CVD is a term used to collectively describe diseases
involving the heart and/or vasculature. CVD mainly includes
diseases caused by atherosclerosis (1). The Emerging Risk Factors Collaboration
is based on a large number of population studies and has found that
CRP concentrations are closely associated with coronary arterial
disease, cancer, ischemic stroke and vascular diseases (18). However, more noteworthy is the
comparison between men and women, as men develop CVD earlier and
the risk of CVD increases with age (19). Atherosclerosis is a chronic
inflammatory disease that is initially asymptomatic. Early
atherosclerosis is associated with limited plaque formation, which
does not affect the blood circulation (20). However, the plaques forming on the
inner arterial wall gradually increase in size, causing narrowing
of the arterial lumen and/or thrombus formation. At this stage, the
blood supply to each organ may become compromised, causing
manifestations of CVD (4,20). Atherosclerosis is the main cause of
the high mortality rates of CVD (21). When CVD occurs in the body, the CRP
levels increase; therefore, it may be inferred that there is an
association between CRP and CVD (22-29).
Based on a large number of animal experiments and clinical studies,
CRP is a pathogenic factor that warrants further investigation
(27,30-34).
The association between CVD and CRP, and whether CRP can be used as
a novel marker or target for the treatment of CVD, must be further
verified in animal experiments and clinical studies.
Mice, rats and rabbits are frequently used to
construct animal models in several preclinical studies
investigating CVD (35), whereas the
majority of the animal models that study CRP use mice and rabbits
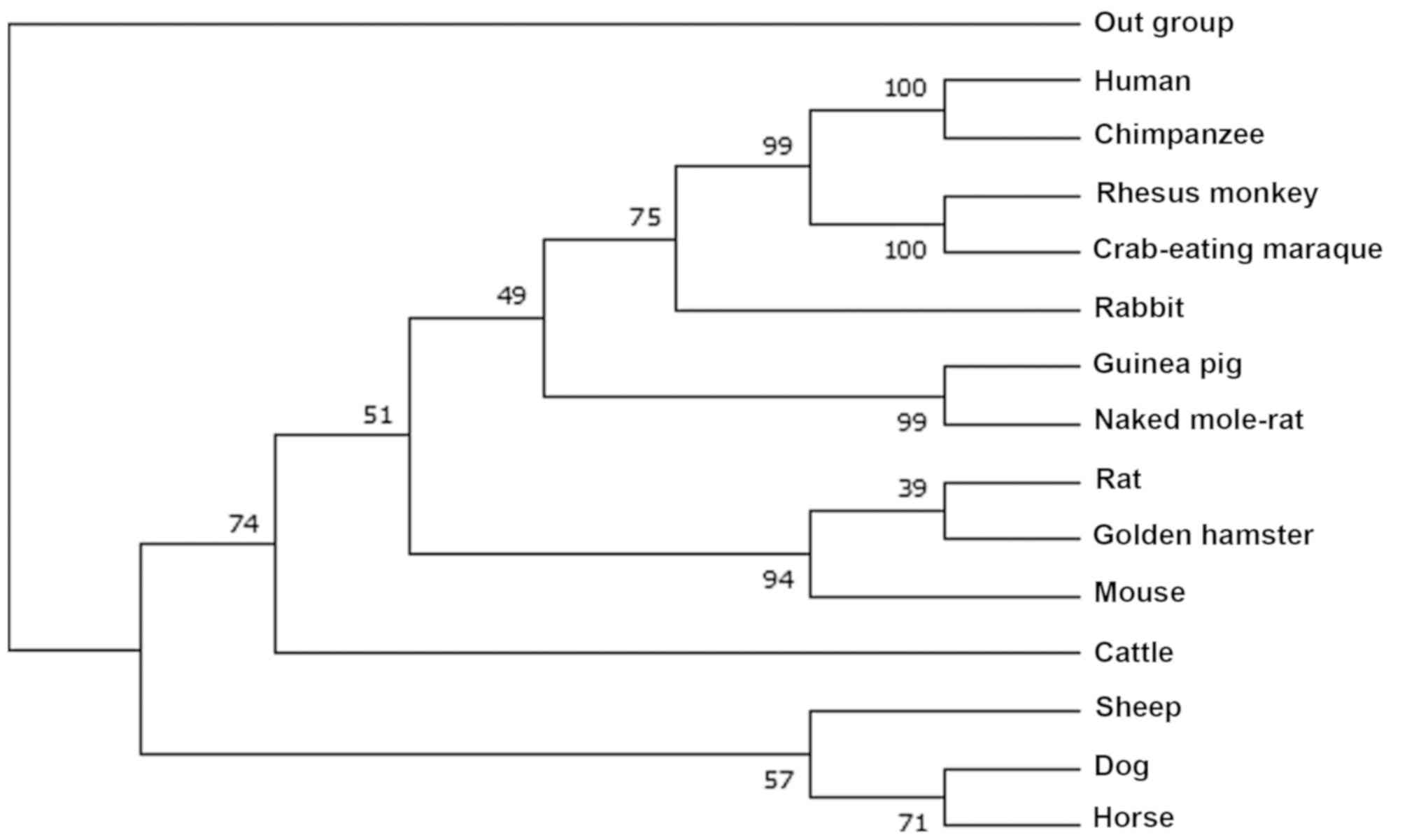
(36). To reveal the phylogenetic
relationships of CRP, the CRP protein sequence of 14 most
frequently used animal models in CVD research, including human
(NP_000558.2), chimpanzee (XP_001170732.2), Rhesus monkey
(XP_001117250.2), crab-eating macaque (NP_001306322.1), rabbit
(NP_001075734.1), guinea pig (XP_003466601.1), naked mole-rat
(XP_004858808.1), rat (NP_058792.1), golden hamster
(XP_005078251.1), mouse (NP_031794.3), cattle (NP_001137569.1),
sheep (XP_027821246.1), dog (NP_001301045.1), horse
(XP_023496680.1) were downloaded from the NCBI protein database
(https://www.ncbi.nlm.nih.gov/protein/). Subsequently,
the phylogenetic tree of maximum likelihood was constructed using
MEGA7(37) (Fig. 1). Except for non-human primates, it
may be inferred that rabbits and humans were placed in the same
cluster. Rats and mice were in relatively far clusters, suggesting
the genetic priority of rabbits and non-human primates as animal
models in studies of CRP-related CVD.
There is controversy regarding the association
between CRP and CVD in animal experiments. Several studies have
demonstrated that CRP can promote the pathological process of
atherosclerosis (30,31,38).
Using a rat carotid angioplasty model, an experiment revealed that
CRP can promote the migration and proliferation of vascular smooth
muscle cells, an increase in the collagen content and the
production of neointima (38). Paul
et al (30) also suggested
that human CRP over expression accelerates the progression of
atherosclerosis in apolipoprotein E knockout (ApoE-/-)
mice and that CRP in lesions is associated with increased C3,
angiotensin type 1 receptor (AT1-R), vascular cell adhesion
molecule 1 and collagen content. However, a previous study by
Hirschfield et al (39)
demonstrated that after 56 weeks of observation, male
ApoE-/- mice expressing human CRP did not display
promotion of the development of atherosclerosis, but human CRP and
mouse complement deposition were found in the plaques. Of note, it
has been previously suggested that human CRP does not promote
atherosclerosis, but rather may reduce the development of
atherosclerosis (40). By contrast,
Teupser et al (41) suggested
that the absence of CRP in mice exacerbates atherosclerotic
lesions.
Our group at the Research Institute of
Atherosclerotic Disease has also performed animal studies to
explore the role of CRP in CVD (31,42).
High-cholesterol feed was used to induce atherosclerosis in rabbits
and the association between CRP and atherosclerosis was
investigated. The results demonstrated that the CRP content was
positively correlated with the size of the atherosclerotic lesions
(31). When an acute embolic stroke
occurs in rabbits, the level of CRP in the plasma increases with
increasing infarct size, and the CRP level in the plasma is closely
associated with the area occupied by the infarcted lesion (42). In addition, we also found that
decreased plasma CRP levels did not affect the development of
atherosclerosis (43). These results
indicate the presence of a close association between CRP and
CVD.
However, several studies have failed to demonstrate
a correlation between CRP and atherosclerosis, and it has been
reported that CRP does not affect the development of
atherosclerosis (43-48).
Tennent et al (44) and
Reifenberg et al (45) found
no significant difference in the formation of atherosclerotic
lesions in ApoE-/- mice between transgenic human and
rabbit CRP. It has also been reported that CRP does not play a role
even in early atherosclerosis (46,47).
However, initial studies have revealed that mouse models for
studying CRP may carry certain disadvantages, as the CRP levels in
the plasma of mice stimulated by inflammation were markedly low
compared with those in humans and rabbits (49). Compared with mice, the lipoprotein
metabolism of rabbits and the response of CRP, an acute phase
reactant, were more similar to that in humans (50,51).
In subsequent animal experiments, researchers have
generally turned to the study of transgenic rabbits. Koike et
al (48) observed that CRP did
not affect the formation of aortic or coronary atherosclerotic
lesions in transgenic rabbits. This suggests that, even at higher
levels, CRP does not affect the occurrence and development of
atherosclerosis. We found that, although antisense oligonucleotides
to CRP were used to reduce the plasma level of CRP, the progression
of atherosclerosis in the aorta and coronary artery of rabbits was
not affected (43). Therefore, in
laboratory animals (mice, rats and rabbits) studies, it has not
been confirmed that an increase or decrease in CRP levels affects
the progression of atherosclerotic lesions. The major animal
studies between CRP and CVD are summarized in Table I. However, concerning the currently
available experimental studies, the results of mouse experiments
have been contradictory. Most researchers have not demonstrated
that CRP affects CVD lesions (39,41,44-47).
Therefore, the results of animal experiments have failed to
determine whether there is a correlation or a causal association
between CRP and CVD, and further studies are required.
A large volume of clinical data indicates that the
detection of hs-CRP is of predictive value in CVD (22-26)
and is also a risk factor and biomarker for CVD (27-29,52).
Studies have demonstrated that the detection of CRP levels may help
identify early complications in patients with acute myocardial
infarction and acute coronary artery disease (33,34).
Similarly, Hutchinson et al (53) found in early large-scale clinical
studies that age increases are directly proportional to CRP levels,
suggesting that CRP may be closely associated with an increased
risk of CVD. Ridker et al (27) monitored the CRP levels of 27,939
patients for up to 8 years and suggested that the probability of
CVD increased with increasing CRP levels. In subsequent study, a
follow-up analysis of >6,000 patients revealed an increased risk
of acute cardiovascular events in patients with higher CRP levels
(54). These larger population
studies have suggested that CRP may be a predictor of CVD.
For patients with stable or unstable angina,
detecting serum CRP levels may also predict coronary events
(55), and real-time detection of
CRP plasma levels in patients with unstable angina after discharge
can effectively predict the risk of recurrent coronary events
(56). Therefore, CRP can predict
the severity of CVD and the detection of the CRP levels may
effectively prevent CVD (27,57,58).
However, whether CRP is merely a predictive biomarker of
inflammation in CVD, or whether reducing the level of CRP is
beneficial in the treatment of CVD, have yet to be clearly
determined. Previous studies have demonstrated that long-term use
of statins can indeed reduce serum CRP levels in patients with
acute myocardial infarction, which may prove beneficial in the
treatment of acute myocardial infarction (52,59). In
the well-known Justification for use of statins in prevention: An
intervention trial evaluating Rosuvastatin (JUPITER) trial, the use
of statins significantly reduced the level of CRP in patients by
37%, while the level of cholesterol was also significantly reduced,
leading to a lower incidence of CVD (60). This result has also been reported in
other clinical studies (59,61-64).
However, the JUPITER study did not clearly
demonstrate whether the cause of CVD protection was a decrease in
cholesterol or a consequence of a decrease in CRP levels. A
previous study reported that CRP appeared to predict CVD better
than low-density lipoprotein cholesterol levels (27). Earlier studies have also reported
that CRP and interleukin-6 are strongly associated with an
increased risk of CVD (22,25). This hypothesis was further confirmed
by Ridker et al (65) in the
recent Canakinumab antiinflammatory thrombosis outcome study
(CANTOS) trial study, where patients with a history of myocardial
infarction were treated with canakinumab, an anti-inflammatory
human monoclonal antibody targeting interleukin-1β. Canakinumab
treatment significantly reduced the level of CRP in plasma without
lowering lipid levels in vivo, thereby reducing the
incidence of recurrent CVD. This is a significant finding, showing
a potential new method for the treatment of atherosclerotic
diseases in the future. There is a close association between CRP
and CVD: The detection of CRP levels may better predict the
incidence of CVD and a decrease in CRP levels may lead to a reduced
risk of CVD. A summary of the results of previous major clinical
studies is shown in Table II.
As for the association between CRP and CVD, CRP has
been confirmed as a predictor of CVD. However, the causal
relationship between CRP and CVD has yet to be confirmed. The
results of animal and clinical studies to date have been
contentious. Due to the differences between animals and humans, the
results of animal models require further research. CRP has long
been used in clinical research as an acute phase protein, and CRP
detection shows predictive value in CVD research (27,57).
Several researchers have classified CRP as a clinical predictor of
CVD (56,104-106).
However, CRP has been found to be associated with the function of
endothelial cells, monocytes/macrophages and smooth muscle cells,
and it has also been detected in atherosclerotic plaques (38,81,85,90,92,97).
Previous studies have demonstrated that CRP is produced by the
liver and it is released in the blood and delivered to the
corresponding tissue when there are inflammatory symptoms (107-110).
However, whether there is another source of CRP remains unknown. If
CRP can promote the migration and proliferation of endothelial
cells, monocytes/macrophages and vascular smooth muscle cells, and
then activate the complement system and participate in the
occurrence of CVD, the association between CRP and CVD would
constitute a major discovery. However, most researchers believe
that the involvement of CRP in the pathogenesis of atherosclerosis
by activating endothelial cells requires further confirmation.
Based on the current experimental results, the causal association
between CRP and CVD is uncertain. Research has long been performed
using mouse models, but these models carry certain disadvantages
when studying the association between CRP and CVD (45,111,112).
In order to better simulate the human inflammatory response, better
animal models must be designed, to simulate the overall or local
mechanisms of action of CRP. Currently, the role of CRP in
inflammation depends on synthetic sources (113), which may be the key to the current
controversy between CRP and CVD. The results of this study show
that CRP secreted by the liver is difficult to enter extrahepatic
tissues, so CRP may be produced by extrahepatic tissues and
transported back to the blood (113).
However, other animal models are required for future
studies, including rabbits and non-human primates. Animal model
studies using different species are valuable. However, these animal
models are all systemic studies, so it is unknown whether the local
effects caused by the expression or deletion of genes in animal
models can more closely simulate human disease. There is evidence
that the level of circulating CRP mainly reflects the underlying
inflammatory state, the expression of local CRP is closely
associated with the development of the disease, and with locally
increased CRP at different sites potentially causing inflammation
(114). Therefore, studying the
local effects of CRP may be a better model of human disease. The
clinical CANTOS experiment was the first to demonstrate that CVD
can be effectively treated by anti-inflammatory drugs and that by
reducing the level of CRP, it may be possible to reduce the risk of
CVD (65). However, there is a
limitation in that the risk of CVD is reduced following
anti-inflammatory therapy, but this inflammatory suppression may
affect the treatment of other diseases. This requires more thorough
research in the clinical setting.
In animal and clinical studies, CRP plays an
important role in CVD. Although the CANTOS study shows that drugs
can reduce CRP levels and the risk of CVD (65), its cardiovascular effects have not
been clearly determined. A large number of animal studies and
clinical conclusions have confirmed CRP as a biomarker, but whether
CRP suppression exerts cardiovascular protective effects and
whether it affects the occurrence and development of other diseases
requires further comprehensive assessment.
Not applicable.
No funding was received.
The datasets generated and/or analyzed during the
current study are available in the NCBI protein database,
[https://www.ncbi.nlm.nih.gov/protein/. human
(NP_000558.2), chimpanzee (XP_001170732.2), Rhesus monkey
(XP_001117250.2), crab-eating macaque (NP_001306322.1), rabbit
(NP_001075734.1), guinea pig (XP_003466601.1), naked mole-rat
(XP_004858808.1), rat (NP_058792.1), golden hamster
(XP_005078251.1), mouse (NP_031794.3), cattle (NP_001137569.1),
sheep (XP_027821246.1), dog (NP_001301045.1), horse
(XP_023496680.1)].
YF wrote the manuscript. YW and EL reviewed and
revised the manuscript. All authors read and approved the final
manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Thomas H, Diamond J, Vieco A, Chaudhuri S,
Shinnar E, Cromer S, Perel P, Mensah GA, Narula J, Johnson CO, et
al: Global Atlas of Cardiovascular Disease 2000-2016: The Path to
Prevention and Control. Glob Heart. 13:143–163. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mortality GBD: Global, regional, and
national age - sex specific all-cause and cause-specific mortality
for 240 causes of death, 1990-2013: A systematic analysis for the
Global Burden of Disease Study 2013. Lancet. 385:117–171.
2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
GBD 2015 Mortality and Causes of Death
Collaborators. Global, regional, and national life expectancy,
all-cause mortality, and cause-specific mortality for 249 causes of
death, 1980-2015: A systematic analysis for the Global Burden of
Disease Study 2015. Lancet. 388:1459–1544. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Ross R: Atherosclerosis - an inflammatory
disease. N Engl J Med. 340:115–126. 1999.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Tillett WS and Francis T Jr: Serological
reactions in pneumonia with a non-protein somatic fraction of
pneumococcus. J Exp Med. 52:561–571. 1930.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Taylor AW, Ku NO and Mortensen RF:
Regulation of cytokine-induced human C-reactive protein production
by transforming growth factor-beta. J Immunol. 145:2507–2513.
1990.PubMed/NCBI
|
|
7
|
Thompson D, Pepys MB and Wood SP: The
physiological structure of human C-reactive protein and its complex
with phosphocholine. Structure. 7:169–177. 1999.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Pepys MB and Baltz ML: Acute phase
proteins with special reference to C-reactive protein and related
proteins (pentaxins) and serum amyloid A protein. Adv Immunol.
34:141–212. 1983.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Shine B, de Beer FC and Pepys MB: Solid
phase radioimmunoassays for human C-reactive protein. Clin Chim
Acta. 117:13–23. 1981.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Pepys MB and Hirschfield GM: C-reactive
protein: A critical update. J Clin Invest. 111:1805–1812.
2003.PubMed/NCBI View
Article : Google Scholar
|
|
11
|
Volanakis JE and Kaplan MH: Interaction of
C-reactive protein complexes with the complement system II.
Consumption of guinea pig complement by CRP complexes: Requirement
for human C1q. J Immunol. 113:9–17. 1974.PubMed/NCBI
|
|
12
|
Claus DR, Siegel J, Petras K, Osmand AP
and Gewurz H: Interactions of C-reactive protein with the first
component of human complement. J Immunol. 119:187–192.
1977.PubMed/NCBI
|
|
13
|
Moutachakkir M, Lamrani Hanchi A, Baraou
A, Boukhira A and Chellak S: Immunoanalytical characteristics of
C-reactive protein and high sensitivity C-reactive protein. Ann
Biol Clin (Paris). 75:225–229. 2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Calabrò P, Golia E and Yeh ET: CRP and the
risk of atherosclerotic events. Semin Immunopathol. 31:79–94.
2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Koenig W: High-sensitivity C-reactive
protein and atherosclerotic disease: From improved risk prediction
to risk-guided therapy. Int J Cardiol. 168:5126–5134.
2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Pearson TA, Mensah GA, Alexander RW,
Anderson JL, Cannon RO III, Criqui M, Fadl YY, Fortmann SP, Hong Y,
Myers GL, et al: Centers for Disease Control and Prevention;
American Heart Association: Markers of inflammation and
cardiovascular disease: application to clinical and public health
practice: A statement for healthcare professionals from the Centers
for Disease Control and Prevention and the American Heart
Association. Circulation. 107:499–511. 2003.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ridker PM: Clinical application of
C-reactive protein for cardiovascular disease detection and
prevention. Circulation. 107:363–369. 2003.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Kaptoge S, Di Angelantonio E, Lowe G,
Pepys MB, Thompson SG, Collins R and Danesh J: Emerging Risk
Factors Collaboration: C-reactive protein concentration and risk of
coronary heart disease, stroke, and mortality: An individual
participant meta-analysis. Lancet. 375:132–140. 2010.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Jousilahti P, Vartiainen E, Tuomilehto J
and Puska P: Sex, age, cardiovascular risk factors, and coronary
heart disease: A prospective follow-up study of 14 786 middle-aged
men and women in Finland. Circulation. 99:1165–1172.
1999.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Ross R: The pathogenesis of
atherosclerosis: A perspective for the 1990s. Nature. 362:801–809.
1993.PubMed/NCBI View
Article : Google Scholar
|
|
21
|
Frostegård J: Immunity, atherosclerosis
and cardiovascular disease. BMC Med. 11(117)2013.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Ridker PM, Cushman M, Stampfer MJ, Tracy
RP and Hennekens CH: Inflammation, aspirin, and the risk of
cardiovascular disease in apparently healthy men. N Engl J Med.
336:973–979. 1997.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Koenig W, Sund M, Fröhlich M, Fischer HG,
Löwel H, Döring A, Hutchinson WL and Pepys MB: C-Reactive protein,
a sensitive marker of inflammation, predicts future risk of
coronary heart disease in initially healthy middle-aged men:
Results from the MONICA (Monitoring Trends and Determinants in
Cardiovascular Disease) Augsburg Cohort Study, 1984 to 1992.
Circulation. 99:237–242. 1999.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Danesh J, Whincup P, Walker M, Lennon L,
Thomson A, Appleby P, Gallimore JR and Pepys MB: Low grade
inflammation and coronary heart disease: Prospective study and
updated meta-analyses. BMJ. 321:199–204. 2000.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Ridker PM, Hennekens CH, Buring JE and
Rifai N: C-reactive protein and other markers of inflammation in
the prediction of cardiovascular disease in women. N Engl J Med.
342:836–843. 2000.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Ridker PM: C-reactive protein and the
prediction of cardiovascular events among those at intermediate
risk: Moving an inflammatory hypothesis toward consensus. J Am Coll
Cardiol. 49:2129–2138. 2007.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ridker PM, Rifai N, Rose L, Buring JE and
Cook NR: Comparison of C-reactive protein and low-density
lipoprotein cholesterol levels in the prediction of first
cardiovascular events. N Engl J Med. 347:1557–1565. 2002.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Shah PK: Circulating markers of
inflammation for vascular risk prediction: Are they ready for prime
time. Circulation. 101:1758–1759. 2000.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Lagrand WK, Visser CA, Hermens WT, Niessen
HW, Verheugt FW, Wolbink GJ and Hack CE: C-reactive protein as a
cardiovascular risk factor: More than an epiphenomenon?
Circulation. 100:96–102. 1999.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Paul A, Ko KW, Li L, Yechoor V, McCrory
MA, Szalai AJ and Chan L: C-reactive protein accelerates the
progression of atherosclerosis in apolipoprotein E-deficient mice.
Circulation. 109:647–655. 2004.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Yu Q, Li Y, Wang Y, Zhao S, Yang P, Chen
Y, Fan J and Liu E: C-reactive protein levels are associated with
the progression of atherosclerotic lesions in rabbits. Histol
Histopathol. 27:529–535. 2012.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Sun H, Koike T, Ichikawa T, Hatakeyama K,
Shiomi M, Zhang B, Kitajima S, Morimoto M, Watanabe T, Asada Y, et
al: C-reactive protein in atherosclerotic lesions: Its origin and
pathophysiological significance. Am J Pathol. 167:1139–1148.
2005.PubMed/NCBI View Article : Google Scholar
|
|
33
|
de Beer FC, Hind CR, Fox KM, Allan RM,
Maseri A and Pepys MB: Measurement of serum C-reactive protein
concentration in myocardial ischaemia and infarction. Br Heart J.
47:239–243. 1982.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Berk BC, Weintraub WS and Alexander RW:
Elevation of C-reactive protein in ‘active’ coronary artery
disease. Am J Cardiol. 65:168–172. 1990.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Zaragoza C, Gomez-Guerrero C,
Martin-Ventura JL, Blanco-Colio L, Lavin B, Mallavia B, Tarin C,
Mas S, Ortiz A and Egido J: Animal models of cardiovascular
diseases. J Biomed Biotechnol. 2011(497841)2011.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Torzewski M, Waqar AB and Fan J: Animal
models of C-reactive protein. Mediators Inflamm.
2014(683598)2014.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Kumar S, Stecher G and Tamura K: MEGA7:
Molecular Evolutionary Genetics Analysis Version 7.0 for Bigger
Datasets. Mol Biol Evol. 33:1870–1874. 2016.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Wang CH, Li SH, Weisel RD, Fedak PW,
Dumont AS, Szmitko P, Li RK, Mickle DA and Verma S: C-reactive
protein upregulates angiotensin type 1 receptors in vascular smooth
muscle. Circulation. 107:1783–1790. 2003.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Hirschfield GM, Gallimore JR, Kahan MC,
Hutchinson WL, Sabin CA, Benson GM, Dhillon AP, Tennent GA and
Pepys MB: Transgenic human C-reactive protein is not proatherogenic
in apolipoprotein E-deficient mice. Proc Natl Acad Sci USA.
102:8309–8314. 2005.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Kovacs A, Tornvall P, Nilsson R, Tegnér J,
Hamsten A and Björkegren J: Human C-reactive protein slows
atherosclerosis development in a mouse model with human-like
hypercholesterolemia. Proc Natl Acad Sci USA. 104:13768–13773.
2007.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Teupser D, Weber O, Rao TN, Sass K, Thiery
J and Fehling HJ: No reduction of atherosclerosis in C-reactive
protein (CRP)-deficient mice. J Biol Chem. 286:6272–6279.
2011.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Yu Q, Lin Y, Yang P, Wang Y, Zhao S, Yang
P, Fan J and Liu E: C-reactive protein is associated with the
progression of acute embolic stroke in rabbit model. J Thromb
Thrombolysis. 33:301–307. 2012.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Yu Q, Liu Z, Waqar AB, Ning B, Yang X,
Shiomi M, Graham MJ, Crooke RM, Liu E, Dong S, et al: Effects of
antisense oligonucleotides against C-reactive protein on the
development of atherosclerosis in WHHL rabbits. Mediators Inflamm.
2014(979132)2014.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Tennent GA, Hutchinson WL, Kahan MC,
Hirschfield GM, Gallimore JR, Lewin J, Sabin CA, Dhillon AP and
Pepys MB: Transgenic human CRP is not pro-atherogenic,
pro-atherothrombotic or pro-inflammatory in apoE-/-
mice. Atherosclerosis. 196:248–255. 2008.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Reifenberg K, Lehr HA, Baskal D, Wiese E,
Schaefer SC, Black S, Samols D, Torzewski M, Lackner KJ, Husmann M,
et al: Role of C-reactive protein in atherogenesis: Can the
apolipoprotein E knockout mouse provide the answer? Arterioscler
Thromb Vasc Biol. 25:1641–1646. 2005.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Torzewski M, Reifenberg K, Cheng F, Wiese
E, Küpper I, Crain J, Lackner KJ and Bhakdi S: No effect of
C-reactive protein on early atherosclerosis in LDLR-/- /
human C-reactive protein transgenic mice. Thromb Haemost.
99:196–201. 2008.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Trion A, de Maat MP, Jukema JW, van der
Laarse A, Maas MC, Offerman EH, Havekes LM, Szalai AJ, Princen HM
and Emeis JJ: No effect of C-reactive protein on early
atherosclerosis development in apolipoprotein E*3-leiden/human
C-reactive protein transgenic mice. Arterioscler Thromb Vasc Biol.
25:1635–1640. 2005.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Koike T, Kitajima S, Yu Y, Nishijima K,
Zhang J, Ozaki Y, Morimoto M, Watanabe T, Bhakdi S, Asada Y, et al:
Human C-reactive protein does not promote atherosclerosis in
transgenic rabbits. Circulation. 120:2088–2094. 2009.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Pepys MB, Baltz M, Gomer K, Davies AJ and
Doenhoff M: Serum amyloid P-component is an acute-phase reactant in
the mouse. Nature. 278:259–261. 1979.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Fan J, Kitajima S, Watanabe T, Xu J, Zhang
J, Liu E and Chen YE: Rabbit models for the study of human
atherosclerosis: From pathophysiological mechanisms to
translational medicine. Pharmacol Ther. 146:104–119.
2015.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Kushner I and Feldmann G: Control of the
acute phase response Demonstration of C-reactive protein synthesis
and secretion by hepatocytes during acute inflammation in the
rabbit. J Exp Med. 148:466–477. 1978.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Ridker PM, Rifai N, Pfeffer MA, Sacks F
and Braunwald E: The Cholesterol and Recurrent Events (CARE)
Investigators. Long-term effects of pravastatin on plasma
concentration of C-reactive protein. Circulation. 100:230–235.
1999.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Hutchinson WL, Koenig W, Fröhlich M, Sund
M, Lowe GD and Pepys MB: Immunoradiometric assay of circulating
C-reactive protein: Age-related values in the adult general
population. Clin Chem. 46:934–938. 2000.PubMed/NCBI
|
|
54
|
Danesh J, Wheeler JG, Hirschfield GM, Eda
S, Eiriksdottir G, Rumley A, Lowe GD, Pepys MB and Gudnason V:
C-reactive protein and other circulating markers of inflammation in
the prediction of coronary heart disease. N Engl J Med.
350:1387–1397. 2004.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Haverkate F, Thompson SG, Pyke SD,
Gallimore JR and Pepys MB: European Concerted Action on Thrombosis
and Disabilities Angina Pectoris Study Group. Production of
C-reactive protein and risk of coronary events in stable and
unstable angina. Lancet. 349:462–466. 1997.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Biasucci LM, Liuzzo G, Grillo RL,
Caligiuri G, Rebuzzi AG, Buffon A, Summaria F, Ginnetti F, Fadda G
and Maseri A: Elevated levels of C-reactive protein at discharge in
patients with unstable angina predict recurrent instability.
Circulation. 99:855–860. 1999.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Ridker PM: C-reactive protein and risks of
future myocardial infarction and thrombotic stroke. Eur Heart J.
19:1–3. 1998.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Liuzzo G, Biasucci LM, Gallimore JR,
Grillo RL, Rebuzzi AG, Pepys MB and Maseri A: The prognostic value
of C-reactive protein and serum amyloid a protein in severe
unstable angina. N Engl J Med. 331:417–424. 1994.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Ridker PM, Cannon CP, Morrow D, Rifai N,
Rose LM, McCabe CH, Pfeffer MA and Braunwald E: Pravastatin or
Atorvastatin Evaluation and Infection Therapy-Thrombolysis in
Myocardial Infarction 22 (PROVE IT-TIMI 22) Investigators.
C-reactive protein levels and outcomes after statin therapy. N Engl
J Med. 352:20–28. 2005.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Ridker PM, Danielson E, Fonseca FA, Genest
J, Gotto AM Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ,
MacFadyen JG, et al: JUPITER Study Group: Rosuvastatin to prevent
vascular events in men and women with elevated C-reactive protein.
N Engl J Med. 359:2195–2207. 2008.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Ridker PM, Rifai N, Pfeffer MA, Sacks FM,
Moye LA, Goldman S, Flaker GC and Braunwald E: Cholesterol and
Recurrent Events (CARE) Investigators. Inflammation, pravastatin,
and the risk of coronary events after myocardial infarction in
patients with average cholesterol levels. Circulation. 98:839–844.
1998.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Ridker PM, Rifai N, Clearfield M, Downs
JR, Weis SE, Miles JS and Gotto AM Jr: Air Force/Texas Coronary
Atherosclerosis Prevention Study Investigators. Measurement of
C-reactive protein for the targeting of statin therapy in the
primary prevention of acute coronary events. N Engl J Med.
344:1959–1965. 2001.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Nissen SE, Tuzcu EM, Schoenhagen P, Crowe
T, Sasiela WJ, Tsai J, Orazem J, Magorien RD, O'Shaughnessy C and
Ganz P: Reversal of Atherosclerosis with Aggressive Lipid Lowering
(REVERSAL) Investigators. Statin therapy, LDL cholesterol,
C-reactive protein, and coronary artery disease. N Engl J Med.
352:29–38. 2005.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Bohula EA, Giugliano RP, Cannon CP, Zhou
J, Murphy SA, White JA, Tershakovec AM, Blazing MA and Braunwald E:
Achievement of dual low-density lipoprotein cholesterol and
high-sensitivity C-reactive protein targets more frequent with the
addition of ezetimibe to simvastatin and associated with better
outcomes in IMPROVE-IT. Circulation. 132:1224–1233. 2015.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Ridker PM, Everett BM, Thuren T, MacFadyen
JG, Chang WH, Ballantyne C, Fonseca F, Nicolau J, Koenig W, Anker
SD, et al: CANTOS Trial Group: Antiinflammatory therapy with
Canakinumab for atherosclerotic disease. N Engl J Med.
377:1119–1131. 2017.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Jialal I, Devaraj S and Venugopal SK:
C-reactive protein: Risk marker or mediator in atherothrombosis?
Hypertension. 44:6–11. 2004.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Labarrere CA and Zaloga GP: C-reactive
protein: From innocent bystander to pivotal mediator of
atherosclerosis. Am J Med. 117:499–507. 2004.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Verma S, Devaraj S and Jialal I: Is
C-reactive protein an innocent bystander or proatherogenic culprit?
C-reactive protein promotes atherothrombosis. Circulation.
113:2135–2150; discussion 2150. 2006.PubMed/NCBI
|
|
69
|
Pasceri V, Cheng JS, Willerson JT and Yeh
ET: Modulation of C-reactive protein-mediated monocyte
chemoattractant protein-1 induction in human endothelial cells by
anti-atherosclerosis drugs. Circulation. 103:2531–2534.
2001.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Boring L, Gosling J, Cleary M and Charo
IF: Decreased lesion formation in CCR2-/- mice reveals a
role for chemokines in the initiation of atherosclerosis. Nature.
394:894–897. 1998.PubMed/NCBI View
Article : Google Scholar
|
|
71
|
Gu L, Okada Y, Clinton SK, Gerard C,
Sukhova GK, Libby P and Rollins BJ: Absence of monocyte
chemoattractant protein-1 reduces atherosclerosis in low density
lipoprotein receptor-deficient mice. Mol Cell. 2:275–281.
1998.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Pasceri V, Willerson JT and Yeh ET: Direct
proinflammatory effect of C-reactive protein on human endothelial
cells. Circulation. 102:2165–2168. 2000.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Qamirani E, Ren Y, Kuo L and Hein TW:
C-reactive protein inhibits endothelium-dependent NO-mediated
dilation in coronary arterioles by activating p38 kinase and
NAD(P)H oxidase. Arterioscler Thromb Vasc Biol. 25:995–1001.
2005.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Devaraj S, Yun JM, Adamson G, Galvez J and
Jialal I: C-reactive protein impairs the endothelial glycocalyx
resulting in endothelial dysfunction. Cardiovasc Res. 84:479–484.
2009.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Hein TW, Singh U, Vasquez-Vivar J, Devaraj
S, Kuo L and Jialal I: Human C-reactive protein induces endothelial
dysfunction and uncoupling of eNOS in vivo. Atherosclerosis.
206:61–68. 2009.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Devaraj S, Kumaresan PR and Jialal I:
C-reactive protein induces release of both endothelial
microparticles and circulating endothelial cells in vitro and in
vivo: Further evidence of endothelial dysfunction. Clin Chem.
57:1757–1761. 2011.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Venugopal SK, Devaraj S, Yuhanna I, Shaul
P and Jialal I: Demonstration that C-reactive protein decreases
eNOS expression and bioactivity in human aortic endothelial cells.
Circulation. 106:1439–1441. 2002.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Verma S, Kuliszewski MA, Li SH, Szmitko
PE, Zucco L, Wang CH, Badiwala MV, Mickle DA, Weisel RD, Fedak PW,
et al: C-reactive protein attenuates endothelial progenitor cell
survival, differentiation, and function: Further evidence of a
mechanistic link between C-reactive protein and cardiovascular
disease. Circulation. 109:2058–2067. 2004.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Verma S, Li SH, Badiwala MV, Weisel RD,
Fedak PW, Li RK, Dhillon B and Mickle DA: Endothelin antagonism and
interleukin-6 inhibition attenuate the proatherogenic effects of
C-reactive protein. Circulation. 105:1890–1896. 2002.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Verma S, Wang CH, Li SH, Dumont AS, Fedak
PW, Badiwala MV, Dhillon B, Weisel RD, Li RK, Mickle DA, et al: A
self-fulfilling prophecy: C-reactive protein attenuates nitric
oxide production and inhibits angiogenesis. Circulation.
106:913–919. 2002.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Teoh H, Quan A, Lovren F, Wang G, Tirgari
S, Szmitko PE, Szalai AJ, Ward ME and Verma S: Impaired endothelial
function in C-reactive protein overexpressing mice.
Atherosclerosis. 201:318–325. 2008.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Fichtlscherer S, Rosenberger G, Walter DH,
Breuer S, Dimmeler S and Zeiher AM: Elevated C-reactive protein
levels and impaired endothelial vasoreactivity in patients with
coronary artery disease. Circulation. 102:1000–1006.
2000.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Tomai F, Crea F, Gaspardone A, Versaci F,
Ghini AS, Chiariello L and Gioffrè PA: Unstable angina and elevated
c-reactive protein levels predict enhanced vasoreactivity of the
culprit lesion. Circulation. 104:1471–1476. 2001.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Cleland SJ, Sattar N, Petrie JR, Forouhi
NG, Elliott HL and Connell JM: Endothelial dysfunction as a
possible link between C-reactive protein levels and cardiovascular
disease. Clin Sci (Lond). 98:531–535. 2000.PubMed/NCBI
|
|
85
|
Devaraj S, Kumaresan PR and Jialal I:
Effect of C-reactive protein on chemokine expression in human
aortic endothelial cells. J Mol Cell Cardiol. 36:405–410.
2004.PubMed/NCBI View Article : Google Scholar
|
|
86
|
Tabas I, García-Cardeña G and Owens GK:
Recent insights into the cellular biology of atherosclerosis. J
Cell Biol. 209:13–22. 2015.PubMed/NCBI View Article : Google Scholar
|
|
87
|
Calabró P, Willerson JT and Yeh ET:
Inflammatory cytokines stimulated C-reactive protein production by
human coronary artery smooth muscle cells. Circulation.
108:1930–1932. 2003.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Chistiakov DA, Orekhov AN and Bobryshev
YV: Vascular smooth muscle cell in atherosclerosis. Acta Physiol
(Oxf). 214:33–50. 2015.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Ryu J, Lee CW, Shin JA, Park CS, Kim JJ,
Park SJ and Han KH: FcgammaRIIa mediates C-reactive protein-induced
inflammatory responses of human vascular smooth muscle cells by
activating NADPH oxidase 4. Cardiovasc Res. 75:555–565.
2007.PubMed/NCBI View Article : Google Scholar
|
|
90
|
Liu N, Liu J, Ji Y, Lu P, Wang C and Guo
F: C-reactive protein induces TNF-α secretion by p38 MAPK-TLR4
signal pathway in rat vascular smooth muscle cells. Inflammation.
34:283–290. 2011.PubMed/NCBI View Article : Google Scholar
|
|
91
|
Liu N, Liu JT, Ji YY and Lu PP: C-reactive
protein triggers inflammatory responses partly via TLR4/IRF3/NF-κB
signaling pathway in rat vascular smooth muscle cells. Life Sci.
87:367–374. 2010.PubMed/NCBI View Article : Google Scholar
|
|
92
|
Cermak J, Key NS, Bach RR, Balla J, Jacob
HS and Vercellotti GM: C-reactive protein induces human peripheral
blood monocytes to synthesize tissue factor. Blood. 82:513–520.
1993.PubMed/NCBI
|
|
93
|
Nakagomi A, Freedman SB and Geczy CL:
Interferon-gamma and lipopolysaccharide potentiate monocyte tissue
factor induction by C-reactive prote in: Relationship with age,
sex, and hormone replacement treatment. Circulation. 101:1785–1791.
2000.PubMed/NCBI View Article : Google Scholar
|
|
94
|
Williams TN, Zhang CX, Game BA, He L and
Huang Y: C-reactive protein stimulates MMP-1 expression in U937
histiocytes through Fc[gamma]RII and extracellular signal-regulated
kinase pathway: An implication of CRP involvement in plaque
destabilization. Arterioscler Thromb Vasc Biol. 24:61–66.
2004.PubMed/NCBI View Article : Google Scholar
|
|
95
|
Ballou SP and Lozanski G: Induction of
inflammatory cytokine release from cultured human monocytes by
C-reactive protein. Cytokine. 4:361–368. 1992.PubMed/NCBI View Article : Google Scholar
|
|
96
|
Torzewski M, Rist C, Mortensen RF, Zwaka
TP, Bienek M, Waltenberger J, Koenig W, Schmitz G, Hombach V and
Torzewski J: C-reactive protein in the arterial intima: Role of
C-reactive protein receptor-dependent monocyte recruitment in
atherogenesis. Arterioscler Thromb Vasc Biol. 20:2094–2099.
2000.PubMed/NCBI View Article : Google Scholar
|
|
97
|
Reynolds GD and Vance RP: C-reactive
protein immunohistochemical localization in normal and
atherosclerotic human aortas. Arch Pathol Lab Med. 111:265–269.
1987.PubMed/NCBI
|
|
98
|
Yasojima K, Schwab C, McGeer EG and McGeer
PL: Generation of C-reactive protein and complement components in
atherosclerotic plaques. Am J Pathol. 158:1039–1051.
2001.PubMed/NCBI View Article : Google Scholar
|
|
99
|
Kobayashi S, Inoue N, Ohashi Y, Terashima
M, Matsui K, Mori T, Fujita H, Awano K, Kobayashi K, Azumi H, et
al: Interaction of oxidative stress and inflammatory response in
coronary plaque instability: Important role of C-reactive protein.
Arterioscler Thromb Vasc Biol. 23:1398–1404. 2003.PubMed/NCBI View Article : Google Scholar
|
|
100
|
Seifert PS and Kazatchkine MD: The
complement system in atherosclerosis. Atherosclerosis. 73:91–104.
1988.PubMed/NCBI View Article : Google Scholar
|
|
101
|
Torzewski J, Bowyer DE, Waltenberger J and
Fitzsimmons C: Processes in atherogenesis: Complement activation.
Atherosclerosis. 132:131–138. 1997.PubMed/NCBI View Article : Google Scholar
|
|
102
|
Niculescu F, Rus HG and Vlaicu R:
Immunohistochemical localization of C5b-9, S-protein, C3d and
apolipoprotein B in human arterial tissues with atherosclerosis.
Atherosclerosis. 65:1–11. 1987.PubMed/NCBI View Article : Google Scholar
|
|
103
|
Torzewski J, Torzewski M, Bowyer DE,
Fröhlich M, Koenig W, Waltenberger J, Fitzsimmons C and Hombach V:
C-reactive protein frequently colocalizes with the terminal
complement complex in the intima of early atherosclerotic lesions
of human coronary arteries. Arterioscler Thromb Vasc Biol.
18:1386–1392. 1998.PubMed/NCBI View Article : Google Scholar
|
|
104
|
Yousuf O, Mohanty BD, Martin SS, Joshi PH,
Blaha MJ, Nasir K, Blumenthal RS and Budoff MJ: High-sensitivity
C-reactive protein and cardiovascular disease: A resolute belief or
an elusive link? J Am Coll Cardiol. 62:397–408. 2013.PubMed/NCBI View Article : Google Scholar
|
|
105
|
Bielas H, Meister-Langraf RE, Schmid JP,
Barth J, Znoj H, Schnyder U, Princip M and von Känel R: C-reactive
protein as a predictor of posttraumatic stress induced by acute
myocardial infarction. Gen Hosp Psychiatry. 53:125–130.
2018.PubMed/NCBI View Article : Google Scholar
|
|
106
|
Best LG, Zhang Y, Lee ET, Yeh JL, Cowan L,
Palmieri V, Roman M, Devereux RB, Fabsitz RR, Tracy RP, et al:
C-reactive protein as a predictor of cardiovascular risk in a
population with a high prevalence of diabetes: The Strong Heart
Study. Circulation. 112:1289–1295. 2005.PubMed/NCBI View Article : Google Scholar
|
|
107
|
Hurlimann J, Thorbecke GJ and Hochwald GM:
The liver as the site of C-reactive protein formation. J Exp Med.
123:365–378. 1966.PubMed/NCBI View Article : Google Scholar
|
|
108
|
Eklund CM: Proinflammatory cytokines in
CRP baseline regulation. Adv Clin Chem. 48:111–136. 2009.PubMed/NCBI View Article : Google Scholar
|
|
109
|
Jensen HS: C-reactive protein. Ugeskr
Laeger. 162:2453–2456. 2000.PubMed/NCBI(In Danish).
|
|
110
|
Deban L, Bottazzi B, Garlanda C, de la
Torre YM and Mantovani A: Pentraxins: Multifunctional proteins at
the interface of innate immunity and inflammation. Biofactors.
35:138–145. 2009.PubMed/NCBI View Article : Google Scholar
|
|
111
|
Laskowitz DT, Lee DM, Schmechel D and
Staats HF: Altered immune responses in apolipoprotein E-deficient
mice. J Lipid Res. 41:613–620. 2000.PubMed/NCBI
|
|
112
|
Grainger DJ, Reckless J and McKilligin E:
Apolipoprotein E modulates clearance of apoptotic bodies in vitro
and in vivo, resulting in a systemic proinflammatory state in
apolipoprotein E-deficient mice. J Immunol. 173:6366–6375.
2004.PubMed/NCBI View Article : Google Scholar
|
|
113
|
Li HY, Liu XL, Liu YT, Jia ZK, Filep JG,
Potempa LA, Ji SR and Wu Y: Matrix sieving-enforced retrograde
transcytosis regulates tissue accumulation of C-reactive protein.
Cardiovasc Res. 115:440–452. 2019.PubMed/NCBI View Article : Google Scholar
|
|
114
|
Su HX, Zhou HH, Wang MY, Cheng J, Zhang
SC, Hui F, Chen XZ, Liu SH, Liu QJ, Zhu ZJ, et al: Mutations of
C-reactive protein (CRP) -286 SNP, APC and p53 in colorectal
cancer: Implication for a CRP-Wnt crosstalk. PLoS One.
9(e102418)2014.PubMed/NCBI View Article : Google Scholar
|