Introduction
A true or pseudo ventricular aneurysm is the worst
complication of transmural myocardial infarction (1). Left ventricular aneurysm after
myocardial infarction is rare and usually occurs during the first
week following the cardiac event but certain patients may present
after a significant time following the cardiac event(s) (2). Interventricular septal perforation is
also an infrequent but severe problem following myocardial
infarction (3). Rapid diagnosis,
immediate evaluation and management are required to prevent
clinical destruction due to myocardial infarction (1). It is important to measure pulmonary
hypertension in patients after myocardial infarction with possible
septal defects (4). Several invasive
and non-invasive imaging modalities are available to rule out this
clinical entity.
Transthoracic echocardiography and right heart
catheterization have been routinely performed in numerous medical
centers worldwide. Right heart catheterization (floating pulmonary
artery catheterization) is the ‘gold standard’ in the diagnosis of
septal perforation but it is an invasive technique and generally
performed when echocardiography is not accessible (4). The International Society for Heart
& Lung Transplantation guidelines (4) consider right heart catheterization as
the most important diagnostic modality, as for critical patients
with acute myocardial infarction and ventricular septal
perforation, right heart catheterization is essential for
evaluating pulmonary capillary wedge pressure, which cannot be
accurately assessed by transthoracic echocardiography due to the
septal perforation. Transthoracic echocardiography is a rapid,
sensitive and non-invasive technique for diagnosing ventricular
septal perforation (5) and may
replace invasive pressure measurements. Transthoracic
echocardiography may strengthen the diagnostic accuracy of right
heart catheterization (6). Left
ventricular angiography is generally used for diagnosing left
ventricular aneurysm (1) but also
has a procedural risk for the patient (7).
The objective of the present study was to compare
radiological and hemodynamic diagnostic parameters of non-invasive
methods with right heart catheterization in patients with suspected
ventricular aneurysm and interventricular septal perforation after
acute myocardial infarction.
Materials and methods
Study population
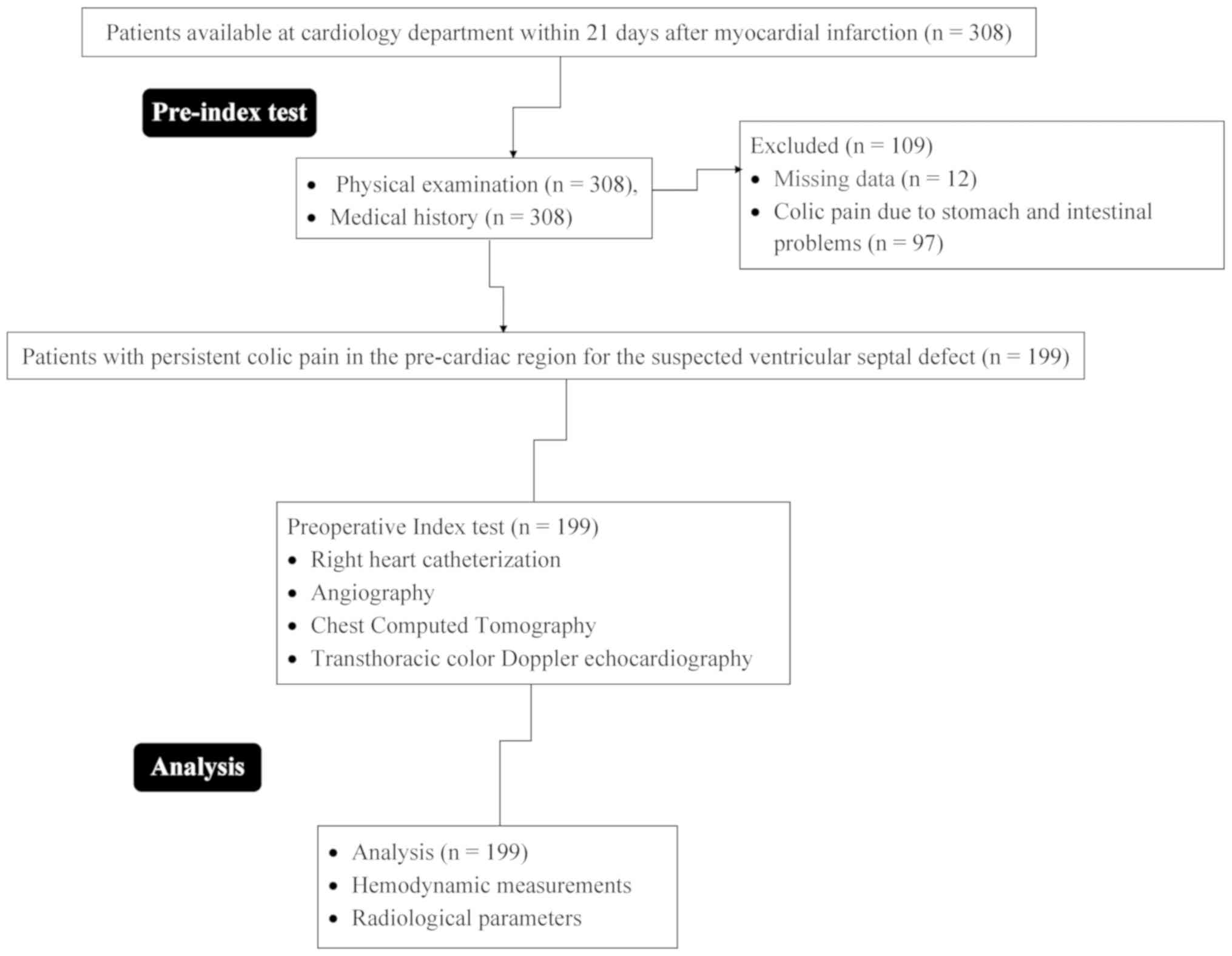
From 16 February 2016 to 3 March 2019, a total of
308 patients (aged ≥18 years) were admitted to the Department of
Cardiology of Zhejiang Province People's Hospital, People's
Hospital of Hangzhou Medical College (Hangzhou, China) and the
referring hospitals within 21 days after myocardial infarction.
Among them, 97 patients had no suspected ventricular aneurysm with
interventricular septal perforation (colic pain only due to stomach
and intestinal problems) and for another 12 patients, the complete
data were not available. Therefore, data of these patients were
excluded from the analysis. Data of demographic parameters,
clinical characteristics, right heart catheterization parameters,
as well as echocardiography and angiographic parameters of the
remaining 199 patients with suspected ventricular septal defect due
to persistent colic pain in the pre-cardiac region were included in
the analysis. The flow diagram of the patients is presented in
Fig. 1.
Data collection
Patient data regarding demographic and clinical
characteristics, physical examination, right heart catheterization,
echocardiography, chest CT, electrocardiogram, angiography and
hemodynamic parameters were obtained from their medical records.
The medical staff (the authors of the current study) of the
institutes was involved in the collection of the data.
Right heart catheterization
Right heart catheterization was performed using
proximal venous access via femoral, subclavian or internal jugular
veins (8) by intensive care
physicians (minimum of 3 years experience) of the institutes using
a continuous pressure monitoring device (CARESCAPE™ V100 Monitor;
GE Healthcare). Device selection, use of ‘off-label’ devices and
multiple implantations were performed by the intensive care
physicians themselves. The catheter was positioned in the pulmonary
artery and the right heart cavity. The transducer was calibrated in
the middle of the chest. The electrical and hemodynamic signals
were digitally recorded. Pulmonary vascular resistance was recorded
as per equation (Eq.) i (9). The
cut-off values for pre- and post-capillary pulmonary hypertension
were selected as ≥25 and ≤15 mmHg, respectively (10).
Equations
The equations used were as follows: (i) Pulmonary
vascular resistance=Mean pulmonary artery pressures-pulmonary
capillary wedge pressure/Cardiac output; (ii) Right atrial
pressure=0.8+1.7 (Early tricuspid Doppler inflow wave peak
velocity/Doppler tissue imaging of early tricuspid annuli peak
velocity); (iii) Systolic pulmonary artery pressure=4*(Tricuspid
regurgitation velocity)/2+Right arterial pressure; (iv) Mean
pulmonary artery pressure=(0.61 x systolic pulmonary artery
pressure)+2; (v) Cardiac output=Π(Left ventricle outflow
tract2/4)*time integral of left ventricle outflow tract
velocity*heart rate; (vi) Pulmonary capillary wedge
pressure=1.24(Early mitral Doppler inflow wave peak
velocity/Doppler tissue imaging of early mitral annuli peak
velocity)+1.9; (vii) Pulmonary vascular resistance=Systolic
pulmonary artery pressure/Time integral of the right ventricular
outflow tract velocity.
Angiography
All patients were subjected to cardiac
catheterization for coronary angiography and left ventricular
angiography (7) by cardiologists
(minimum 3 years experience; blinded regarding results of right
heart catheterization) of the institutes. The culprit vessels were
evaluated as per thrombolysis in myocardial infarction (TIMI).
Transthoracic color Doppler
echocardiography
Color Doppler transthoracic echocardiography was
consecutively performed after right heart catheterization and
angiography in all enrolled patients under the same conditions
using an on-platform ultrasound system (MYLAB™X7; Esaote S.p.A.)
and 3-MHz transducer at a speed of 100 mm/sec (11) by sonographers (minimum 3 years
experience; blinded regarding the results of angiography and right
heart catheterization) of the institutes. The right atrial pressure
was measured as per Eq. 2(12).
Systolic pulmonary artery pressure was calculated as per Eq.
3(11). Mean pulmonary artery
pressures were calculated as per Eq. 4(9). Cardiac output was calculated as per Eq.
5(11). Pulmonary capillary wedge
pressure was calculated as per Eq. 6(9). The pulmonary vascular resistance was
calculated as per Eq. 7(13).
Statistical analysis
The statistical analysis was performed using SPSS
version 25 (IBM Corp.). The χ2 test of independence was
used for comparison of categorical data and a Wilcoxon rank-sum
test was used for continuous data. The confidence level of
significance was set at 95% with P<0.05 considered to indicate
statistical significance.
Results
Demographic parameters and clinical
characteristics
The mean age of the patients was 62.58±7.58 years
and the cohort included 77 (39%) female patients. Patients
presented with one or the other type of cardiovascular
co-morbidity. All patients received standard medical treatment for
acute myocardial infarction. Percutaneous coronary
revascularization was performed in 121 (61%) patients and was not
performed in 78 (39%) patients. The time of intra-aortic
counterpulsation after myocardial infarction was 6±1 days. The
other demographic parameters and clinical conditions of the
patients are presented in Table
I.
 | Table IMedical history of the patients
enrolled (n=199). |
Table I
Medical history of the patients
enrolled (n=199).
| Characteristics | Value |
|---|
| Systolic blood
pressure (mmHg) | 98.12±7.15 |
| Systolic pulmonary
arterial pressure (mmHg) | 42.65±9.11 |
| Intra-aortic
counterpulsation after myocardial infarction (days) | |
|
Minimum | 2 |
|
Maximum | 20 |
|
Mean | 6±1 |
| Left ventricular
ejection fraction (%) | 45.12±8.47 |
| Site of acute
myocardial infarction | |
|
Inferior | 97(48) |
|
Inferior-posterior | 25(13) |
|
Anteroseptal | 77(39) |
| Surgical
pre-procedural data | |
|
Surgical
closure | 128(64) |
|
Percutaneous
closure | 71(36) |
| Co-morbidities | |
|
Diabetes | 71(36) |
|
Smoking | 25(13) |
|
Alcohol
dependence | 12(6) |
|
Hypercholesterolemia | 61(31) |
|
Mean | 2.51±0.15 |
| Cardiac function
typea | |
|
I | 2(1) |
|
II | 53(27) |
|
III | 110(55) |
|
IV | 34(17) |
| Diabetic ketosis | 55(28) |
| Pulmonary
infection | 15(8) |
| Present
treatment(s)b | |
|
Aspirin | 115(58) |
|
Atorvastatin | 65(33) |
|
Frusemide | 35(18) |
|
Spironolactone | 62(31) |
|
Bisoprolol | 72(36) |
|
Clopidogrel | 82(41) |
| Percutaneous coronary
revascularization performed | 121(61) |
| Percutaneous coronary
revascularization not performed | 78(39) |
Physical examination
The patients had a mean body mass index of
24.95±3.11 kg/m2, no cyanosis, no jugular vein
enlargement, no thyroid enlargement and no yellow stain on the skin
sclera. The heart was not enlarged, the heart rhythm was uniform
and the fourth intercostal space on the left edge had a systolic
murmur. The lungs were clear, and no dry and wet voices were heard.
The abdomen was soft and no tenderness or rebound tenderness was
present. The liver and spleen under the ribs had no tenderness.
There were two patients with edema in both lower limbs The other
results of the physical examination are presented in Table II.
| Table IIPhysical examination results in the
cohort (n=199). |
Table II
Physical examination results in the
cohort (n=199).
| Characteristics | Results |
|---|
| Age (years) | |
|
Range | 53-79 |
|
Mean | 62.58±7.58 |
| Sex | |
|
Female | 77(39) |
|
Male | 122(61) |
| Ethnicity | |
|
Han
Chinese | 186(93) |
|
Mongolian | 11(6) |
|
Tibetan | 2(1) |
| Body mass index
(kg/m2) | 24.95±3.11 |
| Adverse events | |
|
Nausea | 8(4) |
|
Vomiting | 2(1) |
|
Chill | 1(1) |
|
Fever | 2(1) |
|
Cough | 3(1) |
| History of
disease | |
|
Heart | 1(1) |
|
Liver
(excludes hepatitis) | 1(1) |
|
Kidney | 2(1) |
|
Hepatitis | 2(1) |
|
Tuberculosis | 2(1) |
|
Thyroid | 2(1) |
| Edema in both lower
limbs | 2(1) |
Angiography
Coronary angiography identified 149 (75%) patients
with single-vessel disease, 42 (21%) patients with two-vessel
disease and 8 (4%) patients with the triple-vessel disease (data
not shown). The right coronary artery was blocked in 99 (50%)
patients, the left anterior descending artery was blocked in 83
(42%) and the circumflex artery was blocked in 17 patients (3%;
Fig. 2). Left ventricular
angiography revealed abnormal wall motion and ventricular aneurysm.
None of the patients had intravenous spontaneous thrombolysis
(Fig. 3).
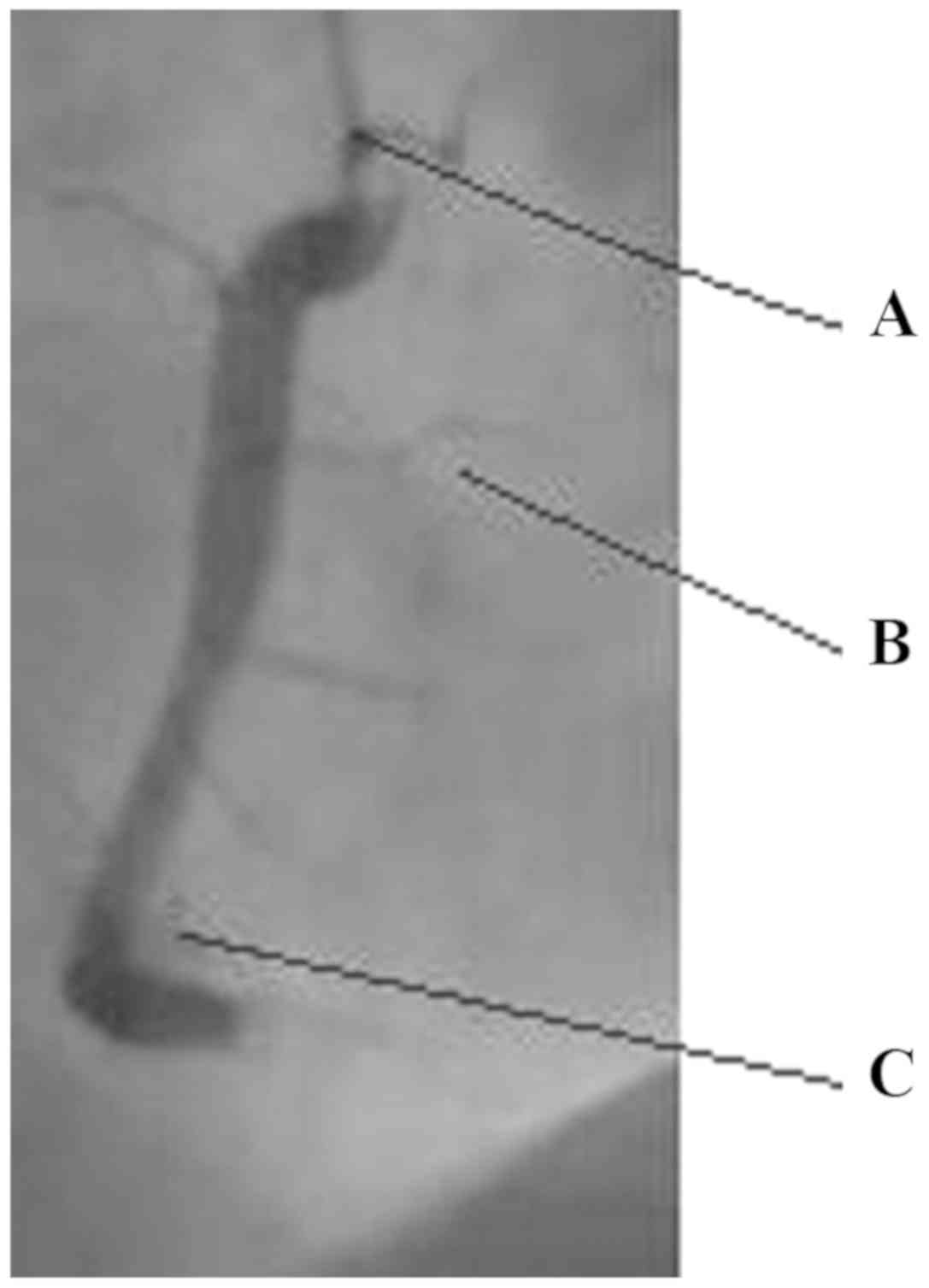 | Figure 2Coronary angiography image of a
representative patient aged 70 years (body weight, 70 kg; body
height, 162 cm; sex, male.) of the right coronary dominant type.
The left major trunk exhibited no obvious stenosis. The anterior
descending branch had 99% stenosis in the proximal segment and
70-80% stenosis in the middle segment with a TIMI blood flow grade
3. The circumflex branch had 40-50% stenosis near the middle
segment and a TIMI blood flow grade 3. The right coronary artery
had 40-50% stenosis in the proximal segment, 30-40% stenosis in the
middle segment and 40% stenosis in the distal segment with a TIMI
blood flow grade 3. A, coronary artery, B, ventricular margin in
anterior descending branch, C, septum in anterior descending
branch. TIMI, thrombolysis in myocardial infarction. |
Chest CT
In most of the patients, the chest CT revealed
inflammation of the bilateral lungs, bilateral pleural effusion
with segmental lung tissue insufficiency and pulmonary
emphysema.
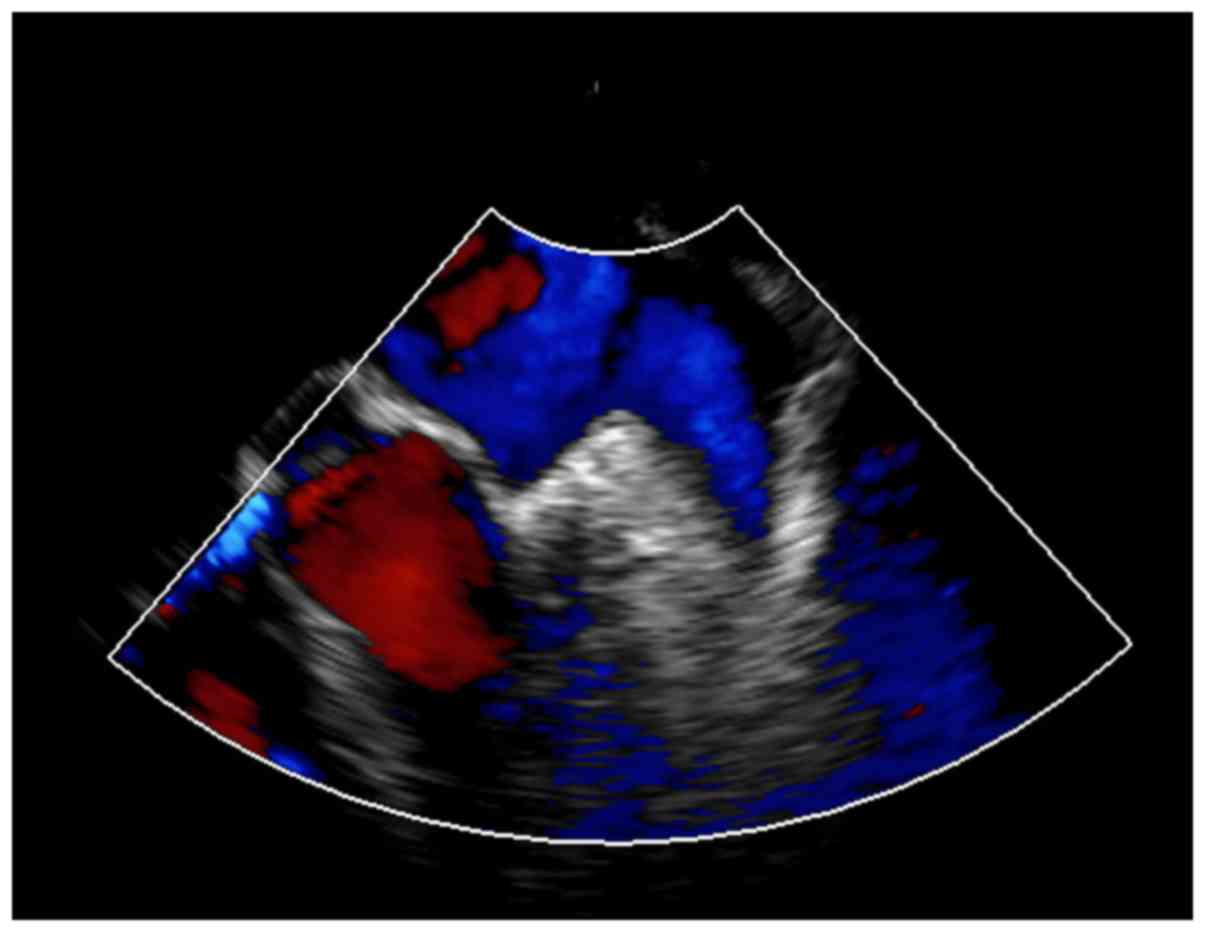
Transthoracic color Doppler
echocardiography
Apical ventricular aneurysm formation with
interventricular septum perforation, left ventricular wall
segmental motor abnormalities (widening anterior wall motion
weakened), aortic sclerosis, ascending aorta widening, mild mitral
regurgitation, moderate tricuspid regurgitation, moderate pulmonary
hypertension, left ventricular systolic and diastolic dysfunction
were observed on transthoracic color Doppler echocardiography in
all patients (see representative image in Fig. 4).
Cervical vascular ultrasound
Bilateral carotid atherosclerosis with multiple
plaque formation, moderate left stenosis of the left common carotid
artery, right carotid sinus and internal carotid artery with severe
or moderate stenosis were observed on cervical vascular ultrasound
in certain patients (10 patients).
Electrocardiogram
The majority of patients had a sinus rhythm in line
with acute extensive anterior wall and inferior myocardial
infarction on the electrocardiogram. In addition, left chest lead,
limb lead QRS complex low voltage and QTc interval prolongation
were observed.
Hemodynamic measurements
All hemodynamic parameters exhibited significant
differences between right heart catheterization and transthoracic
color Doppler echocardiography (P<0.05 for all) except heart
rate (P=0.492). Transthoracic color Doppler echocardiography
underestimated post-capillary pulmonary hypertension (Table III).
| Table IIIHemodynamic measurements by right
heart catheterization and transthoracic color Doppler
echocardiography in the cohort (n=199). |
Table III
Hemodynamic measurements by right
heart catheterization and transthoracic color Doppler
echocardiography in the cohort (n=199).
| Hemodynamic
characteristics | Right heart
catheterization |
Echocardiography | P-value |
|---|
| Heart rate (beats
per minute) | 74±14 | 75±15 | 0.492 |
| Oxygen saturation
(%) | 92±4 | 91±5 | 0.028 |
| Mean blood pressure
(mmHg) | 96±2 | 95±1 | <0.0001 |
| Right atrial
pressure (mmHg) | 8±2 | 7±2 | <0.0001 |
| Systolic pulmonary
artery pressure (mmHg) | 61±2 | 59±3 | <0.0001 |
| Mean pulmonary
artery pressure (mmHg) | 39±2 | 34±3 | <0.0001 |
| Cardiac output
(l/min) | 6.15±0.21 | 5.85±0.15 | <0.0001 |
| Pulmonary capillary
wedge pressure (mmHg) | 14±1 | 11±2 | <0.0001 |
| Pulmonary vascular
resistance (Wood units) | 4.85±0.25 | 3.72±0.18 | <0.0001 |
Procedural complications
Overall, there was no procedural complication
requiring emergent intervention, major complications or any
condition resulting in death due to diagnostic modalities.
Echocardiography exhibited less complications than catheterization
(and angiography; Table IV).
| Table IVProcedural complications in the
patients (n=199). |
Table IV
Procedural complications in the
patients (n=199).
| Hemodynamic
characteristics | Right heart
catheterization |
Echocardiography | Angiography | P-value |
|---|
| Carotid artery
puncture | 5(3) | 0 (0) | 0 (0) | 0.007 |
| Hematoma | 3(1) | 0 (0) | 2(1) | 0.244 |
| Coagulopathy | 2(1) | 0 (0) | 0 (0) | 0.134 |
| Infections | 0 (0) | 0 (0) | 1(1) | 0.367 |
| Respiratory
insufficiency | 0 (0) | 0 (0) | 2(1) | 0.134 |
Discussion
Right heart catheterization and transthoracic color
Doppler echocardiography may provide hemodynamic parameters for
patients with ventricular septal defect following myocardial
infarction. In the present study, coronary and left ventricular
angiography, physical examinations, chest CT and electrocardiogram
did not provide sufficient information for hemodynamic parameters.
Central hemodynamic parameters are important for the diagnosis,
classification (mean pulmonary artery pressure and pulmonary
capillary wedge pressure) and prognosis (the right atrial pressure)
of the ventricular aneurysm with interventricular septal
perforation (9). The present study
recommended either right heart catheterization or transthoracic
color Doppler echocardiography as examinations to provide
pre-operative indexes in patients with suspected ventricular
aneurysm with interventricular septal perforation after acute
myocardial infarction.
Angiography provides information on the degree of
stenosis and culprit vessel(s). Cervical vascular ultrasound may
also provide information on atherosclerosis. Three-dimensional
imaging modalities may reveal acute mechanical complications of
myocardial infarction (5). Chest CT
is effective in detecting pseudo-aneurysms, abscesses and
vegetation (14). Angiography,
cervical vascular ultrasound and chest CT are an essential adjunct
method to transthoracic color Doppler echocardiography or right
heart catheterization for the diagnosis of interventricular septal
defect.
Although a clear assessment of each patient is
important for predicting the prognosis, in the present analysis,
the right atrial pressure was underestimated by transthoracic color
Doppler echocardiography compared with right heart catheterization
(P<0.0001). The right atrial pressure is a component of the
calculation of the systolic pulmonary artery pressure (11) and mean pulmonary artery pressure
(9). Therefore, it is obvious that
they were also underestimated by echocardiography (P<0.0001 for
both) compared to right heart catheterization. The results of the
present study were consistent with those of two prospective studies
(9,15), but results of the right atrial
pressure were not consistent with those of a retrospective
investigation (16) and another
prospective study (17).
Transthoracic color Doppler echocardiography is routinely used for
measurement of the right atrial pressure; the determination of the
right atrial pressure is helpful for the prognosis of the
ventricular aneurysm and interventricular septal perforation after
acute myocardial infarction but not useful for the diagnosis of
pulmonary hypertension (18).
However, the systolic pulmonary artery pressure is the only
parameter that is useful for the diagnosis of pulmonary
hypertension (10) and the
recommended equation for the mean pulmonary artery pressure was
used for calculation (9). Inaccuracy
is always a problem in the determination of the right atrial
pressure by color Doppler echocardiography (17). Doppler echocardiography is frequently
inaccurate in the estimation of pulmonary artery pressure.
Significant differences between the pulmonary
capillary wedge pressure determined by right heart catheterization
technique and that obtained by transthoracic color Doppler
echocardiography modality were obtained in the present study
(P<0.0001). The pulmonary capillary wedge pressure is a strong
and accurate measure of left atrial pressure (19). For hemodynamic parameters/pulmonary
capillary wedge pressure, transthoracic color Doppler
echocardiography has a lower predictive value than right heart
catheterization (20). The results
of the present study were consistent with those of prospective
studies (9,13). It may be concluded that right heart
catheterization is essential for the diagnosis of pulmonary
capillary wedge pressure.
Of note, the present study had various limitations.
For instance, the analysis was retrospective. The patients were in
treatment when the diagnosis was performed. However,
treatment-naïve patients should be used to obtain meaningful
results. Invasive and non-invasive methods were performed
simultaneously but the simultaneous measurements of transthoracic
color Doppler echocardiography may have been inaccurate due to the
suboptimal status of the patients (13). The measurements did not reflect the
baseline status of the patients. A delay by 24 h between invasive
and non-invasive methods is acceptable (21) but a delay of >1 day was observed
between both in a few cases. Correct alignment of the ultrasound
beam is crucial for accurate measurements by echocardiography
(13). It was not possible to
maintain correct alignment of the ultrasound beam for patients in a
few cases.
In conclusion, the prediction of the right heart
anatomy and physiology by different imaging modalities is crucial
besides right heart catheterization in patients with suspected
ventricular aneurism with interventricular septum perforation after
acute myocardial infarction. Transthoracic color Doppler
echocardiography provided information for radiological measurements
but underestimated hemodynamic measurements. Further research is
required to validate the results of transthoracic color Doppler
echocardiography for the evaluation of pulmonary hypertension.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
All authors read and approved the manuscript for
publication. JW contributed to project administration,
conceptualization, software and literature review for the study. MY
contributed to the formal analysis, validation, resources and
literature review of the study. YC contributed to data curation,
investigation, resources and literature review. LC contributed to
the formal analysis, data curation, resources and literature
review. SH contributed to formal analysis and literature review, as
well as drafting, review and editing of the manuscript for
intellectual content. The authors agree to be accountable for all
aspects of the work, ensuring integrity and accuracy.
Ethics approval and consent to
participate
The protocol (no. ZPP/CL/15/2019 dated 4 March 2019)
was approved by the review board of People's Hospital of Hangzhou
Medical College. An informed consent form was signed by all
enrolled patents regarding pathology, anesthesia, radiology and to
have an additional procedure(s) purely for research purpose(s)
during hospitalization. The study reporting adheres to the
STrengthening the Reporting of Observational Studies in
Epidemiology statement: A cross-sectional study, the law of China
and the Declaration of Helsinki (v. 2008).
Patient consent for publication
An informed consent form was signed by all enrolled
patents regarding publication of the study, including personal data
and images in all forms of citable materials irrespective of time
and language during hospitalization.
Competing interests
Authors declare that they have no competing
interests.
References
|
1
|
Marzlin KM: Ventricular aneurysm:
Diagnosis and treatment. AACN Adv Crit Care. 28:391–394.
2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Belkhadir M, MoutakiAllah Y, Raissouni Z,
Abdou A, Bamous M, Nya F, Atmani N, Houssa MA, El Bekkali Y and
Boulahya A: Left ventricular aneurysm and interventricular
communication complicating myocardial infarction. Pan Afr Med J
(French). 17(321)2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Cho JH, Sattiraju S, Mehta S and Missov E:
Delayed ventricular septal rupture complicating acute inferior wall
myocardial infarction. BMC Res Notes. 6(124)2013.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Kaluzna-Oleksy M, Araszkiewicz A, Migaj J,
Lesiak M and Straburzyńska-Migaj E: ‘From right to left’: The role
of right heart catheterization in the diagnosis and management of
left heart diseases. Adv Clin Exp Med. 26:135–141. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Hakuno D, Isobe S, Masaki N and Adachi T:
Right ventricular wall dissection with ventricular septal rupture
following myocardial infarction visualized on 3-dimensional
transthoracic echocardiography. Circ J. 79:2072–2074.
2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Nagueh SF, Smiseth OA, Dokainish H,
Andersen OS, Abudiab MM, Schutt RC, Kumar A, Gude E, Sato K, Harb
SC and Klein AL: Mean right atrial pressure for estimation of left
ventricular filling pressure in patients with normal left
ventricular ejection fraction: Invasive and noninvasive validation.
J Am Soc Echocardiogr. 31:799–806. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Trivedi KR, Aldebert P, Riberi A, Mancini
J, Levy G, Macia JC, Quilicci J, Habib G and Fraisse A: Sequential
management of post-myocardial infarction ventricular septal
defects. Arch Cardiovasc Dis. 108:321–330. 2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Shah S, Boyd G, Pyne CT, Bilazarian SD,
Piemonte TC, Jeon C and Waxman S: Right heart catheterization using
antecubital venous access: Feasibility, safety and adoption rate in
a tertiary center. Catheter Cardiovasc Interv. 84:70–74.
2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Doutreleau S, Canuet M, Enache I, Di Marco
P, Lonsdorfer E, Oswald-Mammoser M and Charloux A: Right heart
hemodynamics in pulmonary hypertension-An echocardiography and
catheterization study. Circ J. 80:2019–2025. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Galie N, Hoeper MM, Humbert M, Torbicki A,
Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS,
et al: Guidelines for the diagnosis and treatment of pulmonary
hypertension: The task force for the diagnosis and treatment of
pulmonary hypertension of the European Society of Cardiology (ESC)
and the European Respiratory Society (ERS), endorsed by the
International Society of Heart and Lung Transplantation (ISHLT).
Eur Heart J. 30:2493–2537. 2009.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Rudski LG, Lai WW, Afilalo J, Hua L,
Handschumacher MD, Chandrasekaran K, Solomon SD, Louie EK and
Schiller NB: Guidelines for the echocardiographic assessment of the
right heart in adults: A report from the American Society of
Echocardiography endorsed by the European Association of
Echocardiography, a registered branch of the European Society of
Cardiology, and the Canadian Society of Echocardiography. J Am Soc
Echocardiogr. 23:685–713. 2010.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Beigel R, Cercek B, Luo H and Siegel RJ:
Noninvasive evaluation of right atrial pressure. J Am Soc
Echocardiogr. 26:1033–1042. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kouzu H, Nakatani S, Kyotani S, Kanzaki H,
Nakanishi N and Kitakaze M: Noninvasive estimation of pulmonary
vascular resistance by Doppler echocardiography in patients with
pulmonary arterial hypertension. Am J Cardiol. 103:872–876.
2009.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Nand N, Singla SK and Magu S: Cardiac
abscess with ventricular aneurysm secondary to old myocardial
infarction. J Assoc Physicians India. 65:95–96. 2017.PubMed/NCBI
|
|
15
|
Fisher MR, Forfia PR, Chamera E,
Housten-Harris T, Champion HC, Girgis RE, Corretti MC and Hassoun
PM: Accuracy of Doppler echocardiography in the hemodynamic
assessment of pulmonary hypertension. Am J Respir Crit Care Med.
179:615–1621. 2009.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kasai H, Matsumura A, Sugiura T, Shigeta
A, Tanabe N, Yamamoto K, Miwa H, Ema R, Sakao S and Tatsumi K: Mean
pulmonary artery pressure using echocardiography in chronic
thromboembolic pulmonary hypertension. Circ J. 80:1259–1264.
2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Aduen JF, Castello R, Daniels JT, Diaz JA,
Safford RE, Heckman MG, Crook JE and Burger CD: Accuracy and
precision of three echocardiographic methods for estimating mean
pulmonary artery pressure. Chest. 139:347–352. 2011.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Saggar R and Sitbon O: Hemodynamics in
pulmonary arterial hypertension: Current and future perspectives.
Am J Cardiol. 110 (Suppl):9S–15S. 2012.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Nagy AI, Venkateshvaran A, Dash PK,
Barooah B, Merkely B, Winter R and Manouras A: The pulmonary
capillary wedge pressure accurately reflects both normal and
elevated left atrial pressure. Am Heart J. 167:876–883.
2014.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Hoeper MM, Bogaard HJ, Condliffe R, Frantz
R, Khanna D, Kurzyna M, Langleben D, Manes A, Satoh T, Torres F, et
al: Definitions and diagnosis of pulmonary hypertension. J Am Coll
Cardiol. 62:D42–D50. 2013.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Vlahos AP, Feinstein JA, Schiller NB and
Silverman NH: Extension of Doppler-derived echocardiographic
measures of pulmonary vascular resistance to patients with moderate
or severe pulmonary vascular disease. J Am Soc Echocardiogr.
21:711–714. 2008.PubMed/NCBI View Article : Google Scholar
|