Introduction
Adequate maternal intake of nutrients during
pregnancy supports the fetal growth and development, thus maternal
malnutrition and supranutrition may have both short-term and
long-term adverse fetal impact (1-3).
Barker's hypothesis on the development of the diseases suggests
that the fetal environment and the changes of the fetal metabolic
pathways cause epigenetic changes that influence the development of
diseases in childhood and adulthood (4). Therefore, it is important to evaluate,
monitor and, if appropriate, take measures to optimize the maternal
diet both preconceptionally and during the gestation and lactation
periods.
Pregnant women should eat nutrient-dense foods to
meet higher nutritional requirements during pregnancy without
exceeding the caloric requirement (5). Consultation of a nutritionist with a
special training in the maternal field is suitable and recommended
for women with special nutritional considerations (6,7) such as
metabolic disorders (diabetes, hypertension, phenylketonuria,
gastrointestinal disorders, bariatric surgical or digestive tract
resection history with impaired absorption), modified caloric
requirements [extreme age (8),
multiple pregnancy, underweight, overweight, obesity (9), personal history of major weight
fluctuations, another fetus with neural tube defect (10)], unhealthy eating habits (restrictive
diets, eating disorders that require medication or hospitalization,
intolerance and food allergies, use of toxic substances or drugs
that affect nutrition). Some women might need adjusted
micronutrient supplementation (8,11,12).
Asking the patient to complete a questionnaire is
helpful in reviewing her typical diet and in identifying obvious
deficiencies (13) or potential
problems such as reducing the number of meals required daily,
following a special diet, the consumption of artificially sweetened
beverages.
The purpose of the study was to analyse food
behavior during pregnancy and to determine the extent to which
pregnant women in the third trimester of pregnancy complied with
the doctors' recommendations regarding nutrition and lifestyle. In
the subsidiary, we aimed to verify the hypothesis that the higher
the biological age of the pregnancy, the higher is the level of
awareness and application of the recommendations on a healthy and
balanced nutrition (based on the food pyramid). Another objective
of the present research involves offering, based on the conclusions
drawn from its development, recommendations to those involved in
reducing the materno-fetal risks of poor maternal feeding and/or
lifestyle.
Subjects and methods
The research data for this study was collected
between 15-30.03.2018 following the application of scale
instruments-questionnaire, using the pencil-paper method, on a
sample of 100 pregnant women aged between 15 and 41 years in the
third trimester of pregnancy. Although this version of the
questionnaire has not yet been scientifically validated, a more
general version has been validated to assess the risk of chronic
diet-related diseases and has been successfully used in women
(13).
The participants were selected by the
criterion-based sampling method. Without neglecting the particular
aspects, we aimed to capture the common experience of the
participants, focusing on more general data. The recruitment
procedure was based on convenience and a voluntary basis, the tests
were applied individually, the questionnaire was completed only
once, with a time limit of ~20 min to guarantee the confidentiality
of the information collected. Statistical methods and tools in
Microsoft Excel were used to group the results and to verify the
proposed research hypothesis.
The main analyzed data concern the dietary behavior,
information by the obstetrician and the extent to which pregnant
women follow these recommendations, the presence of dietary
restrictions, use of foods with infectious risk regarding
listeriosis and toxoplasmosis, the consumption of dietary
supplements, of multivitamins and minerals, lifestyle assessment
(physical activity, smoking, coffee, alcohol, drugs, other
medication in pregnancy).
Analysis of the correlation between
pregnant biological age and dietary behavior
Starting from the hypothesis that the eating
behavior is improved (body mass index-BMI is within the normal
limits) as the biological age of the pregnancy is higher, the
questionnaire investigated the type of food consumed the previous
day and if this feeding mode is usually adhered to. Initially, the
subjects had to choose from 5 food groups, presented in the
questionnaire as the Food Pyramid (group 1 at the base of the
pyramid includes bread, cereals, rice, pasta and potatoes, group 2
contains fruits and vegetables, group 3 includes dairy products,
group 4 products such as red meat, white meat and eggs, and group 5
at the top of the pyramid contains processed sweets). In order to
quantify the nutritional value of each of the five groups in
relation to the other, whereas not to disadvantage a pregnant woman
eating from only two groups of aliments, but of high nutritional
value, compared to those who consume from all or almost all food
groups, the nutritional value of food groups was ascending ranked
(0-4 points) as follows: group 5 (processed sweets), 0; group 4
(white and red meat), 1; group 1 (products of pasta and cereals),
2; group 3 (dairy products), 3; and group 2 (vegetables, fruits), 4
points. In addition, to express the dietary behavior of the
pregnant woman regardless of the number of food groups consumed
daily, a total score was calculated as an arithmetic mean: the sum
of the points related to all the groups that the pregnant women
consumed the previous day divided by the number of food groups.
The final scores expressed the integrated behavior
between 0 and 4, where a score 0 corresponds to the case of eating
only food in group 5 (processed sweets) and a score 4 corresponds
to the case of eating only the food in group 2 (vegetables and
fruits). However, even this score might not be sufficiently
accurate on real food behavior of the pregnant women. For this
reason, the final score should integrate a correction coefficient
depending on the reccurence of the given food behavior from the
previous day. To the final score was added or subtracted 0.5 points
according to the following criteria: For score <2 from the first
formula: if the pregnant woman will keep the inappropriate eating
behavior, then 0.5 points are substracted; otherwise, if the
pregnant woman declares that she changes the dietary behavior
(presumably with a more beneficial one), then 0.5 points are added.
For score ≥2 (eating behavior during the previous day according to
the recommendations): if the pregnant women will keep the eating
behavior, then 0.5 points are added; otherwise if the food behavior
is changed (supposedly with a less beneficial one) then 0.5 points
are substracted. In order to achieve slightly technically this
correction for the final score a Microsoft Excel IF function was
used as follows: = IF (OR (AND (Pn <2; Qn =
‘D’); AND (Pn> = 2; Qn = ‘N’));-0.5;
0.5), where Pn is the final score 1 and Qn is the answer to
question no. 2 (Yes or No). The obtained final score 2 estimates
the eating behavior for each pregnant woman in the study. To the
value of final score 2 was added the number of meals per day (with
the mention that for the answer ‘more than 3 meals’ the ideal case
of 5 meals per day was considered) and the values were further
normalized. The next step was to verify the supposed correlation
with the subject's biological age. Since there are more pregnant
women of same age, there are two further levels of sorting: week of
gestation and body-weight before pregnancy, resulting in 6 age
categories (15-19, 20-24, 25-29, 30-34, 35-39 and 40-44 years).
Several parameters of interest were calculated for each age
group.
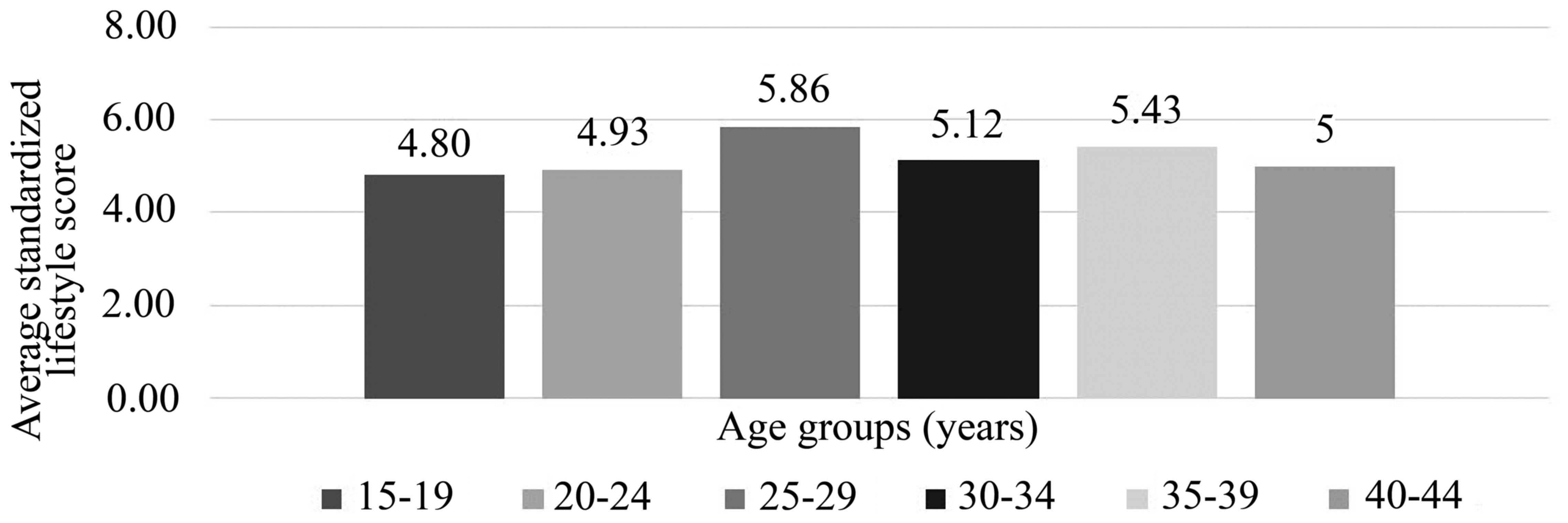
Analysis of the correlation between
biological age of the pregnant woman and lifestyle
To address the lifestyle assessment of pregnant
women, they were questioned about regular physical activity,
smoking, consumption of alcoholic beverages, coffee, medicines and
recreational drugs and specific scores were assigned depending on
the answer options: for the question regarding physical activity
score 1 was assigned to active women and score 0 to sedentary ones;
for the question regarding smoking, the score 0-3 was assigned
depending on the number of cigarettes smoked per day (0
cigarettes/day, 3; 0-10 cigarettes/day, 2; 10-20 cigarettes/day, 1;
20+ cigarettes/day, 0 points); for the question regarding the
consumption of coffee the score 0-2 was assigned depending on the
number of cups consumed per day (0 cups, 2; <4 cups/day, 1; ≥4
cups/day, 0 points); for the question regarding the consumption of
medicines in general, respectively the consumption of medicines not
prescribed by the doctor 0 points were given to the women who
answered positively and 1 point for a negative answer. For each
subject the points were summed up. The data was sorted by age
groups, similarly to the previously used method. The aim was to
verify the hypothesis that as biological age of a pregnant woman
increases, the healthier her lifestyle is.
Results
Regarding the number of meals per day of the
pregnant women, only 44% of our respondents complied with the
recommended number of meals per day, i.e. 3 main meals and 1-2
snacks, while 41% of all pregnant women take only 3 meals a day,
presumably being the main ones. Another 14% of the respondents said
they only have 2 meals a day while one of the 100 pregnant women
said that they only have one meal a day.
Studies have shown that symptoms of nausea and
vomiting are specific to the first trimester of pregnancy and
abnormal in the third trimester; Symptoms of heartburn are normal
starting by week 30 of pregnancy, and constipation are normal in
weeks 10-22. Our results showed that a large number of pregnant
women (44%) report symptoms of nausea/vomiting. Regarding the
sensations of retrosternal burns-pyrosis 64% of pregnant women said
they have such symptoms, and especially those in 33 weeks of
pregnancy, indicating that almost 2/3 of pregnant women have
specific symptoms of pyrosis, moreover, normal for this period.
Regarding the constipation symptoms, the majority (70%) of the
pregnant women responded negatively, thus falling into the norm. To
be more precise, regarding the other 30% of the pregnant women
questioned to which the answer to the question was yes, it would be
necessary to investigate to what extent they had such symptoms
before pregnancy.
Regarding the hypothesis that the higher the
biological age of the pregnant woman, the better her dietary
behavior (BMI within normal limits), after applying the formulas
detailed in methodology, we observed that the average age of
pregnant women in this study is 29.55 years, the initial average
weight is 66.21 kg and the a current weight (third trimester of
pregnancy) is 78.12 kg. We note that BMI at the time of recording
the pregnancy is arround the superior limit of the normal interval,
suggesting that most women were overweight initially (or have been
recorded by the obstetricean when they have already started to gain
weight).
The average value of the score for dietary behavior
and number of meals per day were further correlated and normalized,
the final results being summarized in the last column of Table I. Noticeably, the dietary behavior
improves by age, especially in the case of pregnant women aged over
35 years.
 | Table IAverage values by age group within the
sample of 100 pregnant women. |
Table I
Average values by age group within the
sample of 100 pregnant women.
| Age groups
(years) | N | A (years) | H (cm) | GW | W1
(kg) | BMI1 | W2
(kg) | BMI2 | Average score for
DB | Average of Mpd | X |
|---|
| 15-19 | 5 | 17.6 | 170.4 | 35.6 | 69.4 | 23.7 | 81.6 | 28.0 | 2.1 | 3.8 | 5.9 |
| 20-24 | 14 | 22.0 | 164.8 | 35.1 | 65.2 | 23.8 | 75.5 | 27.7 | 2.2 | 3.5 | 5.7 |
| 25-29 | 29 | 27.2 | 165.0 | 33.5 | 64.1 | 23.5 | 77.0 | 28.3 | 2.2 | 3.7 | 6.2 |
| 30-34 | 33 | 31.9 | 165.8 | 33.7 | 66.8 | 24.1 | 78.4 | 28.3 | 2.1 | 3.8 | 6.1 |
| 35-39 | 14 | 36.5 | 163.1 | 31.4 | 66.1 | 24.8 | 78.3 | 29.4 | 2.8 | 3.7 | 8.5 |
| 40-44 | 5 | 40.2 | 167.0 | 34.6 | 73.4 | 26.1 | 85.4 | 30.4 | 2.7 | 4.2 | 9.6 |
| Total | 100 | 29.5 | 165.3 | 33.7 | 66.2 | 24.1 | 78.1 | 28.5 | 2.3 | 3.7 | 6.5 |
The risk of listeriosis and toxoplasmosis in the
third trimester of pregnancy depends on the dietary behavior
throughout the pregnancy. Risk assessment regarding these
conditions revealed that a large percentage (68%) of the total
pregnant women consumed artisanal, raw milk cheese questioned,
which could denote, on one hand, the influences of traditional
Romanian consumption and, on the other hand, the distrust in the
profile industry and the avoidance of processed cheeses. However,
there is an increased risk of listeriosis in about two thirds of
the pregnant women surveyed. The risk of toxoplasmosis is even
higher since a very large percentage (91%) of women consumed
grilled beef/pork/game, raw smoked sausages, charcuterie, figs or
gizzards in pregnancy and furthermore, 24% of the pregnant women
admitted having had contact with cats/dogs/other animals without
owners during pregnancy.
The study also aimed to analyze the level of medical
nutrition information and awareness of the pregnant women. The
obtained results showed that a majority (72%) of all pregnant women
received dietary information from the doctor when recording the
pregnancy. On the other hand, over a quarter of the pregnant women
(28%) deny having received nutritional recommendations, which
denotes organizational deficiencies in the medical staff. By
corroborating these data with those of eating behavior and risk of
listeriosis and toxoplasmosis, as we determined that a large number
of pregnant women do not meet the number of 4-5 meals a day and
consume inappropriate food, we might think that, although there is
some information coming from the obstetricians, more measures are
needed to raise awareness among pregnant women about the risks of
improper nutrition.
The pregnant women in the sample were also asked
whether they follow certain dietary restrictions for health or
religious reasons and the answers showed that almost one third of
the pregnant women have dietary restrictions.
In order to evaluate the consumption of dietary
supplements recommended before and during pregnancy, the
respondents were questioned on the administration of folic acid,
iron, selective multivitamins and multivitamins + minerals.
Regarding folic acid, which is indicated before pregnancy and in
the first trimester to reduce the fetal risk of neural tube defects
and/or autism, almost one third of women (28%) took preconceptional
folic acid and 82% admitted the administration of folic acid during
pregnancy, a relatively high percentage compared to the percentage
of those who comply with other recommendations on proper nutrition
during pregnancy. Regarding the consumption of iron, it is
recommended starting from the 12th week of pregnancy. Of the
pregnant women surveyed, almost two thirds (65%) answered
affirmatively regarding the administration of iron preparations
during pregnancy. Twenty-seven pregnant women took iron supplements
in the first trimester and did not continue after, most of them
either not being informed that it is necessary to continue iron
treatment, either decided to give up iron supplements due to
adverse effects or the treatment was an additional financial
effort. Five of the eight pregnant women who did not take iron
supplements at all during pregnancy reported that they were not
informed by the doctor regarding a correct diet. The results
regarding other supliments during pregnancy showed that 43% of the
respondents consumed selective vitamins, while 51% of the pregnant
consumed complex multivitamins and multiminerals. A large
percentage, 30%, did not consume such supplements during pregnancy
(in one form or another) and more than half of these pregnant women
reported that they were not informed by the doctor, proving a lack
of information in this regard. For the other pregnant women who,
although informed, did not apply this recommendation, we can either
conclude that they were not aware of the risks, or are afraid to
consume supplements due to some disinformation, or the treatment is
relatively expensive.
The research hypothesis of an existing correlation
between increasing the biological age of pregnancy and a healthier
lifestyle was not confirmed, as presented in Fig. 1, since the average score calculated
for lifestyle is not increasing as the pregnant is older. None of
our respondents stated that they would consume alcoholic beverages
or drugs.
Discussion
Healty dietary behavior depends not only on medical
information (14). Although most of
our pregnant respondents received nutritional recommendations from
the obstetrician, the compliance with these recommendations remains
deficient with regard to certain unhealthy eating habits, diet
restriction and supplement consumption. Our study showed that
eating behavior is more appropriate with the specific dietary
recommendations especially after the age of 35, in the sense of
respecting the beneficial nutritional structure of the Food
Pyramid, keeping the habit of eating healthy and respecting the
optimal number of meals per day. Also, lifestyle improvement was
observed in the age range 25-29 years and 35-39 years. The risk of
listeriosis and toxoplasmosis can be quite high due to poor hygiene
of food preparation, transport and distribution, extended
traditional food consumption, connections with the rural
environment, inadequate food education during pregnancy, modest
financial situation. Training programs for medical staff and
standardized dietary evaluation are needed to ensure that pregnant
women are not only informed, but also aware of the risks in case of
non-compliance with the main recommendations in the field. To
determine more precisely the dietary behavior of pregnant women it
might be necessary to study a larger sample of patients from
various backgrounds.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
ACI, MMC, NT and ID collected, analyzed and
interpreted the patient data regarding the eating behavior during
pregnancy. REB, CAZ and OMT substantially contributed to the
conception of the study and the data interpretation, drafted the
manuscript and were major contributors in the writing of the
manuscript. All authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ramakrishnan U, Grant F, Goldenberg T,
Zongrone A and Martorell R: Effect of women's nutrition before and
during early pregnancy on maternal and infant outcomes: A
systematic review. Paediatr Perinat Epidemiol. 26 (Suppl
1):285–301. 2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
American College of Obstetricians and
Gynecologists. ACOG Committee opinion no. 549: Obesity in
pregnancy. Obstet Gynecol. 121:213–217. 2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Haider BA and Bhutta ZA:
Multiple-micronutrient supplementation for women during pregnancy.
Cochrane Database Syst Rev. 4(CD004905)2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Barker DJ and Thornburg KL: The obstetric
origins of health for a lifetime. Clin Obstet Gynecol. 56:511–519.
2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Kaiser L and Allen LH: American Dietetic
Association. Position of the American Dietetic Association:
Nutrition and lifestyle for a healthy pregnancy outcome. J Am Diet
Assoc. 108:553–561. 2008.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Turcan N, Bohîlţea R, Neacsu A, Baros A
and Cîrstoiu MM: The role of anticoagulant therapy in the
prevention of preeclampsia. Pharmacokinetic and pharmacodinamic
mechanisms. Rev Chim. 70:1424–1428. 2019. View Article : Google Scholar
|
|
7
|
Bohîlţea R, Turcan N, Ionescu C, Toader O,
Nastasia S, Neculcea D, Movileanu I, Munteanu O and Cîrstoiu M: The
incidence of prematurity and associated short-term complications in
a multidisciplinary emergency hospital from Romania. In:
Proceedings of the 5th Congress of the Romanian Society of
Ultrasound in Obstetrics and Gynecology. pp105–112. 2017.
|
|
8
|
Bohîlţea RE, Zugravu CA, Neacsu A, Navolan
D, Berceanu C, Nemescu D, Bodean O, Turcan N, Baros A and Cîrstoiu
MM: The prevalence of vitamin D deficiency and its obstetrical
effects. A prospective study on Romanian patients. Rev Chim.
70:1228–1233. 2019. View Article : Google Scholar
|
|
9
|
Szasz F, Levai C, Navolan D, Farcas S,
Andreescu N, Birsasteanu F, Mehedintu C, Ionescu CA, Bohîlţea R,
Carabineanu A, et al: Weight of pregnant women and their influence
on second trimester biochemical markers. REV CHIM. 69:529–532.
2018. View Article : Google Scholar
|
|
10
|
Wolff T, Witkop CT, Miller T and Syed SB:
U.S. Preventive Services Task Force: Folic acid supplementation for
the prevention of neural tube defects: An update of the evidence
for the U.S. Preventive Services Task Force. Ann Intern Med.
150:632–639. 2009.PubMed/NCBI
|
|
11
|
Wolf HT, Hegaard HK, Huusom LD and Pinborg
AB: Multivitamin use and adverse birth outcomes in high-income
countries: A systematic review and meta-analysis. Am J Obstet
Gynecol. 217(404.e1-404.e30)2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Bohiltea R, Turcan N, Cavinder CM, Ionita
D, Paunica I, Andronache LF and Cirstoiu MM: Risk factors,
predictive markers and prevention strategies for intrauterine fetal
death. An integrative review. J Mind Med Sciences. 7(10)2020.
View Article : Google Scholar
|
|
13
|
Widen E and Siega-Riz AM: Prenatal
nutrition: A practical guide for assessment and counseling. J
Midwifery Womens Health. 55:540–549. 2010.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Lucas C, Charlton KE and Yeatman H:
Nutrition advice during pregnancy: Do women receive it and can
health professionals provide it? Matern Child Health J.
18:2465–2478. 2014.PubMed/NCBI View Article : Google Scholar
|