Case presentation
A 79-year old female presented with acute chest pain
after watching the daily TV report on the death toll of COVID-19
pandemic. Her medical history included arterial hypertension under
treatment with ace-inhibitors. She was haemodynamically stable,
with a blood pressure of 130/70 mmHg, a heart rate of 75 beats/min
in sinus rhythm, and an oxygen saturation of 99% in room air.
Physical examination and body temperature were normal.
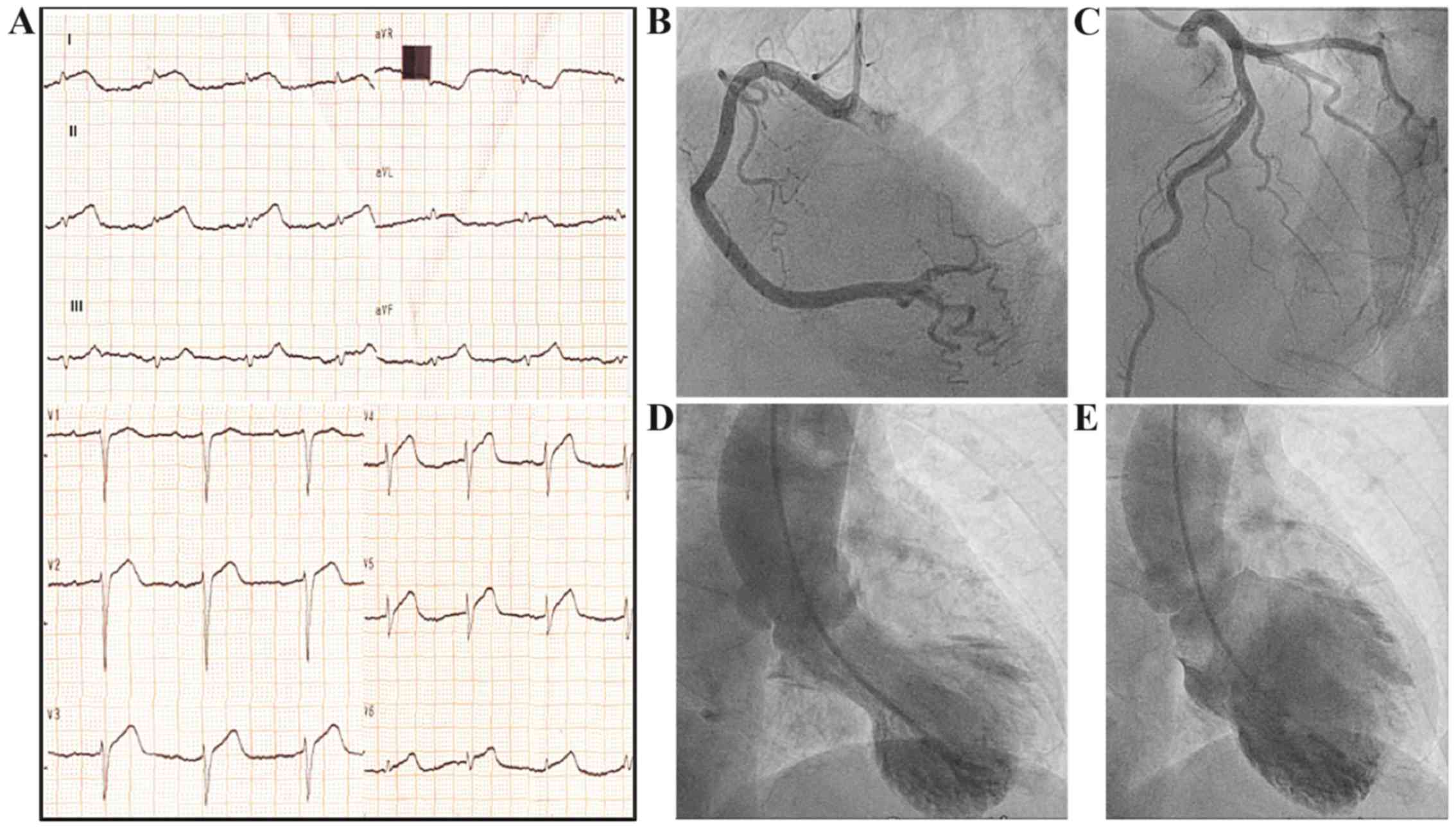
Electrocardiogram recorded diffuse ST segment elevation (Fig. 1A). Emergency coronary angiography
excluded stenotic lesions (Fig. 1B
and C). Left ventriculography
illustrated severe hypokinesia in the mid-apical segments,
hyperdynamic basal segments (Fig.
1D, systole; and E, diastole),
and impaired left ventricular systolic function with an ejection
fraction of 35%. High sensitive troponine-T was elevated reaching a
peak after 12 h (2.950 pg/ml, normal <15.6 pg/ml), whereas other
routine blood tests, including inflammatory markers, were
normal.
The diagnosis
Stress induced (Takotsubo) cardiomyopathy.
Discussion
Takotsubo cardiomyopathy (TC), also called
stress-induced cardiomyopathy, mimics an acute coronary syndrome
(ACS), predominantly affecting elderly women and is triggered by an
emotional or physical stressor (1),
in our case the COVID-19 death update. The term ‘Takotsubo’ means
‘octopus pot’ in Japanese and describes the pathognomonic left
ventricular end-systolic apical ballooning, illustrated in
transthoracic echocardiogram (TTE) and left ventriculography during
cononary angiography (1).
Clinical presentation, electrocardiographic
findings, and biomarker profiles are similar to those of an ACS
(2). TC represents an acute heart
failure syndrome with substantial morbidity and mortality (2). The in-hospital and one-year mortality
of TC has been reported 1-5 and 5.6%, respectively, with a
recurrence rate of ≤5% (1,2). Left ventricular systolic function
usually recovers within four weeks (1). TC is characterized by a low-grade
chronic inflammatory state consisting of myocardial macrophage
inflammatory infiltrates, substantial increase in the
pro-inflammatory, classical monocyte subset
CD14++CD16-, and an increase in the systemic
pro-inflammatory cytokines interleukin-6 (IL-6), IL-8 and chemocine
CXCL1(3). This localized and
systemic inflammatory response plays a pivotal role in the
development of TC, while it might also serve as a promising
therapeutic target for which no effective treatment currently
exists (3).
Τhe brain-heart interaction has been acknowledged as
a significant factor in the pathogenesis of TC. Overstimulation of
the sympathetic nervous system is hypothesized as the underlying
mechanism (2,4). The hypothalamic-pituitary-adrenal axis
(HPA-axis) is a major neuroendocrine system which regulates the
release of cortisol from the adrenal gland, shifting the metabolism
to higher stress levels. Higher serum cortisol levels and increased
sympathetic activity may cause myocardial damage (5). Consequently, acute psychological or
physical stress mediated via the sympathetic-adrenal- medulla axis
with catecholamine release in the adrenal medulla and the HPA axis
with consecutive cortisol release from the adrenal cortex may act
as a trigger for TC (5).
Additionally, regional differences in myocardial expression of
β2-adrenergic receptor density have been shown, which mediate the
cellular effects of the increased catecholamine blood
concentrations and explain the regional left ventricular myocardial
stunning (5).
Therefore, the enormous psychological strain posed
on the community by the pandemic can activate the brain-heart axis
and serve as a potential stressor for TC (4,6).
COVID-19 pandemic has caused an unprecedented health crisis
resulting in individual and societal fear and anxiety, with
emerging cardiovascular implications, which we should be aware of
(4).
The patient was transferred to the coronary unit
where treatment with ace-inhibitor, aspirin, b-blocker and statin
was initiated. Her course was uncomplicated with gradual
normalization of troponin. She was discharged after one week in
good condition and normal echocardiography, and was advised to
avoid following news related to the pandemic.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Not applicable
Authors' contributions
SG and AST wrote the original draft, edited and
critically revised the manuscript. KT, DT, DV, ER, PT, LEP, MSK,
DAS and AJM critically revised and edited the manuscript. All
authors substantially contributed to the conception, writing and
revision of the work and approved the final content of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this article.
The other authors declare that they have no competing
interests.
References
|
1
|
Dagres N, Triantafyllis A and
Anastasiou-Nana M: A 70 year old woman with chest pain after a
stressful event. BMJ. 347(f5583)2013.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Templin C, Ghadri JR, Diekmann J, Napp LC,
Bataiosu DR, Jaguszewski M, Cammann VL, Sarcon A, Geyer V, Neumann
CA, et al: Clinical features and outcomes of Takotsubo (Stress)
cardiomyopathy. N Engl J Med. 373:929–938. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Scally C, Abbas H, Ahearn T, Srinivasan J,
Mezincescu A, Rudd A, Spath N, Yucel-Finn A, Yuecel R, Oldroyd K,
et al: Myocardial and systemic inflammation in acute stress-induced
(Takotsubo) cardiomyopathy. Circulation. 139:1581–1592.
2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Τsamakis K, Triantafyllis AS, Tsiptsios D,
Spartalis E, Mueller C, Tsamakis C, Chaidou S, Spandidos DΑ, Fotis
L, Economou M and Rizos E: COVID-19 related stress exacerbates
common physical and mental pathologies and affects treatment
(Review). Exp Ther Med. 20:159–162. 2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Buchmann SJ, Lehmann D and Stevens CE:
Takotsubo cardiomyopathy-acute cardiac dysfunction associated with
neurological and psychiatric disorders. Front Neurol.
10(917)2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Tsamakis K, Rizos E, Manolis AJ, Chaidou
S, Kympouropoulos S, Spartalis E, Spandidos DA, Tsiptsios D and
Triantafyllis AS: COVID-19 pandemic and its impact on mental health
of healthcare professionals. Exp Ther Med. 19:3451–3453.
2020.PubMed/NCBI View Article : Google Scholar
|