Introduction
Venous thromboembolism (VTE) is a multi-factorial
disease, and several findings have suggested that inflammation
might play a role in shifting the hemostatic balance towards a
pro-thrombotic state (1-4).
Moreover, studies have demonstrated the frequency of VTE events in
infected patients (5,6). The most recent studies on patients
infected by SARS-CoV-2 have shown high levels of D-dimer and
fibrinogen-derived peptide (FDP) (7). Patients infected by SARS-CoV-2 were
affected by very serious VTE events. Thus, VTE is closely linked to
most inflammatory conditions. The role played by inflammation in
promoting hyper-coagulation and counteracting systemic fibrinolysis
seems crucial. The so-called ‘cytokine storm’ triggers excessive
inflammation due to the bloodstream release of several
pro-inflammatory cytokines (8). The
role of leukocytes both in thrombus generation and vein remodeling
has not yet been clarified (9),
whereas pleiotropic interleukin (IL)-6 and the development of
thrombotic plugs in the venous circulation of the lower limbs
(10) seem to play a crucial role.
The hemodynamic disorders in venous circulation especially near
venous valves, provoke hypoxia and oxidative stress, whereas
several endogenous anticoagulants are expressed by intact
endothelium (i.e., thrombomodulin, tissue factor pathway inhibitor,
endothelial protein C receptor) (1). Leukocyte recruitment, adhesion
receptor expression and tissue factor release initiate coagulation
pathways (11-14).
Therefore, activating the coagulation system is the main step in
venous thrombosis, while the role of endothelium activation, as
well as that of platelets, still require clarification. Concerning
the role played by inflammation several studies demonstrated a key
role of IL-6 in the development of deep vein thrombosis (DVT) in
lower limbs (15,16). Hypercoagulation is the main
mechanism to be counteracted in treating patients with VTE, both
DVT and PE. Here it is noted that PE has a high mortality risk,
often the consequence of progressive, under-treated or undiagnosed
and untreated DVT (17).
Anticoagulant drugs are the first response in combating VTE and
DVT. A number of factors (obesity, recent trauma, recent surgery,
reduced mobilization, solid and non-solid cancer and genetic
factors) have been listed as risk factors for DVT although the
mechanisms involved in VTE are still under debate (11,18,19).
Low-molecular-weight heparins (LMWH) show concomitant
anti-coagulant and anti-inflammatory activities reducing levels of
inflammatory factors, including IL-6(20). Recently, direct oral anticoagulants
(DOACs) have demonstrated favorable results in combating VTE. DOACs
showed anti-inflammatory capabilities in reducing the abnormal
release of pro-inflammatory factors in addition to inhibiting the
activation of factor X of the coagulation cascade (21-25).
Our study focuses on the capability of DOACs in reducing plasma
level of IL-6 in patients having DVT of the lower limbs.
Patients and methods
The potential anti-inflammatory activity of DOACs in
20 patients hospitalized with lower limb DVT was investigated. The
patients were hospitalized at the Internal Medicine Unit of the
Catania University Hospital ‘Policlinico-Vittorio Emanuele’
(Catania, Italy). In diagnosing DVT, we checked for compression of
one or more lower limb veins (CUS test) and any echogenic material
(thrombus) inside the veins. These DVT patients were initially
assigned to the conventional therapy of LMWHs (5 days) and then
treated with DOACs (Dabigatran 150 mg daily, Edoxaban 60 mg daily)
from the sixth day. As controls, 22 healthy blood samples were
obtained from previous case-control studies. Clinic, pathologic and
demographic features and routine clinical biochemistry data were
retrieved for each sample (Table
I). The blood samples were drawn in the morning 5 days after
patients started the DOAC therapy and after 12 h of fasting. All
the patients supplied a blood sample 10 days after the starting of
the DOACs drugs. Buffy coats were obtained by centrifuging (2000 x
g for 10 min) according to standard procedure. All the sampled
patients were informed on the study and they gave their verbal
consensus. Total RNA was extracted from the Buffy Coat samples
using TRIzol™ LS reagent (cat. no. 10296028; Thermo Fisher
Scientific, Inc.) according to the manufacturer's instructions.
After treatment with DNase I RNase-free (cat. no. EN0525; Thermo
Fisher Scientific, Inc.), 400 ng of treated RNA (final
concentration 20 ng/µl) was converted into cDNA using the
SuperScript™ IV Reverse Transcriptase kit (cat. no. 18090050;
Thermo Fisher Scientific, Inc.) following the manufacturer's
protocol. Then, 2.5 µl of each cDNA underwent Real-Time
amplification using Luminaris Color HiGreen qPCR Master Mix, high
ROX (cat. no. K0362; Thermo Fisher Scientific, Inc.). The
amplification of IL-6 and the GAPDH gene for reference, was
performed with the 7300 Real-Time PCR System (Applied Biosystems;
Thermo Fisher Scientific, Inc.) using the primer pairs reported as
follows: forward (F): 5'-CACTGGCAGAAAACAACC TGA-3' and reverse (R):
5'-AGCTCTGGCTTGTTCCTC ACT-3' for IL-6 and F:
5'-AGAAGGCTGGGGCTCATTTG-3' and R: 5'-AGGGGCCATCCACAGTCTTC-3' for
GAPDH. Thermal conditions: 50˚C for 2 min, followed by 95˚C for 10
min, and 40 cycles of 95˚C for 15 sec, 60˚C for 30 sec and 72˚C for
30 sec. The relative expression levels of IL-6 were obtained by the
2-ΔΔCq method (26).
 | Table IDemographic and clinicopathological
characteristics of the samples. |
Table I
Demographic and clinicopathological
characteristics of the samples.
| Characteristics | CTRL | DVT | P-value |
|---|
| Age (years), median
(range) | 48 (41.7-62) | 56 (46-71) | 0.2392b |
| Sex, no. (%) | | | |
|
Male | 12 (54.5) | 12 (63.15) | 0.76a |
|
Female | 10 (45.5) | 7 (36.85) | |
| CRP, median
(range) | 2.062
(0.79-6.96) | 6 (3-11) | 0.04b |
The study was conducted in accordance with the
Declaration of Helsinki, and the protocol was approved by the
Ethics Committee of the Garibaldi Hospital (Catania, Italy;
resolution n.23/2016/CECT2). Patients were informed about the
objective of the study and were asked to give verbal informed
consent to participate in it and to withdraw blood samples. All
subjects gave their informed consent for inclusion before
participating in the study.
Statistical analysis
Differential analyses were performed using the
non-parametric Mann-Whitney test. Fisher's exact test was used to
analyze the contingency table of the demographic and
clinical-pathological characteristics. The analyses were performed
using GraphPad Prism (GraphPad Software, Inc.). All experiments
were performed in triplicate.
Results
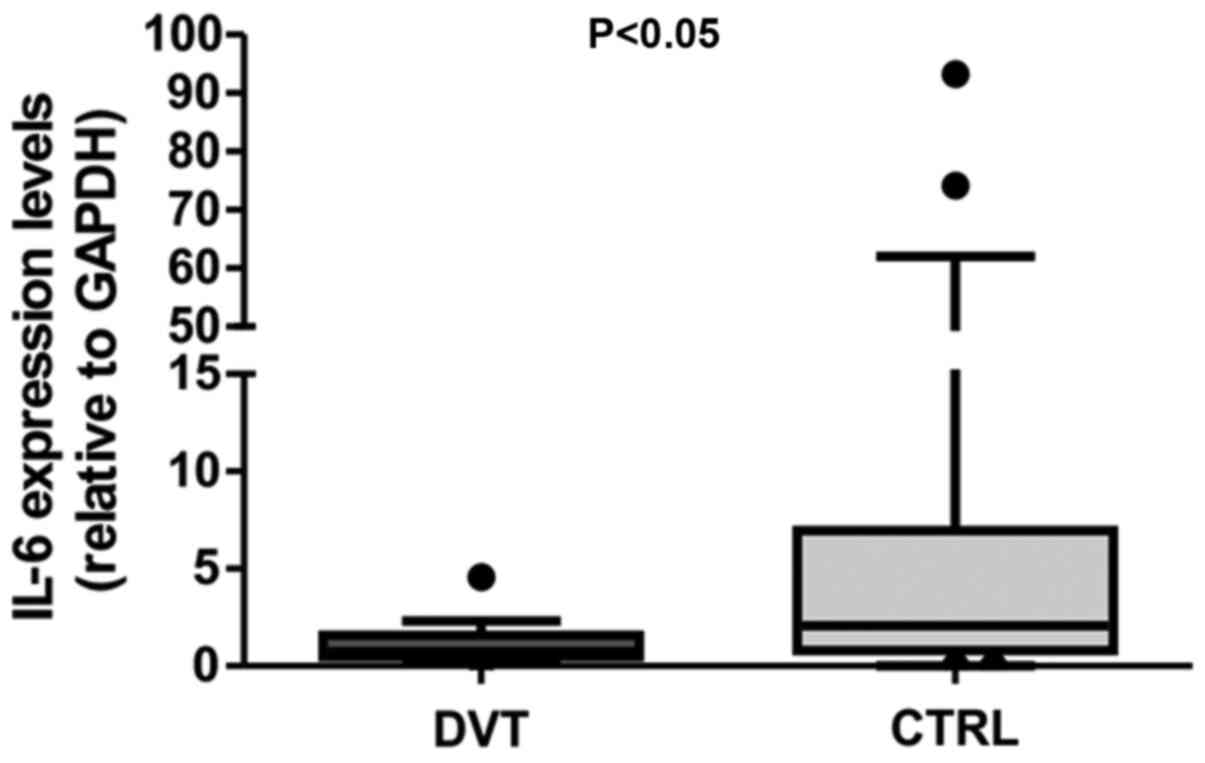
Results of the study showed that IL-6 expression
levels were statistically reduced in the peripheral lymphocytes of
DVT patients compared to controls (fold-change, 2.8; P<0.05)
(Fig. 1). Despite C-reactive
protein (CRP) levels being in the normal range (<15 mg/ml) for
almost all samples, DVT patients showed higher CRP levels compared
to normal samples (P<0.05; Table
I).
Discussion
Traditional knowledge on the pathophysiology of VTE
consists of the three elements of Virchow's triad: endothelial
injury, venous stasis and hypercoagulability (27). More data has been gathered on
extending the pathophysiology of VTE (11). Damaged endothelium expresses
adhesion receptors favoring the recruitment of leukocytes and
platelets. Both bloodstream cell types seem to play a role in VTE
(12,28). Derived leukocyte products are able
to activate coagulative cascade factors (factor X, XII) promoting
intrinsic coagulative pathways. Inflammation correlates with
activated coagulation because it influences the initiation and
propagation of coagulation, it down-regulates physiological
anticoagulant pathways and it inhibits fibrin removal (13). Activated coagulative factors via
protease-activated receptors (PARs) may contribute to endothelial
stress and exposure to adhesion molecules on the disarranged
endothelial barrier leading to inflammation (29).
On VTE pathways, an interesting concept
progressively emerged related to white blood cells (leukocytes and
neutrophils) being rapidly attracted, and retained at the
thrombosis site. Immuno-thrombosis is an interesting interaction
between the innate immune system with the procoagulative condition
(30). In particular, neutrophils
can promote thrombosis by releasing neutrophil extracellular traps
(NETs). NETs show several coagulative properties such as platelet
activation, and fibrin string generation (31), whereas NETs are resistant to
systemic fibrinolysis so they impair thrombus resolution (32,33).
In severe clinical conditions (i.e., acute sepsis), there is
abundant expression of the ILs (e.g., IL-6) with high surface
expression of the tissue factor. The relationship between
inflammation and anti-coagulant balance is well known i.e.
that combined tissue-factor activated factor VII converts factor X
to activated factor, in turn activated factor X generates the
activated factor II (thrombin) of coagulation. Reported evidence on
the relationship between inflammation and the pro-coagulative
activated pathway leads us to the conviction that inflammation must
be considered as one of the most likely risk factors for VTE.
Current approved guidelines for VTE (including DVT) therapy cite
LMWH usage as first line (34).
DOACs were initially approved for VTE prophylaxis in patients with
favorable clinical conditions, to prevent the risk of deterioration
in patients with VTE. Subsequently, DOACs have been also suggested
in treating VTE. To date, DOAC therapy is currently assigned to VTE
patients after discharge in preventing clinical worsening during
follow-up. On the anti-inflammatory response caused by
anti-thrombotic drugs, the anti-inflammatory effects of LMWHs were
recently confirmed by reducing IL-6 and by the increased lymphocyte
percentage found in patients infected by the COVID-19 virus
(35). No specific
anti-inflammatory effects have been reported for DOACs however, it
could be reasonably expected that their potential anti-inflammatory
effects could help in counteracting thrombin generation. In
post-thrombotic syndrome, lower fibrinogen and inflammatory
biomarkers were found in patients assigned to an anti-Xa activated
oral drug (Rivaroxiban) compared to 5-7 days conventional treatment
with LMWH and VKA (36). In
conclusion, our results show lower levels of IL-6 in DVT patients
assigned to DOACs compared to controls. Reduced IL-6 expression in
the lymphocytes of DVT patients may mediate the anti-inflammatory
action of DOACs. Anti-inflammatory activity has yet to be
demonstrated in the LMWHs of patients with high inflammatory levels
affected by acute dramatic thrombotic venous diseases as the
consequence of SARS-CoV-2 infection. To the best of our knowledge,
our study shows the first evidence concerning the anti-inflammatory
properties of DOACs in DVT patients.
In conclusion, anticoagulant drugs such as LMWHs
have demonstrated the direct potential of their anti-inflammatory
capabilities in addition to their anticoagulant properties
(37). Moreover, the involvement of
inflammation in the pathophysiology of the venous thrombotic
process has been clearly established (38). Inflammation is a very interesting
tool for evaluating the potential of the new anti-thrombotic drugs
(DOACs) targeted to inhibite or reduce inflammatory pathways.
Overall, we are confident that these observations will contribute
to clarifying the potential role of DOACs against the high
inflammatory activity that is greatly responsible for favoring
hyper-coagulation and in determining the clinical outcomes for DVT
patients.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
SC, GL, GB, DV, ET, IP, EF, GP, CI, AG and SSS:
substantial contributions to conception and design, acquisition of
data, analysis, and interpretation of data. Drafting the article,
and revising it critically for important intellectual content. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was conducted in accordance with the
Declaration of Helsinki and was approved by the Ethics Committee of
the Garibaldi Hospital (Catania, Italy; resolution
n.23/2016/CECT2). All subjects gave their informed consent for
inclusion before participating in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Mackman N: New insights into the
mechanisms of venous thrombosis. J Clin Invest. 122:2331–2336.
2012.PubMed/NCBI View
Article : Google Scholar
|
|
2
|
Branchford BR and Carpenter SL: The role
of inflammation in venous thromboembolism. Front Pediatr.
6(142)2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Riva N, Donadini MP and Ageno W:
Epidemiology and pathophysiology of venous thromboembolism:
Similarities with atherothrombosis and the role of inflammation.
Thromb Haemost. 113:1176–1183. 2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Prandoni P: Links between arterial and
venous disease. J Intern Med. 262:341–350. 2007.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Smeeth L, Cook C, Thomas S, Hall AJ,
Hubbard R and Vallance P: Risk of deep vein thrombosis and
pulmonary embolism after acute infection in a community setting.
Lancet. 367:1075–1079. 2006.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Tichelaar YI, Kluin-Nelemans HJ and Meijer
K: Infections and inflammatory diseases as risk factors for venous
thrombosis. A systematic review. Thromb Haemost. 107:827–837.
2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Tang N, Li D, Wang X and Sun Z: Abnormal
coagulation parameters are associated with poor prognosis in
patients with novel coronavirus pneumonia. J Thromb Haemost.
18:844–847. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Klok FA, Kruip MJHA, van der Meer NJM,
Arbous MS, Gommers DAMPJ, Kant KM, Kaptein FHJ, van Paassen J,
Stals MAM, Huisman MV, et al: Incidence of thrombotic complications
in critically ill ICU patients with COVID-19. Thromb Res.
191:145–147. 2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Saha P, Humphries J, Modarai B, Mattock K,
Waltham M, Evans CE, Ahmad A, Patel AS, Premaratne S, Lyons OTA, et
al: Leukocytes and the natural history of deep vein thrombosis:
Current concepts and future directions. Arterioscler Thromb Vasc
Biol. 31:506–512. 2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Phillippe HM: Overview of venous
thromboembolism. Am J Manag Care. 23:S376–S382. 2017.PubMed/NCBI
|
|
11
|
Reitsma PH, Versteeg HH and Middeldorp S:
Mechanistic view of risk factors for venous thromboembolism.
Arterioscler Thromb Vasc Biol. 32:563–568. 2012.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Chirinos JA, Heresi GA, Velasquez H, Jy W,
Jimenez JJ, Ahn E, Horstman LL, Soriano AO, Zambrano JP and Ahn YS:
Elevation of endothelial microparticles, platelets, and leukocyte
activation in patients with venous thromboembolism. J Am Coll
Cardiol. 45:1467–1471. 2005.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Levi M, van der Poll T and Büller HR:
Bidirectional relation between inflammation and coagulation.
Circulation. 109:2698–2704. 2004.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Franco RF, de Jonge E, Dekkers PE,
Timmerman JJ, Spek CA, van Deventer SJ, et al: The in vivo kinetics
of tissue factor messenger RNA expression during human endotoxemia:
Relationship with activation of coagulation. Blood. 96:554–559.
2000.PubMed/NCBI
|
|
15
|
Malaponte G, Polesel J, Candido S,
Sambataro D, Bevelacqua V, Anzaldi M, Vella N, Fiore V, Militello
L, Mazzarino MC, et al: IL-6-174 G > C and MMP-9-1562 C > T
polymorphisms are associated with increased risk of deep vein
thrombosis in cancer patients. Cytokine. 62:64–69. 2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Zhang Y, Zhang Z, Wei R, Miao X, Sun S,
Liang G, Chu C, Zhao L, Zhu X, Guo Q, et al: IL (Interleukin)-6
contributes to deep vein thrombosis and is negatively regulated by
miR-338-5p. Arterioscler Thromb Vasc Biol. 40:323–334.
2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Streiff MB, Agnelli G, Connors JM,
Crowther M, Eichinger S, Lopes R, McBane RD, Moll S and Ansell J:
Guidance for the treatment of deep vein thrombosis and pulmonary
embolism. J Thromb Thrombolysis. 41:32–67. 2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Martinelli I, Bucciarelli P and Mannucci
PM: Thrombotic risk factors: Basic pathophysiology. Crit Care Med.
38 (Suppl):S3–S9. 2010.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Shaheen K, Alraies MC, Alraiyes AH,
Christie R and Factor V: Leiden: How great is the risk of venous
thromboembolism? Cleve Clin J Med. 79:265–272. 2012.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Shiqing W, Shengzhong M, Cheng Z,
Guangqing C and Chunzheng G: Efficacy of low molecular weight
heparin in spinal trauma patients after part concentrated screw
surgery and its influence on blood parameters and the incidence of
deep venous thrombosis. Med Hypotheses. 132(109330)2019.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Cirino G, Cicala C, Bucci M, Sorrentino L,
Ambrosini G, DeDominicis G and Altieri DC: Factor Xa as an
interface between coagulation and inflammation. Molecular mimicry
of factor Xa association with effector cell protease receptor-1
induces acute inflammation in vivo. J Clin Invest. 99:2446–2451.
1997.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Borensztajn K, Peppelenbosch MP and Spek
CA: Factor Xa: At the crossroads between coagulation and signaling
in physiology and disease. Trends Mol Med. 14:429–440.
2008.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Bukowska A, Zacharias I, Weinert S, Skopp
K, Hartmann C, Huth C and Goette A: Coagulation factor Xa induces
an inflammatory signalling by activation of protease-activated
receptors in human atrial tissue. Eur J Pharmacol. 718:114–123.
2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Esmon CT: Targeting factor Xa and
thrombin: Impact on coagulation and beyond. Thromb Haemost.
111:625–633. 2014.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kikuchi S, Tsukahara K, Sakamaki K, Morita
Y, Takamura T, Fukui K, Endo T, Shimizu M, Sawada R, Sugano T, et
al: Comparison of anti-inflammatory effects of rivaroxaban vs.
dabigatran in patients with non-valvular atrial fibrillation
(RIVAL-AF study): Multicenter randomized study. Heart Vessels.
34:1002–1013. 2019.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408.
2001.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Kyrle PA and Eichinger S: Deep vein
thrombosis. Lancet. 365:1163–1174. 2005.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Signorelli SS, Malaponte MG, Di Pino L,
Costa MP, Pennisi G and Mazzarino MC: Venous stasis causes release
of interleukin 1beta (IL-1beta), interleukin 6 (IL-6) and tumor
necrosis factor alpha (TNFalpha) by monocyte-macrophage. Clin
Hemorheol Microcirc. 22:311–316. 2000.PubMed/NCBI
|
|
29
|
Kremers BMM, Ten Cate H and Spronk HMH:
Pleiotropic effects of the hemostatic system. J Thromb Haemost.
16:1464–1473. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Brinkmann V: Neutrophil extracellular
traps in the second decade. J Innate Immun. 10:414–421.
2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Fuchs TA, Brill A, Duerschmied D,
Schatzberg D, Monestier M, Myers DD Jr, Wrobleski SK, Wakefield TW,
Hartwig JH and Wagner DD: Extracellular DNA traps promote
thrombosis. Proc Natl Acad Sci USA. 107:15880–15885.
2010.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Brill A, Fuchs TA, Savchenko AS, Thomas
GM, Martinod K, De Meyer SF, Bhandari AA and Wagner DD: Neutrophil
extracellular traps promote deep vein thrombosis in mice. J Thromb
Haemost. 10:136–144. 2012.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Savchenko AS, Martinod K, Seidman MA, Wong
SL, Borissoff JI, Piazza G, Libby P, Goldhaber SZ, Mitchell RN and
Wagner DD: Neutrophil extracellular traps form predominantly during
the organizing stage of human venous thromboembolism development. J
Thromb Haemost. 12:860–870. 2014.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Konstantinides SV, Meyer G, Becattini C,
Bueno H, Geersing GJ, Harjola VP, Huisman MV, Humbert M, Jennings
CS, Jiménez D, et al: 2019 ESC Guidelines for the diagnosis and
management of acute pulmonary embolism developed in collaboration
with the European Respiratory Society (ERS). Eur Heart J.
41:543–603. 2020.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Shi C, Wang C, Wang H, Yang C, Cai F, Zeng
F, Cheng F, Liu Y, Zhou T, Deng B, et al: The potential of low
molecular weight heparin to mitigate cytokine storm in severe
COVID-19 patients: A retrospective cohort study. Clin Transl Sci:
Sep 3, 2020 (Epub ahead of print).
|
|
36
|
Jeraj L, Jezovnik MK and Poredos P:
Rivaroxaban versus warfarin in the prevention of post-thrombotic
syndrome. Thromb Res. 157:46–48. 2017.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Bhalla V, Lamping OF, Abdel-Latif A,
Bhalla M, Ziada K and Smyth SS: Contemporary meta-analysis of
extended direct-acting oral anticoagulant thromboprophylaxis to
prevent venous thromboembolism. Am J Med. 133:1074–1081.e8.
2020.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Borgel D, Bianchini E, Lasne D, Pascreau T
and Saller F: Inflammation in deep vein thrombosis: A therapeutic
target? Hematology. 24:742–750. 2019.PubMed/NCBI View Article : Google Scholar
|