Introduction
Patients with severe recalcitrant infectious
keratitis exhibit deep ulcers, corneal neovascularization, anterior
chamber empyema and a wide range of infections when compared with
common infectious corneal ulcers (1). Affected eyes are at risk of severe
complications including corneal perforation and spreading of
infection to adjacent tissues, which may require subsequent
enucleation (2). In cases where
medical therapy is insufficient, therapeutic penetrating
keratoplasty (TPK) may be promptly considered (3,4).
However, due to the poor pre-operative corneal condition, the early
post-operative intraocular inflammatory response is more serious
than that of non-severe patients (5). Therefore, further research into early
post-operative anti-inflammatories is required.
In the majority of TPK cases, glucocorticoid eye
drops are the gold standard for early anti-inflammatory
post-surgical treatment to reduce intraocular inflammation and
prevent immunological graft rejection (6). However, glucocorticoid eye drops may be
undesirable and possibly contraindicated due to the increased risk
of infection recurrence and lasting infection in patients with
severe infectious keratitis following TPK, particularly affecting
those with fungal corneal ulcers (7). Therefore, research into alternative
anti-inflammatory drugs is required to replace traditional
glucocorticoid treatment in patients with severe infectious
keratitis that have received TPK.
Tacrolimus, which is a macrolide antibiotic purified
from the metabolites of streptavidin, is a novel immunosuppressive
agent that exerts immunosuppressive activity by inhibiting
calcineurin (8). In ophthalmology,
tacrolimus eye drops are mainly administered to prevent rejection
after corneal transplantation (9),
vernal conjunctivitis (10),
refractory inflammatory ocular surface disease (11) and ocular surface problems of
graft-versus-host disease (12).
Previous research into tacrolimus eye drop treatment following
corneal transplantation has aimed to prevent rejection (9,13,14). To
the best of our knowledge, no previous study has assessed early
intraocular inflammation management.
The current study retrospectively evaluated the
effect of tacrolimus eye drops on post-operative inflammation
following TPK treatment in patients with severe infectious
keratitis.
Materials and methods
The current study protocol was approved by the
Institutional Review Board of Capital Medical University, Beijing
Tongren Hospital and conducted in accordance with the Declaration
of Helsinki. Patients provided their written informed consent for
enrollment prior to surgery and oral consent was obtained for the
analysis and publication of their data. Additionally, patients
received an oral explanation regarding the analysis and publication
of relevant data.
Inclusion and exclusion criteria
The present retrospective study included 20 patients
who underwent TPK surgery between January and May in 2017 in the
Beijing Tongren Eye center (Beijing, China). The patients comprised
14 males and 6 females. The average age was 57.1±10.77 years
(range, 40-70 years). Patients included in the current study
underwent TPK and had positive corneal scraping culture results.
Patients suspected of bacterial keratitis routinely underwent
aerobic culture of the specimen. Corneal scrapings were inoculated
onto nutrient broth, blood agar plate (0.05% Defibrinated Sheep
Blood), MacConkey and Chocolate Agar Plate (0.05% Defibrinated
Sheep Blood) medium (Beijing Solarbio Science & Technology Co.,
Ltd.). Subsequently, samples were incubated for 1-2 days at 28˚C
and 50% humidity and isolated individual colonies. The Kirby-Bauer
method (Disc diffusion method) was used to determine antibiotic
sensitivity of different antibiotics. The antibiotics tested were
all purchased from Beijing Solarbio Science & Technology Co.,
Ltd. and included Amikacin (30 µg), Ceftazidime (30 µg), Cefoxitin
(30 µg), Ciprofloxacin (5 µg), Gentamicin (120 µg), Ofloxacin (5
µg), Levofloxacin (5 µg), Rifampicin (5 µg), Moxifloxacin (5 µg),
Gatifloxacin (5 µg), Oxacillin (1 µg). Potato Dextrose Agar (PDA)
(Beijing Luqiao Technology Co., Ltd.) was selected as medium for
specimens suspected as fungal keratits. Specimens were placed in
Thermostatic-Humidistat Cultivating Box at 28˚C and 40% humidity
for 3 to 10 days. After that, the colonies in the positive
specimens were isolated and transferred to PDA dishes (Tianjin
Jinzhang Company). The Rosco paper diffusion method (Neo-Sensitab
drug sensitive paper; Rosco Diagnostica) was used for drug
sensitivity test. Test drugs include: Natamycin (50 µg; Rosco
Diagnostica), Terbinafine (30 µg; Rosco Diagnostica), Itraconazole
(8 µg; Rosco Diagnostica), Fluconazole (15 µg; Rosco Diagnostica),
Amphotericin B (15 µg, Rosco Diagnostica), Voriconazole (1 µg;
Rosco Diagnostica). The diagnostic criteria of severe infectious
keratitis (1) was as follows:
Corneal ulcer area >6 mm2 or lesion depth >2/3 of
corneal thickness; presence of anterior chamber exudate or empyema;
and corneal ulcer perforation or descemetocele. The criteria for
surgery for patients with severe infectious keratitis (15) were: No healing after 7 days of
standard treatment; descematocele with infiltrates; and corneal
perforation >3 mm with active inflammation. All corneal
transplants were performed by the same surgeon (JY) in Beijing
Tongren Eye center (Beijing, China). Excluded patients had a
history of previous corneal transplant and/or had congenital eye
pathologies, such as cornea dystrophy or leucoma.
Patient information
The patients were diagnosed with bacterial keratitis
(n=8) or fungal keratitis (n=12). Each diagnosis was supported by a
positive culture in all cases. Pre-operative assessment indicated
that the patients exhibited iris adhesions (n=4), high intraocular
pressure (n=7) and anterior chamber empyema (n=12). Additionally,
17 eyes presented with pre-operative corneal neovascularization and
a single eye exhibited descemetocele. The mean recipient bed and
recipient graft were 7.8±1.3 and 8.3±1.2, respectively.
Pre-operative data are presented in Table I. Due to corneal ulcers problems,
Digital Tonometry was used as intraocular pressure measurement. (Tn
represented normal pressure. T+1, T+2 and T+3 indicated different
degrees of intraocular pressure increase, with T+3 as the highest).
Corneal perforation or descemetocele was denoted as ‘1 point’, and
the absence of these was denoted as ‘0 points’. A lack of iris
adhesion was recorded as ‘0 point’. If iris adhesion was it was
assigned a score of 1 to 4 quadrants, which was correspondingly
recorded as ‘1-4 points’. The height of hypopyon (h) was based on
the vertical diameter of the cornea. Ulcer depth was based on
central cornea thickness. Ulcer size, ulcer depth and the height of
hypopyon were measured using Image Processing Software (vision
11.0; EdgeView, Apple Corporation). TPK sites were divided into
orthotopic (O) and partial (P) transplantation. Corneal
vascularization was divided into 1-4: 1, ≤25% corneal diameter; 2,
≤50% corneal diameter; 3, ≤75% corneal diameter; 4, ≤100% corneal
diameter. For example, (2,1) represents corneal vascularization
involving 2 quadrants, <25% of the corneal diameter.
 | Table ICornea characteristics prior to
surgery. |
Table I
Cornea characteristics prior to
surgery.
| No. | Sex | Age (years) | Etiological
diagnosis | Corneal
performation | Synechia | IOP | Hypopyon (h) | Ulcer size (mm) | Ulcer depth
(CCT) | Vascularizatio
(quadrant, range) | Descemetocele | Site (O/P) | Recipient bed | Recipient
grafts |
|---|
| 1 | M | 60 |
Fusarium | 0 | 0 | Tn | 1/7 | 4x5 | 2/3 | 2,1 | 0 | O | 9.5 | 10.0 |
| 2 | M | 63 |
Alternaria | 0 | 0 | Tn | 1/5 | 10x7 | 5/6 | 1,1 | 0 | O | 9.0 | 9.5 |
| 3 | M | 48 | Staphylococcus
aureus | 0 | 1 | T+1 | 1/2 | 8x6 | 2/3 | 1,1 | 0 | O | 9.5 | 10.0 |
| 4 | M | 46 | Fusarium
solani | 0 | 0 | T+1 | 1/2 | 8x10 | 2/3 | 0 | 0 | O | 9.5 | 10.0 |
| 5 | F | 61 | Aspergillus
fumigatus | 0 | 0 | T+1 | 1/2 | 5x5 | 2/3 | 0 | 0 | O | 7.0 | 7.5 |
| 6 | M | 63 |
Alternaria | 0 | 1 | T+1 | 1/7 | 5x5 | 2/3 | 1,1 | 0 | O | 7.0 | 7.5 |
| 7 | F | 57 | Staphylococcus
epidermidis | 0 | 0 | Tn | 0 | 7x10 | 3/4 | 3,1 | 0 | O | 9.0 | 9.5 |
| 8 | M | 57 | Candida
albicans | 0 | 0 | Tn | 1/10 | 5x5 | 2/3 | 0 | 0 | O | 7.0 | 7.5 |
| 9 | F | 66 | Fusarium
solani | 0 | 0 | T+1 | 1/2 | 10x5 | 3/4 | 4,1 | 0 | O | 5.5 | 6.0 |
| 10 | M | 64 | Aspergillus
fumigatus | 0 | 4 | T+3 | 0 | 5x8 | 3/4 | 3,1 | 1 | O | 7.0 | 7.5 |
| 11 | F | 65 | Fusarium
solani | 0 | 0 | Tn | 1/5 | 5x6 | 1/2 | 1,2 | 0 | O | 8.25 | 8.8 |
| 12 | M | 64 |
Fusarium | 0 | 0 | Tn | 1/2 | 6x5 | 2/3 | 1,1 | 0 | P | 9.5 | 9.5 |
| 13 | M | 30 | Pseudomonas
aeruginosa | 0 | 0 | Tn | 0 | 6x5 | 2/3 | 4,1 | 0 | O | 7.0 | 7.5 |
| 14 | F | 40 | Fusarium
solani | 0 | 0 | Tn | 1/2 | 10x8 | 1/2 | 2,1 | 0 | O | 9.0 | 9.5 |
| 15 | M | 50 |
Fusarium | 0 | 0 | Tn | 0 | 5x3 | 2/3 | 3,1 | 0 | O | 7.0 | 7.5 |
| 16 | M | 40 |
Fusarium | 0 | 0 | Tn | 0 | 4x4 | 1/2 | 4,1 | 0 | O | 6.0 | 6.5 |
| 17 | M | 67 | Staphylococcus
aureus | 0 | 0 | Tn | 0 | 5x4 | 3/4 | 1,1 | 0 | O | 7.0 | 7.5 |
| 18 | F | 63 |
Fusarium | 0 | 0 | Tn | 0 | 4x4 | 3/4 | 1,1 | 0 | O | 9.0 | 9.5 |
| 19 | M | 68 | Pseudomonas
aeruginosa | 0 | 1 | T+1 | 1/5 | 8x5 | 2/3 | 2,1 | 0 | O | 7.0 | 7.5 |
| 20 | M | 70 | Staphylococcus
epidermidis | 0 | 0 | Tn | 0 | 4x4 | 3/4 | 1,1 | 0 | O | 7.0 | 7.5 |
Anterior chamber washout and
penetrating keratoplasty
All corneal transplants were performed with similar
technique by the same surgeon at Tongren Eye Hospital (14,16).
Donor corneas were stored in OptiSol storage media (Bausch &
Lomb Co., Ltd.) for 7-10 days at 4˚C. The host trephine size was
selected to completely cover the infiltrate edge of the ulcer and
was oversized by 0.25 mm. Anterior chamber washout was performed in
patients with anterior chamber hypopyon as previously described by
Jia et al (17). Furthermore,
patients with synechia or severe anterior chamber empyema prior to
surgery underwent peripheral iridotomy at the 12 o'clock position
at the time of surgery (18). The
cornea grafts were sutured to the host with 16 interrupted 10-0
monofilament nylon sutures. Suture knots were trimmed and buried
toward the donor side. In all cases, the excised host cornea was
sent for microbiologic and histopathologic examination in Beijing
Tongren Eye center (Beijing, China).
Post-operative medication regimen
Selection of the appropriate antibiotic eye drops
and topical antimicrobial agents was based on the microbiological
profile and specific sensitivities of the causative infective agent
(19).
Quinolone eye drops were administered to all
patients as the culture results indicated that gram positive cocci
infections were present. The current study administered 5 ml 0.5%
gatifloxacin eye drops (Anhui Shuangke Pharmaceutical Co., Ltd.) 4
times/day with 5 g 0.3% gatifloxacin gel (Shenyang Xingqi Eye
Medicine Co., Ltd.) 3 times/day for 2 weeks then gradually reduced
the amount according to corneal condition.
All cases of fungal infection were treated with 5 ml
5% natamycin eye drops (Hubei Pharmaceutical Co., Ltd.) and 0.5%
fluconazole eye drops (Yongguang Pharmaceutical Co., Ltd.) 4
times/day for 2 weeks then gradually reduced the amount according
to corneal condition.
Furthermore, 5 mg 0.1% tacrolimus eye drops (Senju
Pharmaceutical Co., Ltd.) were applied 4 times/day for 2 months
then gradually reduced the amount according to corneal condition
starting on the first day post-surgery for all patients.
Steroid eye drops were not administered during the
first post-operative month. However, after a period of one month,
if no signs of active inflammation were present, 1% prednisolone
acetate (Allergan Pharmaceutical Co., Ltd.) was added to the
treatment regimen and applied 4 times/day for a month then
gradually reduced the amount according to corneal condition.
Additionally, 0.3% tobramycin/0.1% dexamethasone eye ointment (S.A.
Alcon Couvreur Pharmaceutical Co., Ltd.) was applied one time at
night for one month (20). After 6
months, the frequency of prednisolone eye drops was reduced to
twice/day and after one year, to once/day. Prednisolone was stopped
after a period of two years.
Follow-up
Eyes were examined daily using a slit lamp (YZ5S
digital slit lamp microscope, Shanghai Hanfei Medical Equipment
Co., Ltd.) for the first 3 post-operative days, then re-examined
once a week and at weekly intervals thereafter for the first month.
Routine examination included uncorrected visual acuity (Snellen
visual acuity chart), intraocular pressure and slit biomicroscopy
examinations. Icare rebound tonometer (TAO1i; Icare Finland Oy) was
selected for intraocular pressure measurement. Digital tonometry
was selected if Icare couldn't get results due to cornea condition.
Slit biomicroscopy was operated by the same skilled
ophthalmologist.
Observation of early post-operative
inflammatory response
The absorption of intraocular inflammation in the
early post-operative period (one month) was assessed under a slit
lamp biomicroscopy. All examinations were operated by the same
ophthalmologist who performed the surgeries. The following
parameters were assessed. The scoring of aqueous flare, aqueous
cells, cellulose exudation and hyphema presence were graded
according to the uveitis inflammation scoring criteria (21). The graft transparency, degree of
graft edema and corneal neovascularization were graded according to
the cornea rejection scoring criteria (22). These items included graft clarity,
graft edema, neovascularization, anterior chamber flare, anterior
chamber cells and exudation received between 0-4 points. Hyphema
received a score of between 0-3 points. When the signs were more
severe, the scores were higher. The grading systems are summarized
in Table II.
| Table IIIntraocular inflammation and graft
survival state evaluation criteria. |
Table II
Intraocular inflammation and graft
survival state evaluation criteria.
| Score | Graft clarity | Graft edema |
Neovascularization | Anterior chamber
flare | Anterior chamber
cells, n | Hyphema | Exudation |
|---|
| 0 | Clear cornea | None | None | None | <5 | 0 | N/A |
| 1 | Slight haze,
details of iris clearly visible | Mild stromal
thickness | Neovascularization
of peripheral cornea | Faint | 6-15 | 0-1/3 | Yarn-like
exudation |
| 2 | Increased haze,
some details of iris no longer visible | Diffuse stromal
edema | Neovascularization
appearing in the graft periphery | Moderate (iris and
lens details clear) | 16-25 | 1/3-2/3 | Cluster-like
exudation |
| 3 | Advanced haze,
pupil still recognizable | Pronounced edema
with small bleb of epithelium | Neovascularization
extending deeper | Marked (iris and
lens details hazy) | 26-50 | 2/3-1 | Transparent mash in
front of the lens or behind the cornea |
| 4 | Opaque cornea
without view of anterior chamber | Bullous
keratopathy | Neovascularization
extending to the entire graft | Intense (fibrin or
plastic aqueous) | >50 | N/A | Pre-iridal adhesion
or Post-iridal adhesion |
S was defined as the post-operative early
intraocular inflammation absorption fraction and was calculated as
the difference between the post-exudation scores on the first day
(T1d) and after one month (T1m; S=T1d-T1m). Additionally, ΔS was
defined as the graft survival state and is the difference between
the graft state on the first post-operative day (SS1d) and one
month post-surgery (SS1m).
Long-term PK results
All 20 patients were followed up for 12-18 months.
Visual acuity, intraocular pressure and thorough slit lamp eye
exams were performed at every visit and symptoms and complications
were documented.
Statistical methods
SPSS software (version 23.0; IBM Corp) was used for
statistical analysis. Data were tested for normality using the
Kolmogorov-Smirnov test and provided as mean and standard deviation
(SD). A paired sample t-test was used to compare the difference
between T1d and T1m and the difference between SS1d and SS1m.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Case data analysis
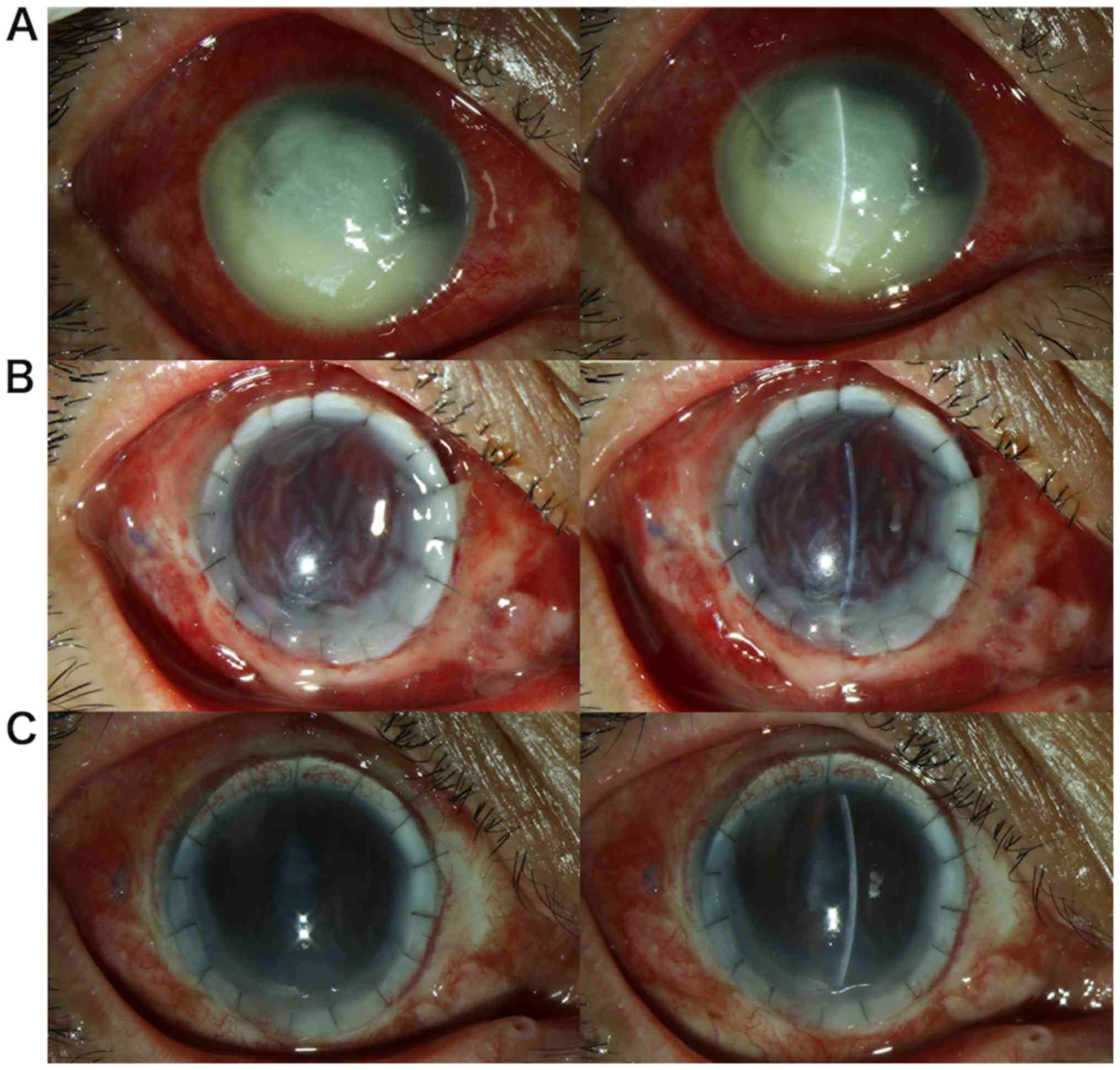
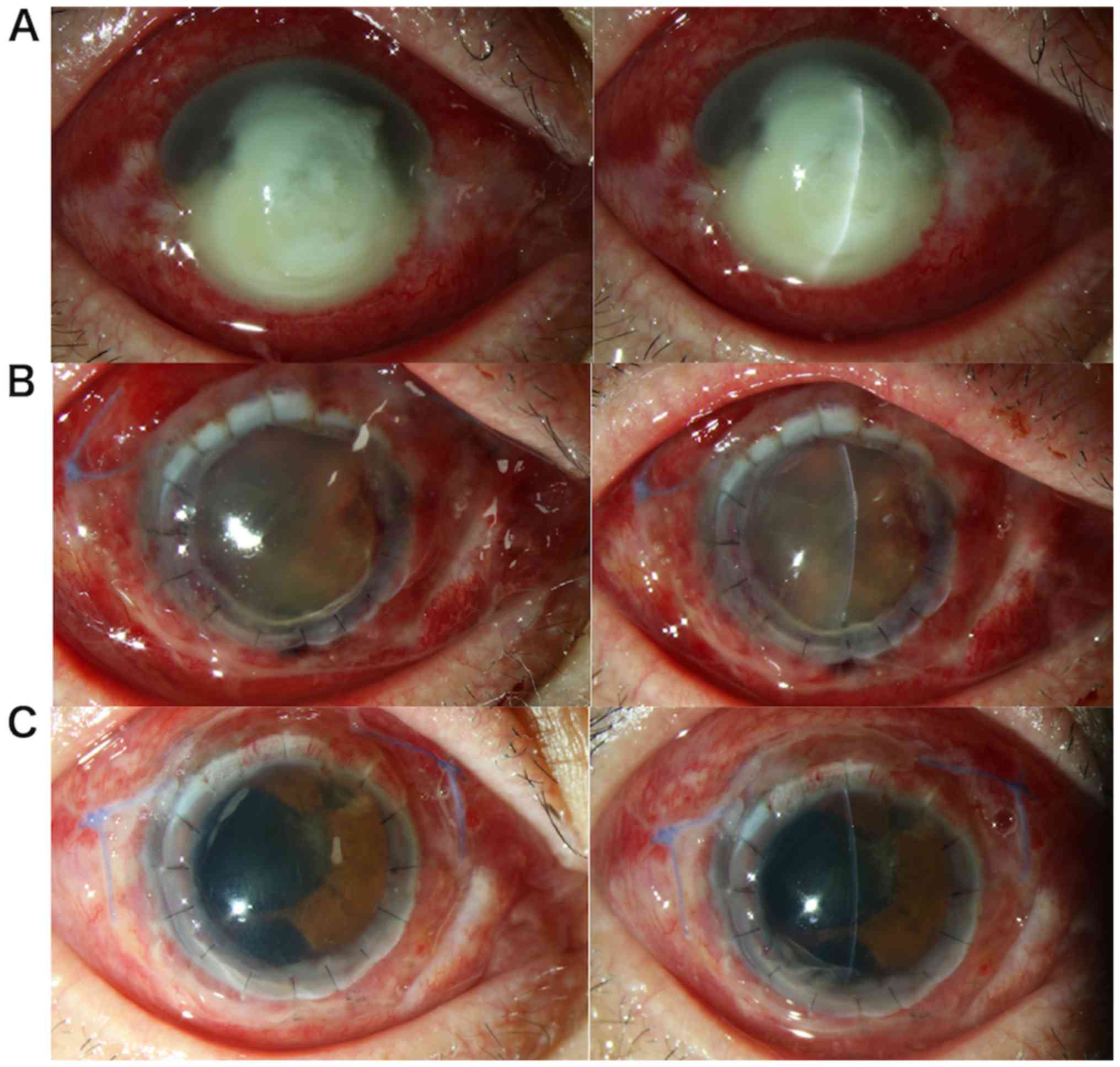
Post-operative inflammatory responses (T1d, T1m and
S) and graft survival state scores (SS1d, SS1m and ΔS) are
summarized in Table III. The
average score of intraocular inflammation was 7.4±2.06 on the first
day and 2.0±2.47 by the first post-operative month. The mean of S
was 5.4±2.13. This difference was statistically significant
(P<0.01). The average of SS1d was 5.3±1.56 and 3.8±1.24 for
SS1m. ΔS was also statistically significant (P<0.01) Early
postoperative anterior images of 2 patients are depicted in
Figs. 1 and 2.
| Table IIIPost-operative intraocular
inflammatory response and graft survival state scores. |
Table III
Post-operative intraocular
inflammatory response and graft survival state scores.
| Patient no. | T1d | T1m | S | SS1d | SS1m | ΔS |
|---|
| 1 | 10 | 2 | 8 | 6 | 4 | 2 |
| 2 | 7 | 0 | 7 | 5 | 3 | 2 |
| 3 | 7 | 4 | 3 | 6 | 3 | 3 |
| 4 | 10 | 4 | 6 | 7 | 4 | 3 |
| 5 | 10 | 6 | 4 | 3 | 2 | 1 |
| 6 | 5 | 0 | 5 | 4 | 2 | 2 |
| 7 | 8 | 0 | 8 | 3 | 2 | 1 |
| 8 | 5 | 0 | 5 | 6 | 2 | 4 |
| 9 | 8 | 4 | 4 | 7 | 5 | 2 |
| 10 | 5 | 4 | 1 | 7 | 5 | 2 |
| 11 | 4 | 1 | 3 | 2 | 5 | -3 |
| 12 | 5 | 2 | 3 | 4 | 4 | 0 |
| 13 | 7 | 0 | 7 | 7 | 6 | 1 |
| 14 | 9 | 1 | 8 | 5 | 4 | 1 |
| 15 | 6 | 0 | 6 | 5 | 4 | 1 |
| 16 | 9 | 2 | 7 | 7 | 4 | 3 |
| 17 | 6 | 0 | 6 | 5 | 3 | 2 |
| 18 | 7 | 0 | 7 | 4 | 4 | 0 |
| 19 | 11 | 9 | 2 | 6 | 6 | 0 |
| 20 | 9 | 1 | 8 | 7 | 4 | 3 |
| Mean | 7.4±2.06 | 2.0±2.47 | 5.4±2.13 | 5.3±1.56 | 3.8±1.24 | 1.5±1.50 |
| P-value | | | <0.01 | | | <0.01 |
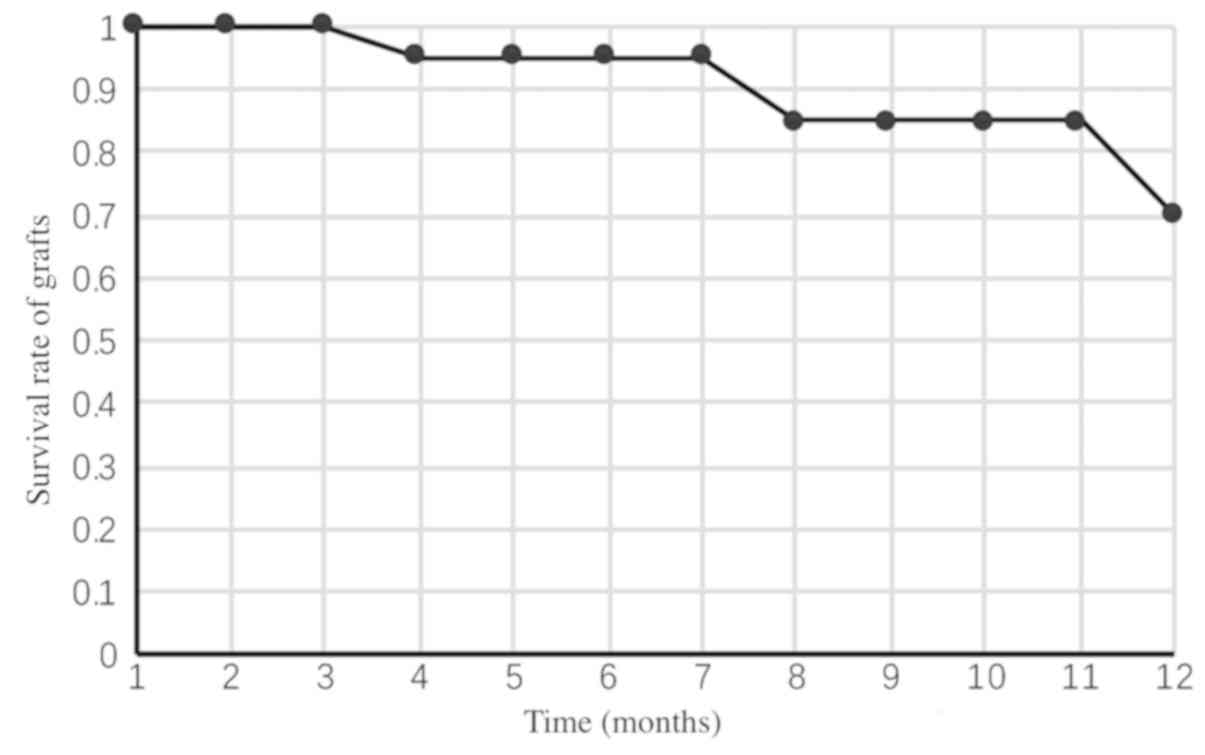
Long-term TPK follow-up
Of the 20 patients, 6 cases resulted in transplant
failure. In these cases, 4 were due to rejection, a single case was
due to corneal epithelial defects and a further case was caused by
uncontrolled infection recurrence. Patient follow-up times and
final outcomes are presented in Table
IV. The survival rates of the grafts are presented in Fig. 3. At 4 months post-surgery, one
patient exhibited transplant rejection leading to graft failure.
Two cases exhibited failure at 8 months post-surgery, one of which
was due to persistent epithelial defects. There were three cases of
graft failure at 11 months post-surgery, two of which were due to
rejection and one failed due to the recurrence of fungal
infection.
| Table IVPatient follow-up times and
prognosis. |
Table IV
Patient follow-up times and
prognosis.
| Case (no.) | Follow-up timepoint
(weeks) | Prognosis |
|---|
| 1 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 32, 33 | Occured at 32nd
week after surgery; persistent epithelial defects; resulting in
failure of grafting; epithelial being stable by wearing bandage
soft contact lens |
| 2 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 36 | No graft failure or
complications and the graft kept clear |
| 3 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 35, 70 | No graft failure or
complications and the graft kept clear |
| 4 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 48, 49 | Occurred at 48th
weeks after surgery; endothelial rejection; reversal after drug
treatment |
| 5 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 37, 72 | No graft failure or
complications and the graft kept clear |
| 6 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 32, 33 | Occurred at the
16th week after surgery; epithelial rejection; reversal after drug
treatment |
| 7 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 48 | No graft failure or
complications and the graft kept clear |
| 8 | 1/7, 2/7, 3/7, 1,
3, 4, 12, 24, 49 | No graft failure or
complications and the graft kept clear |
| 9 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 48 | No graft failure or
complications and the graft kept clear |
| 10 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 48, 49, 72 | Occurred at the
48th week after surgery; endothelial rejection; secondary glaucoma;
abandon treatment |
| 11 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 48 | No graft failure or
complications and the graft kept clear |
| 12 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 22, 45 | No graft failure or
complications and the graft kept clear |
| 13 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 70 | no graft failure or
complications and the graft kept clear |
| 14 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 47 | No graft failure or
complications and the graft kept clear |
| 15 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 6, 7 | Occurred at 32nd
week after surgery; secondary infection; resulting in failure of
grafting; secondary transplantation after drug treatment |
| 16 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 48 | No graft failure or
complications and the graft kept clear |
| 17 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 71 | No graft failure or
complications and the graft kept clear |
| 18 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 48 | No graft failure or
complications and the graft kept clear |
| 19 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 24, 48, 49, 70 | Occurred at the
48th week after surgery, endothelial rejection, reversal after drug
treatment |
| 20 | 1/7, 2/7, 3/7, 1,
2, 3, 4, 12, 23, 50 | No graft failure or
complications and the graft kept clear |
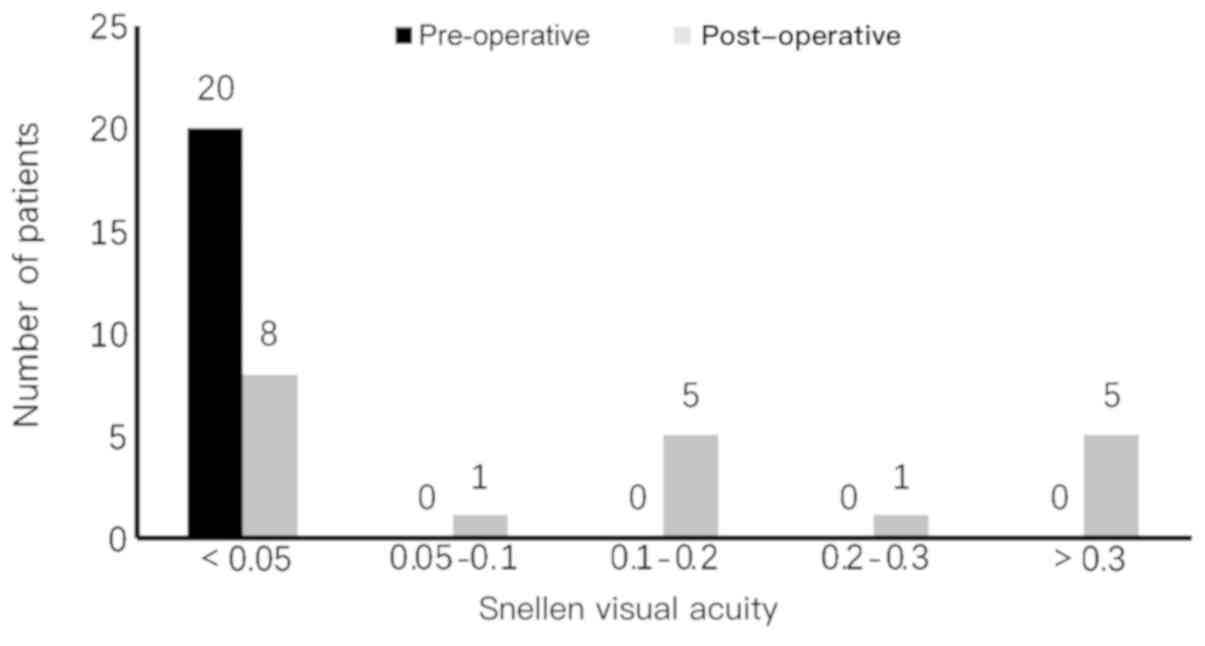
Visual acuity prognosis
The pre-operative visual acuity examination for all
20 patients was light perception. Post-operative visual acuity
increased in 16 patients, decreased in 2 patients and 2 patients
maintained pre-operative visual acuity. The specific vision changes
prior to surgery and the best measured uncorrected visual acuity
during the follow-up period are presented in Fig. 4. The pre-operative visual acuity of
all patients was <0.05 and the optimal visual acuity after
surgery was improved compared with that before surgery.
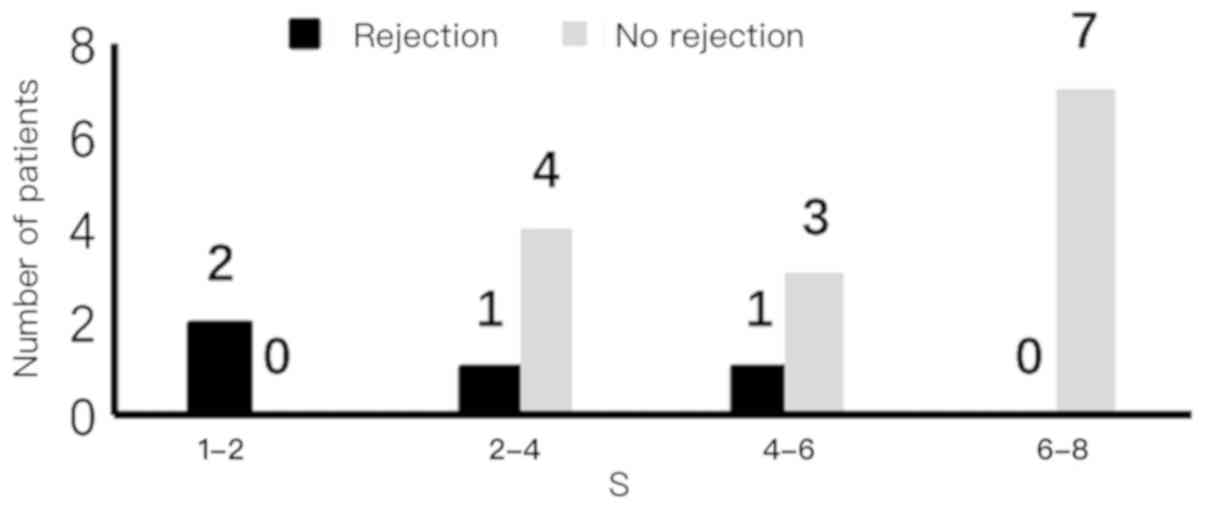
An association between early post-operative
inflammatory absorption and long-term rejection based on a 12-month
follow-up period of 20 patients was observed and is demonstrated in
Fig. 5. In the 4 patients who
exhibited transplant rejection, the early inflammatory absorption
scores were relatively low, suggesting that long-term graft
rejection may have a relationship with poor early inflammation
control.
Complications during post-operative
follow-up
Post-operative complications included a persistent
corneal epithelial defect that ultimately led to failure. A total
of 3 cases were diagnosed with secondary fungal infections (at 6, 8
and 11 months after surgery), of which 2 cases were medically
controlled and a single case resulted in graft failure.
Additionally, one patient developed secondary glaucoma and lost
light perception in that eye. One patient with a 9.5 mm graft had
persistent epithelial defects which ultimately healed by wearing a
soft bandage contact lens.
Discussion
The current retrospective study utilized tacrolimus
eye drops in patients with severe infectious keratitis post-TPK at
Beijing Tongren Hospital. During post-operative follow-up, it was
determined that the drops had an effect on intraocular inflammation
absorption. By reviewing post-operative follow-up patient records
(vision and corrected vision, intraocular pressure and anterior
angiography), a post-operative intraocular inflammatory management
effect of tacrolimus eye drops was observed. According to patient
follow-up time, the condition of the corneal grafts was monitored
and anti-infectives were ceased after the second week. Observation
then continued for 2 weeks until the risk of infection recurrence
had been reduced to very low. At this time, due to the risk of
rejection in high-risk corneal transplantation, glucocorticoids eye
drops were gradually added to the treatment regimen (23). A period of one month post-surgery was
a turning point in terms of drug use and changes in the condition
and in this turning point inflammation of patients was absorbed
significantly. Due to this, one-month post-TPK was defined as an
early post-operative time point in the current study.
Severe post-operative inflammation can result from
an underlying corneal infection and can increase due to severe
neovascularization of the cornea prior to surgery (24) and large corneal grafting (25). To reduce intraocular inflammation,
corticosteroids were the preferred anti-inflammatory drug (19). Intraocular injection of tissue
plasminogen activator may also promote anterior chamber exudation
following TPK (26).
However, for infectious keratitis, especially fungal
keratitis, glucocorticoid drugs are contraindicated considering the
recurrence of infection after TPK (15).
Yu et al (27)
demonstrated in vitro that tacrolimus significantly reduced
pro-inflammatory cytokine expression and increased the
anti-inflammatory cytokine expression in lipopolysaccharide-induced
keratitis. Sakuma et al (28)
also revealed that tacrolimus serves anti-inflammatory and
immunosuppressive roles by inhibiting the release of interleukin
(IL)-2, IL-3, IL-4, interferon γ and granulocyte-macrophage colony
stimulating factor and by inhibiting IL-2 receptor expression in
T-helper (Th) cells. Tacrolimus treatment has demonstrated
significant cytokine production inhibition when compared with
steroids (28). Furthermore, when
compared with glucocorticoid eye drops, which inhibit multiple
pathways of the immune process (29)
by modulating the production of certain proteins including
lipocortin and enzymes, tacrolimus eye drops primarily inhibit
Th1/Th2 cell cytokines by inhibiting calcium- and
calmodulin-dependent dephosphatase activity (30). This, in turn, inhibits T and B cell
activation, as well as other inflammatory cells (30). This mechanism has reportedly resulted
in fewer side effects when compared with glucocorticoid eye drops
(22).
The results of the current study demonstrated that
tacrolimus eye drops promoted the absorption of early
post-operative intraocular inflammation, primarily manifested as
the reduction of anterior chamber flare and exudation. Previous
study (31) have revealed that the
continued aggravation of the aqueous flare may be associated with a
high incidence of graft rejection. The present study revealed that
patients with long-term rejection post-surgery exhibited less
intraocular inflammation absorption scores in the early
post-operative period.
Reinfection may present as a milky white, tongue-
and endothelium-like growth at the junction of the implant and the
graft (32). Shi et al
(7) reported a post-operative
reinfection rate of 6.34% in 899 patients with fungal keratitis who
underwent TKP or lamellar keratoplasty. Among these patients, PK
accounted for 6.79% of 899 patients and a higher rate of recurrence
was identified in those with preoperative hypopyon (10.90%),
corneal perforation (12.00%), corneal infection expanding to limbus
(20.69%) or lens infection with extracapsular cataract extraction
(50%; P<0.05). In the current study, there were 3 cases of
fungal infection recurrence post-surgery. All 3 patients exhibited
varying degrees of neovascularization prior to the operation of
which 2 had anterior chamber hypopyon. There was no increase in
recurrence rate. It was speculated that this may be associated with
performing two bacterial cultures before and during the operation,
and the reasonable use of antibacterial/fungal drugs after TPK.
Dandona et al (33) reported that a higher relative risk of
graft failure was associated with host cornea vascularization prior
to transplantation in 1,725 cases for corneal transplantation in
India. Weisbrod et al (34)
revealed that corneal graft failure was associated with pathogeny
for corneal transplantation, pre-operative pre-iridal adhesion and
the presence of post-operative neovascularization. In a study of
116 cases of fungal keratitis, Li et al (35) demonstrated that when large-diameter
TPK (≥8 mm) was performed, there was a high incidence of failure.
The primary reasons were graft rejection and secondary glaucoma. In
the current study, long-term follow-up post-surgery revealed 6
cases of corneal transplant failure, 4 of which were caused by
rejection mediated by immune factors from tacrolimus and
corticosteroids eye drop use. Rejection rate has been reported to
be associated with the perioperative inflammatory response of the
patient and large corneal lesions prior to TPK (36). A previous case study of 134 patients
post-TPK for infectious keratitis by Sukhija and Jain (37) reported the most common post-operative
complications, which included secondary glaucoma, non-healing
epithelial defects and re-infection. Additionally, glaucoma
occurred more frequently in patients with pre-operative perforated
ulcers and epithelial defects were associated with grafts >9 mm.
In the current study, a single patient with a 9.5 mm graft had
persistent epithelial defects which ultimately healed by wearing a
soft bandage contact lens. Additionally, a second patient who had
pre-operative perforated ulcers developed glaucoma and eventually
lost light perception. In the present study, it was demonstrated
that tacrolimus eye drops facilitated the absorption of intraocular
inflammation in the early post-operative period of TPK and extend
long term survival of grafts in cases of severe infectious
keratitis. Future researches of multi-center including large
samples were needed.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YZ organized data, performed statistical analysis
and wrote the manuscript. SL and FR collected images and raw data.
ZL collected and interpreted the data and revised manuscript
critically for important intellectual content. YJ revised the
manuscript, made substantial contributions to conception and design
of the study and supplied the patient data used the present study.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The current study was approved by the Ethics
Committee of Beijing Tongren Hospital.
Patient consent for publication
The patient, guardian or next of kin (in case of
deceased patients) provided written informed consent for the
publication of any associated data and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jones DB: Decision-making in the
management of microbial keratitis. Ophthalmology. 88:814–820.
1981.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Yang JW, Lin HC, Hsiao CH and Chen PY:
Therapeutic penetrating keratoplasty in severe infective keratitis
using glycerol-preserved donor corneas. Cornea. 31:1103–1106.
2012.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ti SE, Scott JA, Janardhanan P and Tan DT:
Therapeutic keratoplasty for advanced suppurative keratitis. Am J
Ophthalmol. 143:755–762. 2007.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Sharma N, Sachdev R, Jhanji V, Titiyal JS
and Vajpayee RB: Therapeutic keratoplasty for microbial keratitis.
Curr Opin Ophthalmol. 21:293–300. 2010.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Cohen RA, Gebhardt BM and Bazan NG: A
platelet-activating factor antagonist reduces corneal allograft
inflammation and neovascularization. Curr Eye Res. 13:139–144.
1994.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Rahman I, Carley F, Hillarby C, Brahma A
and Tullo AB: Penetrating keratoplasty: Indications, outcomes, and
complications. Eye (Lond). 23:1288–1294. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Shi W, Wang T, Xie L, Li S, Gao H, Liu J
and Li H: Risk factors, clinical features, and outcomes of
recurrent fungal keratitis after corneal transplantation.
Ophthalmology. 117:890–896. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
MacMillan D: FK506 binding proteins:
Cellular regulators of intracellular Ca2+ signalling. Eur J
Pharmacol. 700:181–193. 2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Magalhaes OA, Marinho DR and Kwitko S:
Topical 0.03% tacrolimus preventing rejection in high-risk corneal
transplantation: A cohort study. Br J Ophthalmol. 97:1395–1398.
2013.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wan Q, Tang J, Han Y, Wang D and Ye H:
Therapeutic effect of 0.1% tacrolimus eye drops in the tarsal form
of vernal keratoconjunctivitis. Ophthalmic Res. 59:126–134.
2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lee YJ, Kim SW and Seo KY: Application for
tacrolimus ointment in treating refractory inflammatory ocular
surface diseases. Am J Ophthalmol. 155:804–813. 2013.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Tam PM, Young AL, Cheng LL and Lam PT:
Topical 0.03% tacrolimus ointment in the management of ocular
surface inflammation in chronic GVHD. Bone Marrow Transplant.
45:957–958. 2010.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Abudou M, Wu T, Evans JR and Chen X:
Immunosuppressants for the prophylaxis of corneal graft rejection
after penetrating keratoplasty. Cochrane Database Syst Rev.
(CD007603)2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Yamazoe K, Yamazoe K, Yamaguchi T, Omoto M
and Shimazaki J: Efficacy and safety of systemic tacrolimus in
high-risk penetrating keratoplasty after graft failure with
systemic cyclosporine. Cornea. 33:1157–1163. 2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Miedziak AI, Miller MR, Rapuano CJ,
Laibson PR and Cohen EJ: Risk factors in microbial keratitis
leading to penetrating keratoplasty. Ophthalmology. 106:1166–1171.
1999.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Skeens HM and Holland EJ: Large-diameter
penetrating keratoplasty: Indications and outcomes. Cornea.
29:296–301. 2010.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Jia Y, Gao H, Li S and Shi W: Combined
anterior chamber washout, amniotic membrane transplantation, and
topical use of corticosteroids for severe peripheral ulcerative
keratitis. Cornea. 33:559–564. 2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Cohen EJ, Kenyon KR and Dohlman CH:
Iridoplasty for prevention of post-keratoplasty angle closure and
glaucoma. Ophthalmic Surg. 13:994–996. 1982.PubMed/NCBI
|
|
19
|
Mannis MJ and Holland EJ: Cornea-surgery
of the cornea and conjunctiva. Fourth edition. Elsevier.
1,2(pp1952)2016.
|
|
20
|
Kharod-Dholakia B, Randleman JB, Bromley
JG and Stulting RD: Prevention and treatment of corneal graft
rejection: Current practice patterns of the Cornea Society (2011).
Cornea. 34:609–614. 2015.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Jabs DA, Nussenblatt RB and Rosenbaum JT:
Standardization of Uveitis Nomenclature (SUN) Working Group.
Standardization of uveitis nomenclature for reporting clinical
data. Results of the first international workshop. Am J Ophthalmol.
140:509–516. 2005.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Sloper CM, Powell RJ and Dua HS:
Tacrolimus (FK506) in the management of high-risk corneal and
limbal grafts. Ophthalmology. 108:1838–1844. 2001.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Rinne JR and Stulting RD: Current
practices in the prevention and treatment of corneal graft
rejection. Cornea. 11:326–328. 1992.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Williams KA, Roder D, Esterman A,
Muehlberg SM and Coster DJ: Factors predictive of corneal graft
survival. Report from the Australian corneal graft registry.
Ophthalmology. 99:403–414. 1992.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Panda A, Vanathi M, Kumar A, Dash Y and
Priya S: Corneal graft rejection. Surv Ophthalmol. 52:375–396.
2007.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Snyder RW, Sherman MD and Allinson RW:
Intracameral tissue plasminogen activator for treatment of
excessive fibrin response after penetrating keratoplasty. Am J
Ophthalmol. 109:483–484. 1990.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Yu Y, Zhong J, Peng L, Wang B, Li S, Huang
H, Deng Y, Zhang H, Yang R, Wang C and Yuan J: Tacrolimus
downregulates inflammation by regulating pro-/anti-inflammatory
responses in LPS-induced keratitis. Mol Med Rep. 16:5855–5862.
2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Sakuma S, Higashi Y, Sato N, Sasakawa T,
Sengoku T, Ohkubo Y, Amaya T and Goto T: Tacrolimus suppressed the
production of cytokines involved in atopic dermatitis by direct
stimulation of human PBMC system. (Comparison with steroids). Int
Immunopharmacol. 1:1219–1226. 2001.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Flower RJ: Eleventh Gaddum memorial
lecture. Lipocortin and the mechanism of action of the
glucocorticoids. Br J Pharmacol. 94:987–1015. 1988.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Ho S, Clipstone N, Timmermann L, Northrop
J, Graef I, Fiorentino D, Nourse J and Crabtree GR: The mechanism
of action of cyclosporin A and FK506. Clin Immunol Immunopathol.
80:S40–S45. 1996.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Küchle M, Nguyen NX and Naumann GO:
Aqueous flare following penetrating keratoplasty and in corneal
graft rejection. Arch Ophthalmol. 112:354–358. 1994.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Xie L and Shi W: Comparison of
immunological response after penetrating keratoplasty for three
kinds of infectious corneal ulcers. Chin J Ophthalmol. 18:249–251.
2000.(In Chinese).
|
|
33
|
Dandona L, Naduvilath TJ, Janarthanan M,
Ragu K and Rao GN: Survival analysis and visual outcome in a large
series of corneal transplants in India. Br J Ophthalmol.
81:726–731. 1997.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Weisbrod DJ, Sit M, Naor J and Slomovic
AR: Outcome of repeat penetrating keratoplasty and risk factors for
graft failure. Cornea. 22:429–434. 2003.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Li C, Zhao GQ, Che CY, Lin J, Li N, Jia
WY, Zhang QQ, Jiang N and Hu LT: Effect of corneal graft diameter
on therapeutic penetrating keratoplasty for fungal keratitis. Int J
Ophthalmol. 5:698–703. 2012.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Price MO, Thompson RW Jr and Price FW Jr:
Risk factors for various causes of failure in initial corneal
grafts. Arch Ophthalmol. 121:1087–1092. 2003.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Sukhija J and Jain AK: Outcome of
therapeutic penetrating keratoplasty in infectious keratitis.
Ophthalmic Surg Lasers Imaging. 36:303–309. 2005.PubMed/NCBI
|