Introduction
Atherosclerosis is a cardiovascular disease and a
systemic chronic inflammatory disease that predominantly affects
medium-sized arteries (1).
Atherosclerosis is characterized by autoimmune response damage to
the arterial wall accompanied with the subintimal accumulation of
lipids, vascular smooth muscle cells and immunocompetent cells,
which is pathologically associated with atherosclerotic plaque
development and vascular vulnerability (2-4).
In particular, pathology analysis revealed that the crucial event
in the initiation and development of atherosclerosis is endothelial
injury (5-7).
Previous studies have suggested that atherosclerosis is a
multifactorial disease triggered and sustained by a variety of risk
factors including smoking, dyslipidemia, arterial hypertension and
diabetes mellitus (4,8,9).
At present a number of techniques, including
transesophageal echocardiography, epiaortic ultrasound, magnetic
resonance imaging (MRI) and 3D ultrasound have been applied for
diagnosis of atherosclerosis (10).
A study has summarized current evidence regarding the role of
intracoronary imaging for the diagnosis and risk stratification of
coronary atherosclerosis (11). In
addition, panoramic radiography offers a cost-effective approach in
which early carotid artery calcification diagnosis and subsequent
interventions can be performed (5).
Ultrasound imaging have been widely applied for the diagnosis of
atherosclerosis (12-15).
Intravascular ultrasound (IVUS) is a more often used technique
compared with thoracic ultrasound for the diagnosis of coronary
artery disease, myocardial infarction and carotid atherosclerosis
(16). Although IVUS has proven to
be a highly valuable tool for the evaluation of mild-to-moderate
coronary lesions (17),
improvements in the diagnostic efficacy of IVUS imaging for
patients with atherosclerosis is still required.
Contrast-enhanced ultrasound can be used for the
diagnosis of different types of human atherosclerosis diseases,
including coronary artery disease and peripheral artery disease
(18). Of interest, nanoparticle
technology such as Gd2O3 incorporate a
variety of agents including anticancer compounds, fluorescent dyes
and metal ions through physical encapsulation, covalent coupling or
affinity binding for therapeutic or diagnostic applications
(19). In particular,
Gd2O3-albumin-conjugating photosensitizers
can generate clearer signals in vivo during MRI diagnosis
when coupled with enhanced imaging contrast for the effective
localization of tumors (20).
Additionally, Gd2O3 nanocrystal-based
nanocomposites have been reported to serve as an ideal dual-mode
contrast-enhancing agent for MRI by improving longitudinal
reflexivity (21), which may
provide a versatile platform for molecular imaging and targeted
drug delivery in ultrasound-facilitated diagnosis for human
diseases (22).
Mineralocorticoid receptors are downstream effectors
of angiotensin-II signaling in early atherosclerosis (23). A number of studies have recently
found that mineralocorticoid receptor antagonists can regulate
vascular function and/or contribute to vascular dysfunction
(24-26).
Eplerenone (EPL) is a specific mineralocorticoid receptor
antagonist which has been shown to strengthen endothelium-dependent
relaxation and suppress angiotensin-converting enzyme activity in
the vasculature, thereby inhibiting the development of
atherosclerosis (27).
In the present study,
Gd2O3-coated EPL
(Gd2O3-EPL) were used as the nanoparticles
contrast to explore the diagnostic efficacy of
Gd2O3-EPL combined with IVUS for patients
with suspected atherosclerosis. This study also analyzed
differences in the data obtained regarding vessel size, plaque
burden and minimal lumen area using IVUS and
Gd2O3-EPL-IVUS techniques.
Materials and methods
Participants
A total of 188 patients (sex, 94 men and 94 women;
mean age, 54±12 years; age range, 47-68) with suspected
atherosclerosis were admitted to the Peking University
International Hospital (Beijing, China) between April 2014 and May
2016 were recruited into the present study. The inclusion criteria
are as follows: i) Age of individuals >25 years; ii) individuals
exhibited hypertension, coronary heart disease and hyperlipidemia;
and iii) individuals provided informed consent for participation.
The exclusion criteria for all patients were as follows: i)
Patients with history of cancer; ii) patients who underwent
coronary artery surgery; and iii) patients who underwent heart
stent surgery. Following recruitment, all included patients
underwent IVUS followed by Gd2O3-EPL-IVUS 4
weeks later. CT coronary angiography was then performed at
four-week intervals. The Ethical Committee of the Peking University
International Hospital (approval no. LK20131018) approved this
study. Written informed consent was provided by all patients.
Contrast agent
The Gd2O3-coated EPL contrast
agents were synthesized as described previously (28). Briefly, cetyltrimethylammonium
bromide (C16TAB, 0.2 g) was first dissolved in distilled
water (50 ml). NH3.H2O (2 ml 25%) and
tetraethoxysilane (4.49 mmol) were then added and the subsequent
mixture was stirred at room temperature for 10 min.
Gd2O3 (0.5 mmol) was added to this solution
and stirred at 42˚C for 1 h before EPL (0.1 mmol) was added to the
solution and stirred at room temperature for 1 h. Samples were
calcined at 37˚C for 72 h before the
Gd2O3-EPL nanoparticles were harvested. The
purity and chemical structure of Gd2O3-EPL
was determined by mass spectrometry as described previously
(29). This resultant nanoparticle
contrasting agent would be used for visualization for IVUS. All
individuals received intravenously injections of
Gd2O3-EPL contrast agents (0, 0.4, 0.8, 1.2,
1.6, 2.0, 2.4, 2.8, 3.2, 3.6 and 4.0 mg/kg) 2 h prior to IVUS. The
application of Gd2O3-EPL contrast agents was
approved by China Food and Drug Administration.
Biochemical Analysis
Blood samples (10 ml) were collected from each
individual following overnight fasting for 12 h. Serum was obtained
by centrifugation at 8,000 x g for 15 min at 4˚C. Total serum
levels of triglyceride, cholesterol, low-density lipoprotein (LDL)
cholesterol and high-density lipoprotein (HDL) cholesterol were
measured using a TBA2000FR biochemical analyzer (Toshiba
Corporation) as described previously (30). Metabolism of
Gd2O3-EPL was then determined using
inductively coupled plasma mass spectrometry (ICP-MS; Elan DRC II;
PerkinElmer, Inc.) according to a previous study (31).
Intravascular ultrasound virtual
histology examination
IVUS examination was performed as described
previously (32). All patients
received nonionic contrast medium Gd2O3-EPL
(1.2 mg/ml). IVUS was subsequently performed using a 20 MHz
catheter (2.9F monorail, 0.6 mm/s automatic pullback) after
injection using a dedicated IVUS console (Volcano Corporation;
Philips Healthcare) 2 h following intracoronary administration of
10 µg nitroglycerin. The IVUS images were captured at 30 frames/s
using a DVD-Rom for subsequent offline analysis (Volcano
Corporation; Philips Healthcare) and recorded into high-resolution
super VHS videotapes. Signal intensity was determined from digital
imaging and communications in medicine-stored images using a new
Medical Imaging Bench system (version 4.0; Echoplaque-MIB; INDEC
Medical systems, Inc.).
Acquisition of carotid ultrasound
index
The carotid ultrasound index of individuals was
analyzed using a Siemens ACUSON SequoiaTM Ultrasound
system (Volcano Corporation; Philips Healthcare). The probe
frequency was defined at 12 MHz. Ultrasound was performed to
evaluate wall thickness in the carotid artery by an experienced
professional sonographer. The mean intimal-medial thickness (IMT)
was measured and the number of plaques in left anterior descending
(LAD) artery in all individuals was counted. During the ultrasound
measurement, the systolic lumen diameter (Ds), the
diastolic lumen diameter (Dd), the systolic pressure
(Ps), and diastolic pressure (Pd) of the
carotid artery were input. The arterial compliance (AC) was
measured using the following formula:
AC=π(Ds2-Dd2)/[4
(Ps-Pd)] (33). The degree of plaque was graded using
the CHADS2 method on a scale from 0 to 3 (0, no
observable plaque; 1, one small plaque <30% of lumen diameter;
2, one medium plaque 30-50% of vessel diameter; 3, one large plaque
50% of vessel diameter) as described previously (34). Plaque volume was calculated from the
IVUS images as the total volume of the external elastic membrane
occupied by the atheroma. Plaque burden was calculated as plaque
and media cross-sectional area/external elastic membrane
cross-sectional area. Plaque morphology was assessed on IVUS images
of the LAD. Velocity vector imaging (VVI) was performed using the
VVI software (syngo® US workplace; Siemens Healthineers)
to evaluate speed of blood flow and data were analyzed by two
independent pathologists.
CHADS2 scoring
CHADS2 scores were used to predict the
degree of carotid atherosclerosis. The percentage of excess risk as
calculated using the CHADS2 scoring system was
determined according to current guidelines as described previously
(35).
Coronary angiography
CT-coronary angiography was performed using a
dual-source CT scanner (SOMATOM Definition Flash; Siemens AG)
according to standard techniques as described previously (36). All patients received 370 mg I/ml
Ultravist® nonionic contrast medium (Schering AG) using
a dual-head power injector (SCT-210; Medrad, Inc; Bayer AG).
Measurements of vessel geometry, plaque burden and plaque
morphology using coronary angiography images were performed
according to a previous study (37). Coronary angiography images in LAD
were analyzed using a quantitative coronary angiography program
(version 2.0; Medis Medical Imaging Systems) by two independent
investigators.
Statistical analysis
The pilot trial sample size of this study was
determined using the following formula:
N=(µα+µβ)2/12(1-c)(p'-0.5)2
(µ, standard deviation; α, I error probability; β, II error
probability; p, error probability; c, ration of group) (38). Data are presented as mean ± SD and
statistical analyses were performed using SPSS 19.0 software (IBM
Corp.). A receiver operator characteristic (ROC) curve was used to
analyze sensitivity and specificity determined by Youden's index.
The area under the curve (AUC) and the P-values were obtained using
the SPSS software. Relative risk was expressed as HR with 95%
confidence intervals (95% CI) and global χ2-analyzes
utilized logistic regression and likelihood ratios test. Student's
t-test was used to compare two independent groups of data.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Patients
The clinical characteristics of the patients in the
present study are summarized in Table
I. There were no statistically significant differences in the
baseline clinical parameters between male and female patients with
suspected atherosclerosis. All patients exhibited symptoms of
hypertension, coronary heart disease, and hyperlipidemia.
 | Table IBaseline clinical characteristics of
patients with suspected atherosclerosis. |
Table I
Baseline clinical characteristics of
patients with suspected atherosclerosis.
|
Characteristics | Values |
|---|
| Male (n, %) | 94 (50%) |
| Female (n, %) | 94 (50%) |
| Age (years) | |
|
Mean | 54±12 |
|
Range | 47-68 |
| Hypertension (n,
%) | 134 (71.3%)
(>120 mmHg) |
| Body mass index
(kg/m2 ± SD) | 24.30±3.40 (healthy
range, 18.5-24.0) |
| Cholesterol (mmol/l
± SD) | 4.88±0.76 (healthy
range, 3.0-5.2) |
| HDL cholesterol
(mmol/l ± SD) | 1.40±0.28 (healthy
range, 1.0-2.0) |
| LDL cholesterol
(mmol/l ± SD) | 2.85±0.80 (healthy
range, 2.0-3.0) |
| Triglycerides
(mmol/l ± SD) | 1.62±0.84 (healthy
range, 3.5-4.0) |
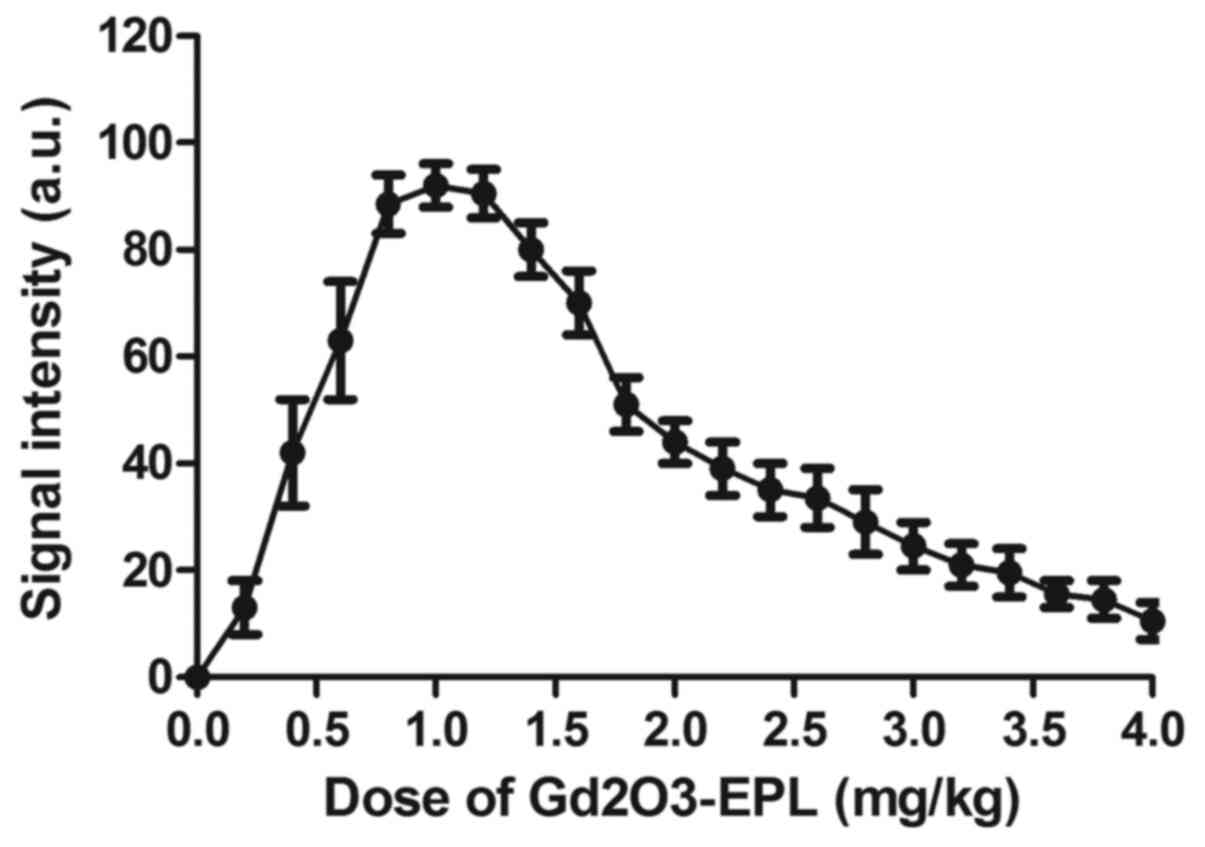
Dose selection and detection time of
Gd2O3-EPL
Results identified 1.2 mg/kg
Gd2O3-EPL to be the optimal dose in
diagnosing carotid atherosclerosis based on signal intensity as
measured using IVUS (Fig. 1). In
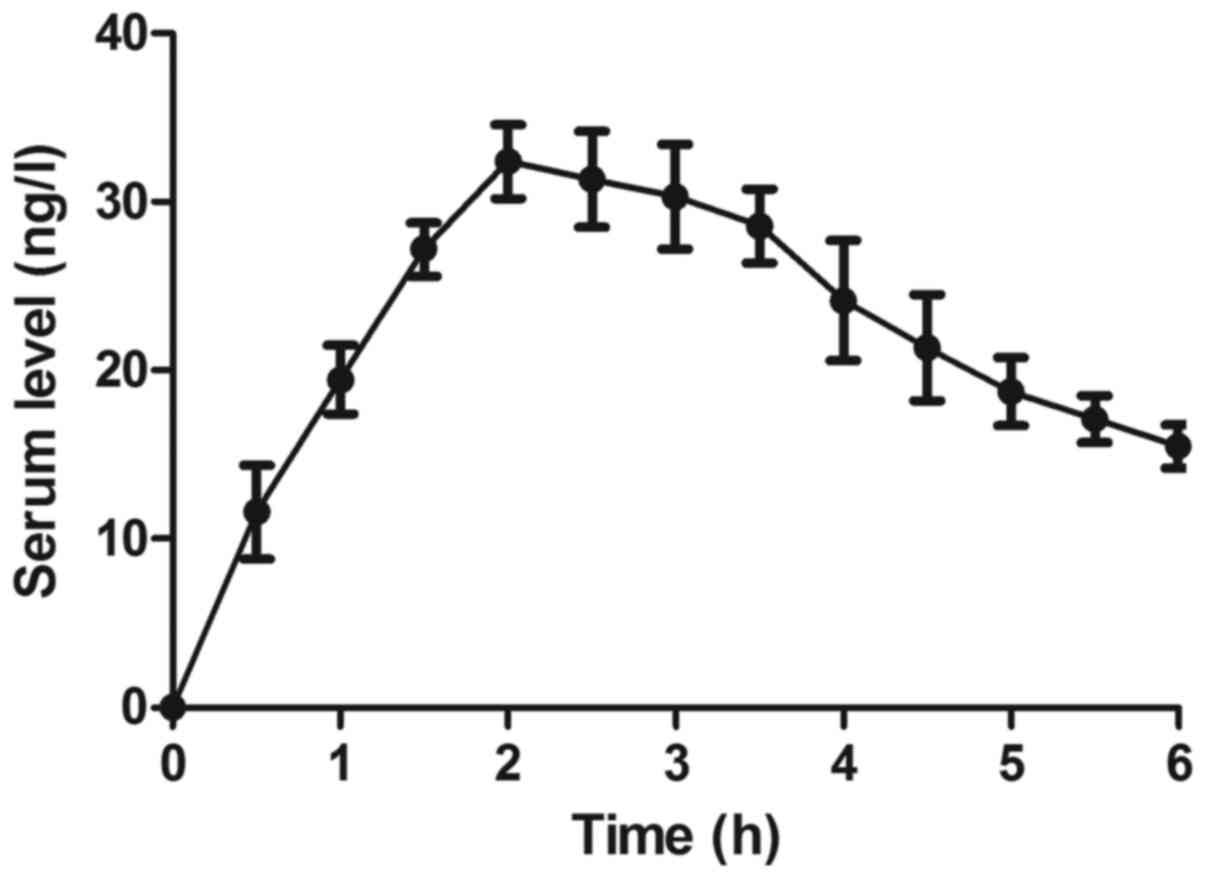
addition, the maximal concentration of
Gd2O3-EPL in the serum was attained 2 h
following injection (Fig. 2).
Therefore, 2 h post-injection was chosen as the timepoint for
performing IVUS imaging on patients with suspected
atherosclerosis.
Diagnostic efficacy of
Gd2O3-EPL-IVUS for patients with suspected
atherosclerosis
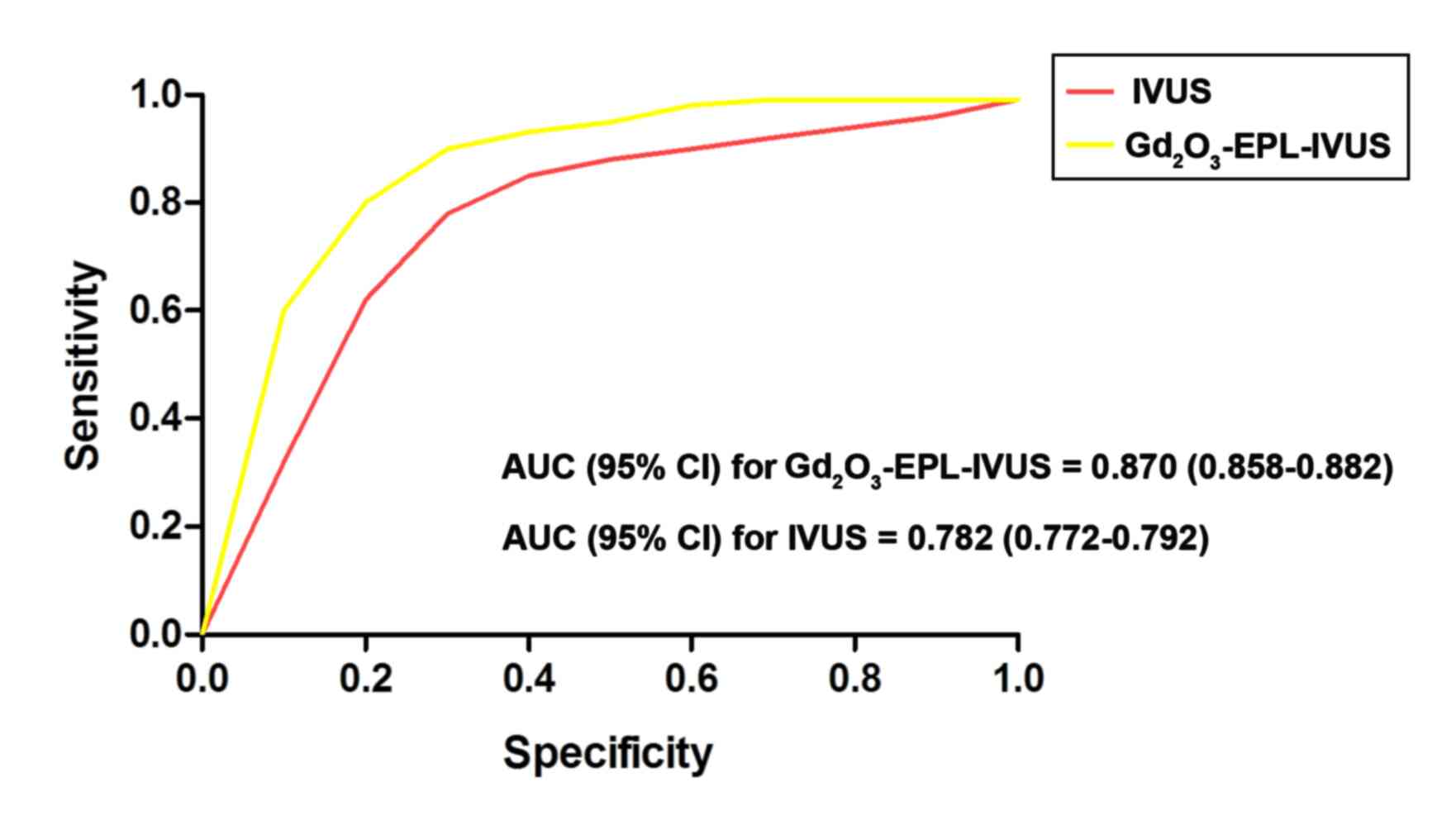
The present study explored the diagnostic efficacy
of Gd2O3-EPL-IVUS in patients with suspected
atherosclerosis. In total, Gd2O3-EPL-IVUS
diagnosed 142 patients out of 188 patients with suspected
atherosclerosis, whilst IVUS diagnosed 124 patients out of 188
patients with suspected atherosclerosis (Table II). ROC analysis also demonstrated
that Gd2O3-EPL-IVUS exhibited higher accuracy
and sensitivity compared with IVUS in diagnosing patients with
suspected atherosclerosis (P<0.05; Fig. 3), since the AUC was 0.870 for the
Gd2O3-EPL-IVUS group (95% CI, 0.858-0.882)
and 0.782 for the IVUS group (95% CI, 0.772-0.792). These data
suggest that Gd2O3-EPL-IVUS can accurately
diagnose atherosclerosis by binding mineralocorticoid receptors in
arterial lesions.
| Table IIDiagnostic efficacy of
Gd2O3-EPL-IVUS for patients with suspected
atherosclerosis. |
Table II
Diagnostic efficacy of
Gd2O3-EPL-IVUS for patients with suspected
atherosclerosis.
| Patient | IVUS (n, %) |
Gd2O3-EPL-IVUS (n,
%) | P-value |
|---|
|
Atherosclerosis | 124 (75.5) | 142 (66.0) | 0.048a |
|
Non-atherosclerosis | 64 (24.5) | 46 (34.0) | 0.035a |
Analysis of carotid ultrasound indices
and VVI indices in patients diagnosed using IVUS and
Gd2O3-EPL-IVUS
Carotid Ultrasound Indices and VVI indices were
subsequently compared between IVUS and
Gd2O3-EPL-IVUS groups. The mean IMT was
calculated to be 0.302±0.045 versus 0.273±0.030 diagnosed by IVUS
and Gd2O3-EPL-IVUS, respectively. There were
significant differences in the CHADS2 scores between
IVUS and Gd2O3-EPL-IVUS group (2.5±1.0 vs.
3.0±1.5, P<0.05). The arterial compliance (AC) index was
2.00±0.82 and 3.50±0.96 in patients diagnosed using IVUS and
Gd2O3-EPL-IVUS, respectively (Table III).
| Table IIIParameters diagnosed using
Gd2O3-EPL-IVUS in patients with suspected
atherosclerosis. |
Table III
Parameters diagnosed using
Gd2O3-EPL-IVUS in patients with suspected
atherosclerosis.
| Parameter | IVUS |
Gd2O3-EPL-IVUS | P-value |
|---|
| IMT (mm) | 0.302±0.045 | 0.273±0.030 | 0.030a |
|
CHADS2 | 2.5±1.0 | 3.0±1.5 | 0.042a |
| AC
(mm2/kPa) | 2.00±0.82 | 3.50±0.96 | 0.016a |
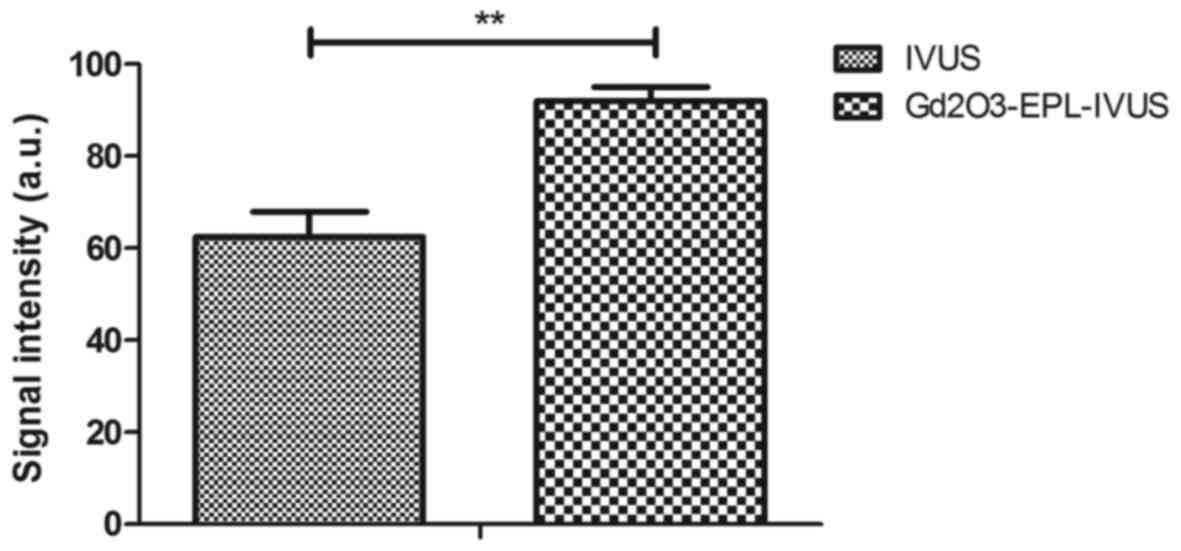
Comparison of atherosclerotic plaque
characteristics using Gd2O3-EPL-IVUS or
IVUS
Multiple plaques were diagnosed on the same patient.
The Gd2O3-EPL-IVUS technique observed
stronger signals associated with the plaque morphology as
determined by measuring signal intensity compared with IVUS in
patients with atherosclerosis (Fig.
4). Gd2O3-EPL-IVUS resulted in clearer
images of arterial plaques compared with IVUS (Fig. 5).
Gd2O3-EPL-IVUS revealed arterial plaque
lesions at higher frequencies compared with IVUS in the same
patients with suspected atherosclerosis (Fig. 6).
Logistic regression to identify risk
factors for atherosclerosis
According to the results of multivariate analysis,
plaque index (OR, 1.062; 95% CI, 0.078-0.096) and CHADS2
score (OR, 0.462; 95% CI, 1.042-1.684) was positively correlated
with atherosclerosis diagnosis (Table
IV). Taking either CHADS2 scores or plaque index
into consideration, Gd2O3-EPL-IVUS was
concluded to be a reliable method in predicting atherosclerotic
lesions.
| Table IVLogistic regression of
Gd2O3-EPL-IVUS to identify risk factors for
atherosclerosis. |
Table IV
Logistic regression of
Gd2O3-EPL-IVUS to identify risk factors for
atherosclerosis.
| Parameter | OR | 95% CI | P-value |
|---|
| Plaque index
(r) | 1.062 | 0.078-0.096 | 0.024a |
| CHADS2
score (r) | 0.462 | 1.042-1.684 | 0.020a |
Confirmation of atherosclerosis in
patients using coronary angiography
The atherosclerosis diagnosis in all patients as
deduced using by Gd2O3-EPL-IVUS and IVUS were
subsequently confirmed using coronary angiography. As shown in
Fig. 7, representative coronary
angiography images showed the presence of pathological
atherosclerotic plaques in patients. Coronary angiography confirmed
four false positive cases in 142/188 patients and three false
negative cases in 46/188 patients following the use of
Gd2O3-EPL-IVUS, whilst eight false positive
cases in 124/188 and 29 false negative cases in 64/188 were
reported as a result of IVUS (Table
V).
| Table VDiagnostic efficacy of
Gd2O3-EPL-IVUS for patients with suspected
atherosclerosis. |
Table V
Diagnostic efficacy of
Gd2O3-EPL-IVUS for patients with suspected
atherosclerosis.
| Type | IVUS (%) |
Gd2O3-EPL-IVUS
(%) | P-value |
|---|
| False positive (n,
%) | 8 (6.5) | 4 (2.8) | 0.034a |
| True positive (n,
%) | 116 (93.5) | 138 (97.2) | 0.049a |
| False negative (n,
%) | 29 (45.3) | 3 (6.5) |
<0.001a |
| True negative (n,
%) | 35 (54.7) | 43 (93.5) |
<0.001a |
Pharmacodynamics of
Gd2O3-EPL in plasma concentration in patients
with atherosclerosis
The serous metabolism of
Gd2O3-EPL was investigated in patients with
atherosclerosis. Gd2O3-EPL was fully
metabolized within 12 h after injection (Fig. 8). No other side effects, including
irritation on the injection site, hypertension and nausea, were
observed in patients with atherosclerosis. These data suggest that
Gd2O3-EPL is a safe contrast agent for use in
IVUS in diagnosing patients with atherosclerosis.
Discussion
Early and accurate diagnosis of atherosclerosis is
crucial for the treatment of this disease (12,39,40).
The present study is the first to examine the diagnostic efficacy
of Gd2O3-EPL combined with IVUS for
atherosclerosis in suspected patients, which provided evidence that
Gd2O3-EPL-IVUS resulted in stronger signals
associated with plaque morphology and generating clearer images of
arterial plaques compared with IVUS alone. In addition,
Gd2O3-EPL-IVUS uncovered higher frequencies
of arterial plaque lesions and diagnosed atherosclerosis in
patients with higher accuracy and sensitivity compared with IVUS
alone.
EPL is one of mineralocorticoid receptor antagonists
where a previous study has found that EPL treatment reduced the
sizes of lesions in early but not advanced atherosclerosis in
Apolipoprotein E-deficient mice (41). EPL strengthened the
endothelium-dependent relaxation and suppressed
angiotensin-converting enzyme activity in the vasculature, which
further prevented the development of atherosclerosis (24). Another study has previously found
that IVUS can produce qualitative and quantitative images with high
accuracies of plaque morphology identification in atherosclerosis
lesions (5). In the present study,
Gd2O3-EPL nanoparticles were introduced and
it was found that the addition of Gd2O3-EPL
enhanced the IVUS signals in evaluating the revascularization
decision of intermediate and ambiguous coronary lesions.
Previously, poor characterization of toxicity in the use of
Gd2O3-SiO2 core-shell
nanoparticles was proving to be an obstacle to the clinical
deployment for its application in diagnosis using MRI in
xenografted murine tumors, due to its the accumulation in tissues
(42). In the present study,
Gd2O3-EPL and IVUS enhanced the diagnostic
efficacy, independent of atherosclerosis severity. Specifically,
data from the pharmacodynamics analysis in the present study
suggest that Gd2O3-EPL may be a safe contrast
agent for IVUS diagnosis due to its metabolism within 12 h after
injection.
IVUS can be to predict and discriminate acute
coronary syndrome culprit lesion phenotypes, which may help to
diagnose active coronary plaques in preventing major adverse
cardiac events in the future (43).
In the present study, it was found that
Gd2O3-EPL-IVUS enabled the accurate
measurements of the vessel size, plaque burden and lumen area by
binding with mineralocorticoid receptors. In addition, the
application of Gd2O3-EPL also reduced the
incidences of false positives and false negatives of IVUS in
diagnosing patients suspected with atherosclerosis.
In conclusion, the findings in the present study
suggest that Gd2O3-EPL-IVUS is a reliable
tool for the evaluation of coronary lesions in patients with
atherosclerosis. In addition, positive associations were found
between the CHADS2 scores and carotid ultrasound
indicators and risk of atherosclerosis using data obtained from
Gd2O3-EPL-IVUS in the present study,
suggesting that images taken using
Gd2O3-EPL-IVUS can reflect the degree of
structural and functional impairment of atherosclerosis.
Consequently, the application of
Gd2O3-EPL-IVUS may contribute to the
assessment of the severity of atherosclerosis and the design of
subsequent treatment strategies.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CYW and DXB made substantial contributions to the
conception and prepared experiments. MYG was responsible for data
acquisition, analysis and interpretation. SLZ designed this study,
was involved in drafting the article and critically revising it for
important intellectual content. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The Ethical Committee of the Peking University
International Hospital (approval no. LK20131018) approved this
study. Written informed consent was provided by all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Yong WC, Sanguankeo A and Upala S:
Association between sarcoidosis, pulse wave velocity, and other
measures of subclinical atherosclerosis: A systematic review and
meta-analysis. Clin Rheumatol. 37:2825–2832. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Zanoli L, Signorelli SS, Inserra G and
Castellino P: Subclinical atherosclerosis in patients with
inflammatory bowel diseases: A systematic review and meta-analysis.
Angiology. 68(463)2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Forgo B, Medda E, Hernyes A, Szalontai L,
Tarnoki DL and Tarnoki AD: Carotid artery atherosclerosis: A review
on heritability and genetics. Twin Res Hum Genet. 21:333–346.
2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Fava C and Montagnana M: Atherosclerosis
is an inflammatory disease which lacks a common anti-inflammatory
therapy: How human genetics can help to this issue. A narrative
review. Front Pharmacol. 9(55)2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Borba DL, Hipolito UV and Pereira YCL:
Early diagnosis of atherosclerosis with panoramic radiographs: A
review. J Vasc Bras. 15:302–307. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Moroni F, Ammirati E, Magnoni M, D'Ascenzo
F, Anselmino M, Anzalone N, Rocca MA, Falini A, Filippi M and
Camici PG: Carotid atherosclerosis, silent ischemic brain damage
and brain atrophy: A systematic review and meta-analysis. Int J
Cardiol. 223:681–687. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Anwaier G, Chen C, Cao Y and Qi R: A
review of molecular imaging of atherosclerosis and the potential
application of dendrimer in imaging of plaque. Int J Nanomedicine.
12:7681–7693. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Chen FH, Liu T, Xu L, Zhang L and Zhou XB:
Association of serum vitamin D level and carotid atherosclerosis: A
systematic review and meta-analysis. J Ultrasound Med.
37:1293–1303. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Mirnejad R, Razeghian-Jahromi I,
Sepehrimanesh M, Zibaeenezhad MJ and Lopez-Jornet P: A proteomics
analysis of the virulence factors of three common bacterial species
involved in periodontitis and consequent possible atherosclerosis:
A narrative review. Curr Protein Pept Sci. 19:1124–1130.
2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Jansen Klomp WW, Brandon Bravo Bruinsma
GJ, van 't Hof AW, Grandjean JG and Nierich AP: Imaging techniques
for diagnosis of thoracic aortic atherosclerosis. Int J Vasc Med.
2016(4726094)2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Koskinas KC, Ughi GJ, Windecker S, Tearney
GJ and Raber L: Intracoronary imaging of coronary atherosclerosis:
Validation for diagnosis, prognosis and treatment. Eur Heart J.
37:524–535a-c. 2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Signorelli SS, Di Pino L, Fichera G,
Celotta G, Pennisi G, Marchese G, Costa MP, Fallico R, Torrisi B
and Virgilio V: Ultrasound diagnosis of carotid artery lesions in a
population of asymptomatic subjects presenting atherosclerosis risk
factors. J Stroke Cerebrovasc Dis. 13:95–98. 2004.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Mougiakakou SG, Golemati S, Gousias I,
Nicolaides AN and Nikita KS: Computer-aided diagnosis of carotid
atherosclerosis based on ultrasound image statistics, laws' texture
and neural networks. Ultrasound Med Biol. 33:26–36. 2007.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Betriu-Bars A and Fernandez-Giraldez E:
Carotid ultrasound for the early diagnosis of atherosclerosis in
chronic kidney disease. Nefrologia. 32:7–11. 2012.PubMed/NCBI View Article : Google Scholar : (In Spanish).
|
|
15
|
Faust O, Acharya UR, Sudarshan VK, Tan RS,
Yeong CH, Molinari F and Ng KH: Computer aided diagnosis of
coronary artery disease, myocardial infarction and carotid
atherosclerosis using ultrasound images: A review. Phys Med.
33:1–15. 2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hibi K, Honda Y, Kimura K and Umemura S:
Atherosclerosis: Progress in diagnosis and treatments. Topics: III.
Progress in diagnosis of atherosclerosis; 5. IVUS (intravascular
ultrasound). Nihon Naika Gakkai Zasshi. 102:344–353.
2013.PubMed/NCBI View Article : Google Scholar : (In Japanese).
|
|
17
|
Chen L, Xu T, Xue XJ, Zhang JJ, Ye F, Tian
NL and Chen SL: Intravascular ultrasound-guided drug-eluting stent
implantation is associated with improved clinical outcomes in
patients with unstable angina and complex coronary artery true
bifurcation lesions. Int J Cardiovasc Imaging. 34:1685–1696.
2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Jiang Y, Zhu J, Hu Y, Xing C, Li D and Hu
B: Can scavenger receptor class B type I loaded ultrasound contrast
agent be a new method for treating atherosclerosis? Med Hypotheses.
73:36–37. 2009.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Jeong H, Huh M, Lee SJ, Koo H, Kwon IC,
Jeong SY and Kim K: Photosensitizer-conjugated human serum albumin
nanoparticles for effective photodynamic therapy. Theranostics.
1:230–239. 2011.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Zhou L, Yang T, Wang J, Wang Q, Lv X, Ke
H, Guo Z, Shen J, Wang Y, Xing C and Chen H: Size-Tunable
Gd2O3@Albumin nanoparticles conjugating
chlorin e6 for magnetic resonance imaging-guided photo-induced
therapy. Theranostics. 7:764–774. 2017.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Wang FH, Bae K, Huang ZW and Xue JM:
Two-photon graphene quantum dot modified
Gd2O3 nanocomposites as a dual-mode MRI
contrast agent and cell labelling agent. Nanoscale. 10:5642–5649.
2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Jung SH, Na K, Lee SA, Cho SH, Seong H and
Shin BC: Gd(III)-DOTA-modified sonosensitive liposomes for
ultrasound-triggered release and MR imaging. Nanoscale Res Lett.
7(462)2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Keidar S, Hayek T, Kaplan M, Pavlotzky E,
Hamoud S, Coleman R and Aviram M: Effect of eplerenone, a selective
aldosterone blocker, on blood pressure, serum and macrophage
oxidative stress, and atherosclerosis in apolipoprotein E-deficient
mice. J Cardiovasc Pharmacol. 41:955–963. 2003.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Greenberg B: Mineralocorticoid receptor
antagonists in heart failure: They work better when patients use
them. Eur J Heart Fail. 20:1335–1337. 2018.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Shiota M, Fujimoto N, Higashijima K, Imada
K, Kashiwagi E, Takeuchi A, Inokuchi J, Tatsugami K, Kajioka S,
Uchiumi T and Eto M: Mineralocorticoid receptor signaling affects
therapeutic effect of enzalutamide. Prostate: May 30, 2018 (Epub
ahead of print).
|
|
26
|
Plieger T, Felten A, Splittgerber H, Duke
E and Reuter M: Corrigendum to ‘The role of genetic variation in
the glucocorticoid receptor (NR3C1) and mineralocorticoid receptor
(NR3C2) in the association between cortisol response and cognition
under acute stress’ [Psychoneuroendocrinology 87 (2018) 173-180].
Psychoneuroendocrinology. 94:169–170. 2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Takai S, Jin D, Muramatsu M, Kirimura K,
Sakonjo H and Miyazaki M: Eplerenone inhibits atherosclerosis in
nonhuman primates. Hypertension. 46:1135–1139. 2005.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Shao Y, Tian X, Hu W, Zhang Y, Liu H, He
H, Shen Y, Xie F and Li L: The properties of Gd2O3-assembled silica
nanocomposite targeted nanoprobes and their application in MRI.
Biomaterials. 33:6438–6446. 2012.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Li X, Hu J, Yin D and Hu X: Solid-phase
extraction coupled with ultra high performance liquid
chromatography and electrospray tandem mass spectrometry for the
highly sensitive determination of five iodinated X-ray contrast
media in environmental water samples. J Sep Sci. 38:1998–2005.
2015.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Zhang GM, Bai SM, Ma XB and Goyal H: A
novel method for estimating low-density lipoprotein (LDL) levels:
Total cholesterol and non-high-density lipoprotein (HDL) can be
used to predict abnormal LDL level in an apparently healthy
population. Med Sci Monit. 24:1688–1692. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Moustakas M, Hanc A, Dobrikova A,
Sperdouli I, Adamakis IS and Apostolova E: Spatial heterogeneity of
cadmium effects on salvia sclarea leaves revealed by chlorophyll
fluorescence imaging analysis and laser ablation inductively
coupled plasma mass spectrometry. Materials (Basel).
12(2953)2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Calvert PA, Obaid DR, O'Sullivan M,
Shapiro LM, McNab D, Densem CG, Schofield PM, Braganza D, Clarke
SC, Ray KK, et al: Association between IVUS findings and adverse
outcomes in patients with coronary artery disease: The VIVA
(VH-IVUS in vulnerable atherosclerosis) study. JACC Cardiovasc
Imaging. 4:894–901. 2011.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Zhang P, Guo R, Li Z, Xiao D, Ma L, Huang
P and Wang C: Effect of smoking on common carotid artery wall
elasticity evaluated by echo tracking technique. Ultrasound Med
Biol. 40:643–649. 2014.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Falcão JL, Falcão BA, Gurudevan SV, Campos
CM, Silva ER, Kalil-Filho R, Rochitte CE, Shiozaki AA, Coelho-Filho
OR and Lemos PA: Comparison between MDCT and Grayscale IVUS in a
quantitative analysis of coronary lumen in segments with or without
atherosclerotic plaques. Arq Bras Cardiol. 104:315–323.
2015.PubMed/NCBI View Article : Google Scholar : (In English,
Portuguese).
|
|
35
|
Lip GY, Nieuwlaat R, Pisters R, Lane DA
and Crijns HJ: Refining clinical risk stratification for predicting
stroke and thromboembolism in atrial fibrillation using a novel
risk factor-based approach: The euro heart survey on atrial
fibrillation. Chest. 137:263–272. 2010.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Xu L and Sun Z: Coronary CT angiography
evaluation of calcified coronary plaques by measurement of left
coronary bifurcation angle. Int J Cardiol. 182:229–231.
2015.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Zhou Y, Tian F, Wang J, Yang JJ, Zhang T,
Jing J and Chen YD: Efficacy study of olmesartan medoxomil on
coronary atherosclerosis progression and epicardial adipose tissue
volume reduction in patients with coronary atherosclerosis detected
by coronary computed tomography angiography: Study protocol for a
randomized controlled trial. Trials. 17(10)2016.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Yin D, Matsumura M, Rundback J, Yoho JA,
Witzenbichler B, Stone GW, Mintz GS and Maehara A: Comparison of
plaque morphology between peripheral and coronary artery disease
(from the CLARITY and ADAPT-DES IVUS substudies). Coron Artery Dis.
28:369–375. 2017.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Adams A, Bojara W and Schunk K: Early
diagnosis and treatment of coronary heart disease in symptomatic
subjects with advanced vascular atherosclerosis of the carotid
artery (type III and IV b findings using ultrasound). Cardiol Res.
8:7–12. 2017.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Fujiyoshi A, Jacobs DR Jr, Alonso A,
Luchsinger JA, Rapp SR and Duprez DA: Validity of death certificate
and hospital discharge ICD codes for dementia diagnosis: The
multi-ethnic study of atherosclerosis. Alzheimer Dis Assoc Disord.
31:168–172. 2017.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Raz-Pasteur A, Gamliel-Lazarovich A,
Coleman R and Keidar S: Eplerenone reduced lesion size in early but
not advanced atherosclerosis in apolipoprotein E-deficient mice. J
Cardiovasc Pharmacol. 60:508–512. 2012.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Tian X, Yang F, Yang C, Peng Y, Chen D,
Zhu J, He F, Li L and Chen X: Toxicity evaluation of Gd2O3@SiO2
nanoparticles prepared by laser ablation in liquid as MRI contrast
agents in vivo. Int J Nanomedicine. 9:4043–4053. 2014.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Murray SW, Stables RH, Garcia-Garcia HM,
Grayson AD, Shaw MA, Perry RA, Serruys PW and Palmer ND:
Construction and validation of a plaque discrimination score from
the anatomical and histological differences in coronary
atherosclerosis: The liverpool IVUS-V-HEART (Intra vascular
ultrasound-virtual-histology evaluation of atherosclerosis
requiring treatment) study. EuroIntervention. 10:815–823.
2014.PubMed/NCBI View Article : Google Scholar
|