Introduction
Acute kidney injury (AKI) refers to a broad spectrum
of clinical conditions ranging from mild injury dysfunction to
severe renal failure and can result in the permanent and complete
loss of renal function (1). The
pooled incidence of AKI in hospitalized patients in Eastern Asia
(mainly including China, Japan and south Korea) is 15% from 2004 to
2012(2) and has been increasing
over the past few decades (3). The
incidence of AKI in critically ill patients worldwide ranges from
20 to 50%, with a mortality rate as high as 50% since 2004
(4,5), where continuous renal replacement
therapy was used in 10-15% critically ill patients with AKI in a
large multicenter study conducted in Finnish intensive care units
and the Acute Kidney Injury-Epidemiologic Prospective Investigation
study (6,7). Cisplatin (CP), a common cause of AKI,
can induce the progression of chronic kidney disease if left
untreated (8). Dose-dependent and
cumulative nephrotoxicity are major side effects of this
chemotherapeutic compound and patients often require a reduction in
dose or discontinuation of treatment (9). A total of ~1/3 patients experience
nephrotoxicity following an initial dose (50-100 mg/m2)
of CP (10). The pathophysiological
features of CP-induced AKI include proximal tubular injury
(including apoptosis, autophagy, DNA damage and mitochondrial
dysfunction), oxidative stress, inflammation and vascular injury in
the kidneys (9).
Previous studies have demonstrated that inflammation
and apoptotic cell death in renal tissues serve an important role
in the progression of AKI (11-15).
High mobility group box 1 (HMGB1) is an alarmin that is released by
activated inflammatory cells, necrotic and apoptotic cells
(16). HMGB1 has been shown to
enhance the progression of acute injury (17,18).
Previous studies have reported that AKI induced by
ischemia-reperfusion (19), CP
(20) or folic acid (21) contribute to the release of HMGB1 in
renal tissues, resulting in the promotion of the inflammatory
response. Administration of exogenous HMGB1 aggravates kidney
injury whereas HMGB1 inhibition significantly attenuates tubular
injury and renal dysfunction (19).
Furthermore, HMGB1 expression was previously found to be increased
in a sepsis AKI mouse model with 5/6 nephrectomy where serum HMGB1
levels are positively associated with the severity of sepsis
(22). These studies supported the
notion that HMGB1 is a mediator of inflammation in AKI that can be
used as an intervention target for AKI treatment.
Activation of the mitochondria-dependent apoptotic
pathway also serves an important role in CP-induced nephrotoxicity,
as evidenced by the upregulation of the pro-apoptotic protein Bax
in renal tubular cells in a CP-treated mouse model (23). CP-induced renal damage was found to
be attenuated in Bax-knockout mice (23). In addition, Bcl-2, an anti-apoptotic
protein, inhibits CP-induced Bax translocation, which suppresses
apoptosis in T24R2 human bladder cancer cells (24). The protein ratio of Bax/Bcl-2 is
associated with cell survival and apoptotic cell death in
CP-treated proximal tubule cells (25).
Over the past decade, mesenchymal stem cells (MSCs)
derived from bone marrow, umbilical cords and adipose tissues have
been reported to be some of the most promising tools for treating
AKI in various animal models, including CP-induced nephrotoxicity
models (26-28).
Compared with MSCs from other tissues, human umbilical cord-derived
MSCs (hUCMSCs) can be separated from discarded umbilical cords,
which are routinely harvested with no risk to donors and are rarely
contaminated by infectious agents, including cytomegalovirus
(29). Human cord blood mononuclear
cells (hCBMNCs) are mononuclear cells (MNCs) derived from cord
blood which exhibit similar advantages to hUCMSCs (30). hCBMNCs are composed of lymphocytes,
hematopoietic stem cells, endothelial progenitor cells, monocytes
and MSCs, which provides these cells with high regenerative and
differentiation potentials (31).
While the protective effects of hUCMSCs against
CP-induced AKI have been demonstrated, the role of hCBMNCs in renal
diseases, particularly AKI, remain unknown. It is unclear whether
hCBMNCs transplantation therapies exhibit similar protective
effects and mechanisms of action. The present study aimed to
investigate the protective effects of the transplantation of
hUCMSCs and hCBMNCs on a CP-induced AKI rat model and elucidate the
underlying molecular mechanisms of action. The results may provide
experimental evidence for the future application of hUCMSCs and
hCBMNCs for the treatment of patients with AKI.
Materials and methods
Sample collection
Umbilical cord and umbilical cord blood were
collected from a 23-year-old woman in the Third Hospital of
Guangdong Pharmaceutical University (Guangzhou, China) by Guangzhou
Cedicine Biotechnology Co., Ltd. on March 12th, 2016. Umbilical
cord blood was used to prepare hCBMNCs by Guangzhou Cedicine
Biotechnology Co., Ltd. whilst umbilical cord was sent to Professor
Jie Liu (China-US Research Center for Stem Cell, Shanghai, China)
to prepare hUCMSCs. The project was carried out under the
cooperation between the Second Xiangya Hospital and Guangzhou
Cedicine Biotechnology Co., Ltd. Our study obtained the approval
from the Medical Ethics Committee of the Second Xiangya Hospital of
Central South University (Changsha, China) and written informed
consent from the donor. Only one donor was recruited in our study.
The present study was registered with the Chinese Clinical Trial
Registry (November 1st, 2018; registration no.
ChiCTR1800019254).
Preparation of hUCMSCs
Isolation and preparation of hUCMSCs were performed
within 24 h, as previously described (32). Briefly, hUCMSCs were identified
according to expressed antigens CD90, CD73 and CD105(33) using flow cytometry with the flow
cytometer BD FACSCanto™ II (BD Biosciences). Fluorescently-labelled
primary antibodies against CD90 [allophycocyanin (APC); cat. no.
17-0909-42; 5 µl/ml], CD73 [phycoerythrin (PE); cat. no.
12-0739-42; 5 µl/ml), CD105 (PE; cat. no. 12-1057-42; 5 µl/ml),
CD45 (FITC; cat. no. 11-0459-42; 5 µl/ml), CD34 (eFluor®
450; cat. no. 48-0349-42; 5 µl/ml), CD133 (PE; cat. no. 12-1338-42;
5 µl/ml), provided by Thermo Fishier Scientific. Inc., were used
for flow cytometry. The cells were blocked in 1% bovine serum
albumin (BSA; Affinity BioReagents, Thermo Fisher Scientific, Inc.)
for 30 min at room temperature in the dark, washed with PBS twice
and then incubated with the primary antibodies for 30 min at room
temperature at a cell density of 3x107/ml prior to
analysis. The data were analyzed using BD CellQuest™ software
(version 5.1; BD Biosciences). The adipogenic, osteogenic and
chondrogenic differentiation potentials were determined by using a
Human Mesenchymal Stem Cell Functional Identification kit (R&D
Systems, Inc.) according to the manufacturer's protocol. The
adhesive capacity of the hUCMSCs was observed under a fluorescence
microscope (magnification, x40; Leica M205 FA; Leica Microsystems
GmbH).
Preparation of hCBMNCs
Umbilical cord blood was collected in 250 ml
standard blood collection bags (Baxter International, Inc.)
containing citrate-phosphate-dextrose anticoagulant, as previously
described (34). Briefly, samples
were tested for pathogens of communicable diseases, including
hepatitis B and C, human immunodeficiency virus, cytomegalovirus
and Treponema pallidum within 24 h of collection. MNCs were
isolated from the umbilical cord blood using Ficoll-Paque TM PLUS
medium (Amersham Biosciences). Flow cytometry was used to examine
the expressed antigens of hCBMNCs using a flow cytometer (BD
FACSCanto™ II; BD Biosciences). Fluorescently-labelled primary
antibodies against CD38 (PE-Cyanine7; cat. no. 25-0389-42; 5
µl/ml), CD5 (PE; cat. no. 12-0059-42; 5 µl/ml), CD3
(APC-eFluor® 780; cat. no. 47-0038-42; 5 µl/ml), CD34
(eFluor® 450; cat. no. 48-0349-42; 5 µl/ml), CD133 (PE;
cat. no. 12-1338-42; 5 µl/ml) provided by Thermo Fishier
Scientific. Inc., were used for flow cytometry. The cells were
blocked in 1% bovine serum albumin (BSA; Affinity BioReagents,
Thermo Fisher Scientific, Inc.) for 30 min at room temperature in
the dark, washed with PBS twice and then incubated with primary
antibodies for 30 min at room temperature at a cell density of
3x107/ml prior to the analysis. The data were analyzed
using BD CellQuest™ software (version 5.1; BD Biosciences). hCBMNCs
were then collected and washed twice with DMEM, diluted to a cell
density of 3x107 MNCs/ml and cryopreserved in sterile 2
ml cryovials with 10% DMSO. Prior to cell transplantation, cell
viability was evaluated using trypan blue assays before and then
diluted with PBS (concentration, 2x106 MNCs/ml)
(35).
Study design
Male Sprague-Dawley rats (age, ~8 weeks; weight,
250±10 g) were obtained from Laboratory Animal Center of Southern
Medical University (Guangzhou, China). All rats in experiments were
provided free access to water and normal rat chow and were
acclimatized for 7 days at 24˚C, 60±10% humidity and 12-h
light/dark cycles before each animal experiment. To determine the
effects of hUCMSCs and hCBMNCs on CP-induced AKI rats, 24 rats with
similar body weights after 7 days of acclimatization (310±10 g)
were selected and randomly assigned into 4 groups (n=6/group) as
follows: i) normal control (CN); ii) model (CP); iii) hCBMNCs (CP +
hCBMNCs); and iv) hUCMSCs (CP + hUCMSCs). AKI models were
established by subcutaneous injections of the nephrotoxic drug CP
(Qilu Pharmaceutical Co., Ltd.) at a dose of 8 mg/kg. hUCMSCs
(2.0x106 cells) and hCBMNCs (2.0x106 cells)
were injected into the femoral vein of rats 24 h following CP
treatment. On day 5 following CP injection, all rats were
intraperitoneally injected with 2% pentobarbital sodium (45 mg/kg)
for anesthesia. Following the collection of 2 ml blood from the
auricula dextra, rats were sacrificed by exsanguination. All
animal-related operations were conducted under the approval of the
Animal Care and Use Committee of the Second Xiangya Hospital,
Central South University, Changsha, China (approval no. SYXK(Xiang)
2017-0002).
Measurement of blood urea nitrogen
(BUN) and creatinine
Blood samples were collected for BUN and serum
creatinine (SCr) measurements on days 0, 3 and 5 following CP
injection. On days 0 and 3, 1 ml blood was collected from the
orbital venous plexus after inhalation anesthesia with 5%
isoflurane. Blood collection was performed within 2 min. Rats were
then put back to their cages to keep raising after compression
hemostasis and provided free access to water and normal rat chow.
On day 5, 2 ml blood was collected from the auricula dextra after
anesthesia with an intraperitoneal injection of 2% pentobarbital
sodium (45 mg/kg) for anesthesia, where the blood collection was
done within 10 min. Rats were sacrificed by exsanguination after
blood collection. Death was confirmed by the absence of heartbeat.
BUN and SCr levels were determined using an automatic biochemical
analyzer (Shimadzu Corporation; CL-8000) at the Chinese Academy of
Sciences Guangzhou Institute of Biomedicine and Health Laboratory
Animal Center.
Renal histological evaluation
Right kidneys were fixed with 10% buffered formalin
for 24 h at room temperature and embedded in paraffin.
Subsequently, kidney samples were cut into 3 µm thick sections and
stained with hematoxylin and eosin at room temperature for 15 and 3
min, respectively. Histological changes were observed and
semi-quantitative scoring was performed. A minimum of 10 fields
were assessed and graded per biopsy using a light microscope
(magnification, x200; BX51TF; Olympus Corporation). For tubular
injury assessment, the following scale was used: i) 0, no tubular
injury; ii) 1, <25% of tubules injured; iii) 2, 25-50% of
tubules injured; iv) 3, 51-75% of tubules injured; and v) 4, ≥76%
of tubules injured (36).
Apoptosis analysis of renal tubular
epithelial cells
Renal samples were fixed in 10% buffered formalin as
aforementioned. Apoptotic cells in renal tissue were quantified by
terminal deoxynucleotidyl transferase dUTP nick end labeling
(TUNEL) assays using an in situ cell detection kit
(TdT-FragEL™ DNA fragmentation detection kit; Merck KGaA) according
to the manufacturer's protocol. At room temperature, renal sections
were labeled with biotin-dUTP for 60 min and combined with
streptavidin-horseradish peroxidase for 10 min. They were then
labeled with 3,3' diaminobenzidine (Dako; Agilent Technologies,
Inc.) for 10 min, counterstained with methyl green (Vector
Laboratories, Inc.; Maravai LifeSciences) for 1 min at room
temperature and mounted with glycerinum (Beyotime Institute of
Biotechnology). To compare the abundance of TUNEL-positive renal
tubular cells among groups, 10 different fields from each group
were chosen and 1x102 renal tubular epithelial cells in
each group were examined by a light microscope (magnification,
x200; BX51TF; Olympus Corporation). Tubular apoptosis was evaluated
by counting TUNEL-positive cells. The obtained results are
presented as TUNEL positive cells per 1x102 renal
tubular cells.
Expression of high mobility group box
1 (HMGB1) and Bax/Bcl2 in renal tissues
Protein expression levels of HMGB1 in renal tissues
were detected using Rat HMGB-1 ELISA Kit (cat. no. E-EL-R0505c;
Elabscience, Inc.) and western blotting (Affinity BioReagents;
Thermo Fisher Scientific, Inc.). Protein expression levels of Bax
and Bcl-2 in renal tissues were examined by western blotting.
Briefly, 100 mg samples of subpolar tissues from
right kidneys were treated with a mixture of ice-cold RIPA lysis
buffer and PMSF (100:1; Beyotime Institute of Biotechnology) for 60
min and centrifugated at 10,000 x g for 20 min at 4˚C. Supernatants
were collected and stored at -70˚C. Protein concentrations were
determined using a bicinchoninic acid Protein Assay Reagent kit
(Beyotime Institute of Biotechnology). Following this, protein
samples (50 µg protein/lane) were loaded, separated by 12% SDS-PAGE
and transferred to nitrocellulose filter membranes. Membranes were
blocked by incubation with TBS-T (TBS with 0.05% Tween-20, pH 7.4)
and 5% BSA (Affinity BioReagents, Thermo Fisher Scientific, Inc.)
at room temperature for 1 h. Following this, membranes were
incubated with HMGB1 (cat. no. PA5-27378), Bax (cat. no. PA5-39778)
and Bcl-2 (cat. no. PA5-27094) primary antibodies (polyclonal;
rabbit anti-rat; 1:1,000, Affinity BioReagents; Thermo Fisher
Scientific, Inc.) and anti-β-actin antibodies (polyclonal; rabbit
anti-rat; 1:2,000; Santa Cruz Biotechnology, Inc.) at 4˚C overnight
with shaking. Membranes were rinsed with TBST 4 times and incubated
with horseradish peroxidase-conjugated secondary antibodies
(1:5,000; cat. no. ab98364; Abcam). Finally, protein bands were
detected using ECL western blotting detection reagent (EMD
Millipore) and quantified using Tanon 5200 Multi Image Analysis
software 1.0 (Tanon Science & Technology Co., Ltd.).
Statistical analysis
SPSS Statistics software (version 20.0; IBM Corp.)
was used for statistical analyses. Data are presented as mean ±
standard deviation. Data were analyzed using one-way ANOVA and
two-group comparisons among multiple samples was analyzed using
Tukey's multiple comparison test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Phenotypic characterization and flow
cytometric analysis of isolated hUCMSCs and hCBMNCs
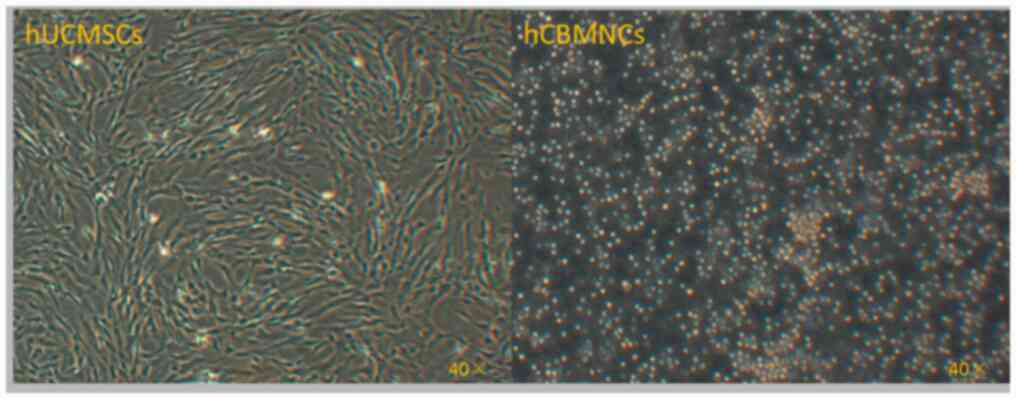
hUCMSCs were spindle shaped and arranged in a radial
pattern following passage, hCBMNCs did not adhere and exhibited a
single or multiple cell aggregate suspension state (Fig. 1). Flow cytometric analysis revealed
that hUCMSCs were positive for CD90, CD73 and CD105 and negative
for CD45, CD34 and CD133. The percentage of CD90, CD73 and CD105
positive cells were 83.00, 82.25 and 80.11%, respectively, whilst
CD45, CD34 and CD133 were only expressed in 4.08, 1.31 and 0.70% of
hUCMSCs, respectively (data not shown). A clonal hUCMSCs population
was chosen for following experiments and used at passage 4. hCBMNCs
mainly expressed CD38, CD5 and CD3 with the positive rates being
39.32, 38.50 and 41.10%, respectively; whilst 2.11% hCBMNCs
expressed CD34 and 2.31% expressed CD133 (data not shown).
Changes in BUN and SCr levels
Compared with the CN group, BUN and SCr levels in
the CP group were significantly raised on day 3 and 5 following CP
injection (P<0.01). The levels of BUN (P<0.05, hUCMSCs vs.
CP; P<0.01, hCBMNCs vs. CP group) and SCr (P<0.01) in the
hUCMSCs and hCBMNCs groups were significantly decreased compared
with those in the CP group on day 5. There were no significant
differences in BUN and SCr levels between the hUCMSCs and hCBMNCs
group (Table I).
 | Table IChanges in the levels of BUN and SCr
in each group. |
Table I
Changes in the levels of BUN and SCr
in each group.
| A, BUN |
|---|
| | Group | | |
|---|
| Day | CN | CP | hCBMNCs | hUCMSCs |
|---|
| 0 | 7.15±1.24 | 6.41±1.08 | 5.13±1.51 | 6.92±1.73 |
| 3 | 6.09±1.31 |
31.14±7.75a |
19.98±7.56a,b |
20.16±10.99a,b |
| 5 | 5.28±1.83 |
56.97±15.55a |
29.39±18.10a,c |
41.02±13.27a,b |
| B, SCr |
| | Group | | |
| Day | CN | CP | hCBMNCs | hUCMSCs |
| 0 | 20.82±3.22 | 21.35±1.59 | 18.95±3.99 | 20.83±2.97 |
| 3 | 19.15±4.78 |
122.52±41.6a |
65.52±21.18a,c |
68.73±21.52a,c |
| 5 | 19.50±8.39 |
206.87±57.7a |
140.25±38.2a,c |
148.38±30.77a,c |
Renal histopathology
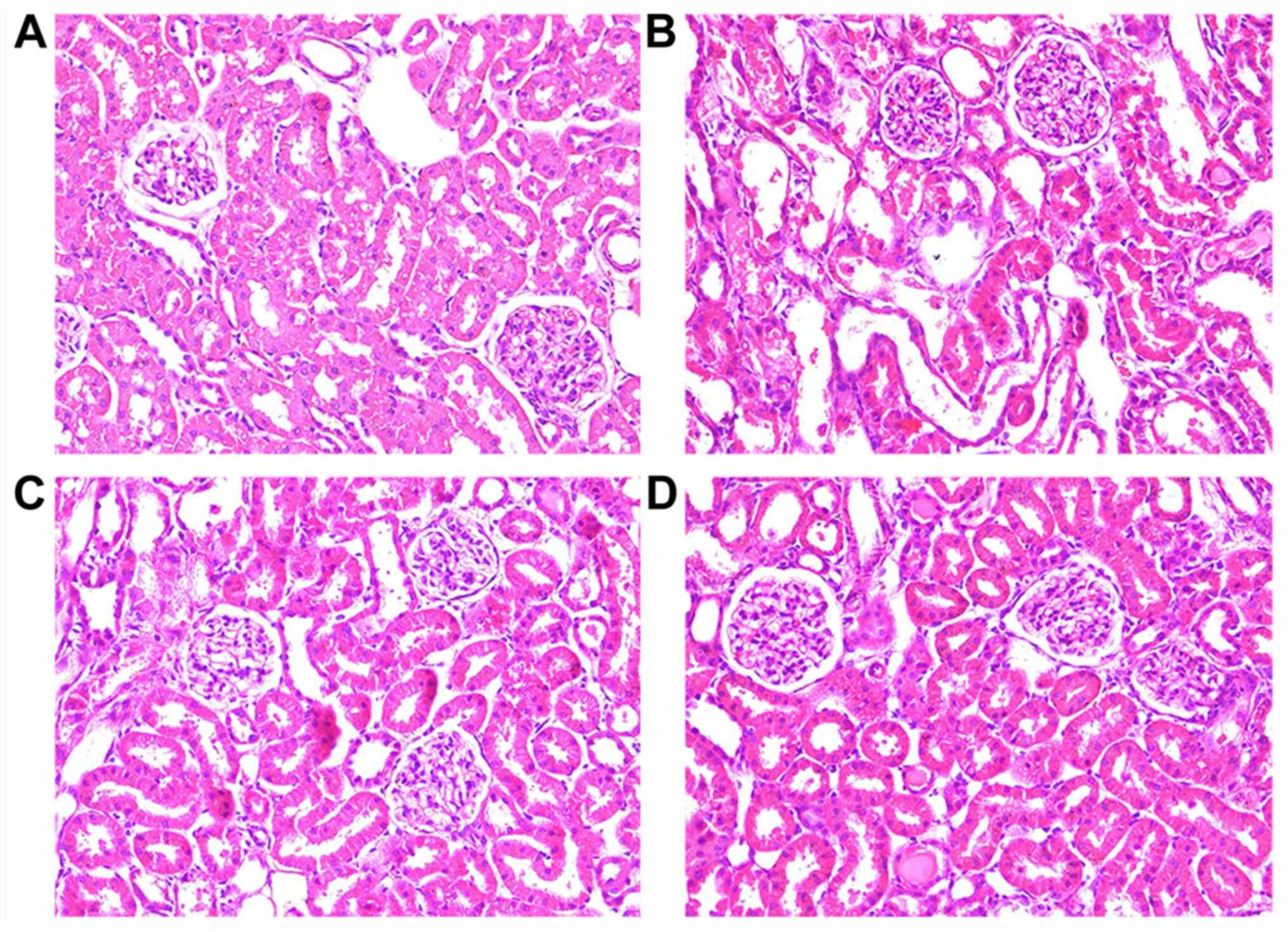
The morphology of renal tubules was normal in normal
control group (Fig. 2A). No tubular
dilation, cast formation or vacuolar degeneration of tubular
epithelial cells were observed. However, vacuolar degeneration,
tubular dilation, cast formation and loss of the tubular brush
border were observed in CP-injected rats (Fig. 2B). Rats treated with hCBMNCs
(Fig. 2C) or hUCMSCs (Fig. 2D) exhibited a mild loss of the
tubular brush border and cast formation in focal tubular epithelial
cells. Semi-quantitative analysis of the tubular injury score in
renal tissues revealed that renal tubular damage was significantly
aggravated in the model, hUCMSCs and hCBMNCs groups compared with
that in the normal control group (P<0.01; Table II). Tubular injury score was found
to be significantly attenuated in rats injected with hUCMSCs or
hCBMNCs compared with the CP group (P<0.05; Table II). There were no significant
difference in the severity of renal tubular damage between the
hUCMSCs and hCBMNCs groups (P>0.05).
| Table IISemi-quantitative analysis of renal
tubular damage in each group. |
Table II
Semi-quantitative analysis of renal
tubular damage in each group.
| Group | Tubular injury
score | Apoptosis of renal
tubular epithelial cells, % |
|---|
| CN | 0.1±0.316 | 1.3±0.949 |
| CP |
2.5±0.527a |
12.5±1.08a |
| hCBMNCs |
1.7±0.675a,b |
6.1±1.524a,c |
| hUCMSCs |
1.6±0.699a,b |
6.6±0.843a,c |
Apoptosis of renal tubular epithelial
cells
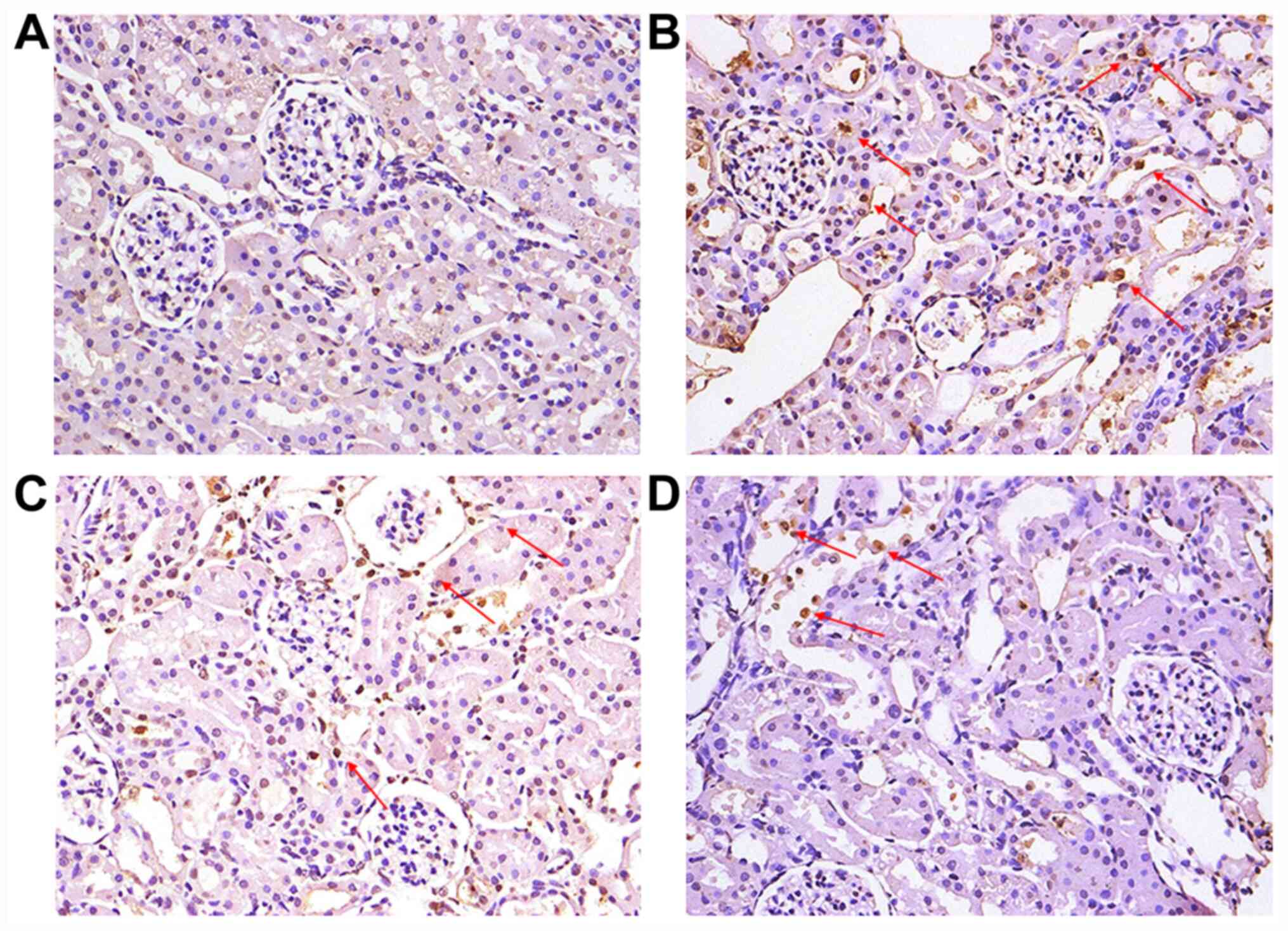
TUNEL staining was performed to detect apoptosis of
renal tubular epithelial cells. Cells with brownish yellow granules
in the nucleus were considered to be apoptotic renal tubular
epithelial cells. Apoptotic renal tubular epithelial cells were not
observed in the normal control group (Fig. 3A) but could be seen in hUCMSCs or
hCBMNCs group (Fig. 3C and D), and were widely distributed in the
renal tubules of the model group (Fig.
3B). Semi-quantitative analysis showed that the percentage of
apoptotic renal tubular cells in the hUCMSCs and hCBMNCs groups
were significantly increased compared with the normal control group
(P<0.01; Fig. 3 and Table II) and significantly decreased
compared with model group (P<0.01).
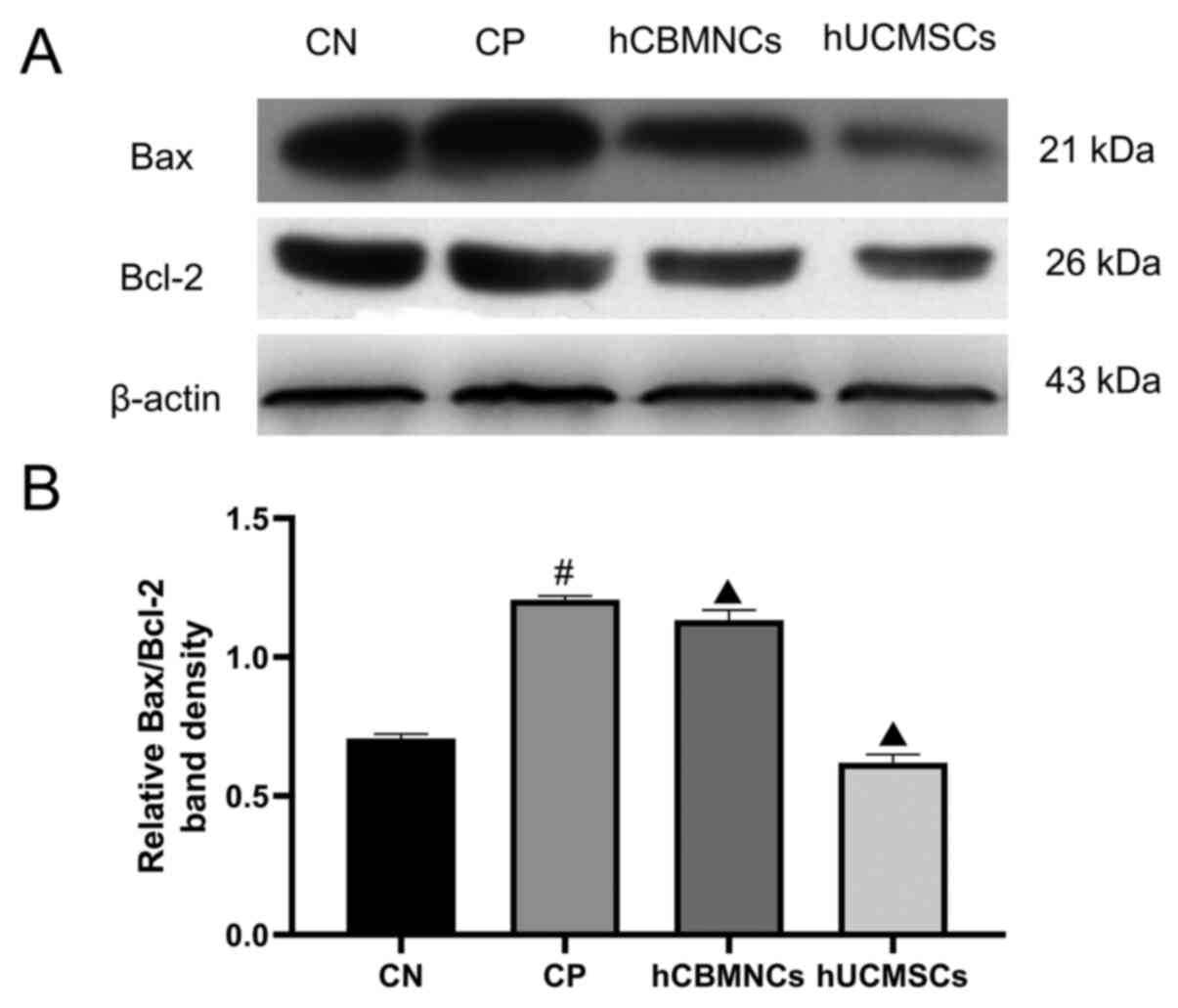
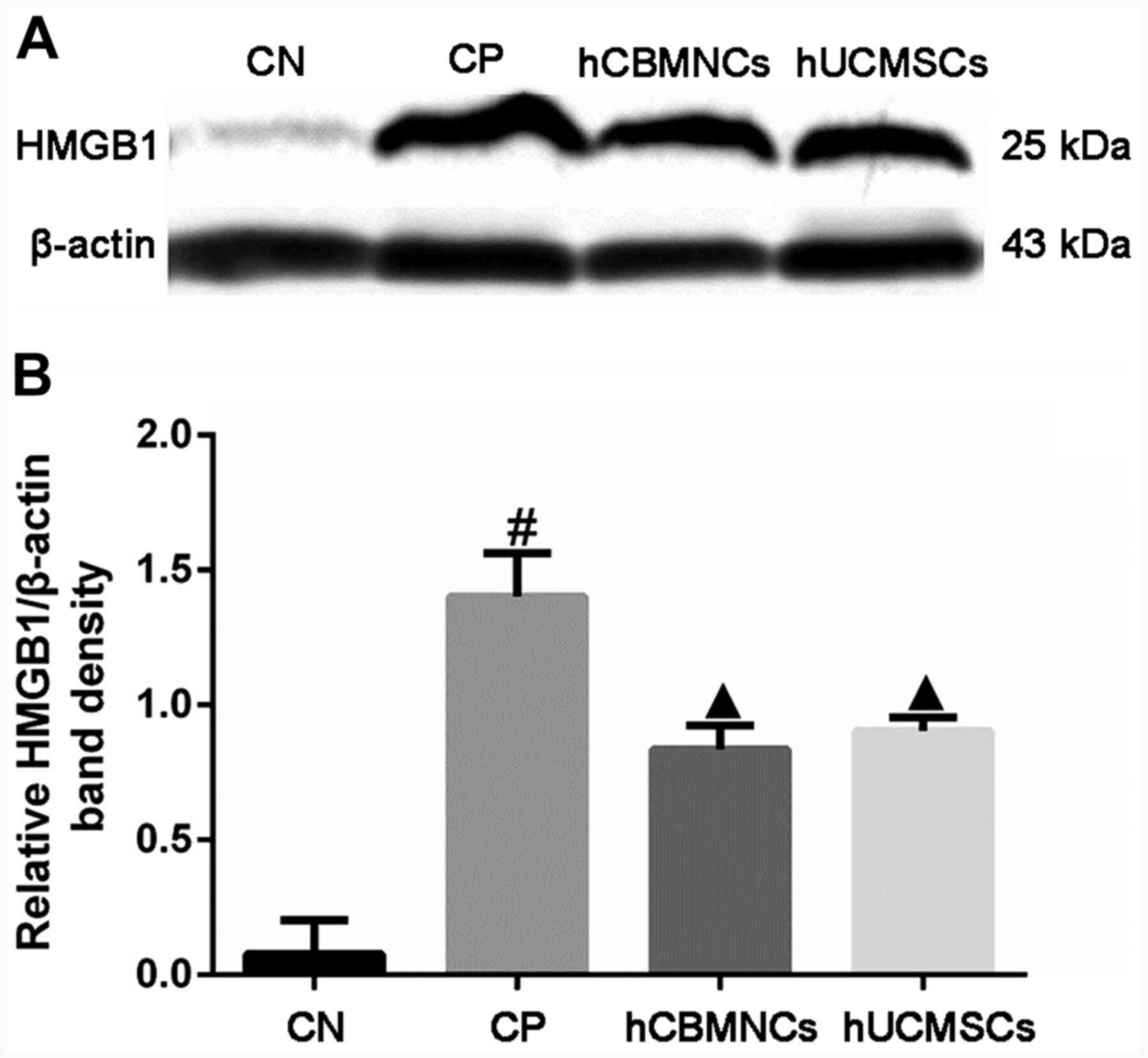
Protein expression of HMGB1, Bcl-2 and
Bax, in renal tissues
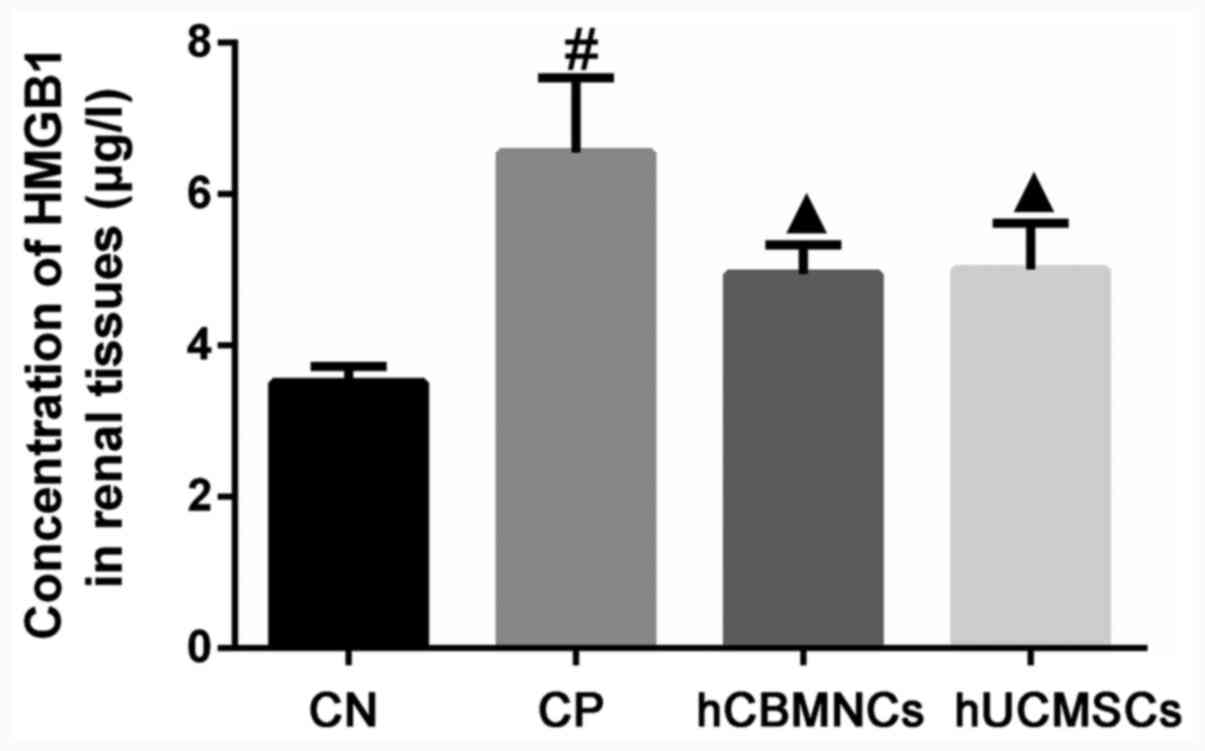
CP administration significantly increased the
expression levels of HMGB1 in renal tissues in the CP group
compared with CN group (Fig. 4;
P<0.01). Furthermore, treatment with hCBMNCs and hUCMSCs
significantly downregulated HMGB1 in renal tissues compared with
the CP group (P<0.01). Western blotting results demonstrated
that the ratio of Bax/Bcl-2 and the expression of HMGB1 were
significantly higher in the CP group compared with the CN group
(P<0.01; Figs. 5 and 6). Additionally, in both the hUCMSCs group
or hCBMNCs group, the expression of HMGB1 and ratio of Bax/Bcl-2
were significantly lower in the hUCMSCs and hCBMNCs groups compared
with the CP group (P<0.01).
Discussion
The results of the present study demonstrated that
hUCMSCs and hCBMNCs exhibited similar protective effects in
CP-induced AKI rats. These protective effects may be associated
with HMGB1 downregulation and a decreased Bax/Bcl-2 ratio.
Due to the widespread use of CP and other platinum
derivatives as chemotherapeutic agents to treat solid tumors,
CP-induced AKI has become a common side effect and accounts for
8-60% of hospital-acquired cases of AKI (37). CP-induced AKI is characterized by
renal tubular epithelial cell injury, renal dysfunction and high
mortality with no effective prevention measures (9). Clinically, CP-induced nephrotoxicity
is mainly prevented by hydration therapy, proper administration
times and dose restriction (38).
However, the occurrence of CP-induced kidney injury remains high
(39). Therefore, the development
of novel and effective strategies for CP-induced AKI are urgently
needed.
MSCs are a group of undifferentiated pluripotent
cells in higher organisms that have been widely employed in the
research of human diseases (40-43).
Previous studies have demonstrated that MSCs significantly improve
the survival rate and renal function in CP-induced AKI animal
models with normal or compromised immune systems (44,45).
Another previous study has reported that early, rather than late,
treatment with hUCMSCs attenuates CP-induced nephrotoxicity through
immunomodulation (46). Jiao et
al (28) revealed that bone
marrow MSC-derived conditioned medium prevented CP-induced AKI
through the activation of the Wnt/β-catenin pathway. However, few
studies have compared the effects of hUCMSCs and hCBMNCs on
CP-induced AKI. The present study evaluated the therapeutic
potentials of hUCMSCs and hCBMNCs in CP-induced AKI in rat models.
The results demonstrated that hUCMSCs and hCBMNCs significantly
improved renal function, as evidenced by improved renal morphology;
decreased concentrations of BUN and SCr; and a reduced percentage
of apoptotic renal tubular cells. This indicated that hUCMSCs and
hCBMNCs had protective effects on CP-induced AKI rats. Following
this, the possible mechanisms underlying the renoprotective effects
of hUCMSCs and hCBMNCs on CP-induced AKI were further investigated
in the present study.
The present study demonstrated that renal HMGB1
protein expression was significantly upregulated in rats with
CP-induced renal toxicity. However, in rats administrated with
hUCMSCs or hCBMNCs, HMGB1 expression levels decreased significantly
compared with the CP group, indicating that hUCMSCs or hCBMNCs may
protect against CP-induced AKI in rat models by suppressing the
release of HMGB1. CP also significantly increased the number of
TUNEL-positive cells and the Bax/Bcl-2 ratio. Additionally, the
results demonstrated that the number of TUNEL-positive cells and
the ratio of Bax/Bcl-2 decreased in rats treated with hUCMSCs or
hCBMNCs. These results suggested alleviated kidney tissue injury
and improved renal function. The present study confirmed the role
of Bax/Bcl-2 in CP-induced AKI demonstrated in previous studies
(24,25,47),
where the level of Bax was shown to be upregulated during CP
treatment accompanied with the release of mitochondrial cytochrome
c and cell apoptosis. This indicates the involvement of the
intrinsic pathway of apoptosis in CP-induced nephrotoxicity
(25,47), Bcl-2 downregulation by RNA
interference potentiates the redistribution of Bax and cytochrome
c and promotes apoptosis (24). The present study further indicated
that hUCMSCs and hCBMNCs attenuated CP-induced nephrotoxicity by
inhibiting apoptosis in renal tubular cells and reducing the
Bax/Bcl-2 ratio.
However, it is unknown whether this protective
effect is due to the local action or a systemic effect of the MSCs.
It has been reported that stem cells exert therapeutic effects via
two distinct mechanisms: i) differentiation into target tissue
cells; and ii) secretion of regulatory factors (48). Previous studies have demonstrated
that stem cell-mediated protection is a result of their ability to
engraft into a damaged kidney (44,49)
and PKH-26-labeled hUCMSCs have been detected in CP-injured kidneys
(46). By contrast, other studies
have reported that the beneficial effect of stem cells is mediated
through paracrine activities, in which MSCs produce various
cytokines and growth factors, including VEGF (50,51).
Furthermore, the administration of secreted microvesicles from stem
cells loaded with mRNA and microRNA alleviates renal tubular injury
and improves renal function in models of AKI (52,53).
Due to the inconsistencies in the reported mechanisms of action
behind the renoprotective effects of stem cells by previous
studies, it is crucial to further investigate whether the
renoprotective effect of stem cells are associated with local or
systemic effects, or a combination of both.
The present study had certain limitations. Firstly,
there was a lack of in vitro and clinical experiments to
support the animal experiments. Secondly, the distribution of stem
cells in the renal tissues of AKI models were not observed.
Thirdly, the possible role of HMGB1 in the renoprotective
mechanisms of action of hUCMSCs and hCBMNCs requires further
verification by gene silencing or knockout experiments. Therefore,
future work should focus on elucidating the renoprotective
mechanisms of action of hUCMSCs and hCBMNCs, as well as the
functional role of HMGB1 and relevant signaling pathways, which
could confirm the results of the current study.
In conclusion, the present study demonstrated that
hUCMSCs and hCBMNCs exert similar renoprotective effects on
CP-induced AKI rat models. The renoprotective mechanisms of action
may be associated with HMGB1 downregulation, anti-apoptosis in
renal tubular cells and a decrease in the Bax/Bcl-2 ratio.
Transplantation of hUCMSCs and hCBMNCs may be a potential novel
therapy for patients with AKI.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Clinical
Medical Technology Innovation Guide Project of Hunan Province
(grant no. 2017SK50117), the National Natural Science Foundation of
China (grant no. 81570618), the Development and Reform Commission
of Hunan Province (grant no. 2014-658) and the Scientific
Foundation of Hunan Province (grant no. S2013F1022).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
SBD designed the present study and revised the
manuscript critically for important intellectual content. QX, PY
and XJD acquired, analyzed and interpreted the data, and drafted
the manuscript. XW, XJC, ML, JCP, LXF and WC analyzed and
interpreted the data, and revised the manuscript critically for
important intellectual content. JL provided the hUCMSCs, analyzed
and interpreted the data, and revised the manuscript critically for
important intellectual content. HLZ and QYZ provided the hCBMNCs,
analyzed and interpreted the data, and revised the manuscript
critically for important intellectual content. All authors read and
approved the final manuscript, and agreed to be accountable for all
aspects of the work.
Ethics approval and consent to
participate
All animal experimental procedures and protocols
were approved by the Animal Care and Use Committee of the Second
Xiangya Hospital, Central South University, Changsha, China. Human
umbilical cords were collected after obtaining written informed
consent from the donors with institutional review board
approval.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hoste EAJ, Kellum JA, Selby NM, Zarbock A,
Palevsky PM, Bagshaw SM, Goldstein SL, Cerdá J and Chawla LS:
Global epidemiology and outcomes of acute kidney injury. Nat Rev
Nephrol. 14:607–625. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Susantitaphong P, Cruz DN, Cerda J,
Abulfaraj M, Alqahtani F, Koulouridis I and Jaber BL: Acute Kidney
Injury Advisory Group of the American Society of Nephrology: World
incidence of AKI: A meta-analysis. Clin J Am Soc Nephrol.
8:1482–1493. 2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Negi S, Koreeda D, Kobayashi S, Yano T,
Tatsuta K, Mima T, Shigematsu T and Ohya M: Acute kidney injury:
Epidemiology, outcomes, complications, and therapeutic strategies.
Semin Dial. 31:519–527. 2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Schiffl H, Lang SM and Fischer R:
Long-term outcomes of survivors of ICU acute kidney injury
requiring renal replacement therapy: A 10-year prospective cohort
study. Clin Kidney J. 5:297–302. 2012.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Case J, Khan S, Khalid R and Khan A:
Epidemiology of acute kidney injury in the intensive care unit.
Crit Care Res Pract. 2013(479730)2013.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Nisula S, Kaukonen KM, Vaara ST, Korhonen
AM, Poukkanen M, Karlsson S, Haapio M, Inkinen O, Parviainen I,
Suojaranta-Ylinen R, et al: Incidence, risk factors and 90-day
mortality of patients with acute kidney injury in finnish intensive
care units: The FINNAKI study. Intensive Care Med. 39:420–428.
2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Hoste EA, Bagshaw SM, Bellomo R, Cely CM,
Colman R, Cruz DN, Edipidis K, Forni LG, Gomersall CD, Govil D, et
al: Epidemiology of acute kidney injury in critically ill patients:
The multinational AKI-EPI study. Intensive Care Med. 41:1411–1423.
2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Uchino S, Kellum JA, Bellomo R, Doig GS,
Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, et al:
Acute renal failure in critically ill patients: A multinational,
multicenter study. JAMA. 294:813–818. 2005.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ozkok A and Edelstein CL: Pathophysiology
of cisplatin-induced acute kidney injury. Biomed Res Int.
2014(967826)2014.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Shiraishi F, Curtis LM, Truong L, Poss K,
Visner GA, Madsen K, Nick HS and Agarwal A: Heme oxygenase-1 gene
ablation or expression modulates cisplatin-induced renal tubular
apoptosis. Am J Physiol Renal Physiol. 278:F726–F736.
2000.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Zhang B, Ramesh G, Uematsu S, Akira S and
Reeves WB: TLR4 signaling mediates inflammation and tissue injury
in nephrotoxicity. J Am Soc Nephrol. 19:923–932. 2008.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Faubel S, Lewis EC, Reznikov L, Ljubanovic
D, Hoke TS, Somerset H, Oh DJ, Lu L, Klein CL, Dinarello CA and
Edelstein CL: Cisplatin-induced acute renal failure is associated
with an increase in the cytokines interleukin (IL)-1beta, IL-18,
IL-6, and neutrophil infiltration in the kidney. J Pharmacol Exp
Ther. 322:8–15. 2007.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Deng J, Kohda Y, Chiao H, Wang Y, Hu X,
Hewitt SM, Miyaji T, McLeroy P, Nibhanupudy B, Li S and Star RA:
Interleukin-10 inhibits ischemic and cisplatin-induced acute renal
injury. Kidney Int. 60:2118–2128. 2001.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ni J, Hou X, Wang X, Shi Y, Xu L, Zheng X,
Liu N, Qiu A and Zhuang S: 3-deazaneplanocin A protects against
cisplatin-induced renal tubular cell apoptosis and acute kidney
injury by restoration of E-cadherin expression. Cell Death Dis.
10(355)2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lu QB, Du Q, Wang HP, Tang ZH, Wang YB and
Sun HJ: Salusin-β mediates tubular cell apoptosis in acute kidney
injury: Involvement of the PKC/ROS signaling pathway. Redox Biol.
30(101411)2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Scaffidi P, Misteli T and Bianchi ME:
Release of chromatin protein HMGB1 by necrotic cells triggers
inflammation. Nature. 418:191–195. 2002.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Wu H, Ma J, Wang P, Corpuz TM,
Panchapakesan U, Wyburn KR and Chadban SJ: HMGB1 contributes to
kidney ischemia reperfusion injury. J Am Soc Nephrol. 21:1878–1890.
2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Doi K, Ishizu T, Tsukamoto-Sumida M,
Hiruma T, Yamashita T, Ogasawara E, Hamasaki Y, Yahagi N, Nangaku M
and Noiri E: The high-mobility group protein B1-Toll-like receptor
4 pathway contributes to the acute lung injury induced by bilateral
nephrectomy. Kidney Int. 86:316–326. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Ruan Y, Wang L, Zhao Y, Yao Y, Chen S, Li
J, Guo H, Ming C, Chen S, Gong F and Chen G: Carbon monoxide
potently prevents ischemia-induced high-mobility group box 1
translocation and release and protects against lethal renal
ischemia-reperfusion injury. Kidney Int. 86:525–537.
2014.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kim J: Poly(ADP-ribose) polymerase
activation induces high mobility group box 1 release from proximal
tubular cells during cisplatin nephrotoxicity. Physiol Res.
65:333–340. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Zhu F, Chong Lee Shin OL, Xu H, Zhao Z,
Pei G, Hu Z, Yang J, Guo Y, Mou J, Sun J, et al: Melatonin promoted
renal regeneration in folic acid-induced acute kidney injury via
inhibiting nucleocytoplasmic translocation of HMGB1 in tubular
epithelial cells. Am J Transl Res. 9:1694–1707. 2017.PubMed/NCBI
|
|
22
|
Leelahavanichkul A, Huang Y, Hu X, Zhou H,
Tsuji T, Chen R, Kopp JB, Schnermann J, Yuen PST and Star RA:
Chronic kidney disease worsens sepsis and sepsis-induced acute
kidney injury by releasing high mobility group box protein-1.
Kidney Int. 80:1198–1211. 2011.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Wei Q, Dong G, Franklin J and Dong Z: The
pathological role of Bax in cisplatin nephrotoxicity. Kidney Int.
72:53–62. 2007.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Cho HJ, Kim JK, Kim KD, Yoon HK, Cho MY,
Park YP, Jeon JH, Lee ES, Byun SS, Lim HM, et al: Upregulation of
Bcl-2 is associated with cisplatin-resistance via inhibition of Bax
translocation in human bladder cancer cells. Cancer Lett.
237:56–66. 2006.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Nagothu KK, Bhatt R, Kaushal GP and
Portilla D: Fibrate prevents cisplatin-induced proximal tubule cell
death. Kidney Int. 68:2680–2693. 2005.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Morigi M, Rota C, Montemurro T,
Montelatici E, Cicero VL, Imberti B, Abbate M, Zoja C, Cassis P,
Longaretti L, et al: Life-sparing effect of human cord
blood-mesenchymal stem cells in experimental acute kidney injury.
Stem Cells. 28:513–522. 2010.PubMed/NCBI View
Article : Google Scholar
|
|
27
|
Peired AJ, Sisti A and Romagnani P:
Mesenchymal stem cell-based therapy for kidney disease: A review of
clinical evidence. Stem Cells Int. 2016(4798639)2016.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Jiao X, Cai J, Yu X and Ding X: Paracrine
activation of the wnt/β-catenin pathway by bone marrow stem cell
attenuates cisplatin-induced kidney injury. Cell Physiol Biochem.
44:1980–1994. 2017.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Fang TC and Poulsom R: Cell-based
therapies for birth defects: A role for adult stem cell plasticity?
Birth Defects Res C Embryo Today. 69:238–249. 2003.PubMed/NCBI View Article : Google Scholar
|
|
30
|
El-Ashmawy NE, Khedr EG, El-Bahrawy HA and
El-Berashy SA: Effect of human umbilical cord blood-derived
mononuclear cells on diabetic nephropathy in rats. Biomed
Pharmacother. 97:1040–1045. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Pimentel-Coelho PM, Rosado-de-Castro PH,
da Fonseca LM and Mendez-Otero R: Umbilical cord blood mononuclear
cell transplantation for neonatal hypoxic-ischemic encephalopathy.
Pediatr Res. 71:464–473. 2012.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Cui X, Chen L, Xue T, Yu J, Liu J, Ji Y
and Cheng L: Human umbilical cord and dental pulp-derived
mesenchymal stem cells: Biological characteristics and potential
roles in vitro and in vivo. Mol Med Rep. 11:3269–3278.
2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Pittenger MF, Mackay AM, Beck SC, Jaiswal
RK, Douglas R, Mosca JD, Moorman MA, Simonetti DW, Craig S and
Marshak DR: Multilineage potential of adult human mesenchymal stem
cells. Science. 284:143–147. 1999.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Rubinstein P, Dobrila L, Rosenfield RE,
Adamson JW, Migliaccio G, Migliaccio AR, Taylor PE and Stevens CE:
Processing and cryopreservation of placental/umbilical cord blood
for unrelated bone marrow reconstitution. Proc Natl Acad Sci USA.
92:10119–10122. 1995.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Seo Y, Yang SR, Jee MK, Joo EK, Roh KH,
Seo MS, Han TH, Lee SY, Ryu PD, Jung JW, et al: Human umbilical
cord blood-derived mesenchymal stem cells protect against neuronal
cell death and ameliorate motor deficits in Niemann Pick type C1
mice. Cell Transplant. 20:1033–1047. 2011.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Duan SB, Liu GL, Chen GC, Wang P, Pan P
and Xu XQ: Aged rats are susceptible to nephrotoxicity induced by
iodinated contrast media. Ren Fail. 35:150–154. 2013.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Schetza M, Dastab J, Goldsteinc S and
Golperd T: Drug-induced acute kidney injury. Curr Opin Crit Care.
11:555–565. 2005.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Launay-Vacher V, Rey JB, Isnard-Bagnis C,
Deray G and Daouphars M: European Society of Clinical Pharmacy
Special Interest Group on Cancer Care: Prevention of cisplatin
nephrotoxicity: State of the art and recommendations from the
european society of clinical pharmacy special interest group on
cancer care. Cancer Chemother Pharmacol. 61:903–909.
2008.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Perazella MA and Moeckel GW:
Nephrotoxicity from chemotherapeutic agents: Clinical
manifestations, pathobiology, and prevention/therapy. Semin
Nephrol. 30:570–581. 2010.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Freitag J, Bates D, Boyd R, Shah K,
Barnard A, Huguenin L and Tenen A: Mesenchymal stem cell therapy in
the treatment of osteoarthritis: Reparative pathways, safety and
efficacy-a review. BMC Musculoskelet Disord. 17(230)2016.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Eom YW, Shim KY and Baik SK: Mesenchymal
stem cell therapy for liver fibrosis. Korean J Intern Med.
30:580–589. 2015.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Bagno L, Hatzistergos KE, Balkan W and
Hare JM: Mesenchymal stem cell-based therapy for cardiovascular
disease: Progress and challenges. Mol Ther. 26:1610–1623.
2018.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Mendt M, Rezvani K and Shpall E:
Mesenchymal stem cell-derived exosomes for clinical use. Bone
Marrow Transplant. 54 (Suppl 2):S789–S792. 2019.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Morigi M, Imberti B, Zoja C, Corna D,
Tomasoni S, Abbate M, Rottoli D, Angioletti S, Benigni A, Perico N,
et al: Mesenchymal stem cells are renotropic, helping to repair the
kidney and improve function in acute renal failure. J Am Soc
Nephrol. 15:1794–1804. 2004.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Eliopoulos N, Zhao J, Forner K, Birman E,
Young YK and Bouchentouf M: Erythropoietin gene-enhanced marrow
mesenchymal stromal cells decrease cisplatin-induced kidney injury
and improve survival of allogeneic mice. Mol Ther. 19:2072–2083.
2011.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Park JH, Jang HR, Kim DH, Kwon GY, Lee JE,
Huh W, Choi SJ, Oh W, Oh HY and Kim YG: Early, but not late,
treatment with human umbilical cord blood-derived mesenchymal stem
cells attenuates cisplatin nephrotoxicity through immunomodulation.
Am J Physiol Renal Physiol. 313:F984–F996. 2017.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Lee RH, Song JM, Park MY, Kang SK, Kim YK
and Jung JS: Cisplatin-induced apoptosis by translocation of
endogenous Bax in mouse collecting duct cells. Biochem Pharmacol.
62:1013–1023. 2001.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Phinney DG and Prockop DJ: Concise review:
Mesenchymal stem/multipotent stromal cells: The state of
transdifferentiation and modes of tissue repair-current views. Stem
Cells. 25:2896–2902. 2007.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Herrera MB, Bussolati B, Bruno S, Fonsato
V, Romanazzi GM and Camussi G: Mesenchymal stem cells contribute to
the renal repair of acute tubular epithelial injury. Int J Mol Med.
14:1035–1041. 2004.PubMed/NCBI
|
|
50
|
Tögel F, Weiss K, Yang Y, Hu ZM, Zhang P
and Westenfelder C: Vasculotropic, paracrine actions of infused
mesenchymal stem cells are important to the recovery from acute
kidney injury. Am J Physiol Renal Physiol. 292:F1626–F1635.
2007.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Tögel F, Zhang P, Hu ZM and Westenfelder
C: VEGF is a mediator of the renoprotective effects of multipotent
marrow stromal cells in acute kidney injury. J Cell Mol Med.
13:2109–2114. 2009.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Zhou Y, Xu H, Xu W, Wang B, Wu H, Tao Y,
Zhang B, Wang M, Mao F, Yan Y, et al: Exosomes released by human
umbilical cord mesenchymal stem cells protect against
cisplatin-induced renal oxidative stress and apoptosis in vivo and
in vitro. Stem Cell Res Ther. 4(34)2013.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Zhang G, Zou X, Huang Y, Wang F, Miao S,
Liu G, Chen M and Zhu Y: Mesenchymal stromal cell-derived
extracellular vesicles protect against acute kidney injury through
anti-oxidation by enhancing Nrf2/ARE activation in rats. Kidney
Blood Press Res. 41:119–128. 2016.PubMed/NCBI View Article : Google Scholar
|