Introduction
Uterine fibroids, commonly referred to as myomas or
leiomyomas, are the most common benign lesion occurring in females
of child-bearing age. While the majority of uterine fibroids are
benign, they may negatively affect the female reproductive system,
reducing fertility and causing significant morbidity for
symptomatic patients, which may decrease their overall quality of
life (1,2). It is estimated that 25% of females of
reproductive age develop uterine fibroids (3). At present, there are limited
non-surgical options for the long-term treatment of uterine
fibroids. While surgery is the primary and most effective
treatment, uterine fibroids have high recurrence rates after
treatment, leading to psychological and economic burdens to the
patients and society at large (4,5). Uterine
artery embolization (UAE) is a safe and highly effective minimally
invasive approach for treating symptomatic patients (6). However, this approach exposes the
uterus and ovaries to high levels of ionizing radiation, which may
negatively affect the child-bearing ability of females. In
addition, UAE is a complex procedure requiring skilled and
well-trained interventionists (7).
In recent years, several techniques have been proposed for reducing
the dosage of ionizing radiation, including bilateral femoral
access and low imaging frame rates (8). However, these techniques may lead to
low image quality and an increased risk of injury to the
patient.
During the UAE procedure, imaging guidance is of
critical importance to increase the accuracy of UAE and minimize
any potential complications associated with this highly complex
procedure (9,10). Image guidance under 2-dimentional
(2-D) digital subtraction angiography (DSA) for UAE is widely
reported in the literature (7,11).
However, with the development of new imaging
modalities, it has become possible to obtain optimal images using
enhanced 3-D functional and axial-anatomic adjunctive technologies
(12,13). Dyna CT, which is also known as modern
C-arm CT or cone-beam CT angiography, uses all of the capabilities
of modern C-arm digital angiography systems commonly available in
endovascular suites. Dyna CT has become increasingly adopted in the
clinical community due to its high image quality, versatility and
dedicated applications for planning, guiding, monitoring and
assessing interventional procedures (14). In a previous study, the usefulness of
3-D angiography was demonstrated using Dyna CT in the treatment of
hepatocellular carcinoma via transcatheter arterial
chemoembolization (15). In
addition, 3-D angiography using Dyna CT was also reported to be
useful in diagnostic and interventional radiology procedures
involving the head, specifically cerebral aneurysms (16).
Despite the apparent advantages of Dyna CT, the use
of imaging technology for UAE of fibroids has rarely been reported.
It was hypothesized that Dyna CT may be a valuable imaging tool for
improving the treatment of fibroids during UAE. The present study
aimed to determine whether 3-D angiography by Dyna CT may replace
conventional digital subtraction angiography anterior-posterior
imaging in the transarterial embolization of fibroids.
Materials and methods
Study design
The present study was approved by the Institutional
Review Board and Ethics Committee of the First People's Hospital of
Changzhou (Changzhou, China). All patients provided written
informed consent prior to participation. The study population was
comprised of patients with symptomatic uterine fibroids who were
scheduled to undergo transarterial UAE at the Department of
Interventional Radiology at the First People's Hospital of
Changzhou (Changzhou, China) between May 2016 and September 2018.
Dyna CT and DSA were performed in all patients during angiographic
embolization of the bilateral internal iliac arteries.
The inclusion criteria for the present study were as
follows: i) Females aged <50 years of age with uterine fibroids
(types I-III) as determined by the International Federation of
Gynecology and Obstetrics assessed by B-ultrasound (17), sessile with intramural extension of
fibroid <50% (type I), sessile with intramural extension by
>50% (type II) or lesions localized in the myometrium with no
deformation of the endometrial cavity (type III); ii) good general
health; and iii) willing to undergo UAE. The exclusion criteria for
the present study were as follows: i) Presence of other malignant
or benign tumors; ii) tumors of >10 cm in diameter or
non-submucosal myomas <3 cm in diameter; iii) presence of
endometriosis or adenomyosis; iv) acute or chronic inflammation of
the pelvic cavity; v) allergy to the contrast agents used during
intervention therapy; and vi) patient age >50 years.
Angiography
Angiography was performed on the Siemens Artis zeego
Syngo Dyna CT 360 digital angiography system (Siemens Medical
Solutions) with a C-arm rotational speed of 30 degrees/sec and a
rotational range of 200 degrees.
The operation was performed by a single physician
with 10 years of experience at the Department of Interventional
Radiology of the First People's Hospital of Changzhou (Changzhou,
China). The diameter of the image intensifier on the C-arm was 16
inches. The Dyna CT software, non-ionic iodinated contrast agent
(Omnipaque; GE Healthcare) and high-pressure syringe (Mark V
Provis; Medrad, Inc.) were used as described below.
For angiography, the Seldinger technique was
implemented using a 5F sheath (18).
The 5F-RH catheter was placed in the bilateral internal iliac
arteries for Dyna CT imaging of the bilateral internal iliac
arteries, after confirming the origin of the bilateral uterine
arteries by Dyna CT 3-D angiography. The contrast agent was
injected into patients to observe the vascular architecture of the
uterine arteries and fibroid staining. Using the contrast agent
Omnipaque (300 mg/ml; internal iliac arteries, 6 ml at 1 ml/sec),
the DSA scan was performed 2 sec after starting the injection, with
an acquisition frame rate of 4 frames/sec, collection matrix of
1,024 by 1,024 and acquisition time of 4 sec.
Masked images were obtained with a 360-degree
rotation of the C-arm, followed by a return to the start position.
The patients included in the present study were <50 years of age
and were able to effectively hold their breath, which minimized the
risk of motion artifacts. The whole procedure lasted only 7 sec and
only a short breath hold was required, which minimized the number
of artifacts.
Since the present study aimed to assess the
usefulness of Dyna CT angiography in transarterial UAE of fibroids,
it was important to visualize the uterus and fibroid. Therefore, it
was necessary to image the uterine arteries and stained fibroids
during rotational DSA. To fulfill this requirement, the timing of
contrast agent injection and the amount of agent injected were
determined based on previously performed internal iliac artery
angiography, as an equal amount was required for the contrast media
to fill the artery and reveal fibroid staining throughout the
entire rotational DSA session. During internal iliac artery
angiography, the time elapsed until visualization of the stained
fibroids on the DSA images was determined and the start of contrast
agent injection preceded the start of rotational DSA by this amount
of time. The contrast agent injection continued until the end of
the rotational DSA. The contrast agent for Dyna CT was Omnipaque
(300 mg/ml; bilateral internal iliac, 3 ml/sec; imaging was
performed 2 sec after the start of contrast agent injection).
Imaging data from Dyna CT were automatically transferred to the
Siemens X-Leonardo image processing workstation (Siemens Medical
Solutions) for vascular imaging processing with volume-rendering
technology. This allowed for better visualization of the origin of
uterine arteries and fibroids with an acquisition frame rate of 60
frames/sec and a matrix size of 1,024 by 1,024. Although the
density resolution of Dynamic CT is lower than that of conventional
CT, the radiation dose was lower than that of conventional CT.
Volume-rendering technology was used to locate the origin of
uterine arteries and fibroids during transarterial UAE of the
fibroids.
Contrast agent and radiation dose
The radiation dose of Dyna CT was 233 mGy per scan
with a bilateral dose of 466 mGy. The DSA contrast agent
(Omnipaque) was given manually at a volume of 5-8 ml, with a
bilateral volume of 10-16 ml. Since the location and angle of the
tube were adjusted for each patient during surgery, the operation
times varied between patients. The radiation doses given to
patients were between 200 and 500 mGy.
Image analysis
The visualization qualities of the origin of uterine
arteries and stained fibroids imaged by Dyna CT 3-D rotational
angiography and DSA anterior-posterior images were compared. DSA
anterior-posterior images were evaluated at the workstation, while
Dyna CT images were assessed by rotating the images created using
volume-rendering technology. 3-D rotational angiography images were
available for examination at the workstation immediately after
completing the Dyna CT scans. The preparation of volume-rendering
technology images required 1 min. The volume-rendering technology
images are the most straightforward reconstructed images. Two
experts in angiography (ZHH and QW) assessed the origin of uterine
arteries and stained fibroids independently and any discrepancies
were resolved by consensus.
Statistical analysis
Continuous data were expressed as the mean ±
standard deviation and enumeration data as n (%). Data were
compared by the McNemar test using SPSS software (v19.0, IBM
Corp.). P<0.05 was considered to indicate statistical
significance.
Results
Baseline characteristics of the
patients
A total of 74 patients were considered for the
present study and 9 were excluded based on the inclusion and
exclusion criteria. Finally, 65 patients were included in the
study. The average age of the patients was 38.5±9.5 years. A total
of 21 patients had type I submucosal myomas, 14 had type II
submucosal myomas, 19 had intramural myoma (type III) and 11
patients had mixed myomas (types I-III). The detailed patient
characteristics are summarized in Table
I.
 | Table IPatient baseline characteristics. |
Table I
Patient baseline characteristics.
| Variable | Value |
|---|
| Age (years) | 38.5±9.5 |
| Type of fibroid | |
|
I | 21 (32.3) |
|
II | 14 (21.5) |
|
III | 19 (29.3) |
|
Mixed | 11 (16.9) |
| Previous history of
uterine surgery | |
|
Yes | 23 (35.4) |
|
No | 42 (64.6) |
| Dysmenorrhea | |
|
Yes | 25 (38.5) |
|
No | 40 (61.5) |
| Development of the
ovarian branch of the uterine artery | |
|
Bilateral | 12 (18.5) |
|
Unilateral | 11 (16.9) |
|
None | 42 (64.6) |
Image processing in different
modalities
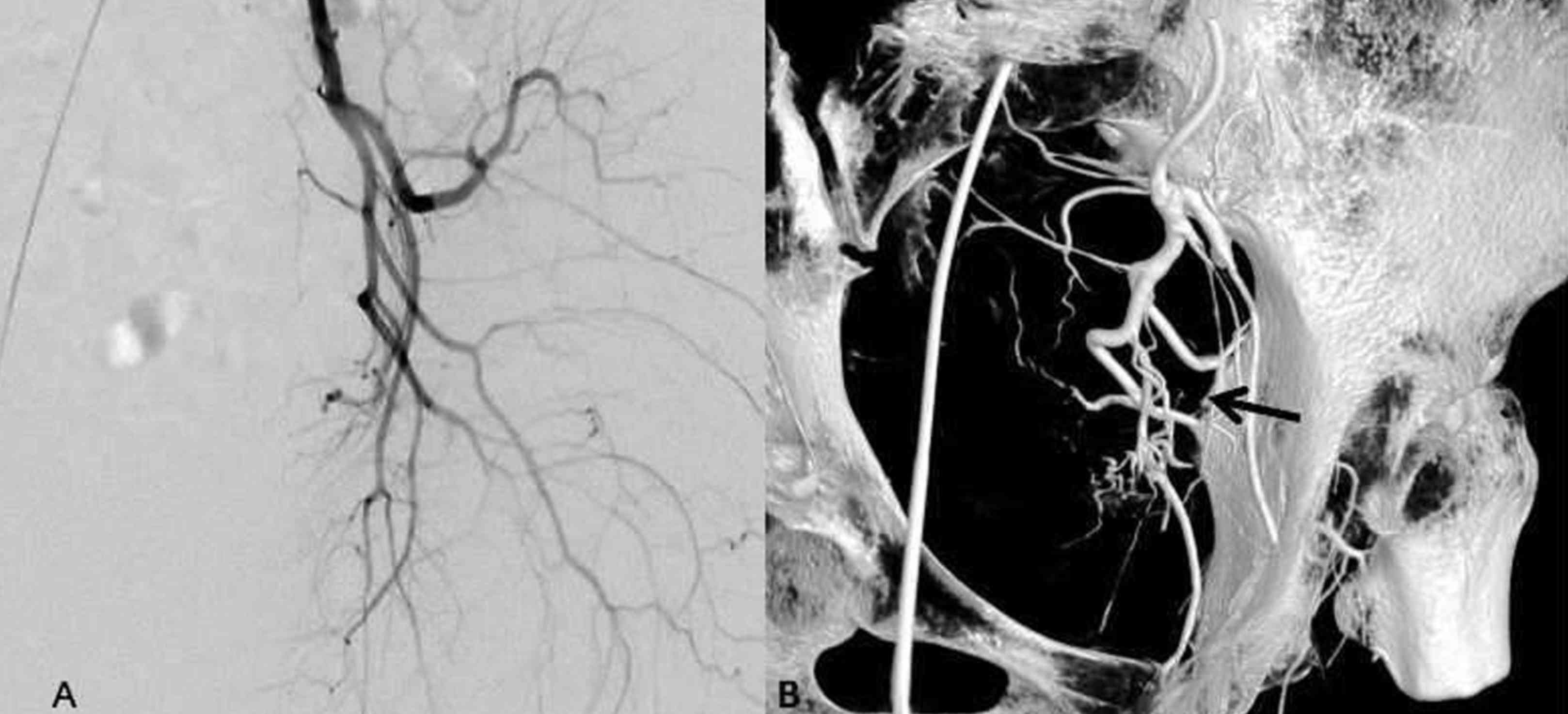
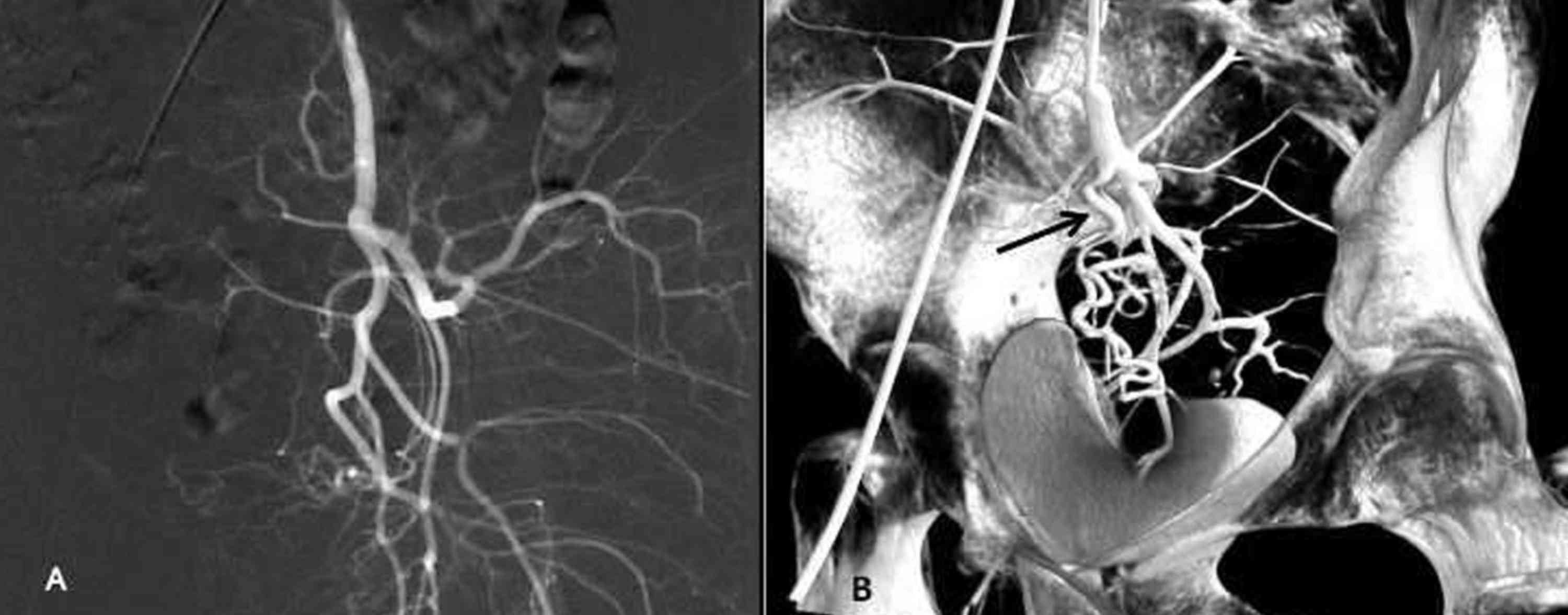
Dyna CT imaging was successfully completed in all of
the patients. The 3-D rotational angiographic images, including the
volume-rendering technology images, are superior for 3-D
visualization of specific vascular structures of the uterine
arteries (19), particularly for
identifying 3-D structures of the origin of uterine arteries in
patients where DSA anterior-posterior images display complex pelvic
vessel anatomy or overlapping arteries (Figs. 1 and 2). Maximum intensity projection images and
shaded surface display images may display the 3-D structures of
arteries, yet volume-rendering technology images are more efficient
for identifying the 3-D structures of arterial branches (15).
Outcomes of Dyna CT angiography vs.
DSA-AP imaging
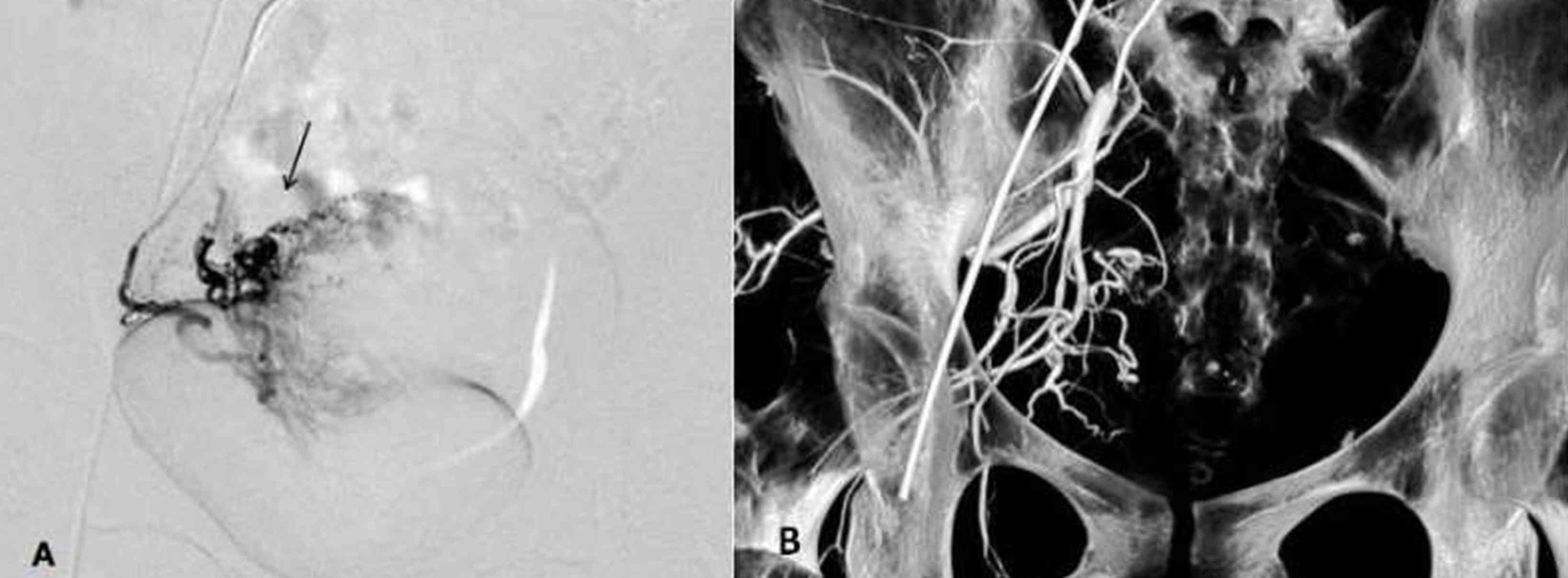
Dyna CT 3-D angiography displayed the origin of
uterine arteries in all patients (100%), while DSA
anterior-posterior only displayed the origin in 45 cases (69.2%,
P=0.03). There were 12 cases with overlapping uterine arteries and
8 cases with complex vascular anatomies. However, the detection
rate of fibroids on Dyna CT 3-D angiography was lower than that on
DSA anterior-posterior imaging (Fig.
3). Stained fibroids were identified in 57 cases (87.7%) by
Dyna CT and in all 65 cases (100%, P=0.03) by DSA
anterior-posterior imaging. There were statistically significant
differences in the detection rates for fibroids and the origin of
bilateral uterine arteries between the two imaging modalities
(Table II).
| Table IIOutcomes of Dyna CT angiography vs.
DSA-AP imaging. |
Table II
Outcomes of Dyna CT angiography vs.
DSA-AP imaging.
| Detected item | Dyna CT | DSA-AP | P-value |
|---|
| Origin of bilateral
uterine arteries (n=65) | 65 (100) | 45 (69.2) | 0.03 |
| Fibroids (n=65) | 57 (87.7) | 65 (100) | 0.03 |
Discussion
In the present study, Dyna CT was superior to DSA
anterior-posterior imaging in detecting the origin of bilateral
uterine arteries, particularly in cases with overlapping uterine
arteries on DSA anterior-posterior images or in patients with
complex vascular anatomies. However, Dyna CT was less efficient in
detecting stained fibroids. To the best of our knowledge, there are
no other studies on whether Dyna CT was superior to DSA imaging in
detecting the origin of bilateral uterine arteries.
Due to recent technological advances in angiography,
it is now possible to perform rotational DSA using a C-arm equipped
with a large diameter image intensifier, which may be used to image
pelvic vascular structures (19). A
fundamental requirement of imaging procedures for transarterial UAE
of fibroids is angiography, yet the understanding of the spatial
distribution of vascular structures is highly dependent on the
physician's anatomical knowledge, since the images are 2-D
(7). Any method that relies heavily
on the expertise and experience of physicians may have limited
utility in the clinic, as misunderstandings are more likely to
occur (15). Transarterial UAE of
fibroids requires a detailed understanding of 3-D vascular anatomy
prior to embolization. For this reason, 3-D angiography using
rotational DSA during pelvic angiography was performed for
transarterial embolization of fibroids and its usefulness in
transarterial embolization of fibroids was assessed.
The success of transarterial UAE of fibroids depends
on precisely identifying the origin of uterine arteries, along with
highly selective catheterization (20). Previous studies have indicated that
excessive embolization may damage normal myometrium, ovaries or
fallopian tubes, resulting in uterine necrosis, infections or
ovarian failure in rare cases. However, incomplete therapy or
further blood supply to the tumor may result in treatment failure
(21). Angiography images are
generally 2-D, yet it is essential to assess the 3-D anatomy of the
vasculature in patients with overlapping vessels or complex
vascular structures (19,22). In the present study, Dyna CT detected
the origin of bilateral arteries in all of the patients, while DSA
anterior-posterior images were unable to detect the origin in all
of the patients, corroborating the notion that Dyna CT may be
useful in patients with overlapping uterine arteries or complex
vascular anatomies on DSA anterior-posterior images.
In a previous study, Gupta et al (23) demonstrated that 3-D rotational
angiography is preferable to 2-D techniques for UAE. When using 3-D
angiography by Dyna CT in the transarterial embolization of
fibroids, it was esteemed to overcome the limits of DSA
anterior-posterior imaging. As the ultimate objective, it was
evaluated whether 3-D rotational angiography may be used in place
of DSA anterior-posterior imaging by assessing the status of
stained fibroids. Compared with DSA anterior-posterior imaging,
Dyna CT demonstrated inferior visualization quality for the stained
fibroids. In certain patients, fibroids were visualized by DSA
anterior-posterior imaging, but not by Dyna CT 3-D rotational
angiography.
One reason for this finding may be the difficulty in
simultaneously visualizing the origin of uterine arteries and
fibroids. During Dyna CT, the internal iliac artery and fibroids
are filled with contrast media. Therefore, the time from the start
of contrast agent injection to the visualization of stained
fibroids in DSA imaging during internal iliac artery angiography is
measured and Dyna CT is initiated when the fibroid staining begins
to appear. In return, contrast agent injection is commenced prior
to Dyna CT and it is continuously administered until completion.
However, this increases the concentration of contrast agent in the
uterus and may lead to poor fibroid visualization. In addition,
there was a difference in radiation dose required for each frame.
The radiation dose is measured as the mass voltage (V) and the mass
is measured by current (mA) multiplied by time (sec). In Dyna CT,
the X-ray tube rotates to restrict the exposure time. For
compensation, the current (mA) increases within a specific limit,
which increases the voltage and light scatter and decreases the
image contrast. Motion artifacts may be another factor. 3-D
angiography by Dyna CT does not require the patients to hold their
breath, since it is performed in the head region. However, in the
abdominal region, the patient must hold his/her breath for at least
7 sec from the start of masked images to the end of rotational DSA
and another 2 sec for contrast agent injection (24,25). In
the present study, poor image quality of the fibroids was noted
directly below the bottom of the uterus. This may be a result of
motion artifacts due to patients not adequately holding their
breath.
In the present study, patients over the age of 50
years were excluded, as older females experience menopause, which
frequently results in the shrinkage of fibroids, reducing clinical
symptoms. US is the gold standard as it allows physicians to
accurately visualize the location and size of fibroids.
Pathological diagnoses require highly invasive biopsies or
surgeries, which should be avoided if possible. The present study
had certain limitations that should be addressed. First, selection
bias may have been present due to patients being selected from a
single center. In addition, the sample size was relatively small.
Further studies with larger sample sizes using patients from
multiple clinical centers are required to confirm the present
results.
In conclusion, 3-D angiography by Dyna CT is useful
for identifying the 3-D anatomy of the bilateral internal iliac
arteries during the transarterial UAE of fibroids, particularly in
patients with the origin of uterine overlapping on DSA
anterior-posterior images and patients with complex vascular
branches. Compared with DSA anterior-posterior imaging, Dyna CT
exhibited reduced visualization quality for fibroids. Therefore,
Dyna CT cannot replace DSA anterior-posterior imaging for
procedural evaluation of patients during transarterial embolization
of fibroids. However, Dyna CT may provide information supplementary
to DSA anterior-posterior images, which may assist physicians
during treatment planning.
Acknowledgements
The authors wish to thank the patient advisers (Mrs.
Chun-lan Xu, Mrs. Hui Wang and Dr Yuanquan Huang from the First
People's Hospital of Changzhou, Changzhou, Jiangsu, China) for
their assistance.
Funding
The present study was supported by the Natural
Science Foundation of Jiangsu Province (grant no. BK20180185) and
the Youth Foundation of Changzhou First People's Hospital (grant
no. yy2017006).
Availability of data and materials
The datasets generated and analyzed during the
present study are available from the corresponding author on
reasonable request.
Authors' contributions
CYW, JGX and WHC performed most of the
investigations, the data analysis and wrote the manuscript; JGX
supervised CYW and WHC during the UAE procedure. YFL provided
assistance during the UAE procedure and performed statistical
analysis. CYW, ZHH and QW contributed to the interpretation of the
data and analyses. All of the authors read and approved the
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board and Ethics Committee of the First People's Hospital of
Changzhou (Changzhou, China). All procedures performed in studies
involving human participants were in accordance with the ethical
standards of the institutional and/or national research committee
and with the 1964 Helsinki declaration and its later amendments or
comparable ethical standards. All patients provided written
informed consent prior to participation.
Patient consent for publication
All data of the present study were published with
the written informed consent of the patients.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Stewart EA: Clinical practice. Uterine
fibroids. N Engl J Med. 372:1646–1655. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Olejek A, Olszak-Wasik K and
Czerwinska-Bednarska A: Long-term intermittent pharmacological
therapy of uterine fibroids-a possibility to avoid hysterectomy and
its negative consequences. Prz Menopauzalny. 15:48–51.
2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Zhao H, Li Y, Xu Q, Peng F, Zhao J, Webb
RC, Peng C and Yu C: Establishment of a rat model for uterine
leiomyomas based on western and traditional Chinese medicine
theories. Braz J Med Biol Res. 51(e7627)2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bulun SE: Uterine fibroids. N Engl J Med.
369:1344–1355. 2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Mas A, Tarazona M, Dasí Carrasco J, Estaca
G, Cristóbal I and Monleón J: Updated approaches for management of
uterine fibroids. Int J Womens Health. 9:607–617. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ananthakrishnan G, Murray L, Ritchie M,
Murray G, Bryden F, Lassman S, Lumsden MA and Moss JG: Randomized
comparison of uterine artery embolization (UAE) with surgical
treatment in patients with symptomatic uterine fibroids (REST
trial): Subanalysis of 5-year MRI findings. Cardiovasc Intervent
Radiol. 36:676–681. 2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Gupta JK, Sinha A, Lumsden MA and Hickey
M: Uterine artery embolization for symptomatic uterine fibroids.
Cochrane Database Syst Rev. CD005073:2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Sapoval M, Pellerin O, Rehel JL, Houdoux
N, Rahmoune G, Aubert B and Fitton I: Uterine artery embolization
for leiomyomata: Optimization of the radiation dose to the patient
using a flat-panel detector angiographic suite. Cardiovasc
Intervent Radiol. 33:949–954. 2010.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ko HK, Shin JH, Ko GY, Gwon DI, Kim JH,
Han K and Lee SW: Efficacy of prophylactic uterine artery
embolization before obstetrical procedures with high risk for
massive bleeding. Korean J Radiol. 18:355–360. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Mara M and Kubinova K: Embolization of
uterine fibroids from the point of view of the gynecologist: Pros
and cons. Int J Womens Health. 6:623–629. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Salazar GM, Gregory Walker T, Conway RF,
Yeddula K, Wicky S, Waltman AC and Kalva SP: Embolization of
angiographically visible type I and II utero-ovarian anastomoses
during uterine artery embolization for fibroid tumors: Impact on
symptom recurrence and permanent amenorrhea. J Vasc Interv Radiol.
24:1347–1352. 2013.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Firouznia K, Ghanaati H, Sharafi A,
Abahashemi F, Hashemi H, Jalali AH and Shakiba M: Comparing ovarian
radiation doses in flat-panel and conventional angiography during
uterine artery embolization: A randomized clinical trial. Iran J
Radiol. 10:111–115. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Maleux G, Michielsen K, Timmerman D, Poppe
W, Heye S, Vaninbroukx J and Bosmans H: 2D versus 3D roadmap for
uterine artery catheterization: Impact on several angiographic
parameters. Acta Radiol. 55:62–70. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Fahrig R, Dixon R, Payne T, Morin RL,
Ganguly A and Strobel N: Dose and image quality for a cone-beam
C-arm CT system. Med Phys. 33:4541–4550. 2006.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Wang C, Wang Q, Chen W, He Z, Huang Y, Lu
Y and Miao Y: Dyna CT arteriographic evaluation of hepatocellular
carcinoma for treatment by trans-catheter arterial
chemoembolization. Int J Clin Exp Med. 8:20548–20555.
2015.PubMed/NCBI
|
|
16
|
Colombo F, Cavedon C, Francescon P,
Casentini L, Fornezza U, Castellan L, Causin F and Perini S:
Three-dimensional angiography for radiosurgical treatment planning
for arteriovenous malformations. J Neurosurg. 98:536–543.
2003.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Doherty L, Mutlu L, Sinclair D and Taylor
H: Uterine fibroids: Clinical manifestations and contemporary
management. Reprod Sci. 21:1067–1092. 2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Guan YS, He Q and Wang MQ: Transcatheter
arterial chemoembolization: History for more than 30 years. ISRN
Gastroenterol. 2012(480650)2012.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Tanigawa N, Komemushi A, Kojima H, Kariya
S and Sawada S: Three-dimensional angiography using rotational
digital subtraction angiography: Usefulness in transarterial
embolization of hepatic tumors. Acta Radiol. 45:602–607.
2004.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Czuczwar P, Woźniak S, Szkodziak P,
Woźniakowska E, Paszkowski M, Wrona W, Milart P, Paszkowski T and
Popajewski M: Predicting the results of uterine artery
embolization: Correlation between initial intramural fibroid volume
and percentage volume decrease. Prz Menopauzalny. 13:247–252.
2014.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Pelage JP, Cazejust J, Pluot E, Le Dref O,
Laurent A, Spies JB, Chagnon S and Lacombe P: Uterine fibroid
vascularization and clinical relevance to uterine fibroid
embolization. Radiographics. 25 (Suppl 1):S99–S117. 2005.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Lanzavecchia S, Bellon PL and Radermacher
M: Fast and accurate three-dimensional reconstruction from
projections with random orientations via radon transforms. J Struct
Biol. 128:152–164. 1999.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Gupta A, Zuurmond K, Grünhagen T and
Maleux G: Three-dimensional rotational angiography is preferable to
conventional two-dimensional techniques for uterine artery
embolization. Diagn Interv Radiol. 19:418–422. 2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Tacher V, Radaelli A, Lin M and Geschwind
JF: How I do it: Cone-beam CT during transarterial
chemoembolization for liver cancer. Radiology. 274:320–334.
2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Huber ME, Hengesbach D, Botnar RM,
Kissinger KV, Boesiger P, Manning WJ and Stuber M: Motion artifact
reduction and vessel enhancement for free-breathing navigator-gated
coronary MRA using 3D k-space reordering. Magn Reson Med.
45:645–652. 2001.PubMed/NCBI View
Article : Google Scholar
|