Introduction
Chest trauma is the second leading cause of
trauma-related deaths, accounting for 20-25% of all trauma-related
deaths (1). Multiple rib fractures,
especially in patients with flail chest, are often accompanied by
severe pain, chest wall softening, abnormal breathing and severe
lung contusion. As multiple rib fractures may easily lead to
respiratory failure and even threaten life, thoracic surgery is
often required. The surgical treatment of patients with flail chest
and >4 consecutive dislocated rib fractures has achieved
satisfactory results (2-5).
Since the ribs are flat bones in long arc shape, the surface area
of the chest is large, and the operation involves multiple ribs, a
large incision is required to obtain a satisfactory exposure of the
surgical field. Some chest wall muscles, blood vessels and nerves
are often injured during operation, resulting in increased
infection rate of the incision after operation, which easily leads
to dysfunction and skin numbness on the lateral chest wall. The
improvement of operation incision accuracy can reduce the injury to
chest wall muscles, peripheral blood vessels and nerves, save
operation time, reduce postoperative pain, and accelerate the
recovery of patients. Therefore, determining the incision before
operation is very important. In the present study, 80 patients with
rib fracture treated by internal fixation in Tianjin Hospital
Affiliated to Tianjin University (Tianjin, China) from May 2018 to
April 2019 were selected and divided into two groups. The patients
in the two groups were treated following different methods of rib
positioning before operation. The clinical value of using rib
surface positioning ruler (National Patent Application, patent no.
201920 189426.4) (6) combined with
volumetric CT measurement technique to determine the operative
incision was investigated.
Patients and methods
Clinical information
A total of 80 patients who received internal
fixation of rib fractures in Tianjin Hospital Affiliated to Tianjin
University from May 2018 to April 2019 were selected as research
subjects, including 47 males and 33 females. Patients were 25-73
years of age, with an average age of 44.5 years. There were 48
patients injured in traffic accidents, 17 patients injured after
falling from high places, 9 patients injured from falls, and 6
patients with severe crush injuries. All patients had multiple rib
fractures (≥4 with dislocation of the broken ends) and pulmonary
contusion after injury. Among them, 51 patients had flail chest or
local chest wall deformity. The patients were divided into two
groups, the experimental and the control group. In the experimental
group, 42 patients were treated with rib surface positioning ruler
combined with CT measurement method. In the control group, 38
patients were treated with traditional positioning method. There
was no significant difference in clinical data between the two
groups, as shown in Table I.
 | Table IComparison of general information
between the two groups of patients. |
Table I
Comparison of general information
between the two groups of patients.
| Group | Male/female | No. of fixed
bones | No. of fixed plates
used |
|---|
| Experimental
group | 25/17 | 4.96±1.18 | 5.02±1.02 |
| Control group | 22/16 | 4.76±1.04 | 5.08±1.16 |
| t/χ2 | 0.042 | 0.568 | 0.412 |
| P-value | 0.812 | 0.572 | 0.658 |
Indications and timing for
operation
Operation for multiple rib fractures with
dislocation of ≥4 broken ends should be performed 2-5 days after
injury. Patients with multiple injuries should receive surgical
treatment after their general condition was stable, but no more
than >7 days. Patients with severe abnormal breathing and flail
chest should be treated surgically in time.
Operation incision position
The position of the operation incision should first
meet the needs of surgery, and then ensure that the operation is
minimally invasive. Operation incision based on traditional
positioning and on the method of rib surface positioning ruler
combined with volumetric CT measurement was explored. Traditional
positioning group: Combined with three-dimensional (3D) CT imaging
and chest wall contusion marks, transverse or longitudinal incision
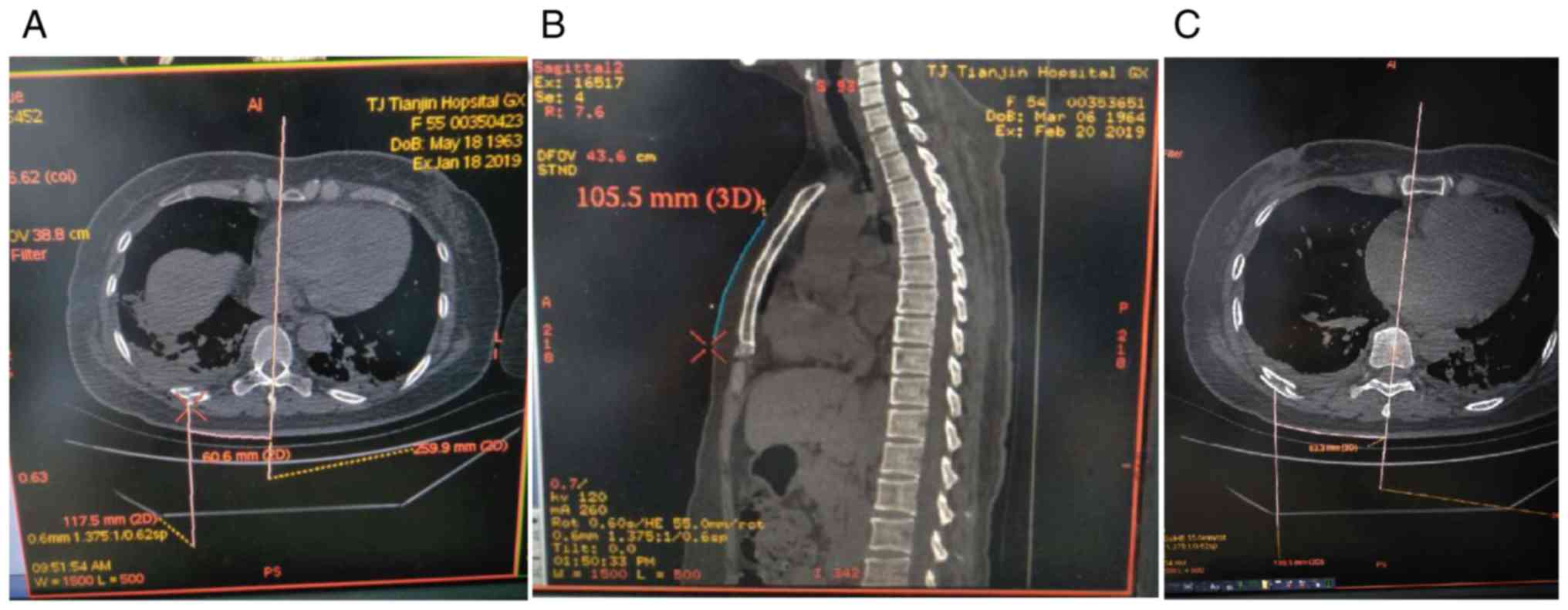
was made along the ribs. Method of rib surface positioning ruler:
Before operation, the surface distance between the fracture plane
of the ribs and the surface sign plane of the chest was measured as
the longitudinal coordinate in the fusion CT image system (the
distance between the anterior ribs and the sternum angle plane, the
distance between the posterior ribs and the body spinous process of
the cervical 7 vertebrae). The surface distance between the
fracture lines of the ribs and the midline of the human body was
measured as the transverse coordinate (the midline of the sternum
or spinous process of the spine) (Fig.
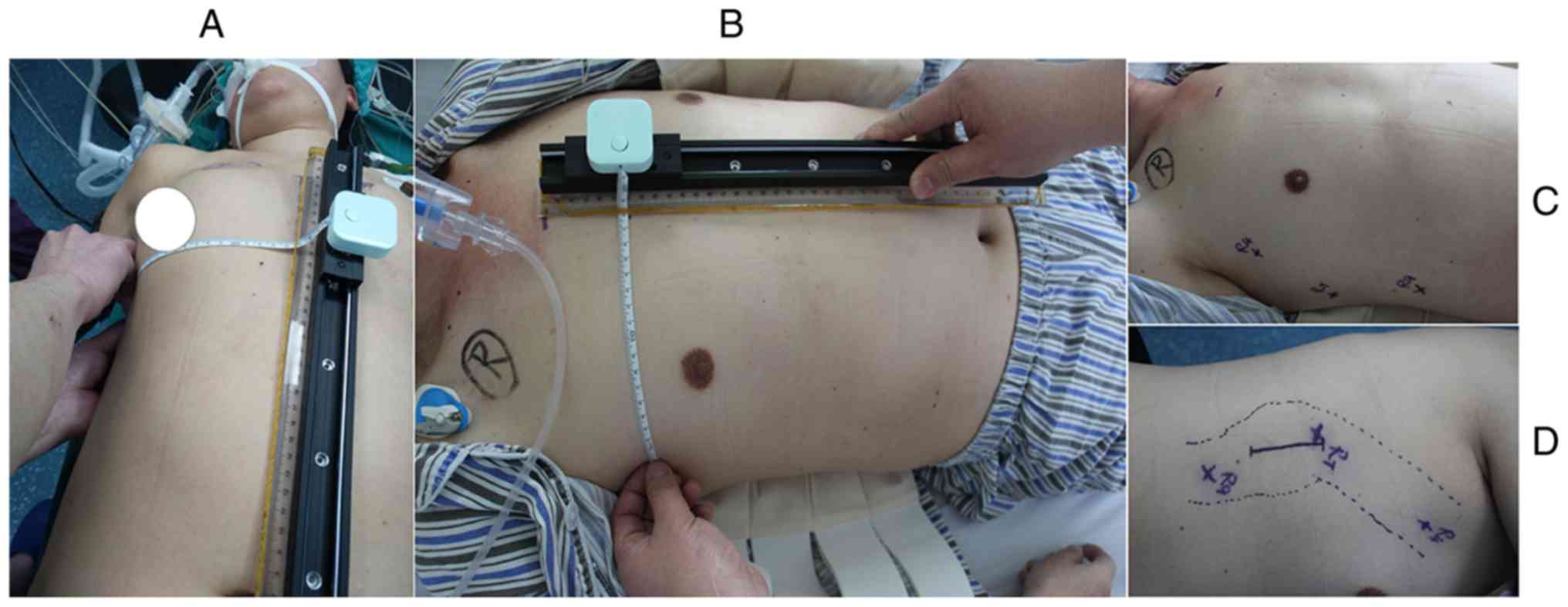
1). The frame surface positioning ruler was used to determine
the ordinate. The ‘0’ scale corresponds to the sternal angle plane
or the cervical 7 vertebral body spinous process plane, the slide
slips to the longitudinal coordinate value; then, the ulna was
pulled horizontally, and the sternal midline or spinal spinous
process was taken as the ‘0’ scale to locate the transverse
coordinate value. The line-drawing pen was used to mark the surface
position of the broken end of the fracture of the ribs (Fig. 2).
Operation method
All patients underwent transosseous thoracic
tunnel-type endoscopic internal fixation of ribs (7). Pure titanium rib bone plate was used as
the fixation material. The specific surgical procedure was as
follows: Single cavity intubation was performed under general
anesthesia. According to the location and number of ribs fractured,
the patient's surgical position (such as, the hypothesis, the prone
position, left and right lateral position) was designed. The
surface position was located through the combined use of frame body
positioning ruler and marked volumetric CT measurement data, and
the location of incision was identified according to the surface
position and the fracture position of chest wall muscles anatomical
distribution. General center of the juggle multiple fractured ribs
and chest wall muscle clearance (commonly used approaches:
Pectoralis major approach, lower marginal mammary approach,
auscultation triangle approach, vertical spinal muscle lateral
approach, axillary approach) were taken into consideration.
Incision could be transverse, longitudinal or oblique, fully free
of subcutaneous and muscle layers. The incision should be made
along the muscle gap and muscle texture to the surface of the bone
thorax, avoiding breaking the muscle, cutting off part of the
muscle attachment points along the surface of the bone thorax, and
using a special intrathoracic wall extension surgical instrument to
support the muscle thorax in the direction perpendicular to the
bone thorax, so as to separate the skeletal thorax and muscle
thorax. Using this space, thoracoscopy was used to free the
necessary muscle chest, forming a temporary tunnel in the chest
wall. After the fracture in the distance of the tunnel was reset, a
rib fixing plate was required to be buckled on both sides of the
rib fracture of the anatomical reduction along the running
direction of the rib, and the rib fixing plate was fixed on the
broken-end surface of the fracture by using a special clamp.
Observation indices
The preset incision accuracy, incision length,
operation time, intraoperative bleeding volume, postoperative wound
drainage volume and postoperative pain score were recorded and
compared between the two groups.
Statistical analysis
SPSS 19.0 software (IBM Corp.) was used for
statistical analysis of the data. The results were expressed as the
mean ± standard deviation (SD). VAS score, intraoperative bleeding
volume, postoperative wound drainage volume, operation time and
incision length were analyzed by t-test, whereas Chi-square test
was used for the accuracy of preset incision. P<0.05 was
considered to indicate a statistically significant difference.
Results
Postoperative pain was significantly reduced in
patients who underwent transosseous thoracic tunneling internal
fixation, and the difference between the two groups was
statistically significant (P<0.05). In the experimental group,
the accuracy of the preset incision was significantly increased
(Table II), and the operation time,
incision length (Table III),
intraoperative bleeding volume, postoperative wound drainage volume
(Table IV) and postoperative pain
score (Table V) were significantly
reduced, compared with those on the control group. The differences
were statistically significant (Tables
II-V).
| Table IIAccuracy of preset incision in the two
groups. |
Table II
Accuracy of preset incision in the two
groups.
| Group | Cases | Accurate
prediction | Inaccurate
prediction |
|---|
| Experimental
group | 42 | 39 | 3 |
| Control group | 38 | 30 | 8 |
| Table IIIComparison of operation time and
incision length between the two groups. |
Table III
Comparison of operation time and
incision length between the two groups.
| Group | Operation time
(min) | Length of operation
incision (cm) |
|---|
| Experimental
group | 53.26±9.32 | 6.25±1.02 |
| Control group | 70.50±11.01 | 10.23±1.35 |
| P-value | 0.003 | 0.017 |
| Table IVComparison of intraoperative bleeding
volume and postoperative wound drainage volume between the two
groups. |
Table IV
Comparison of intraoperative bleeding
volume and postoperative wound drainage volume between the two
groups.
| Group | Bleeding volume
(ml) | Wound drainage volume
(ml) |
|---|
| Experimental
group | 20.17±10.43 | 45.72±7.21 |
| Control group | 40.58±12.15 | 65.35±14.13 |
| P-value | 0.001 | 0.002 |
| Table VComparison of VAS scores before and
after operation. |
Table V
Comparison of VAS scores before and
after operation.
| Time | Experimental
group | Control group | t | P-value |
|---|
| Before operation | 7.32±1.05 | 7.35±1.04 | -1.132 | 0.173 |
| 1 day after
operation | 3.75±1.12 | 4.75±1.05 | 1.022 | 0.003 |
| 3 days after
operation | 3.53±1.07 | 3.97±1.13 | 1.017 | 0.002 |
Discussion
Multiple rib fractures often occur in chest
injuries, accompanied by local pain and limited breathing. When
flail chest is present, patients may exhibit abnormal breathing
movements, which may lead to circulatory dysfunction, acute
respiratory distress syndrome, or multiple organ failure.
Therefore, fixing rib fractures in chest injuries is necessary
(8-12).
For multiple rib fractures, methods such as chest band compression
external fixation and ventilator-assisted breathing, were used in
the past to improve the condition of chest wall collapse and
abnormal breathing to some extent. Currently, with the development
of medical technology and the emergency of new internal fixation
materials (13,14), the treatment of multiple rib
fractures by internal rib fixation has become an industry
consensus. Internal rib fixation surgery can relieve patients' pain
and reduce the related complications, speed the recovery of the
patients, and improve the prognosis of patients. Due to the
progress made on surgical techniques, including the clinical
application of 3D printing and the emergence of new operation
materials, especially the fracture fixation material, surgery is
becoming minimally invasive, leading to the reduction of surgical
complications (15-17)
and requiring accurate positioning of the incision. Some studies
have analyzed the problem of surgical approach, but the incision
site cannot be accurately positioned yet (18).
Currently, patients with rib fractures usually
receive 3D CT examination of the ribs for a clear diagnosis of the
contraposition of fracture ends. In the traditional rib-positioning
method, the surgeon determines the operation incision of the
patient relying on his own 3D interpretation through 3D CT imaging
of the ribs before surgery, which usually has some errors. Some
experts have tried thoracoscopy (VATS) to locate the fractured end
of rib fractures; however, this operation requires the insert of
the scope tube into the chest cavity, breaking the integrity of the
pleural cavity. The surgical path in order to fix the ribs is
through the rib cage, rather than through the bony extrathoracic
tunnel path, causing heavy damage. Clinical practice confirms that
severely misplaced rib fractures are difficult to fix with ribs in
the thorax. In addition, there are few options for fixing
materials. Therefore, it is difficult to promote in clinical
practice. B-ultrasound positioning of rib fractures before surgery
may cause severe pain. Moreover, the surgeon is important to have
certain experience in B-ultrasonic operation, and it is difficult
to locate a fracture with minor displacement. According to a
cross-sectional study (19) on the
evaluation of 61 patients with rib fractures, B-ultrasound is more
sensitive than X-rays and requires less time to diagnose. Because
of the anatomical characteristics of the ribs and the large surface
area of the chest wall, it is very important to determine the
incision of internal fixation of rib fracture. Accurately selecting
the incision can make the surgery minimally invasive, reduce the
injury of chest wall muscles, the damage to peripheral blood
vessels and nerves, the operation time and the postoperative pain,
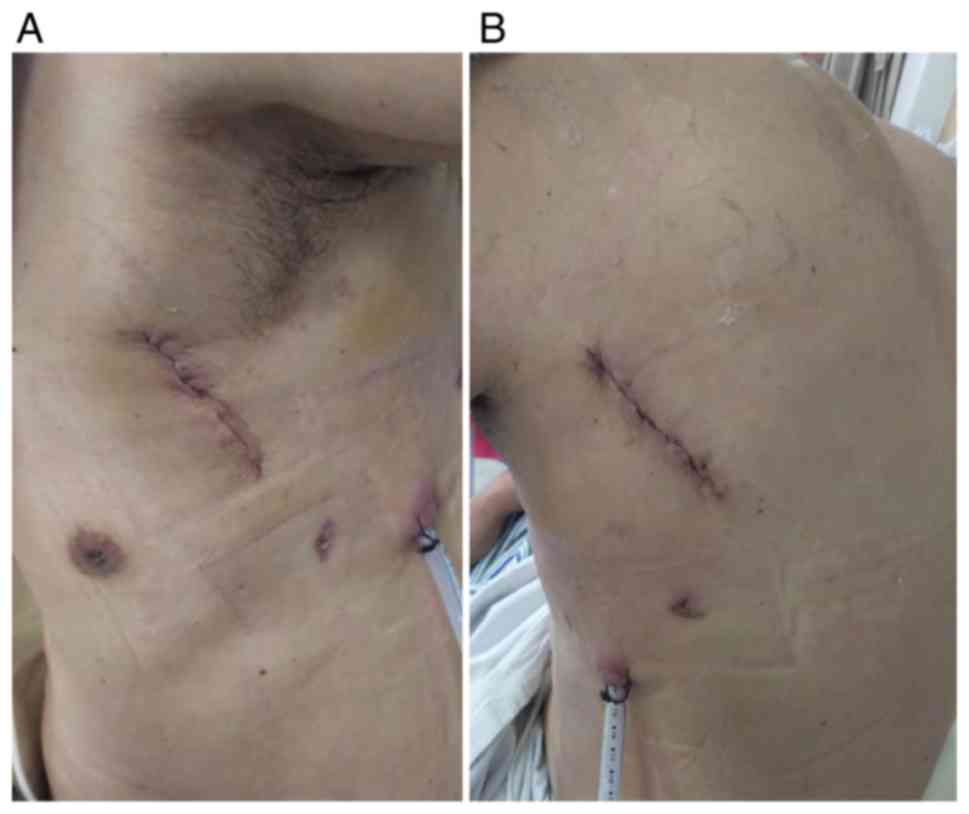
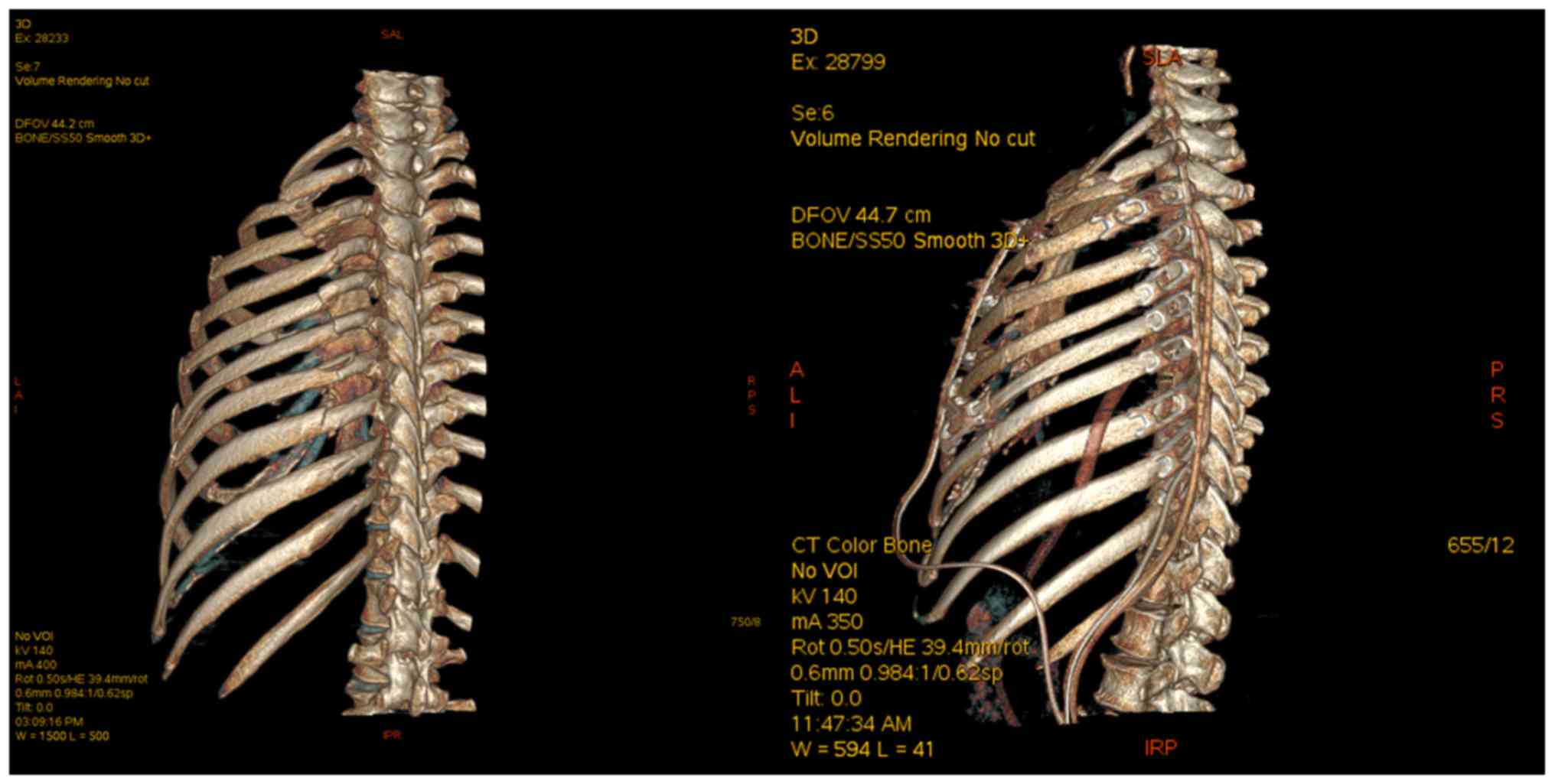
and accelerate the recovery of patients. The application of the rib
surface positioning ruler combined with the CT measurement
technique can more accurately determine the surface position of the
rib fracture and preset the operation incision (Figs. 3 and 4). Although the change of posture may cause
some errors, compared with the traditional rib-positioning method,
it still has obvious advantages, which can make the operation more
smooth and lead to fewer postoperative complications.
In summary, in the surgical treatment of multiple
rib fractures, the preoperative use of rib surface positioning
ruler combined with volumetric CT measurement and positioning
method to preset the operation incision, can reduce the length of
operation incision, the operation time, the postoperative pain of
patients, and the incidence of related complications, suggesting
that this method is worthy of wide promotion in clinical
practice.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
HX, ZS and JW conceived and designed the study. AT
and JL acquired the data. XL was responsible for the determination
of the operation incision site. SZ, JM and DW were responsible for
the operation. All authors read and approved the final version of
the manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Tianjin Hospital Affiliated to Tianjin University (Tianjin, China).
Signed written informed consents were obtained from the patients
and/or guardians.
Patient consent for publication
Patients agreed to their data to be published by
providing signed written informed consents.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ho XN, Wee IJ, Syn N, Harrison M, Wilson L
and Choong AM: The endovascular repair of blunt traumatic thoracic
aortic injury in Asia: A systematic review and meta-analysis.
Vascular. 27:213–223. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Brasel KJ, Moore EE, Albrecht RA, deMoya
M, Schreiber M, Karmy-Jones R, Rowell S, Namias N, Cohen M, Shatz
DV and Biffl WL: Western trauma association critical decisions in
trauma: Management of rib fractures. J Trauma Acute Care Surg.
82:200–203. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Pieracci FM, Majercik S, Ali-Osman F, Ang
D, Doben A, Edwards JG, French B, Gasparri M, Marasco S, Minshall
C, et al: Consensus statement: Surgical stabilization of rib
fractures rib fracture colloquium clinical practice guidelines.
Injury. 48:307–321. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bemelman M, de Kruijf MW, van Baal M and
Leenen L: Rib fractures: To fix or not to fix? An evidence-based
algorithm. Korean J Thorac Cardiovasc Surg. 50:229–234.
2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Kocher GJ, Sharafi S, Azenha LF and Schmid
RA: Chest wall stabilization in ventilator-dependent traumatic
flail chest patients: Who benefits. Eur J Cardiothorac Surg.
51:696–701. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sun ZY, Wang DB, Xia HG, Zhu DQ, Zhu PZ,
Deng LM, Zhang YM and Zhang HQ: Rib surface positioning ruler.
Patent CN209733991U and ZL 201920 189426.4. Filed February 11,
2019; Issued December 6, 2019.
|
|
7
|
Xia H, Zhu P, Li J, Zhu D, Sun Z, Deng L,
Zhang Y and Wang D: Thoracoscope combined with internal support
system of chest wall in open reduction and internal fixation for
multiple rib fractures. Exp Ther Med. 16:4650–4654. 2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Correction. No benefit to surgical
fixation of flail chest injuries compared with modern comprehensive
management: Results of a retrospective cohort study. Can J Surg.
60(7)2017.PubMed/NCBI
|
|
9
|
Uchida K, Nishimura T, Takesada H, Morioka
T, Hagawa N, Yamamoto T, Kaga S, Terada T, Shinyama N, Yamamoto H
and Mizobata Y: Evaluation of efficacy and indications of surgical
fixation for multiple rib fractures: A propensity-score matched
analysis. Eur J Trauma Emerg Surg. 43:541–547. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Pieracci FM, Lin Y, Rodil M, Synder M,
Herbert B, Tran DK, Stoval RT, Johnson JL, Biffl WL, Barnett CC, et
al: A prospective, controlled clinical evaluation of surgical
stabilization of severe rib fractures. J Trauma Acute Care Surg.
80:187–194. 2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Wiese MN, Kawel-Boehm N, de la Santa PM,
Al-Shahrabani F, Toffel M, Rosenthal R, Schäfer J, Tamm M,
Bremerich J and Lardinois D: Retraction to ‘Functional results
after chest wall stabilization with a new screwless fixation
device’ (Eur J Cardiothorac Surg 47: 868-875, 2015). Eur J
Cardiothorac Surg. 53(695)2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Dehghan N: Challenges in plate fixation of
chest wall injuries. Injury. 49 (Suppl 1):S39–S43. 2018.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Klein GT, Lu Y and Wang MY: 3D printing
and neurosurgery-ready for prime time. World Neurosurg. 80:233–235.
2013.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Nolasco-de la Rosa AL, Mosiñoz-Montes R,
Matehuala-García J, Román-Guzmán E, Quero-Sandoval F and
Reyes-Miranda AL: Unstable thorax fixation with bioabsorbable
plates and screws. Presentation of some cases. Cir Cir. 83:23–28.
2015.PubMed/NCBI View Article : Google Scholar : (In Spanish).
|
|
15
|
Morodomi Y, Okamoto T, Tagawa T, Shoji F,
Katsura M, Fujishita T, Fujiyoshi T, Akahoshi T, Yasuda M and
Maehara Y: A novel method of using bioabsorbable materials for the
surgical repair of flail chest. J Trauma Acute Care Surg.
81:984–987. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Nolasco-de la Rosa AL, Mosiñoz-Montes R,
Matehuala-García J, Cuautle-Ramírez AA, Román-Guzmán E,
Reyes-Miranda AL and Quero-Sandoval F: Thoracic inestability fixed
with bioabsorbable screws and plates. Acta Ortop Mex. 30:311–315.
2016.PubMed/NCBI(In Spanish).
|
|
17
|
Zhuo C, Lei L, Yulin Z, Wentao L,
Shuangxia W, Chao W, Yaqian Z, Shuman H and Dong D: Creation and
validation of three-dimensional printed models for basic nasal
endoscopic training. Int Forum Allergy Rhinol. 9:695–701.
2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Taylor BC, French BG and Fowler TT:
Surgical approaches for rib fracture fixation. J Orthop Trauma.
27:e168–e173. 2013.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Pishbin E, Ahmadi K, Foogardi M, Salehi M,
Seilanian Toosi F and Rahimi-Movaghar V: Comparison of
ultrasonography and radiography in diagnosis of rib fractures. Chin
J Traumatol. 20:226–228. 2017.PubMed/NCBI View Article : Google Scholar
|