comparative study in 323
patients. J Vasc Interv Radiol. 24:772–778. 2013.PubMed/NCBI View Article : Google Scholar
|
|
40
|
de Bruijn AM, Lohle PN, Huirne JA, de
Vries J, Twisk M, QUESTA-Trial Group and Hehenkamp WJ:
Uterine artery embolization versus hysterectomy in the treatment of
symptomatic adenomyosis: Protocol for the randomized QUESTA trial.
JMIR Res Protoc. 7(e47)2018.PubMed/NCBI View Article : Google Scholar
|