Introduction
Epilepsy is a common neurological encephalopathy
mainly caused by abnormal discharge of brain neurons, with
transient functional abnormalities of the nervous system as the
main characteristic (1). Epileptic
patients who suffer from long-term recurrent seizures are likely to
develop further brain injury (2).
Recently, the development of medical technology had made the
diagnosis of epilepsy more accurate, and epilepsy treatment is
mainly based on antiepileptic drugs. However, although the symptoms
of epilepsy are manageable in most patients, not all can be
effectively treated (3,4).
Antiepileptic drugs comprise traditional and new
antiepileptic drugs. Traditional antiepileptic drugs are mainly
represented by carbamazepine. Although they have good efficacy,
compared with new epilepsy drugs, most patients have more adverse
reactions when taking traditional antiepileptic drugs, leading to
drug intolerance, which causes patients to end treatment (5,6).
Oxcarbazepine, a copper-based derivative of carbamazepine, can
reduce the induction of liver enzymes and improve patient tolerance
while playing a therapeutic role (7). Lamotrigine is also an antiepileptic
drug, which is widely used clinically. As a derivative of
benzotriazine, lamotrigine not only has better efficacy in
epilepsy, but also has less of an effect on liver and kidney
function (8). The incidence of
depression is high in epileptic patients due to the use of
long-term medication and the adverse effects of the disease on
quality of life. Depression will not only further aggravate the
epileptic seizures, but also seriously affects the quality of life
of patients (9). Therefore, it is
imperative for epileptic patients to receive antidepressant
treatment while treating epilepsy. However, both lamotrigine and
oxcarbazepine have only recently been used in patients with
epilepsy and depression, with relatively few clinical applications
(10,11). Escitalopram, a new antidepressant,
can inhibit the reuptake of 5-hydroxytryptamine (5-HT) to achieve a
better antidepressant effect (12).
However, to the best of our knowledge, relatively
few studies on the efficacy of oxcarbazepine and lamotrigine
combined with escitalopram in epileptic patients have been
performed. Hence, the efficacy of oxcarbazepine and lamotrigine
combined with escitalopram in epileptic patients and its influence
on prognostic quality of life were studied, so as to provide a more
appropriate treatment scheme for patients with epilepsy and
depression.
Materials and methods
General data
A total of 108 patients with epilepsy combined with
depression were selected for the present study between July 2014 to
March 2017. There were 58 males and 50 females, with an age range
of 28-38 years (mean age, 33.97±3.26 years). All were of Han
Chinese descent. Loss of consciousness was the main seizure
symptom. Among the cohort, 53 patients treated with oxcarbazepine
combined with escitalopram were assigned to group A, and 55
patients treated with lamotrigine combined with escitalopram were
assigned to group B. The inclusion criteria were as follows: i)
Patients who met the criteria for diagnosis and classification of
epilepsy with depression (11); ii)
course of disease >3 months and seizure frequency >1 month;
and iii) patients with depressive disorder (Zung Self-Rating
Depression Scale >53) (11). The
exclusion criteria were as follows: i) Patients had previously
taken antiepileptic or antidepressant drugs; ii) patients with
severe liver and kidney dysfunction; iii) pregnant or lactating
patients; iv) patients with central nervous system diseases such as
cerebral infarction and hemorrhage; v) patients with communication
and cognitive dysfunction; and vi) patients who did not cooperate
with the experiment. Patients agreed to participate in the
experiment and signed written informed consent.
Treatment plan
Patients in group A were treated with oxcarbazepine
(Novartis International AG) combined with escitalopram.
Oxcarbazepine was initially taken at a dose of 300 mg/day twice a
day, and the dose was increased by 100 mg every 3 days until the
does reached 900 mg. On this basis, escitalopram (Sichuan Kelun
Pharmaceutical Co., Ltd.) was added, and the initial dose was 5
mg/d, once a day. After one week, the dose was adjusted according
to patients' tolerance. The maximum dose was no more than 10
mg/d.
Patients in group B were treated with lamotrigine
(Guilin Sanjin Pharmaceutical Co., Ltd.) combined with
escitalopram. The initial dose of lamotrigine was 25 mg/day, twice
a day. After 1-week administration, the daily dose was adjusted by
increasing the dose by 25 mg per week. Once the dose reached the
effective therapeutic dose, the increase was stopped, with the
maximum dose not exceeding 150 mg/day. The initial dose of
escitalopram was 5 mg/day, once a day. After 1 week, the dose was
adjusted according to the tolerance of patients, with the maximum
dose not exceeding 10 mg/day.
Observational indicators
The efficacy of the drugs after 6-month treatment in
patients from the two groups was evaluated and categorized as
‘cured’ (no seizure during the observation period), ‘significantly
effective’ (seizure frequency reduced by >75%), ‘effective’
(seizure frequency reduced by >50%) and ‘ineffective’ (seizure
frequency not significantly reduced or even increased). The total
efficacy rate of the treatment was calculated based on the
following formula: (Number of ‘cured’ + number of ‘significantly
effective’ + number of 'effective')/total number of patients x100.
The frequency and duration of epileptic seizures were recorded and
compared before and 6 months after treatment. Hamilton Depression
Rating (HAMD) (13) and
Montgomery-Asberg Depression Rating (MADRS) (14) scores were used to evaluate and
compare the depressive states of patients from both groups before
and 6 months after treatment. The improvement of
electroencephalogram (EEG) epileptic discharge between the two
groups was categorized as ‘control’ (epileptic discharge completely
disappeared), ‘significantly improved’ (epileptic discharge was
reduced by >50%), ‘improved’ (epileptic discharge was reduced by
>25%) and ‘ineffective’ (epileptic discharge was reduced by
<25%). The improvement rate was calculated using the following
formula: (Number of ‘control’ patients + number of ‘significantly
improved’ patients + number of 'improved' patients)/total number of
patients x100. Adverse reactions of patients, which included
nausea, lethargy, dizziness, headache, rash and loss of appetite
from both groups throughout 6-month treatment were recorded and
compared. The Quality of Life in Epilepsy-Patients-Weighted 31p
scoring system was used to evaluate and compare the quality of life
of patients 6 months after treatment (15). The following domains were assessed:
Emotion, cognition, social relations, energy, health status and
overall quality of life, with a total score of 100 points. Higher
scores represent a higher quality of life. The patients were
followed up by telephones, outpatient services and WeChat (Tencent)
for 1 year. The 1-year drug retention rates of patients from the
two groups were recorded and compared, and the time and reason of
drug withdrawal were recorded.
Statistical analysis
SPSS 19.0 (IBM Corp.) was used for statistical
analysis and data were expressed as the mean ± SD (n=3). Counting
data were analyzed using χ2 test. Comparisons between
two groups were analyzed by Student's unpaired t-test and those
before and after treatment within one group were analyzed by paired
t-test. Two-way ANOVA was used for multiple comparisons, followed
by Tukey's HSD post hoc test. GraphPad Prism 6.0 (GraphPad, Inc.)
was used for graphical representation. P<0.05 was considered to
be statistically significant.
Results
Comparison of general data
No significant difference in sex, age, body mass
index, course of disease, marital status, seizure type, creatinine
and urea nitrogen levels and place of residence was found between
the two groups (Table I).
 | Table IGeneral characteristics of
patients. |
Table I
General characteristics of
patients.
| Characteristics | Group A n=53 | Group B n=55 | t/χ2
value | P-value |
|---|
| Sex | | | 0.032 | 0.858 |
|
Male | 28 (52.83) | 30 (54.55) | | |
|
Female | 25 (47.17) | 25 (45.45) | | |
| Age, years | | | 0.157 | 0.692 |
|
≤33 | 24 (45.28) | 27 (49.10) | | |
|
>33 | 29 (54.72) | 28 (50.90) | | |
| BMI,
kg/m2 | | | 0.000 | 0.997 |
|
≤22 | 26 (49.06) | 27 (49.10) | | |
|
>22 | 27 (50.94) | 28 (50.90) | | |
| Course of disease,
years | 3.52±0.26 | 3.49±0.24 | 0.623 | 0.534 |
| Marital status | | | 0.019 | 0.892 |
|
Married | 35 (66.04) | 37 (67.27) | | |
|
Unmarried | 18 (33.96) | 18 (32.73) | | |
| Seizure type | | | 0.125 | 0.724 |
|
Systemic | 31 (58.49) | 34 (61.82) | | |
|
Partial | 22 (41.51) | 21 (38.18) | | |
| Creatinine,
μmol/l | 69.31±9.26 | 70.09±9.37 | 0.435 | 0.665 |
| Urea nitrogen,
mmol/l | 6.15±1.42 | 6.11±1.37 | 1.049 | 0.882 |
| Place of
residence | | | 0.040 | 0.842 |
|
Cities and
towns | 28 (52.83) | 28 (50.91) | | |
|
Countryside | 25 (47.17) | 27 (49.09) | | |
Comparison of drug efficacy in
patients
No significant difference in the total efficacy rate
of treatment was found between the two groups (Table II).
| Table IIComparison of drug efficacy between
patients groups. |
Table II
Comparison of drug efficacy between
patients groups.
| Efficacy | Group A n=53 | Group B n=55 | t/χ2
value | P-value |
|---|
| Cured | 25 (47.17) | 26 (47.27) | 0.000 | 0.992 |
| Significantly
effective | 16 (30.19) | 17 (30.91) | 0.007 | 0.935 |
| Effective | 6 (11.32) | 7 (12.73) | 0.050 | 0.822 |
| Ineffective | 6 (11.32) | 5 (9.09) | 0.147 | 0.702 |
| Total efficacy
rate | 47 (88.68) | 50 (90.90) | 0.147 | 0.702 |
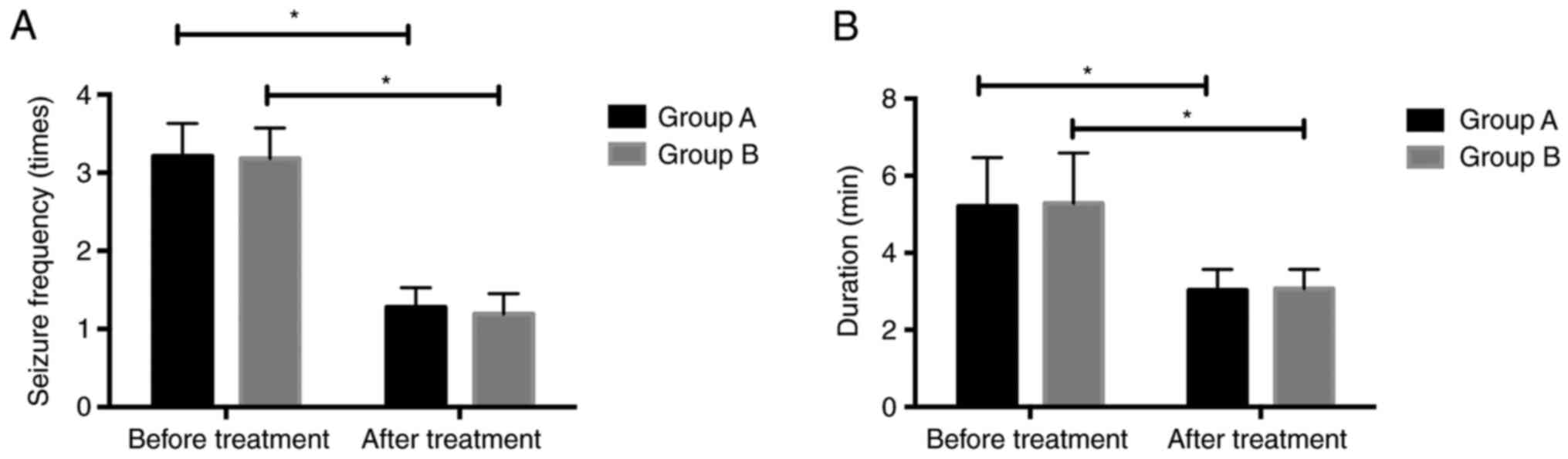
Comparison of frequency and duration
of epileptic seizures before and after treatment
The epileptic seizure frequency of patients from
group A before and 6 months after treatment was 3.21±0.42
times/month and 1.28±0.25 times/month, with a duration of 5.21±1.26
and 3.03±0.54 min, respectively. The frequency of epileptic
seizures of patients from group B before and six months after
treatment was 3.18±0.39 times/month and 1.19±0.26 times/month, with
a duration of 5.28±1.31 and 3.07±0.50 min, respectively. The
frequency and duration of epileptic seizures after treatment in
both groups decreased significantly compared with before treatment.
No significant difference was found in the frequency and duration
of epileptic seizures between groups A and B before or after
treatment (Fig. 1).
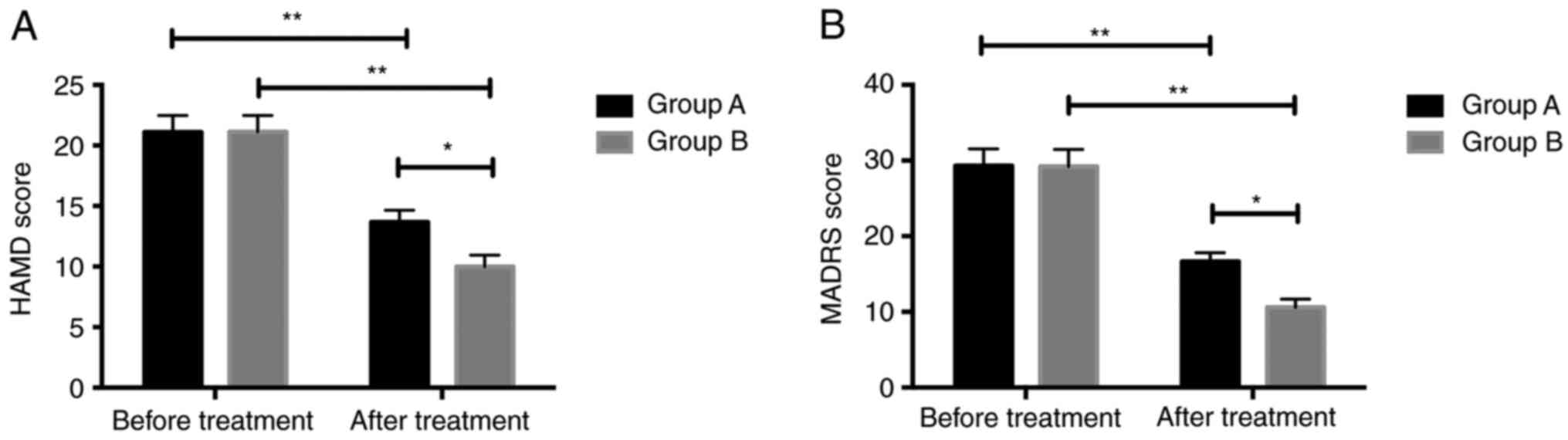
Comparison of HAMD and MADRS scores
before and after treatment
The HAMD scores of patients from group A were
21.11±1.37 and 13.67±0.98 before and six months after treatment,
respectively, while the MADRS scores of group A patients were
29.33±2.21 and 16.65±1.18 before and six months after treatment,
respectively. The HAMD scores of patients from group B were
21.13±1.35 and 9.98±0.96 before and six months after treatment,
respectively, while the MADRS scores of group B patients were
29.22±2.25 and 10.59±1.09 before and six months after treatment,
respectively. The HAMD and MADRS scores of patients of both groups
after treatment were significantly lower compared before treatment.
The scores of patients in group B after treatment were
significantly lower compared with those of group A patients
(Fig. 2).
Improvement of EEG epileptic discharge
of patients in the two groups
No significant difference in the improvement rate of
EEG epileptic discharge was measured between the two groups
(P>0.05). The control rate of group B was significantly higher
than that of group A (P=0.001) (Table
III).
| Table IIIImprovement of electroencephalogram
epileptic discharge in patients |
Table III
Improvement of electroencephalogram
epileptic discharge in patients
| Efficacy | Group A n=53 | Group B n=55 | t/χ2
value | P-value |
|---|
| Control | 11 (20.75) | 23 (41.82) | 10.89 | 0.001 |
| Significantly
improved | 21 (39.62) | 12 (21.82) | 4.032 | 0.045 |
| Improved | 14 (26.42) | 12 (21.82) | 0.312 | 0.576 |
| Ineffective | 7 (13.21) | 8 (14.55) | 0.040 | 0.841 |
| Improvement
rate | 46 (86.79) | 47 (85.45) | 0.040 | 0.841 |
Comparison of adverse reactions from
patients
The total incidence rate of adverse reactions of
patients in group B was significantly lower compared with that of
those in group A (Table IV).
| Table IVComparison of adverse reactions
between patients groups. |
Table IV
Comparison of adverse reactions
between patients groups.
| Reaction | Group A n=53 | Group B n=55 | t/χ2
value | P-value |
|---|
| Nausea | 1 (5.66) | 0 | 1.047 | 0.306 |
| Sleepiness | 2 (3.77) | 1 (1.82) | 0.382 | 0.567 |
| Dizziness,
headache | 2 (3.77) | 1 (1.82) | 0.382 | 0.567 |
| Rash | 6 (3.77) | 1 (1.82) | 4.021 | 0.045 |
| Loss of
appetite | 1 (5.66) | 1 (1.82) | 0.000 | 0.979 |
| Overall incidence
rate of adverse reactions | 12 (22.64) | 4 (7.27) | 5.052 | 0.025 |
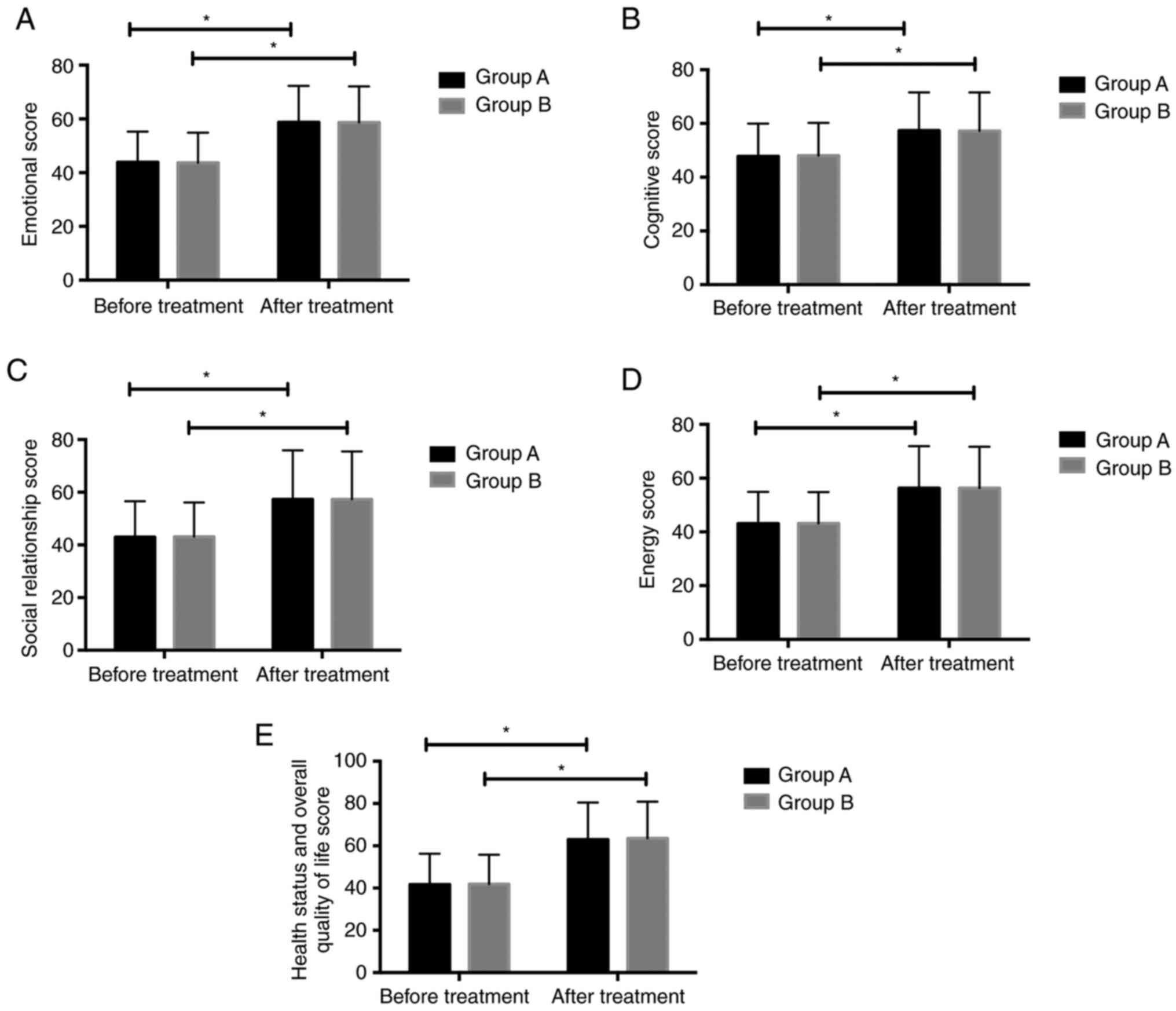
Comparison of quality of life of
patients before and after treatment
Emotional, cognitive, social relationship, energy,
health status and overall quality of life scores before treatment
in group A were 43.92±11.37, 47.79±12.18, 42.96±13.62, 43.09±11.79
and 41.67±14.66, respectively. Emotional, cognitive, social
relationship, energy, health status and overall quality of life
scores after treatment in group A were 58.74±13.54, 57.34±14.23,
57.29±18.63, 56.31±15.58 and 62.92±17.54, respectively. Emotional,
cognitive, social relationship, energy, health status and overall
quality of life scores before treatment in group B were
43.67±11.26, 48.01±12.21, 43.11±12.99, 43.17±11.67 and 41.89
±13.91, respectively. Emotional, cognitive, social relationship,
energy, health status and overall quality of life scores after
treatment in group B were 58.71±13.41, 57.26 ±14.31, 57.33±18.14,
56.27±15.43 and 63.56±17.33, respectively. No significant
difference in the quality of life was measured between both groups
before treatment. Quality of life scores in the two groups were all
higher after treatment compared with before treatment. No
significant difference in the quality of life after treatment was
found between groups A and B (Fig.
3).
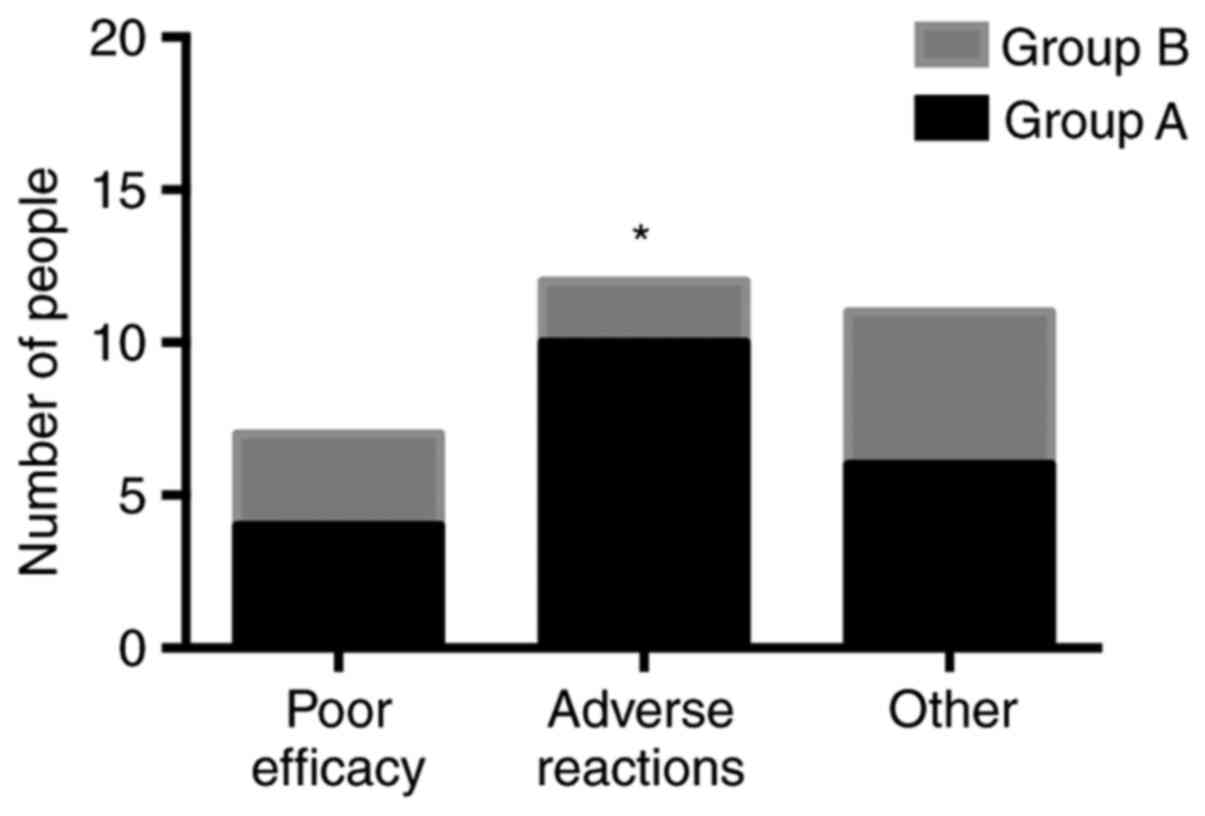
One-year drug withdrawal rate and
withdrawal reason records of patients
Twenty patients in group A stopped taking the drugs
within one year, with a withdrawal rate of 37.73%. Among them, 4
patients stopped taking the drugs due to poor efficacy, 10 patients
stopped taking the drugs due to adverse reactions and 6 stopped
taking the drugs due to other reasons (Fig. 4). Ten patients from group B stopped
taking the drugs within one year, with a withdrawal rate of 18.18%.
Among them, 3 patients stopped taking the drugs due to poor
efficacy, 2 patients stopped taking the drugs due to adverse
reactions and 5 patients stopped taking the drugs due to other
reasons (Fig. 4). The one-year
withdrawal rate of patients from group B was significantly lower
compared with that of those from group A (Table V).
| Table VOne-year drug withdrawal rate of
patients. |
Table V
One-year drug withdrawal rate of
patients.
| Factor | Group A n=53 | Group B n=55 | t/χ2
value | P-value |
|---|
| Drug
withdrawal | | | 5.144 | 0.023 |
|
Yes | 20 (37.73) | 10 (18.18) | | |
|
No | 33 (62.26) | 45 (81.82) | | |
Discussion
Epilepsy is a chronic nervous system disease with
paroxysmal cranial nerve dysfunction caused by abnormal discharge
of brain neurons. Its pathogenesis is very complex and it is often
accompanied by depressive disorders (16). Epilepsy and depressive disorder are
pathogenically similar and might be caused by reduced
neurotransmitter release (17). The
occurrence of epilepsy could promote the production of excitatory
amino acids. This could lead to a reduction in 5-HT activity, which
is one of the main causes of depression (18). A decrease in 5-HT activity can also
further induce epilepsy, resulting in a cycle of epilepsy and
depressive disorder (19).
The present study explored the efficacy of two new
antiepileptic drugs (oxcarbazepine and lamotrigine) combined with
the antidepressant escitalopram for the treatment of epilepsy
combined with depressive disorder. The efficacy in patients from
the two groups was compared, and the results showed that there was
no significant difference in the total efficacy rates. The
frequency and duration of epileptic seizures after treatment from
the two groups significantly reduced compared with before
treatment, and EEG epileptic discharge also improved. These results
suggested that oxcarbazepine and lamotrigine had good efficacy in
epilepsy patients. Another study showed that oxcarbazepine and
lamotrigine had good efficacy on epilepsy patients, consistent with
the present results (20). The main
mechanism of oxcarbazepine is inhibiting the repeated discharge of
neurons by blocking voltage-dependent sodium ion channels in brain
cells (21). The main mechanism of
lamotrigine is inhibiting voltage-dependent calcium and sodium
channels to control the temperature of the presynaptic membrane and
inhibit the release of neurotransmitters, ultimately reducing
abnormal discharge of neurons (22). The HAMD and MADRS scores of patients
from both groups before and after treatment were also compared. The
results showed that the two scores of patients after treatment were
significantly lower compared with before treatment and the scores
of patients in group B after treatment were obviously lower
compared those of patients in group A. The results suggested that
the depressive disorders in patients from the two groups after
treatment were significantly relieved, and lamotrigine combined
with escitalopram was more effective than oxcarbazepine combined
with escitalopram at relieving depressive disorders. A previous
study verified that lamotrigine showed antiepileptic and
anti-bipolar depression effects (23). Lamotrigine treatment managed
epileptic symptoms, and improved depressive symptoms and the
quality of life of patients (24).
Escitalopram was chosen as a combination drug as it has a selective
inhibitory effect on 5-HT and an antidepressant effect (25).
Subsequently, the adverse reactions of patients from
the two groups were recorded and compared. The results showed that
the total incidence rate of adverse reactions of patients from
group B was significantly lower compared with that of group A.
Although the incidence rate of rash in patients from group A was
higher compared with that in group B patients, all patients
experienced relief from their adverse reactions after symptomatic
treatment. A previous study indicated that rash was the most common
adverse reaction of oxcarbazepine, which was due to the possibility
of rash induced by the human leukocyte antigen allele
HLA-B*1502(26). Finally, the
quality of life before and after treatment and the 1-year drug
retention rate of patients from both groups were compared. The
results showed that the quality of life scores of patients after
treatment significantly improved compared with before treatment.
The 1-year drug retention rate of patients from group B was
significantly higher compared with patients from group A. A
previous study found that the drug retention rate of oxcarbazepine
was significantly lower compared with that of lamotrigine when
recording the drug retention rate of epileptic patients 3 years
after treatment (27). Another
study found that the main reason for the lower drug retention rate
of oxcarbazepine compared with lamotrigine was the higher rate of
adverse reactions, which was also the primary reason for patients
to stop taking the drugs (28).
To summarize, oxcarbazepine and lamotrigine combined
with escitalopram showed good efficacy in epileptic patients with
depressive disorder, and they may effectively improve quality of
life. Lamotrigine combined with escitalopram presented with a
better antidepressant effect and better safety compared with
oxcarbazepine and escitalopram. However, there are still some
limitations to the present study. For example, the efficacy of
different doses of drugs has not been discussed. There may be some
differences in the conclusion due to the small sample size; on the
other hand, because of individual differences, the dosages of drugs
were not the same among all patients, which may also lead to some
differences in the results.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XZ conceived and designed the study and drafted the
paper. XZ and WZ collected, analyzed and interpreted the
experimental data, and critically revised the manuscript. Both
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Sunshine Union Hospital. Written informed consent was obtained from
patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kanner AM, Ashman E, Gloss D, Harden C,
Bourgeois B, Bautista JF, Abou-Khalil B, Burakgazi-Dalkilic E,
Llanas Park E, Stern J, et al: Practice guideline update summary:
Efficacy and tolerability of the new antiepileptic drugs II:
Treatment-resistant epilepsy: Report of the Guideline Development,
Dissemination, and Implementation Subcommittee of the American
Academy of Neurology and the American Epilepsy Society. Neurology.
92:82–90. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Chen Z, Brodie MJ, Liew D and Kwan P:
Treatment outcomes in patients with newly diagnosed epilepsy
treated with established and new antiepileptic drugs: A 30-year
longitudinal cohort study. JAMA Neurol. 75:279–286. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Cooper YA, Pianka ST, Alotaibi NM, Babayan
D, Salavati B, Weil AG, Ibrahim GM, Wang AC and Fallah A:
Repetitive transcranial magnetic stimulation for the treatment of
drug-resistant epilepsy: A systematic review and individual
participant data meta-analysis of real-world evidence. Epilepsia
Open. 3:55–65. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Beamer E, Fischer W and Engel T: The
ATP-gated P2X7 receptor as a target for the treatment of
drug-resistant epilepsy. Front Neurosci. 11(21)2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Zhang L, Wang C and Li W: A meta-analysis
of randomized controlled trials on levetiracetam in the treatment
of pediatric patients with epilepsy. Neuropsychiatr Dis Treat.
14:769–779. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Liu JT, Liu B and Zhang H: Surgical versus
medical treatment of drug-resistant epilepsy: A systematic review
and meta-analysis. Epilepsy Behav. 82:179–188. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Yun JH: Comparison of lamotrigine and
oxcarbazepine monotherapy for pediatric focal epilepsy: An
observational study. Seizure. 60:123–126. 2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Tombini M, Pellegrino G, Assenza G and
Lazzaro VD: De novo multifocal myoclonus induced by lamotrigine in
a temporal lobe epilepsy case. J Neurol Sci. 373:31–32.
2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Singh T, Kaur T and Goel RK: Adjuvant
quercetin therapy for combined treatment of epilepsy and comorbid
depression. Neurochem Int. 104:27–33. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Luszczki JJ, Wlaz A, Karwan S,
Florek-Luszczki M and Czuczwar SJ: Effects of WIN 55,212-2 mesylate
on the anticonvulsant action of lamotrigine, oxcarbazepine,
pregabalin and topiramate against maximal electroshock-induced
seizures in mice. Eur J Pharmacol. 720:247–254. 2013.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Thelengana A, Shukla G, Srivastava A,
Singh MB, Gupta A, Rajan R, Vibha D, Pandit AK and Prasad K:
Cognitive, behavioural and sleep-related adverse effects on
introduction of levetiracetam versus oxcarbazepine for epilepsy.
Epilepsy Res. 150:58–65. 2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Gorman JM, Korotzer A and Su G: Efficacy
comparison of escitalopram and citalopram in the treatment of major
depressive disorder: Pooled analysis of placebo-controlled trials.
CNS Spectr. 7 (Suppl 1):40–44. 2002.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Gill SJ, Lukmanji S, Fiest KM, Patten SB,
Wiebe S and Jetté N: Depression screening tools in persons with
epilepsy: A systematic review of validated tools. Epilepsia.
58:695–705. 2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Carneiro AM, Fernandes F and Moreno RA:
Hamilton depression rating scale and montgomery-asberg depression
rating scale in depressed and bipolar I patients: psychometric
properties in a Brazilian sample. Health Qual Life Outcomes.
13(42)2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Wijnen BF, Mosweu I, Majoie MH, Ridsdale
L, de Kinderen RJ, Evers SM and McCrone P: A comparison of the
responsiveness of EQ-5D-5L and the QOLIE-31P and mapping of
QOLIE-31P to EQ-5D-5L in epilepsy. Eur J Health Econ. 19:861–870.
2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Peng WF, Fan F, Li X, Zhang QQ, Ding J and
Wang X: Different behavioral and pathological changes between
epilepsy-associated depression and primary depression models.
Epilepsy Behav. 83:212–218. 2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Rider FK, Danilenko OA, Grishkina MN,
Kustov GV, Akzhigitov RG, Lebedeva AV and Gekht AB: Depression and
epilepsy: Comorbidity, pathogenetic similarity, and principles of
treatment. Neurosci Behav Physiol. 48:78–82. 2018.
|
|
18
|
Josephson CB, Lowerison M, Vallerand I,
Sajobi TT, Patten S, Jette N and Wiebe S: Association of depression
and treated depression with epilepsy and seizure outcomes: A
multicohort analysis. JAMA Neurol. 74:533–539. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Mula M: Depression in epilepsy. Curr Opin
Neurol. 30:180–186. 2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Johannessen Landmark C, Baftiu A, Tysse I,
Valsø B, Larsson PG, Rytter E and Johannessen SI: Pharmacokinetic
variability of four newer antiepileptic drugs, lamotrigine,
levetiracetam, oxcarbazepine, and topiramate: A comparison of the
impact of age and comedication. Ther Drug Monit. 34:440–445.
2012.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Glauser TA: Oxcarbazepine in the treatment
of epilepsy. Pharmacother J Hum Pharmacol Drug Ther. 21:904–919.
2012.
|
|
22
|
D'Anto J, Wnuk W, Rossetti AO, Decosterd
LA, Buclin T and Novy J: Lamotrigine serum levels: Ceiling effect
in people with epilepsy in remission? Epilepsy Behav. 74:41–44.
2017.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Zhang M, Ming LI, Zhang X, et al:
The clinical efficacy of lamotrigine in the treatment of epilepsy
with depression and the influence on cognitive function. Chinese
Journal of Medicinal Guide, 2017.
|
|
24
|
Martinović Z, Buder N, Milovanović M and
Velićković R: Antiepileptic, behavioral, and antidepressant effects
of adjuvant lamotrigine therapy in drug-resistant epilepsy.
Vojnosanit Pregl. 61:485–490. 2004.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Azorin JM, Llorca PM, Despiegel N and
Verpillat P: Escitalopram is more effective than citalopram for the
treatment of severe major depressive disorder. Encephale.
30:158–166. 2004.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Kutluay E, McCague K, D'Souza J and
Beydoun A: Safety and tolerability of oxcarbazepine in elderly
patients with epilepsy. Epilepsy Behav. 4:175–180. 2003.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Sunwoo JS, Park BS, Ahn SJ, Hwang S, Park
CY, Jun JS, Kim DW, Lee ST, Jung KH, Park KI, et al: Three-year
retention rates of levetiracetam, topiramate, and oxcarbazepine: A
retrospective Hospital-based Study. Clin Neuropharmacol. 40:56–62.
2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Reilly C, Atkinson P, Das KB, Chin RF,
Aylett SE, Burch V, Gillberg C, Scott RC and Neville BG:
Neurobehavioral comorbidities in children with active epilepsy: A
population-based study. Pediatrics. 133:e1586–e1593.
2014.PubMed/NCBI View Article : Google Scholar
|