Introduction
The increasing prevalence of obesity and overweight
is a public health problem, it has been estimated that in 2038
approximatively 38% of the world population will be overweight and
20% will be obese (1). However,
PREDATORR study, a study performed on a Romanian population sample
between 2012 and 2014, revealed that already these predictions have
come true, with a prevalence of obesity and overweight of 31.90 and
37.40% (2).
Obesity and overweight have a multi-factorial
aetiology, but the most important factor appears to be the shift in
the environmental and socioeconomic conditions in the last century
with unlimited access to hypercaloric food and decreased physical
activity (3). Current data point to
the fact that although genetic factors contribute to the risk of
obesity, the influence is modest with an average difference of only
2.7 kg/m2 between individuals with high genetic risk and
those with low genetic risk (4). On
the other hand, the weight gain is strongly associated with
unhealthy diet consisting of high intake of fast-food,
sugar-sweetened beverages, processed meat and low intake of whole
grains, fruits and vegetable (5).
Sedentary behaviour is another important risk factor for weight
gain, studies indicate that at least 150-200 min per week of
physical exercise is necessary in order to prevent weight gain
(6). The reason why the study of
obesity is so intense in the last decades is that adipose tissue is
associated with increased risk of cardiovascular morbidity. Obesity
is associated with increased inflammation as a result of production
of proinflammatory cytokines, insulin resistance, endothelial
dysfunction, increased reactive oxygen species production and
reactive, sympathetic nervous system activation and coagulation
activation that result in high incidence of type 2 diabetes
mellitus, dyslipidaemia, hypertension and atherosclerosis (7).
This study determined the prevalence of the risk
factors for adiposity in a population from Oradea, Bihor County,
Romania, and determined their impact on the prevalence of obesity
and overweight. The evaluated risk factors in our study included
fast-food consumption, alcohol intake, sleeping duration, presence
of depression, family history of obesity, caloric consumption, and
level of physical activity.
Materials and methods
An observational study was conducted. The subjects
included in the study were individuals registered on the patient
lists of two general practitioners from Oradea, Romania. All the
individuals aged between 18-65 years in these lists were considered
for inclusion in the study. The inclusion criteria were:
individuals that gave their written accept for participation in the
study, individuals with the age criteria specified above. The
exclusion criteria were: individuals with psychiatric diseases,
individuals with neurodegenerative disorders, subjects with
neoplastic diseases, subjects with endocrine diseases
(hypothyroidism, hyperthyroidism, Cushing disease, etc.), patients
with liver cirrhosis, patients with end stage kidney disease and
subjects that in the past 3 months were under treatment with drugs
that can significantly increase/decrease weight. An initial 1,120
number of individuals were considered for inclusion in the study.
After applying the inclusion and exclusion criteria 900 individuals
remained in the study.
The research was performed according the WMA
Declaration of Ethics, Helsinki - Medical Research Involving Human
Principles for Subjects. All the subjects signed a written consent
giving their acceptance to participate in the study. The study was
approved by the Ethics Council of the Clinical Emergency Hospital
of Oradea (Oradea, Romania).
The initial 1,120 individuals were asked to come for
a first presentation at the general practitioners. The subjects
that were eligible for participation in the study, were instructed
to come on a specific day for further evaluation and to keep a
journal of the entire food intake two days before that day (for
evaluation of caloric intake). At the second presentation, the
subject was clinically evaluated, and blood was collected for
laboratory work-up. Body-mass index was calculated, abdominal
circumference was measured, and blood pressure was taken. The
patients completed a questionnaire regarding their lifestyle and
Beck's questionnaire for depression. Food intake in the past two
days before presentation was evaluated and caloric intake average
between the 2 days was determined. Frequent fast-food consumption
was defined as buying, ordering fast-food products at least three
times a week. Excessive alcohol consumption was defined as
consumption of >2 measures (12 g pure alcohol) of alcohol for
men and 1 measure of alcohol for women a day. Hyper caloric diet
was defined as consumption of more calories than the recommended
daily intake according to BMI and physical activity. Sedentary
lifestyle was defined as performing physical exercise <150
min/week. Presence of depression was defined as a Beck's score ≥14.
Unhealthy lifestyle was defined as the presence of at least 4 of
the 6 criteria: hypercaloric nutrition, frequent fast-food
consumption, <3 meals/day, excessive alcohol consumption,
sedentary lifestyle and <6 h of sleep/day. Statistical analysis
was done using Biostat software. Relative risk was calculated with
the formula RR=Pe/Pu, where Pe is
the prevalence in the exposed group while Pu is the
prevalence in the unexposed group. A value of P<0.05 was
considered statistically significant.
Results
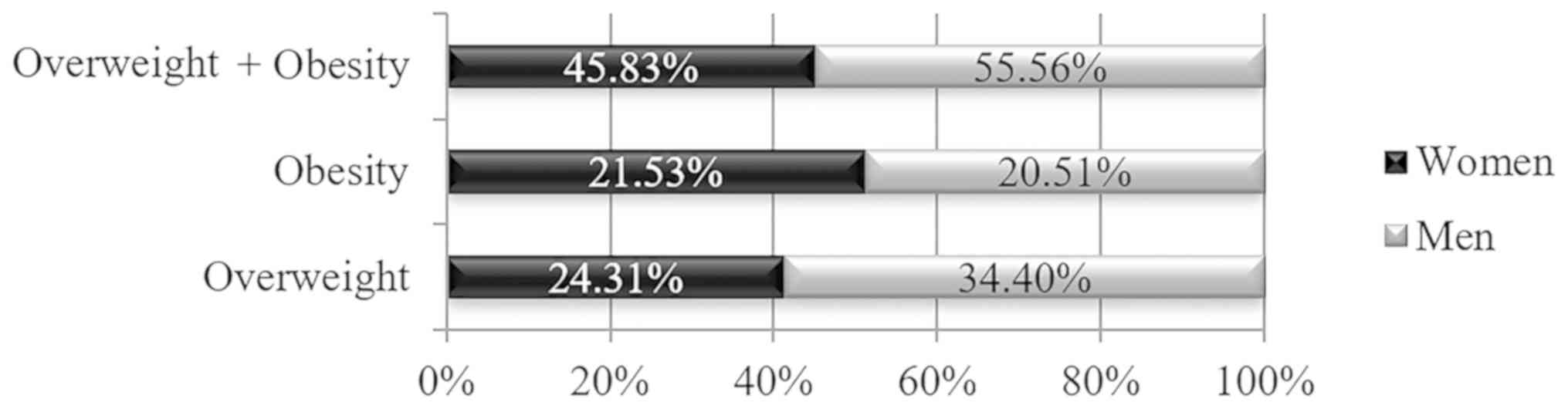
In the current study, 48% (432 individuals) were
females, and 52% (468 individuals) were males. Overweight
prevalence was 29.56% (266 individuals), while obesity prevalence
was 21.33% (192 individuals). The prevalence of normal weight was
49.11%. Overall the prevalence of overweight and obesity was 50.89%
(458 ndividuals).
Overweight prevalence was statistically
significantly higher among men than among women (34.40 vs. 24.31%,
P<0.01) while the prevalence of obesity was statistically
non-significantly higher among women (21.53 vs. 20.51%, P=0.70)
(Fig. 1).
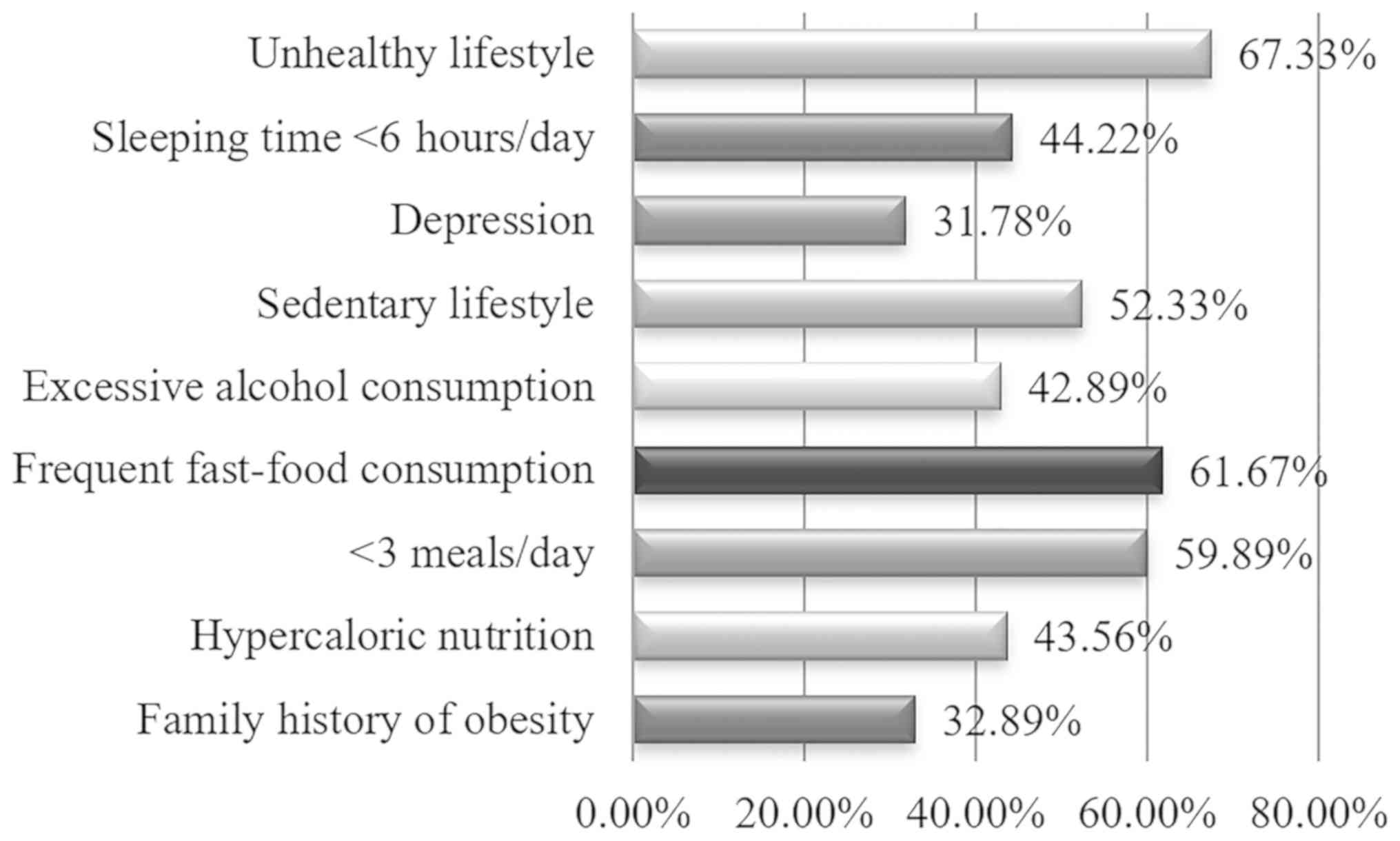
The prevalence of risk factors for overweight and
obesity was the fallowing: sleeping time <6 h/day in 44.22% of
the included individuals, depression in 31.78%, sedentary lifestyle
in 52.33%, excessive alcohol consumption in 42.89%, frequent
fast-food consumption in 61.67%, <3 meals/day in 59.89%,
hypercaloric nutrition in 43.56% and family history of diabetes in
32.89% (Fig. 2).
Comparing the frequency of risk factors for
adiposity in the men and women it was observed that family history
of obesity was statistically non-significantly more prevalent among
women (35.65 vs. 30.34%, P=0.09), hypercaloric nutrition was
statistically non-significantly more prevalent among men (45.73 vs.
41.20%, P=0.17), eating <3 meals/day was statistically
non-significantly more prevalent among women (60.19 vs. 59.62%,
P=0.86), frequent fast-food consumption was statistically
non-significantly more prevalent among men (63.68 vs. 59.49%,
P=0.83), excessive alcohol consumption was statistically
significantly more prevalent among men (58.55 vs. 25.93%,
P<0.01), sedentary lifestyle was statistically significantly
more prevalent among women (61.11 vs. 44.23%, P<0.01),
depression was statistically significantly more prevalent among
women (35.88 vs. 27.99%, P=0.01), sleeping time <6 h/day was
statistically significantly more prevalent among women (48.84 vs.
39.96%, P<0.01), unhealthy lifestyle was non-significantly more
prevalent among men (68.59 vs. 65.97%, P=0.40). The data are
summarized in Table I. As shown in
Table II unhealthy lifestyle was
defined as the presence of at least 4 of the 6 criteria:
hypercaloric nutrition, frequent fast-food consumption, <3
meals/day, excessive alcohol consumption, sedentary lifestyle and
<6 h of sleep/day, was associated with the greatest risk of
overweight and obesity, a 3.15-fold higher risk compared to the
persons with healthy lifestyle. Family history of obesity was
associated with a 1.46-fold higher risk of overweight and obesity,
hypercaloric diet with a 1.61-fold higher risk, eating <3
meals/day with a 1.63-fold higher risk, frequent fast-food
consumption with a 1.85-fold higher risk, excessive alcohol
consumption with a 1.53-fold higher risk, sedentary lifestyle with
a 1.79-fold higher risk, depression with a 1.77-fold higher risk,
sleeping <6 h/day with a 1.71-fold higher risk.
 | Table IPrevalence of risk factors for
adiposity according to sex: women/men (432/468). |
Table I
Prevalence of risk factors for
adiposity according to sex: women/men (432/468).
| | % | |
|---|
| General
characteristics | Women | Men | P-value |
|---|
| Family history of
obesity | 35.65 | 30.34 | 0.09 |
| Hypercaloric
nutrition | 41.20 | 45.73 | 0.17 |
| <3 meals/day | 60.19 | 59.62 | 0.86 |
| Frequent fast-food
consumption | 59.49 | 63.68 | 0.83 |
| Excessive alcohol
consumption | 25.93 | 58.55 | <0.01 |
| Sedentary
lifestyle | 61.11 | 44.23 | <0.01 |
| Depression | 35.88 | 27.99 | 0.01 |
| Sleeping time <6
h/day | 48.84 | 39.96 | <0.01 |
| Unhealthy
lifestyle | 65.97 | 68.59 | 0.40 |
| Table IIInfluence of risk factors for
adiposity on the prevalence of overweight and obesity. |
Table II
Influence of risk factors for
adiposity on the prevalence of overweight and obesity.
| | Prevalence | |
|---|
| | | % | |
|---|
| Risk factors and
protective factors | Patients No. | Overweight | Obesity | Overweight +
obesity | Relative increase of
risk for being overweight/obese |
|---|
| Without family
history of obesity | 604 | 25.16 | 18.70 | 43.86 | 1.46 |
| Family history of
obesity | 296 | 38.17 | 26.01 | 64.18 | |
| Normocaloric
diet | 508 | 21.06 | 19.09 | 40.16 | 1.61 |
| Hypercaloric
diet | 392 | 40.56 | 24.23 | 64.80 | |
| 3 meals/day | 361 | 20.78 | 16.07 | 36.84 | 1.63 |
| <3 meals/day | 539 | 35.44 | 24.86 | 60.30 | |
| Without frequent
fast-food consumption | 345 | 20.29 | 13.04 | 33.33 | 1.85 |
| Frequent fast-food
consumption | 555 | 35.32 | 26.49 | 61.80 | |
| Without excessive
alcohol consumption | 514 | 21.40 | 20.04 | 41.44 | 1.53 |
| Excessive alcohol
consumption | 386 | 40.41 | 23.06 | 63.47 | |
| Active lifestyle | 429 | 19.58 | 16.32 | 35.90 | 1.79 |
| Sedentary
lifestyle | 471 | 38.64 | 25.90 | 64.54 | |
| Without
depression | 614 | 21.99 | 18.89 | 40.88 | 1.77 |
| Depression
presence | 286 | 45.80 | 26.57 | 72.38 | |
| Sleep ≥6 h/day | 508 | 21.51 | 17.13 | 38.65 | 1.71 |
| Sleep <6
h/day | 392 | 39.70 | 26.63 | 66.33 | |
| Healthy
lifestyle | 294 | 10.88 | 9.86 | 20.75 | 3.15 |
| Unhealthy
lifestyle | 606 | 38.61 | 26.90 | 65.51 | |
Discussion
In this study, the prevalence of obesity and
overweight was lower compared to the prevalence of obesity and
overweight identified in PREDATORR study (2). Percentarge of 29.56 of the individuals
in our study were overweight while 21.33% were obese. However, when
comparing to the prevalence of obesity worldwide of 13% in 2016
according to WHO (8), it can be
concluded that in Romania according to our study which reports a
prevalence of obesity of 21.33% and to PREDATORR study which
reports a prevalence of 31.90%, the population is significantly
more frequently obese and therefore exposed to a higher risk of
early death. In our study overweight prevalence was statistically
significantly higher in men compared to women, while the prevalence
of obesity was higher in women. Similar observations were confirmed
in the NHANES study (9) were the
prevalence of overweight in the USA population was 38.7% in men and
26.5% in women while the prevalence of obesity was 35% in men and
40.4% in women.
This study revealed that the unhealthy lifestyle was
a composite risk factor for adiposity and was present in 67.33% of
the individuals. It was observed that frequent fast-food
consumption was the most prevalent risk factor for adiposity in our
study being identified in 61.67% of the individuals and also it was
the most important factor that increased the risk for overweight
and obesity 1.85 times. Data from literature is abundant regarding
the association between fast-food consumption and obesity. Research
demonstrated that compared to non-consumers individuals that
consume fast-food products have a risk of obesity increased by
20-129% (10). Consumption of
fast-food products is not only associated with obesity but also
with cardiovascular disease, increasing the prevalence of these
pathologies with 52-162% (10).
Individuals with fast-food consumption also consume a high quantity
of sweetened beverages (11).
Nutrition interventions are effective measures to improve diet
quality (12). One meta-analysis
evaluating 14 studies carried out on college students demonstrated
that nutrition education provided as lectures, web education or
giving informative supplements, significantly improves nutrition
knowledge and dietary practices (13). Obesity and overweight are also
associated with a high oncogenic and/or infections risk. It was
demonstrated that the antioxidants have an important role related
to the mechanistic approach of the metabolic disorders (14,15).
Sedentary lifestyle in our study was associated with a 1.79 higher
risk for being obese or overweight. Studies demonstrate that among
sedentary behaviours TV viewing was strongly associated with
obesity (16). Physical inactivity
is also associated, by reducing energy expenditure and increasing
visceral adiposity, with a high risk of diabetes mellitus type 2
and cardiovascular disease (17).
The association between depression and obesity was observed in many
studies, one study reporting that individuals with depression had a
26% higher risk of being obese (18). However, the relationship is complex
and is not completely understood weather depression causes obesity
or obesity causes depression by generation of inflammatory
biomarkers that disrupt the hypothalamus-pituitary-adrenal axis.
Sleep disturbances are associated with obesity, as demonstrated in
our study, because they disrupt the orexin system being associated
with increased appetite (19). A
study that explored the effects of sleep restriction demonstrated
that it is associated with statistically significant lower levels
of leptin, a hormone that decreases appetite, and higher ghrelin
levels, a hormone that increases appetite (20). Epidemiological evidence from >50
studies demonstrates that short sleep (<6 h/day) is associated
with obesity risk (19). Short sleep
duration is highly prevalent in modern society because longer
working hours, working during the night, longer time needed for
commuting and long hours spent in front of TV (21).
Research regarding risk factors for adiposity is of
maximum importance because overweight or obesity once installed is
extremely difficult to combat. Research demonstrates that diet and
physical effort are efficient for weight loss, but weight-loss
maintenance has a low prevalence, the only effective method for a
long-term weight-loss maintenance is bariatric surgery (22). Therefore, preventive measures
(informative and educative programs, changing of the diet and of
the life-style, politics and legislation) are necessary in order to
decrease the prevalence of overweight and obesity in the general
population. The most worrying aspect is the high prevalence of
overweight and obesity among children, it is considered that 1 in
every 3 children from United States of America is either overweight
or obese (23).
In conclusion, in the present study, which included
900 individuals from Oradea, Romania, the prevalence of overweight
was 29.56%, while the prevalence of obesity was 21.33%. Unhealthy
lifestyle was highly prevalent among the included persons being
reported in 67.33%. Having an unhealthy lifestyle increases the
risk of being overweight or obese by 3.15-fold. Fast-food
consumption was a major contributor to unhealthy lifestyle being
reported in 61.67% of persons.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
At the private medical offices where the data were
collected.
Authors' contributions
ARP, OF, MR, RACA and CMV collected, analysed and
interpreted the patient data regarding BMI determination and
completion of questionnaires. CP, CCD, OB, SB and SN made
substantial contributions to the conception of the work and
interpretation of data; also, they drafted the manuscript and were
major contributors in writing the manuscript. All authors read and
approved the final manuscript to be published. All the authors
agreed to be accountable for all aspects of the work in ensuring
that questions related to the accuracy or integrity of any part of
the work are appropriately investigated and resolved.
Ethics approval and consent to
participate
The research was performed according the WMA
Declaration of Ethics, Helsinki - Medical Research Involving Human
Principles for Subjects. All the subjects signed a written consent
giving their acceptance to participate in the study. The study was
approved by the Ethics Council of the Clinical Emergency Hospital
of Oradea (Oradea, Romania).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kelly T, Yang W, Chen C-S, Reynolds K and
He J: Global burden of obesity in 2005 and projections to 2030. Int
J Obes. 32:1431–1437. 2008.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Popa S, Moţa M, Popa A, Moţa E,
Serafinceanu C, Guja C, Catrinoiu D, Hâncu N, Lichiardopol R, Bala
C, et al: Prevalence of overweight/obesity, abdominal obesity and
metabolic syndrome and atypical cardiometabolic phenotypes in the
adult Romanian population: PREDATORR study. J Endocrinol Invest.
39:1045–1053. 2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Hamulka J, Wadolowska L, Hoffmann M,
Kowalkowska J and Gutkowska K: Effect of an education program on
nutrition knowledge, attitudes toward nutrition, diet quality,
lifestyle, and body composition in Polish teenagers. The ABC of
healthy eating project: Design, protocol, and methodology.
Nutrients. 10(1439)2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Speliotes EK, Willer CJ, Berndt SI, Monda
KL, Thorleifsson G, Jackson AU, Lango Allen H, Lindgren CM, Luan J,
Mägi R, et al: Procardis Consortium: Association analyses of
249,796 individuals reveal 18 new loci associated with body mass
index. Nat Genet. 42:937–948. 2010.PubMed/NCBI View
Article : Google Scholar
|
|
5
|
Wadden TA, Webb VL, Moran CH and Bailer
BA: Lifestyle modification for obesity: New developments in diet,
physical activity, and behavior therapy. Circulation.
125:1157–1170. 2012.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Donnelly JE, Blair SN, Jakicic JM, Manore
MM, Rankin JW and Smith BK: American College of Sports Medicine.
American College of Sports Medicine Position Stand. Appropriate
physical activity intervention strategies for weight loss and
prevention of weight regain for adults. Med Sci Sports Exerc.
41:459–471. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Cercato C and Fonseca FA: Cardiovascular
risk and obesity. Diabetol Metab Syndr. 11(74)2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
WHO: Overweight and obesity. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
Accessed December 6, 2019.
|
|
9
|
Fryar CD, Carroll MD and Ogden CL:
Prevalence of overweight, obesity, and extreme obesity among adults
aged 20 and over: United States, 1960-1962 through 2015-2016.
National Center for Health Statistics Data, Health E-Stats, July
2016. https://www.cdc.gov/nchs/data/hestat/obesity_adult_13_14/obesity_adult_13_14.htm.
Accessed December 6, 2019.
|
|
10
|
Bahadoran Z, Mirmiran P and Azizi F: Fast
food pattern and cardiometabolic disorders: A review of current
studies. Health Promot Perspect. 5:231–240. 2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Popa AR, Vesa CM, Uivarosan D, Jurca CM,
Isvoranu G, Socea B, Stanescu AMA, Iancu MA, Scarneciu I and Zaha
DC: Cross-sectional study regarding the association between
sweetened beverages intake, fast-food products, body mass index,
fasting blood glucose and blood pressure in the young adults from
North-western Romania. Rev Chim-Bucharest. 70:156–160. 2019.
|
|
12
|
Popa AR, Bungau S, Vesa CM, Bondar AC,
Pantis C, Maghiar O, Dimulescu (Nica) IA, Nistor Cseppento DC and
Rus M: Evaluating the efficacy of the treatment with benfotiamine
and alpha-lipoic acid in distal symmetric painful diabetic
polyneuropathy. Rev Chim. 70:3108–3114. 2019.
|
|
13
|
Lua PL and Wan Putri Elena WD: The impact
of nutrition education interventions on the dietary habits of
college students in developed nations: A brief review. Malays J Med
Sci. 19:4–14. 2012.PubMed/NCBI
|
|
14
|
Abdel-Daim MM, El-Tawil OS, Bungau SG and
Atanasov AG: Applications of antioxidants in metabolic disorders
and degenerative diseases: Mechanistic approach. Oxid Med Cell
Longev. 2019(4179676)2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Glevitzky I, Dumitrel GA, Glevitzky M,
Pasca B, Otrisal P, Bungau S, Cioca G, Pantis C and Popa M:
Statistical analysis of the relationship between antioxidant
activity and the structure of flavonoid compounds. Rev
Chim-Bucharest. 70:3103–3107. 2019.
|
|
16
|
Heinonen I, Helajärvi H and Pahkala K:
Sedentary behaviours and obesity: in adults: the cardiovascular
risk in young Finns study. BMJ Open. (3e002901)2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
González K, Fuentes J and Márquez JL:
Physical inactivity, sedentary behavior and chronic diseases.
Korean J Fam Med. 38:111–115. 2017.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Mulugeta A, Zhou A, Power C and Hyppönen
E: Obesity and depressive symptoms in mid-life: A population-based
cohort study. BMC Psychiatry. 18(297)2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Beccuti G and Pannain S: Sleep and
obesity. Curr Opin Clin Nutr Metab Care. 14:402–412.
2011.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Spiegel K, Tasali E, Penev P and Van
Cauter E: Brief communication: Sleep curtailment in healthy young
men is associated with decreased leptin levels, elevated ghrelin
levels, and increased hunger and appetite. Ann Intern Med.
141:846–850. 2004.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Chaput JP, Després JP, Bouchard C and
Tremblay A: The association between sleep duration and weight gain
in adults: A 6-year prospective study from the Quebec Family Study.
Sleep. 31:517–523. 2008.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Lagerros YT and Rössner S: Obesity
management: What brings success? Therap Adv Gastroenterol. 6:77–88.
2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Kumar S and Kelly AS: Review of childhood
obesity: From epidemiology, etiology, and comorbidities to clinical
assessment and Treatment. Mayo Clin Proc. 92:251–265.
2017.PubMed/NCBI View Article : Google Scholar
|