Introduction
Drug rash with eosinophilia and systemic symptoms
(DRESS) syndrome represents an severe adverse reaction after
medication and is defined by the following elements: Skin symptoms,
fever, lymph node enlargement, eosinophilia and modified
lymphocytes, as well as internal organs dysfunction (1,2). This
syndrome appears frequently after anticonvulsant therapy, usually
after a period of up to 6 weeks following the beginning of the
treatment and the possibility of worsening the symptoms after drug
withdrawal (3,4). In addition, there are other drugs
responsible for DRESS, such as nonsteroidal anti-inflammatory
compounds, antidepressants and some antimicrobial substances
(5,6).
The difficulty in diagnosing DRESS resides in the
fact that eosinophilia is inconstant and skin and systemic symptoms
are variable (7,8). It is a life-threatening condition and
it requires early diagnosis with immediate withdrawal of the drug,
as well as hospitalization (9,10).
Case report
We encountered a male patient aged 49, with a
history of morbid obesity undergoing bariatric surgery and alcohol
addiction. Patient informed consent for publication of the
data/images associated with the manuscript was obtained. The
authors followed the international and national regulations in
accordance with the Declaration of Helsinki and all identifying
information was removed.
The patient received chronic treatment with
carbamazepine, diazepam, zolpidem and cipralex (escitalopram) for 1
month in order to treat his alcohol addiction. Upon admission, the
patient presented right ear pain for 7 days, recurrent fever and
satellite enlarged lymph nodes on the inferior parotid gland pole.
He had self-administered amoxicillin 500 mg every 12 h for 2 days,
without previous allergic reactions. Subsequently, he developed a
generalized skin reaction with erythema and pruriginous papules.
Over the previous 24 h, he had trouble swallowing and cough
(Fig. 1).
Blood results revealed marked eosinophilia without
leukocytosis: 6,010 leucocytes, 14.7% eosinophils,
125,000/mm3 platelets. In addition, he presented
respiratory alkalosis, due to hyperventilation, with pH of 7.434,
32 mmHg pCo2 and 53.9 mmHg pO2. Respiratory
distress signaled with 85% O2 saturation in breathing
air and 91% with oxygen mask. Liver enzymes ALT=114 U/l, AST=66 U/l
and reactive C protein above 30 mg/l; with coagulation status of
INR 1.37 and PT 63%.
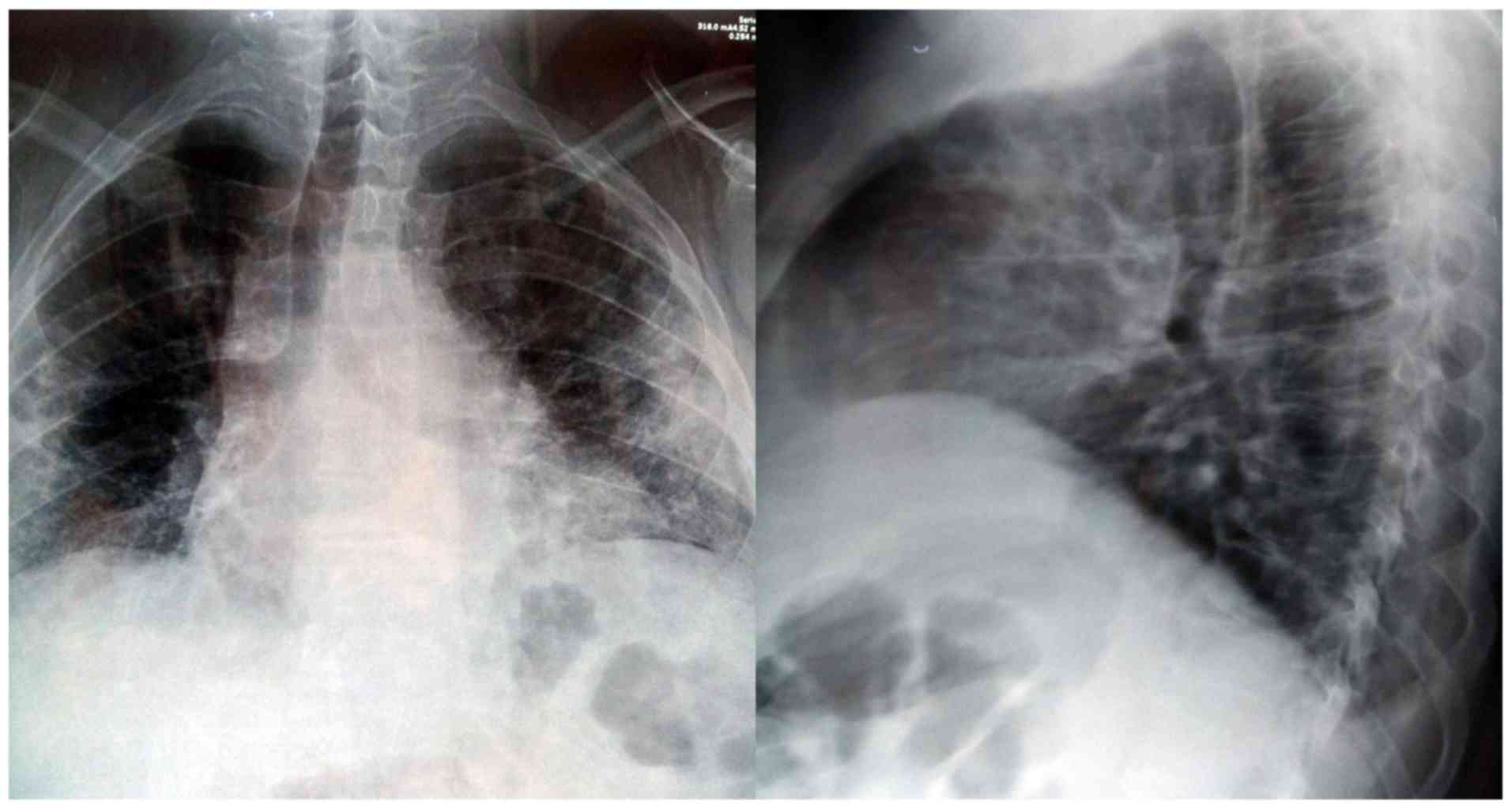
The thoracic X-ray underlined diminished
transparency in both lungs, with associated alveolar opacities. In
the right side, the authors observed a small transparency in the
hilum, indicating a possible old cavern, as well as enlarged
cardiac opacity through enlargement of the inferior left arch
(Fig. 2).
On admission, the patient presented altered general
status with whole body skin reaction and creasing of palms and
legs. General data: Body weight 147 kg, height 185 cm and body
temperature 36.2 Celsius degrees.
The ENT clinical exam recorded a right parotid lymph
node with pain on palpation, an edema of the epiglottis without the
possibility of visualizing the vocal cords and inflammation of oral
and lingual mucosa.
The patient was admitted to our ENT clinic under the
suspicion of acute edema of the epiglottis due to an allergic
reaction and generalized skin reaction after medication. Systemic
treatment with dexamethasone at 12 h was provided, arnetin
(ranitidine) at 12 h, desloratadine at 12 h, clindamycin 300 mg at
8 h, as indicated by the specialist of infectious diseases. The
allergy examination recommended stopping the administering of
carbamazepine due to a DRESS suspicion. The psychiatry examination
diagnosed a background of depression and chronic alcohol
consumption and changed the medication scheme to zolpidem once per
day, diazepam 10 mg distributed in three fractions per day,
Depakine (valproic acid) 150 mg twice per day, as well as stopping
carbamazepine. The internal medicine specialist recommended the
continuation of antibiotics, plus corticoid and antihistaminic
medication. The case had a favorable evolution after the first 24
h, with lowering of the eosinophils and remission of the laryngeal
edema.
A thorax CT scan was performed without contrast
media, which revealed interstitial densities with honeycomb aspect
in the periphery without pleural reaction. However, various
mediastinum lymph nodes of up to 12 mm in diameter were noted. This
raised the suspicion of an infectious process overlying the
idiopathic interstitial pneumonia (Fig.
3).
After 5 days, worsening of the skin condition was
observed with a novel increase of eosinophils: up to 20.2% of 8,500
leucocytes/mm3. Antibody levels of EBV, CMV, rubella,
toxoplasma, toxocara were in the normal range. The laryngeal edema
was in remission. In addition, this episode associated a fever
spike of 38.1 degrees Celsius.
Taking into consideration the joint opinion of our
allergy, dermatology and infectious diseases specialists, the
authors referred the case to a tertiary university dermatology
clinic for further treatment.
Discussion
This case reunited all the criteria for
carbamazepine-induced DRESS: Acute skin reaction, fever above 38
degrees Celsius, and the presence of enlarged lymph nodes both in
the neck and mediastinum, increased liver enzymes and eosinophilia
(11). Moreover, there was lung
involvement due to eosinophilic interstitial infiltration.
Additional criteria, such as hospital admission and
the reaction triggered by medication were also present (12). The patient received carbamazepine for
3 weeks, in addition to the previous antidepressant therapy and the
self-administering of penicillin-derived antibiotics, taken 1 week
prior to the skin reaction.
Taking into consideration the chest X-ray, the
authors also initiated antibiotic treatment with clindamycin, which
can be used even in severe cases of penicillin anaphylactic shock
(13). The most difficult aspect of
this case was the progression towards acute respiratory distress
through acute epiglottis edema. This case also presented increased
progression of symptoms, despite the suspected drug retrieval and a
period of ~72 h of systemic corticoid and antihistaminic therapy.
Such late response to common treatment for controlling systemic
immune response is considered extremely rare and life-threatening
(14).
This case tested negative for tuberculosis, but the
authors could not ascertain the presence of HHV type 6, which has
been previously associated with drug sensitivity reactions by
Pereira de Silva et al (15).
The major difficulty in this case resided in the
complex drug scheme self-administered by the patient prior to
admission, as well as the necessity to withdraw all of these
compounds and to replace them with other drugs while controlling
associated pathologies and comorbidities.
In conclusion, the elements defining DRESS and the
pathology mechanisms are not fully understood and any new reported
case brings new data to this puzzle. The case presented unites the
criteria of DRESS after carbamazepine, including additional
aspects. Among the specific elements were the pulmonary
interstitial reaction and the acute epiglottis edema with the
prospect of acute respiratory insufficiency. This is a
life-threatening situation with evolution even after the drug
withdrawal. The authors consider that hospital admission is
mandatory and the systemic treatment with corticoids and
antihistamines is broadly approved.
Acknowledgements
Professional editing, linguistic and technical
assistance was provided by Irina Radu, Individual Service Provider,
certified translator in Medicine and Pharmacy (certificate
credentials: Series E no. 0048).
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
DV and MD treated the patient, performed literature
research and wrote the manuscript. AS treated the patient and was
also involved in the conception of the study. AN, GM and EAN
offered second opinion during the patient treatment, performed
literature research and wrote the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The study followed the international and national
regulations in accordance with the Declaration of Helsinki.
Patients consent for publication
Patient informed consent for publication of the
data/images associated with the manuscript was obtained. The
authors followed the international and national regulations in
accordance with the Declaration of Helsinki and all identifying
information was removed.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Cho YT, Yang CW and Chu CY: Drug reaction
with eosinophilia and systemic symptoms (DRESS): An interplay among
drugs, viruses, and immune system. Int J Mol Sci. 18:1243–1264.
2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Wu X, Yang F, Chen S, Xiong H, Zhu Q, Gao
X, Xing Q and Luo X: Clinical, viral and genetic characteristics of
drug reaction with eosinophilia and systemic symptoms (DRESS) in
Shanghai, China. Acta Derm Venereol. 98:401–405. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
El Omairi N, Abourazzak S, Chaouki S,
Atmani S and Hida M: Drug reaction with eosinophilia and systemic
symptom (DRESS) induced by carbamazepine: A case report and
literature review. Pan Afr Med J. 18(9)2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Hiransuthikul A, Rattananupong T,
Klaewsongkram J, Rerknimitr P, Pongprutthipan M and Ruxrungtham K:
Drug-induced hypersensitivity syndrome/drug reaction with
eosinophilia and systemic symptoms (DIHS/DRESS): 11 years
retrospective study in Thailand. Allergol Int. 65:432–438.
2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Musette P and Janela B: New insights into
drug reaction with eosinophilia and systemic symptoms
pathophysiology. Front Med (Lausanne). 4(179)2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Oliveira AM, Carvalho R, Martins A and
Reis J: Acute hepatitis in the DRESS syndrome. GE Port J
Gastroenterol. 23:304–308. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Wang L and Li LF: Difficult clinical
management of antituberculosis DRESS syndrome complicated by MRSA
infection: A case report. Medicine (Baltimore).
96(e6346)2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Munch M, Peuvrel L, Brocard A, Saint Jean
M, Khammari A, Dreno B and Quereux G: Early-onset
vemurafenib-induced DRESS syndrome. Dermatology. 232:126–128.
2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Anghel AG, Anghel I, Dumitru M and Soreanu
CC: Respiratory and phonatory impairment due to iatrogenic vocal
fold paralysis and paresis. A retrospective study of 188 patients.
Rev Med Leg. 20:287–290. 2012.
|
|
10
|
Thongsri T, Chularojanamontri L and
Pichler WJ: Cardiac involvement in DRESS syndrome. Asian Pac J
Allergy Immunol. 35:3–10. 2017.PubMed/NCBI View
Article : Google Scholar
|
|
11
|
Bommersbach TJ, Lapid MI, Leung JG,
Cunningham JL, Rummans TA and Kung S: Management of psychotropic
drug-induced DRESS syndrome: A systematic review. Mayo Clin Proc.
91:787–801. 2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Misthaq AR, Pirasath S and Sugathapala AG:
DRESS syndrome associated with sulfasalazine therapy. Jaffna Med J.
31:46–47. 2019.
|
|
13
|
Ozdemir O and Genc G: Drug reaction with
eosinophilia and systemic symptoms syndrome associated with
ampicillin-sulbactam and clindamyc in: A case report. Istanb Med J.
20:256–260. 2019.
|
|
14
|
Kang SY, Kim J, Ham J, Cho SH, Kang HR and
Kim HY: Altered T cell and monocyte subsets in prolonged immune
reconstitution inflammatory syndrome related with DRESS (drug
reaction with eosinophilia and systemic symptoms). Asia Pac
Allergy. 10(e2)2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Pereira de Silva N, Piquioni P, Kochen S
and Saidon P: Risk factors associated with DRESS syndrome produced
by aromatic and non-aromatic antipiletic drugs. Eur J Clin
Pharmacol. 67:463–470. 2011.PubMed/NCBI View Article : Google Scholar
|