Introduction
The working environment of industries in the
construction branch, both in underground and in outdoor activities,
is by its nature burdened with particulate dust (1,2). This
dust, either inert or with inherent toxic properties, along with
other chemicals that exist in the working environments, constitute
a threat to the health and safety of workers, since chronic
exposure can lead to serious respiratory diseases and even systemic
disorders (3-5). In
particular, when the dust contains free crystalline silicon dioxide
(silica, SiO2) special measures and precautions are
required since once inhaled, the dust ceases to be inert and can
cause chronic lung diseases such as silicosis, chronic obstructive
pulmonary disease (COPD; emphysema) and lung cancer (1,2,6).
Silicon dioxide is the second most abundant element
(following oxygen) in the earth's crust, is a group IV metal oxide
that occurs in nature in three 3 forms: crystalline,
microcrystalline (or cryptocrystalline) and amorphous
(non-crystalline) (7). The term
‘crystalline’ that is commonly used refers to the orientation of
silicon molecules (SiO2) in a fixed configuration
against a non-periodic, random molecular arrangement, designated as
amorphous. The three most common crystalline forms (3 main
polymorphs) of silicon that occur in the working environment are
quartz, cristobalite and tridymite (2,8,9). Quartz is the second most common mineral
in the world (8).
Inhalation of respirable crystalline silica (RCS)
can lead to serious health effects, such as silicosis, COPD,
tuberculosis and lung cancer (10-14).
Respiratory diseases often occur in construction workers operating
in underground excavation and tunneling constructions (15-17),
as well as in outdoor ones (18).
Studies have shown that the potential exposure of construction
workers to RCS exceeds that of 3 million in the European Union, 1.7
million in the US and 350,000 in Canada (6).
Silicosis is a type of pneumoconiosis caused by
exposure of workers to inhaled crystalline silica powder (19). Crystalline silicon dioxide, in the
form of quartz powder or ‘cristobalite’ and tridymite, is
responsible for causing silicosis that is categorized as an
occupational disease (10,11). It is characterized by the appearance
of pulmonary fibrosis and silica nodules. The development -
progression of the disease continues even after the interruption of
the exposure (15,16). There are 3 forms of the disease:
Chronic, acute and lightning stroke. The latter occurs after
massive exposure to silica dust. It presents with shortness of
breath, fever, cough and weight loss and soon progresses to
respiratory failure not responding to corticosteroids (20,21).
Cancer is the first cause of work-related deaths in
the EU (9). The International Cancer
Research Organization (IARC) stated in its 100C monograph that
‘silica or inhalation of quartz or cristobalite powder is
carcinogenic to humans (Group 1 of carcinogens for humans)’
(15,17,22).
The European Union Scientific Committee on
Occupational Exposure Limits (SCOEL) has assessed the impact of
crystalline silica (respiratory dust) on employee health, and has
proposed a limit value of 0.1 mg/m3 which would mean
avoiding 99,000 cancer cases by 2069 with total health benefits
valued at between 34 billion and 89 billion euros (9). The above proposal by SCOEL has led to
the adoption of the European Union Directive 2017/2398 L 345/87
that aims at improving the prevention of occupational cancer cases
that can be avoided (9).
Given the nature of the materials used in the
construction industry, the powder may contain significant amounts
of SiO2 (1,18,23).
According to the International Labor Organization (ILO), silicosis,
an incurable disease, requires quantitative and qualitative control
of respiratory crystalline silica and the development of
appropriate control measures (24).
The importance of the current study is based on the
fact that we need to take under consideration the high occupational
exposure to airborne powders of people working at underground and
outdoor construction, drilling, concrete launching and machinery
movement together with the absence of relevant studies in Greece.
The purpose of the study herein was to evaluate the exposure of
workers to respiratory crystalline silica (SiO2) and
examine the condition of workers' pulmonary function.
Materials and methods
Patients
The study involved 59 employees from one
construction company mainly engaged in outdoor construction and 27
employees from a second construction company working exclusively at
underground projects with their main activity being tunneling. A
total of 86 employees participated all of whom, suffered from
active exposure to inhalable crystalline silicon dioxide. The
construction workers who participated were categorized as artisans
- builders, machine operators, builders - contractors, blasters,
electricians, sorting and packaging workers. The
clinical/epidemiological history included both the medical and the
professional one, in order to determine the relationship between
exposure to a substance and the development of respiratory disease.
The relevant information included the aggravating factors, the
appearance and progression of the disease, the family and medical
history of each exposed worker. Other medical allergic or
respiratory disorders in childhood were also reported in the
medical history together with the smoking habits of each
participant (25). Certain
characteristics (height, weight, age, years of work) of the exposed
workers were recorded.
Environmental measurements
In the present study samplings took place during the
year of 2015. To test for dust at the workplace (solid particles or
mixtures suspended in the air), environmental measurements -
samplings were performed to ensure compliance with national and
European legislation on industrial hygiene. In the above
measurements, the sampling time corresponded to at least 4 hours
and the analysis technique for determining the content of
SiO2 (mainly quartz and cristobalite) was carried out by
various methods such as X-ray diffraction (XRD), NMAM 7500 method,
or by infrared spectroscopy via Fourier (Fourier Transform Infrared
Spectroscopy) NIOSH 7602, or by visible VIS spectroscopy with the
NIOSH 7601 method (1,25). According to the National legislation
for the protection of workers from natural, chemical and biological
factors, when there is a group of workers who perform the same or
similar tasks in the same place and under the same conditions, in a
way that they can reasonably be considered to be subjected to
approximately the same degree of exposure to this particular
chemical agent, in that case the testing may take place in groups
and in a way that gives representative results. In our work, an
individual testing was performed on 1 for every 10 employees in the
same job. In particular, individual sampling was performed on 3
employees in a total of 27 in the underground construction projects
where the sampling equipment was placed (26). We followed the method of Fourier
transform infrared spectroscopy (FTIR) that uses 3 sampling filters
in underground projects in order to calculate the individual
exposure of respiratory SiO2 in workers. A breathing
zone was considered as an imaginary hemisphere with a radius of 30
cm extending in front of the employee's face and centered on the
middle of the imaginary line connecting his ears. Sampling was
performed on workers in workplaces with high exposure to dust and
on sprayed concrete operators, builders, machine operators,
engineers, blasters and material sorters. The sampling time was 8 h
for each sample taken. During the period of the environmental tests
and of the individual sampling from underground workers at all
jobs, a high accumulation of dust was recorded because of the use
of GUNITE spray concrete. This concrete contains chemical agents
such as sodium silicate (Na2SiO3; chemical
compound with cement that dries it immediately). In cases where
cement contains >2% of quartz, workers are likely to present
radiological findings of silicification several years after
exposure (27). Individual sampling
was performed with a SKC 224-PCTX Respiratory Dust Sampling Pump
(SKC Inc.). The device is intended for the detection and
measurement of particles (inert dust, toxic dust, etc.) in the work
environment. The above device is a pump with a flow rate of
750-4,000 ml/min with a built-in battery. Samples were collected on
a filter which was weighed before and after sampling and analyzed
for the detection of crystalline silica. For the current samplings,
a Dorr Oliver type head with a flow of 2 l/min was used to collect
samples of 960 liters of air each, on a 37 mm cellulose ester
filter. Flow was checked before and after sampling. The analysis
procedure using the IR technique follows these steps: a known
amount of 1,3-butanediol was added at the sampling filter on which
the powder was collected and incubation at 600˚C followed. The
residue was then mixed with a given amount of potassium bromide
(KBr), triturated and homogenized in a vibrating mill. Part of this
mixture was used to produce a KBr tablet, which was placed as a
cell in the infrared spectroscope. Absorption was performed on an
FTIR spectrometer (model WQF-510A) at wavelengths 779/798
cm-1 to identify and quantify quartz.
Lung function
Pulmonary function tests (PFTs) in our study were
performed at the 1st Academic Department of Pneumonology of the
General Hospital of Thoracic Diseases of Athens ‘Sotiria’ using a
spirometer (Cosmed, Quark PFT Pulmonary Function Testing and Sensor
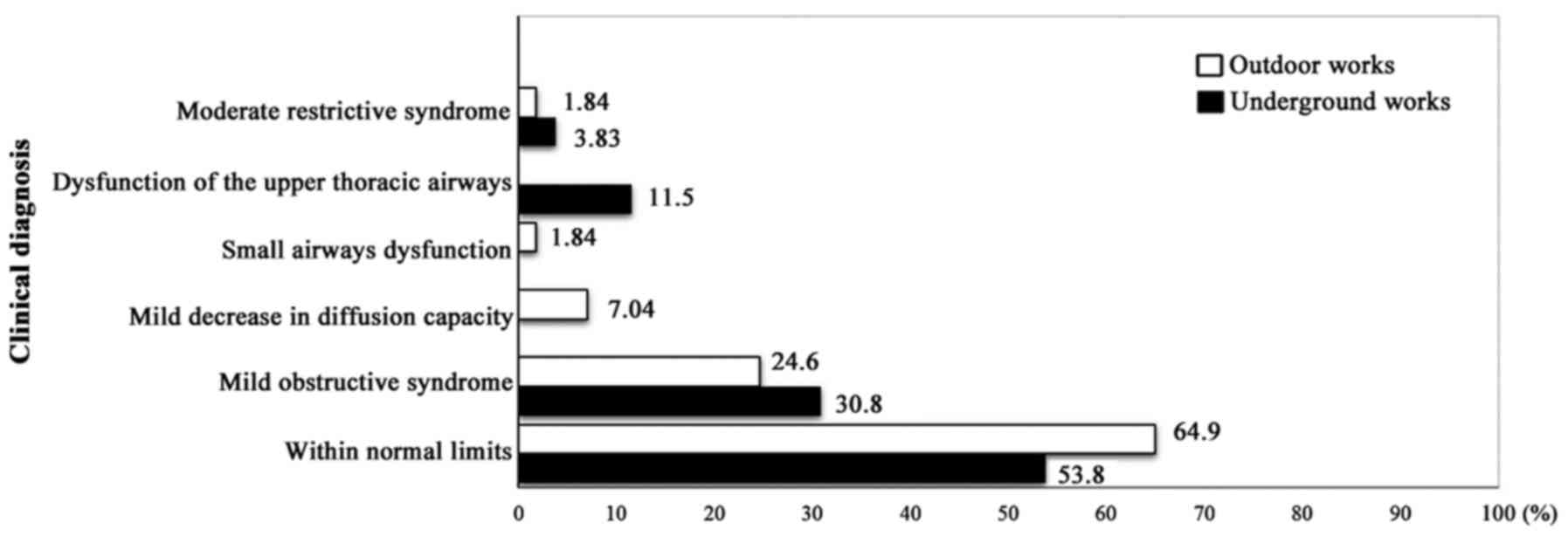
Medics™ Erich Jaeger). PFT results were categorized as within
normal limits, mild obstructive syndrome, mild decrease in
diffusion capacity, small airway dysfunction, moderate restrictive
syndrome, and upper thoracic airway dysfunction.
PFTs were performed using a commercially available
system (Master Screen, Erich Jaeger GmbH, Wuerzburg, Germany).
Forced expiratory volume in one second (FEV1), forced vital
capacity (FVC), FEV1/FVC ratio, the mean Forced Expiratory Flow
between the 25 and 75% of the FVC (FEF25-75), total
pulmonary capacity (TLC) - total lung capacity, diffusing capacity
or transfer factor (TLCO) for carbon monoxide
(DLCO), and the carbon monoxide transfer coefficient
(diffusing capacity for carbon monoxide adjusted for alveolar
ventilation) [KCO (DLCO/VA)] were recorded.
Post-bronchodilator values were obtained 20 min after the
administration of 400 mg salbutamol via a spacer (100 mg x 4
puffs). DLCO and diffusing capacity for carbon monoxide
adjusted for alveolar volume (DLCO/VA) were assessed by
means of the single breath method with the patient in the sitting
position (28). Lung function
measurements were expressed as percentages of predicted values
(20). The results were interpreted
in accordance with the guidelines of the American Thoracic Society
(29-31).
Moderate restrictive pulmonary syndrome was defined
as patients presenting TLC ranging from 60 to 79% of the predictive
values, small airway dysfunction was defined as patients presenting
FEF25-75 less than 65% of the predictive values with FVC
and FEV1 >80% of the predictive values, mild decrease in
diffusion capacity was defined as patients presenting DLCO ranging
from 60 to 79% of the predictive values and mild obstructive was
defined as patients presenting FEV1/FVC <75% and FEV1 >80% of
the predictive values.
Radiological findings
The chest X-rays of the participants were performed
at the Department of Imaging and Interventional Radiology of the
above-mentioned hospital; the Siemens X-RAY Diagnostics Axiom
Vertix Solitaire M radiograph was used. To perform the chest high
resolution computed tomography (HRCT), the INGENUITY CORE 64 system
(PHILIPS®) was used. The radiographs were evaluated
according to the system developed by the International Labor Office
Classification System in 1980 (32,33).
Statistical analysis
Statistical analysis was performed with IBM-SPSS
v.21 (IBM Corp.). The level of statistical significance was set at
5% (P=0.05). The detection of any possible correlation between the
type of construction and the radiological findings was performed
using Pearson's χ2 test.
Ethical approval
This research was approved by the bioethics and
ethics committee of the Medical School of the National and
Kapodistrian University of Athens under the decision 6323 received
on the 6th March 2013. Written consent was obtained from each
employee who participated in the study.
Results
All workers belonged to the same socioeconomic
class, with an average age of 41.04 years [standard deviation (SD):
9.68] and an average of 15.69 years of work (SD: 10.30); 70
employees were former and current smokers and did not use
prescription drugs. In more detail, underground construction
workers had an average age of 41.26 years (SD: 9.67) and an average
of 18.70 (SD: 11.32) working years. Outdoor construction workers
had an average age of 40.93 years (SD: 9.76) and an average of
14.31 (SD: 9.59) working years.
Environmental SiO2
measurements
The period when samples were received was the one in
which at the tunneling process a spray gun, also known as GUNITE
was extensively used; GUNITE contains Na2SiO3
and was present at all the working positions. Moreover, splashed
concrete contains components such as cement (containing 5%
silica-SiO2), additives, aggregates, coagulation
accelerators and silica foam. It is often used in tunnels,
underground works to stabilize slopes and excavations. Low exposure
to respiratory crystalline silica powder was observed among workers
in underground excavation and tunneling. In particular, the
concentration of SiO2 in underground construction was
0.0125 mg/m3 at all working positions from which samples
were drawn (Table I).
 | Table IEnvironmental testing of employees
working in underground construction projects. |
Table I
Environmental testing of employees
working in underground construction projects.
| Job position | Dust quantity
(mg) | Quantity of
SiO2 at the filter (µg) | Quantity of
SiO2 in the air (mg/m3) | Limit according to
the EU 2398/2017 |
|---|
| GUNITE launcher
concrete operator | 2.59 | 12 | 0.0125 | 0.1
mg/m3 |
| Craftsman
builder | 4.50 | 12 | 0.0125 | 0.1
mg/m3 |
| Machine
operator | 4.70 | 12 | 0.0125 | 0.1
mg/m3 |
PFTs
The results of the PFTs performed are shown in
Table II. According to analysis of
the results, 51 employees (61.4%) were within normal limits, 22
(26.5%) were diagnosed with mild obstructive syndrome, 4 (4.7%)
were diagnosed with mild impairment of diffusing capacity and 2
(2.4%) were diagnosed with moderate restrictive syndrome. However,
groups did not differ statistically significantly. The type of
working activity (underground-outdoor) was significantly associated
with categorization of PFT (P=0.038). The comparison of underground
and outdoor construction workers (Fig.
1) revealed that underground workers were less likely to lie
within normal limits compared to those working outdoors (53.8 vs.
64.9% respectively, P=0.038). In Fig.
1, the comparison of the functional respiratory testing results
for the various working activities are presented.
| Table IIPulmonary function test results. |
Table II
Pulmonary function test results.
| | Average values ±
SD | | | | |
|---|
| Test | Pre values | Post values |
Characterization | Frequency | % | Normal values |
|---|
| FVC % PRED (liters;
n=82) | 73.0±3.74 | 71.5±2.50 | Not normal | 3 | 3.74 | 80-120% |
| | 107±12.1 | 106±11.9 | Normal | 79 | 96.3 | |
| FEV1% PRED (liters;
n=82) | 75.8±1.48 | 85.5±10.9 | Not normal | 4 | 4.9 | 80-120% |
| | 101±11.1 | 103±15.7 | Normal | 78 | 95.1 | |
| FEV1/FVC
(n=81) | 68.8±5.24
97.7±11.5 | 71.7±5.00
94.4±15.7 | Not normal
Normal | 6 75 | 7.44 92.6 | >75 (in normal
patients or patients with moderate restrictive syndrome) |
|
FEF25-75% PRED (l/sec;
n=82) | 52.9±9.17 | 65.2±8.56 | Not normal | 9 | 11.0 | 65-135% |
| | 86.4±20.6 | 97.9±21.1 | Normal | 73 | 89.0 | |
| TLC % PRED
(n=83) | 67.9±11.8 | | Not normal | 8 | 9.63 | 80-120% |
| | 100±10.3 | | Normal | 75 | 90.4 | |
| DLCO
(mmol/kPa.min) | 71.0±4.38,
138±10.9 | Not normal | 9 | 10.7 | 80-120% |
| % PRED (n=84) | 96.2±11.5 | | Normal | 75 | 89.3 | |
| KCO
(DLCO/VA) % PRED (n=84) | 136±9.34 | | Not normal | 2 | 2.42 | 80-120% |
| | 105±33.2 | | Normal | 82 | 97.6 | |
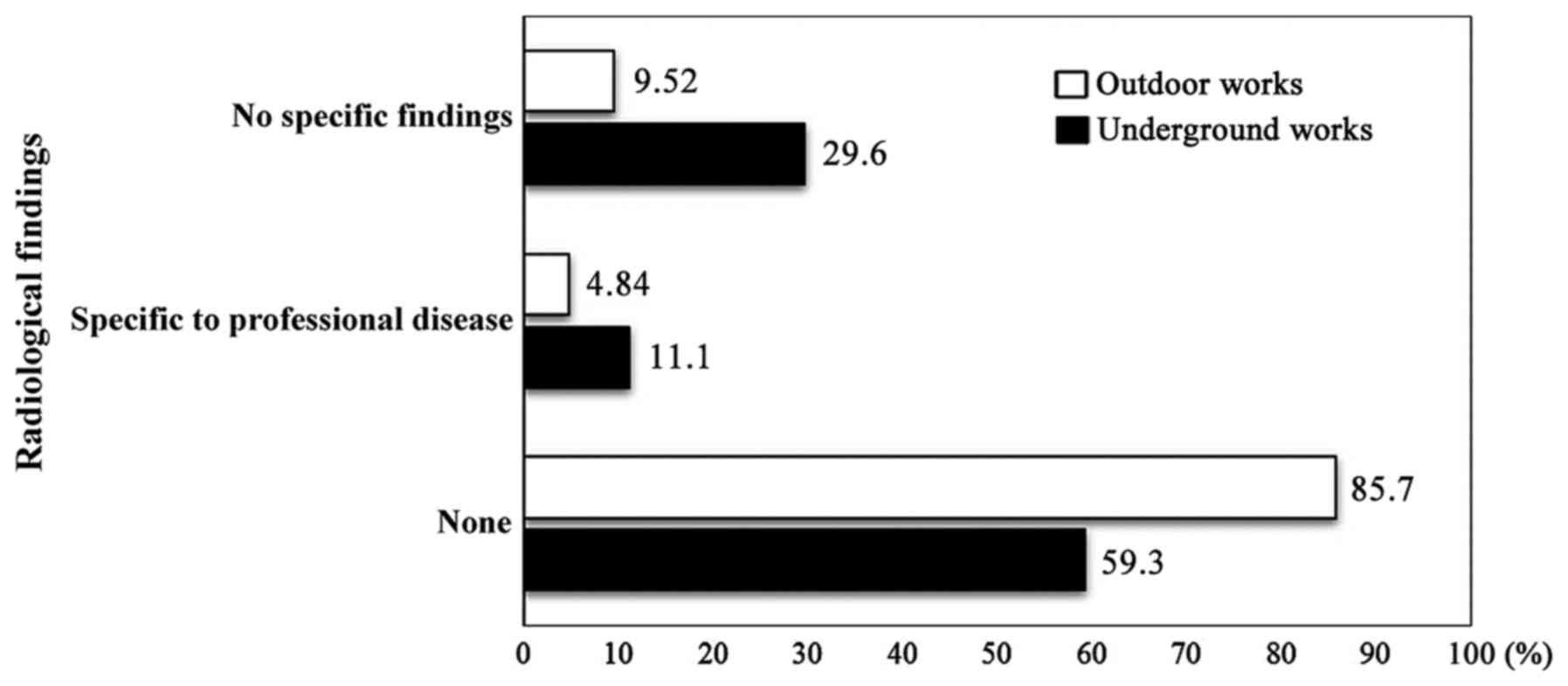
Radiology testing
Of the 86 workers, 69 participated in the
radiological examination. The remaining 17 employees from the
company engaged in outdoor construction projects, refused to
participate in the radiological examination because they stated
that they had performed this test at the same year as part of their
collaboration with the company. Of the 69 employees, in 52 (75.4%)
no findings were recorded and five (7.2%) were diagnosed with
specific occupational disease findings, while 12 (17.4%) presented
non-specific findings. Then, 1 out of the 5 subjects with abnormal
findings in chest X-ray was diagnosed with lung cancer three months
later. The comparison of underground and outdoor construction
workers (Table III, Fig. 2) showed that underground workers were
almost 30% more prone to develop radiological findings compared to
those working outdoors (P=0.044). Furthermore, underground jobs
were more likely to be linked both to specific (11.1% vs 4.8%,
P=0.044) and non-specific (29.6 vs. 9.5%, P=0.044) occupational
radiological findings compared to outdoor workers. The relationship
between job type and categorization of radiological findings was
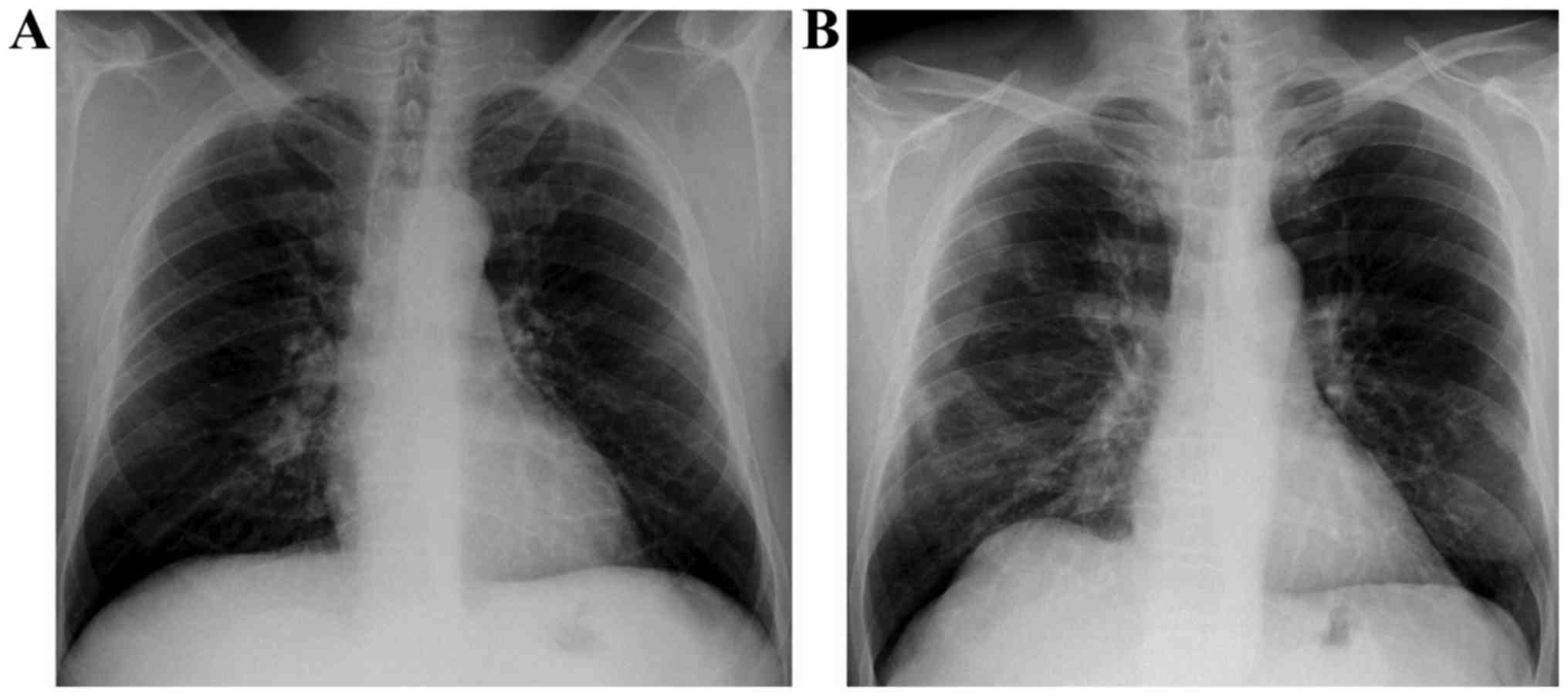
significant (Pearsons χ2=6.261, P=0.044). Corresponding
radiological findings are shown in Fig.
3. In one patient the chest X-ray revealed a suspicious right
hilar enlargement, as an incidental finding. A subsequent CT scan
of the chest confirmed the presence of a right hilar mass,
consistent with lung cancer.
| Table IIIRadiological findings and type of
job. |
Table III
Radiological findings and type of
job.
| Type of job | No findings | Specific to
occupational disease | Non-specific |
|---|
| Underground | 16 (59.30%) | 3 (11.10%) | 8 (29.6%) |
| Outdoor | 36 (85.7%) | 2 (4.80%) | 4 (9.5%) |
Discussion
Historically, silicosis is considered as a
significant occupational disease and is still of interest (34). During our study, environmental
measurements were performed, samples were collected to detect
breathable crystalline silica (SiO2) in the workplace of
outdoor and underground construction works, and medical tests of
the PFTs of workers were carried out. Chest X-rays, as well as HRCT
were also performed where deemed appropriate in order to obtain a
better picture of the diagnosis. Low exposure to respiratory
crystalline silica powder was observed among workers in underground
excavation and tunneling. In particular, the concentration of
SiO2 in underground construction was 0.0125
mg/m3, according to the limit value of 0.1
mg/m3 set by the European Union Directive
2017/2398/L345/87. This limit value is also laid down in the
National Mining and quarrying legislation (35). The above concentration of
SiO2 in the dust generated in underground construction
projects does not make it detrimental to the workers' health in the
area (36). According to the study
of Leung et al (37) low
environmental concentrations rarely pose any risk for silicosis. On
the contrary, in the study of Tavakol et al (18) construction workers' exposure to
respirable dust of crystalline silica dust exceeded the threshold
limit value. A similar conclusion on the exposure limit on
respiratory SiO2 in underground excavation works is
presented by the study of Mazurek and Attfield (38). An important factor regarding exposure
is the production process carried out in underground excavation
projects that involves the frequent use of sprayed concrete, also
known as GUNITE. Based on the results of the pulmonary function
testing in the present study, underground workers were more likely
to lie outside the normal limits compared to those working
outdoors. In the study by Hochgatterer et al (39), occupational quartz exposure adversely
affected lung function parameters. The finding that 5 workers
presented occupational disease-specific pathological findings can
be considered serious especially since these workers had worked for
>15 years in underground construction-excavation and tunneling
projects. In our study, lung function and X-ray findings did not
differ significantly between workers with more than 15 working
years against those with less than 15 working years. This is
further supported by the establishment of lung cancer diagnosis in
one employee three months after the inclusion into the current
study. This employee had a 30.5 year working history and was a
current smoker (60 packs/year). He mentioned that he was exposed to
Sodium silicate (Na2SiO3), sprayed concrete,
also known as GUNITE, dust from moving machinery and sand while he
also stated that his workplace did not have proper ventilation,
while he was wearing personal protective equipment (gloves, masks,
helmets, glasses). Since smoking is a risk factor for lung cancer,
the employee's lung cancer may be attributed both to environmental
working exposure and smoking. According to the study of Kachuri
et al (40), exposure of
workers for more than 30 years to crystalline SiO2,
which is considered a long exposure, is likely to increase the risk
of developing lung cancer (12,40). It
is worth noting that people working in underground construction
projects were fewer in number due to the financial crisis in Greece
from 2010 to date. Underground and outdoor projects have been
reduced in number throughout the country.
In conclusion, people in the Greek construction
industry were not exposed to crystalline silica powder that
exceeded the limit value as laid down in the European legislation.
Workers in underground tunneling projects with more than 15 years
exposure to SiO2 are more likely to develop silicosis in
its chronic form (27). Pulmonary
function testing revealed that underground workers were less likely
to lie within normal limits compared to those working outdoors. As
a result, further precautionary measures are required for workers
in the construction sector to promote their health and safety. In
particular, the following steps are suggested: i) a more frequent
training in safe work practices (41,42); ii)
the use of appropriate respiratory protection devices in accordance
with the requirements of European legislation (43); iii) undertaking of workers to
precautionary measures; iv) undergoing of medical tests every year;
and v) periodic workplace sampling to perform respiratory
crystalline silicon analyses with the results being compulsory
reported to the Competent Authority (36,44).
Finally, the establishment of a National Occupational Health and
Safety System is needed to identify risk factors in the work
environment in accordance with the National Occupational Health and
Safety Strategy (45).
Acknowledgements
The authors would like to thank all study
participants. The authors would also like to thank ‘Sotiria’
Hospital, both the Department of Imaging and Interventional
Radiology, and 1st Department of Pneumonology, Medical School,
National and Kapodistrian University of Athens for their evaluation
of the study participants and for providing use of the radiology
and imaging laboratory. Special thanks for her total contribution
to Dr Nektaria Sidiropoulou, Doctor Radiologist.
Funding
This study was funded by own revenue.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
All authors have read and approved the final version
of this manuscript. DK: Organization and performing of research,
collecting and testing samples, writing of the research article,
overall project management. MA, KT: Evaluation of radiological
reports. PB: Evaluation of pulmonary tests. GC: Statistical
analysis, data assessment. CT, KT, EC: Statistical analysis and
evaluation of the results, preparation, and writing of the research
article. IC, VD, AP, EP, TCC, NK, EP, DAS: Reviewing and
comprehensive manuscript plan assessment. ACL and PP: Assistance to
collecting the necessary samples, in cooperation with DK, data
assessment, total preparation and writing of the research article,
organizing the references, reviewing and plan assessment.
Ethics approval and consent to
participate
The current study was approved by the Ethics and
Bioethics Committee of the Medical School of the National and
Kapodistrian University of Athens (Protocol no. 6323 received 6th
March, 2013. All procedures were in accordance with the ethical
standards of the responsible committee on human experimentation and
patient's evaluation reports (institutional and national) and in
agreement with the Helsinki Declaration of 1964 and later versions.
All the data were original, used in the current study with
anonymity and confidentiality. Informed consent or substitute for
it was obtained from all study participants-workers prior to
enrolment.
Patient consent for publication
All study participants were informed in detail and
agreed to the publication of associated data (and any accompanying
images or reports) as appropriate, fully respecting their anonymity
and medical ethics. The worker's consent forms from the current
study are available from the corresponding author, on reasonable
request.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this article.
The other authors declare that they have no competing
interests.
References
|
1
|
NEPSI The European Network on Silica:
Agreement on Workers Health Protection through the Good Handling
and Use of Crystalline Silica and Products containing it.
https://www.nepsi.eu/sites/nepsi.eu/files/content/editor/agreement_-_english.pdf.
Updated December 18, 2017.
|
|
2
|
European Commission: Guidance for National
Labour Inspectors on addressing risks from worker exposure to
respirable crystalline silica (RCS) on construction sites.
https://osha.europa.eu/en/guidance-national-labour-inspectors-on-addressing-risks-from-worker-exposure-to-respirable-crystalline-silica.
Accessed October 2016.
|
|
3
|
Apatsidou M, Konstantopoulou I, Foufa E,
Tsarouhas K, Papalexis P, Rezaee R, Spandidos DA, Kouretas D and
Tsitsimpikou C: Safe use of chemicals by professional users and
health care specialists. Biomed Rep. 8:160–165. 2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Fenga C, Gangemi S, Giambò F, Tsitsimpikou
C, Golokhvast K, Tsatsakis A and Costa C: Low-dose occupational
exposure to benzene and signal transduction pathways involved in
the regulation of cellular response to oxidative stress. Life Sci.
147:67–70. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Koulaouzidou EA, Roussou K, Sidiropoulos
K, Nikolaidis A, Kolokuris I, Tsakalof A, Tsitsimpikou C and
Kouretas D: Investigation of the chemical profile and cytotoxicity
evaluation of organic components eluted from pit and fissure
sealants. Food Chem Toxicol. 120:536–543. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sauvé JF, Beaudry C, Bégin D, Dion C,
Gérin M and Lavoué J: Silica exposure during construction
activities: statistical modeling of task-based measurements from
the literature. Ann Occup Hyg. 57:432–443. 2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Steenland K and Ward E: Silica: A lung
carcinogen. CA Cancer J Clin. 64:63–69. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
No authors listed: IARC Working Group on
the Evaluation of Carcinogenic Risks to Humans: IARC Working Group
on the Evaluation of Carcinogenic Risks to Humans: Silica, Some
Silicates, Coal Dust and Para-Aramid Fibrils. Lyon, 15-22 October
1996. IARC Monogr Eval Carcinog Risks Hum 68: 1-475, 1997.
|
|
9
|
European Commission: Proposal for a
Directive of The European Parliament and of The Council amending
directive 2004/37/EC on the protection of workers from the risks
related to exposure to carcinogens or mutagens at work. https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A52016PC0248.
Accessed May 13, 2016.
|
|
10
|
European Comission: Commission
Recommendation of 19 September 2003 concerning the European
schedule of occupational diseases (Text with EEA relevance)
(notified under document number C(2003) 3297). https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX%3A32003H0670.
Accessed September 19, 2003.
|
|
11
|
Hellenic Republic Presidential: Decree no.
41/2012, National list of occupational diseases, in accordance with
Commission Recommendation 2003/670/EC 19.09.2003.
|
|
12
|
Rees D and Murray J: Silica, silicosis and
tuberculosis. Int J Tuberc Lung Dis. 11:474–484. 2007.PubMed/NCBI
|
|
13
|
Arndt V, Rothenbacher D, Daniel U,
Zschenderlein B, Schuberth S and Brenner H: All-cause and cause
specific mortality in a cohort of 20,000 construction workers;
results from a 10 year follow up. Occup Environ Med. 61:419–425.
2004.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Beaudry C, Lavoué J, Sauvé J-F, Bégin D,
Senhaji Rhazi M, Perrault G, Dion C and Gérin M: Occupational
exposure to silica in construction workers: A literature-based
exposure database. J Occup Environ Hyg. 10:71–77. 2013.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Oliver LC, Miracle-McMahill H, Littman AB,
Oakes JM and Gaita RR Jr: Respiratory symptoms and lung function in
workers in heavy and highway construction: A cross-sectional study.
Am J Ind Med. 40:73–86. 2001.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Arcangeli G, Cupelli V, Montalti M,
Pristera M, Baldasseroni A and Giuliano G: Respiratory risks in
tunnel construction workers. Int J Immunopathol Pharmacol. 17
(Suppl):91–96. 2004.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ellingsen DG, Ulvestad B, Bakke B,
Seljeflot I, Barregard L and Thomassen Y: Serum pneumoproteins in
tunnel construction workers. Int Arch Occup Environ Health.
88:943–951. 2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Tavakol E, Azari M, Zendehdel R, Salehpour
S, Khodakrim S, Nikoo S and Saranjam B: Risk Evaluation of
Construction Workers' Exposure to Silica Dust and the Possible Lung
Function Impairments. Tanaffos. 16:295–303. 2017.PubMed/NCBI
|
|
19
|
Khoza NN, Grové T and Schutte PC: Worker
exposure to silica dust in South African non-mining industries in
Gauteng: An exploratory study. Occup Health S Africa. 18:18–26.
2012.
|
|
20
|
Hellenic Pulmonary Society: Occupational
and environmental lung diseases. Hellenic Pulmonary Society,
Athens, 2007. http://www.hts.org.gr/assets/files/biblia_epe/epaggelmatika_nosimata.pdf.
|
|
21
|
Hellenic Republic Joint Ministerial
Decision: F.80000/45219/1864/2017 Single Disability Identification
Table.
|
|
22
|
IARC monographs: Arsenic, metals, fibres,
and dusts. Volume 100 C. A review of human carcinogens. IARC, Lyon,
2012. https://monographs.iarc.
fr/wp-content/uploads/2018/06/mono100C.pdf.
|
|
23
|
Linch KD: Respirable concrete dust -
silicosis hazard in the construction industry. Appl Occup Environ
Hyg. 17:209–221. 2002.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Tavakol E, Azari MR, Salehpour S and
Khodakarim S: Determination of Construction Workers' Exposure to
Respirable Crystalline Silica and Respirable Dust. J Saf Promot Inj
Prev. 3:263–270. 2016.
|
|
25
|
European Commission: Regulation (EC) No.
1272/2008 of the European Parliament and of the Council of 16
December 2008 on classification, labelling and packaging of
substances and mixtures, amending and repealing Directives
67/548/EEC and 1999/45/EC, and amending Regulation (EC) No.
1907/2006. https://eur-lex.europa.eu/eli/reg/2008/1272/oj.
Accessed December 31, 2008.
|
|
26
|
Hellenic Republic Presidential: Decree
77/1993, For the protection of workers against physical, chemical
and biological agents and amending and supplementing Presidential
Decree 307/86 in accordance with its Directive Council Regulation
88/642/EEC.
|
|
27
|
Patakas D: Epithelial pulmonology. 2nd
edition. University Studio Press, Thessaloniki, 2006.
|
|
28
|
Macintyre N, Crapo RO, Viegi G, Johnson
DC, van der Grinten CP, Brusasco V, Burgos F, Casaburi R, Coates A,
Enright P, et al: Standardisation of the single-breath
determination of carbon monoxide uptake in the lung. Eur Respir J.
26:720–735. 2005.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Miller MR, Hankinson J, Brusasco V, Burgos
F, Casaburi R, Coates A, Crapo R, Enright P, van der Grinten CP,
Gustafsson P, et al: ATS/ERS Task Force: Standardisation of
spirometry. Eur Respir J. 26:319–338. 2005.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Pellegrino R, Viegi G, Brusasco V, Crapo
RO, Burgos F, Casaburi R, Coates A, van der Grinten CP, Gustafsson
P, Hankinson J, et al: Interpretative strategies for lung function
tests. Eur Respir J. 26:948–968. 2005.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Kreider ME and Grippi MA: Impact of the
new ATS/ERS pulmonary function test interpretation guidelines.
Respir Med. 101:2336–2342. 2007.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Webb WR and Higgins CB: Thoracic imaging:
pulmonary and cardiovascular radiology. 3rd edition. LWW, 2017.
|
|
33
|
Cox CW and Lynch DA: Medical imaging in
occupational and environmental lung disease. Curr Opin Pulm Med.
21:163–170. 2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Greenberg MI, Waksman J and Curtis J:
Silicosis: A review. Dis Mon. 53:394–416. 2007.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Hellenic Republic: Ministerial Decision
Δ7/Α/off.12050/2223/2011 ‘Mining and Quarry Works Regulation’,
Government Gazette, Series II, No. 1227/2011.
|
|
36
|
European Comission: Directive (EU)
2017/2398 of the European Parliament and of the Council of 12
December 2017 amending Directive 2004/37/EC on the protection of
workers from the risks related to exposure to carcinogens or
mutagens at work. https://eur-lex.europa.eu/eli/dir/2017/2398/oj.
Accessed December 27, 2017.
|
|
37
|
Leung CC, Yu ITS and Chen W: Silicosis.
Lancet. 379:2008–2018. 2012.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Mazurek JM and Attfield MD: Silicosis
mortality among young adults in the United States, 1968-2004. Am J
Ind Med. 51:568–578. 2008.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Hochgatterer K, Moshammer H and Haluza D:
Dust is in the air: Effects of occupational exposure to mineral
dust on lung function in a 9-year study. Lung. 191:257–263.
2013.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Kachuri L, Villeneuve PJ, Parent M-É,
Johnson KC and Harris SA: Canadian Cancer Registries Epidemiology
Group: Occupational exposure to crystalline silica and the risk of
lung cancer in Canadian men. Int J Cancer. 135:138–148.
2014.PubMed/NCBI View Article : Google Scholar
|
|
41
|
European Commission: Council Directive
89/391/EEC of 12 June 1989 on the introduction of measures to
encourage improvements in the safety and health of workers at work.
https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX%3A31989L0391.
Accessed June 29, 1989.
|
|
42
|
Hellenic Parliament: Law No. 3850 of 2010
ratifying the Code of Laws related to Occupational Safety and
Health.
|
|
43
|
European Commission: Regulation (EU)
2016/425 of the European Parliament and of the Council of 9 March
2016 on personal protective equipment and repealing Council
Directive 89/686/EEC. https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32016R0425.
Accessed March 31, 2016.
|
|
44
|
European Commission: Consolidated text:
Directive 2004/37/EC of the European Parliament and of the Council
of 29 April 2004 on the protection of workers from the risks
related to exposure to carcinogens or mutagens at work (Sixth
individual Directive within the meaning of Article 16(1) of Council
Directive 89/391/EEC) (codified version). https://eur-lex.europa.eu/legal-content/en/TXT/?uri=CELEX%3A02004L0037-20140325.
Accessed April 30, 2004.
|
|
45
|
Hellenic Republic Ministerial: Decision
no. 48416/2564/2017 - Adoption of National Strategy for Health and
Safety at Work for the years 2016-2020, 2017.
|