1. Introduction
Severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2) is a novel β-coronavirus, which has caused an ongoing
outbreak of atypical pneumonia worldwide. According to official
data from the World Health Organization (1), by October 7, 2020, >35,347,404
people have been affected by the SARS-CoV-2, and >1,039,406
patients had succumbed to the disease. A number of countries have
required that residents reduce social activities and
self-quarantine to limit the spread of coronavirus disease 2019
(COVID-19), which has caused major changes and disruptions to daily
life, including work, school, sports, events and social activities
(2,3). During the mandatory isolation, it is
crucial to maintain mental and physical health through physical
exercise (4,5). The clinical manifestations of COVID-19
are non-specific and range from asymptomatic infection to severe
respiratory failure. The most common symptoms of COVID-19 include
cough, fever and dyspnea (6).
Elderly individuals and those with underlying conditions, such as
cardiovascular and lung diseases, may suffer from more severe
symptoms and mortality (7). Obesity
has also been identified as a risk factor for the disease (8). Environmental factors, social customs
and epidemic-specific attitudes, administrative issues and other
factors will all have a major impact on the prevalence of
COVID-19(9).
The pathogen of COVID-19, SARS-CoV-2, is a
positive-sense single-stranded RNA virus of the β-coronavirus genus
(10,11). SARS-CoV-2 has been demonstrated to
have a spherical morphology with spike projections on the surface
(12), and it shares a high
sequence identity with severe acute respiratory syndrome
coronavirus (SARS-CoV) (13). The
spike S glycoprotein serves a major role in viral infections and is
one of the main targets in the design of therapeutic drugs and
vaccines (14). At present there is
no specific therapeutic drug or vaccine for SARS-CoV-2(15), so the drugs currently used are aimed
at suppressing inflammation or improving symptoms. Some antiviral
drugs appear to serve a positive role in treating COVID-19,
particularly at the early phase, such as interferon, lopinavir,
chloroquine/hydroxychloroquine and ribavirin (16). Traditional Chinese medicines,
including Lianhuaqingwen, have also demonstrated beneficial
outcomes when used to treat cases with mild symptoms (17). However, further clinical trials of
drugs and vaccines for SARS-CoV-2 are required to assess their
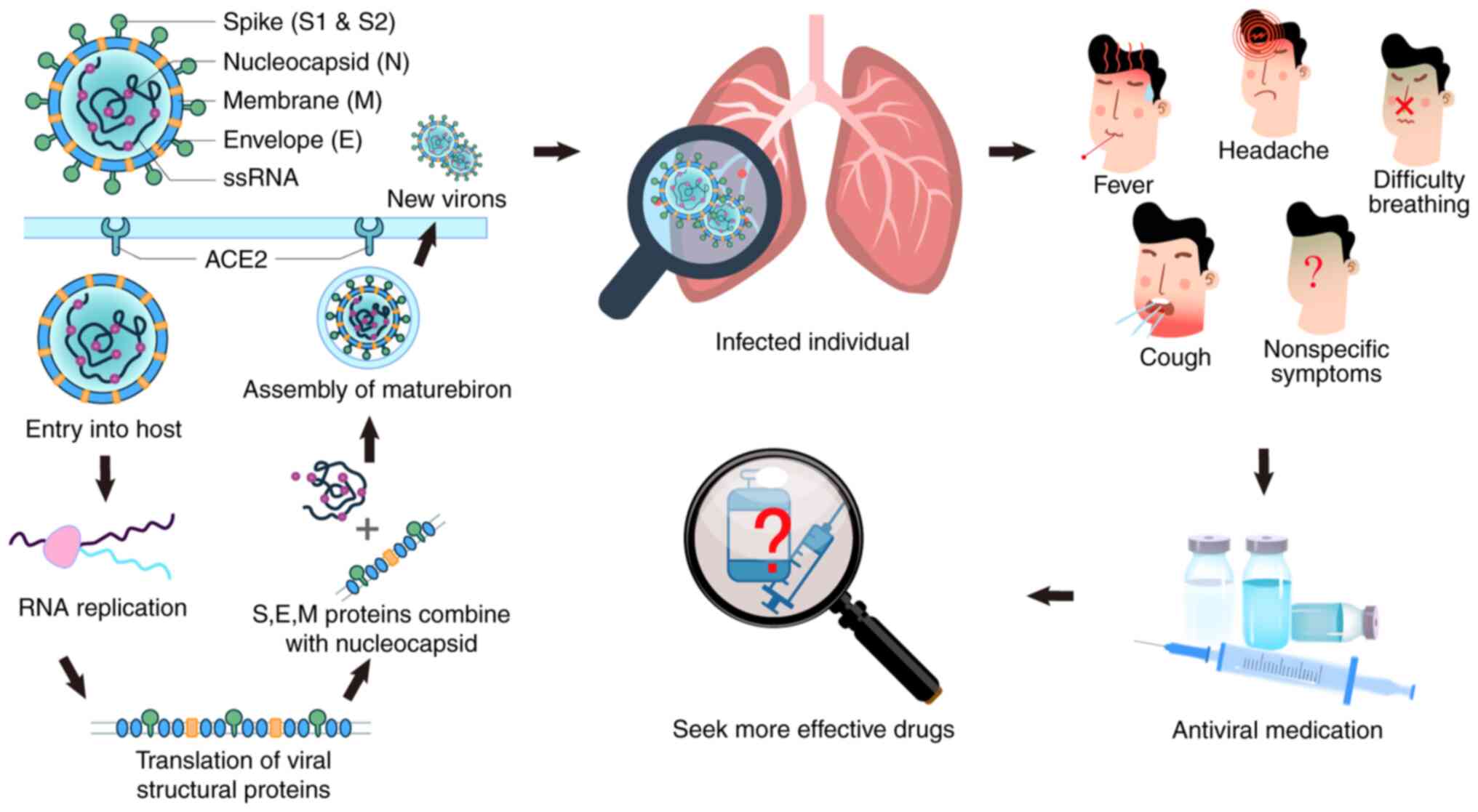
efficacy and safety. Fig. 1
presents the SARS-CoV-2 infection. SARS-CoV-2 can enter the host
cell through the angiotensin-converting enzyme 2 (ACE2) site.
Infected individuals usually exhibit non-specific symptoms such as
a cough and fever. Clinically, antiviral drugs are usually used for
treatment, but there are no specific drugs and vaccines that are
used.
Lactoferrin (LF), which is an iron-binding
glycoprotein with a molecular weight in the range of 70-80 kDa, can
transport iron in the blood and serum (18). LF is a simple polypeptide chain that
is assembled into two symmetrical lobes (19). Each lobe contains two domains, which
can bind a metal atom. It has been previously reported that the
antiviral effect of LF is mediated by binding iron and is not
affected by unsaturated iron levels (20). According to the available
literature, the sequences and structures of LF from different
sources (including from human, bovine and camel) are similar,
except the N-terminal part of camel LF, as the first 50 residues of
the N-terminus of camel LF shares less than 40% sequence identity1
with other sources of lactoferrin (21,22).
LF is produced by mucosal epithelial cells in a number of different
mammalian and fish species, and is found in mucosal secretions,
bodily fluids and secondary neutrophil granules (23).
After LF is successfully isolated and purified, a
number of its physiological activities have been gradually
uncovered, including antifungal, antiviral and anti-inflammatory
activities, as well as effects on the immune response (18,24,25).
These activities are mediated through the capacity of LF to bind
iron and to interact with components of the host and the pathogens
(23). LF is positively charged
in vivo, and can bind large molecules with negative charges,
such as lipopolysaccharides and glycosaminoglycans, which is one of
the key mechanisms underlying its antiviral activity (26). The protective effects of LF were
first confirmed in 1987 in mice infected with the
polycythemia-inducing strain of friend virus complex (27). LF has been identified to be
effective against several viruses, which are listed in Table I (28-37).
 | Table IThe antivirus activities of LF for
some viruses. |
Table I
The antivirus activities of LF for
some viruses.
| Authors, year | Type of virus |
Enveloped/naked | DNA/RNA | Sources of LF | Mechanism | (Refs.) |
|---|
| Oda et al,
2020 | Influenza A | Enveloped | RNA | Bovine | Interfering with
the fusogenic function of viral hemagglutinin | (28) |
| Sano et al,
2003 | RSV | Enveloped | RNA | Human | Modulating
RSV-induced IL-8 secretion and binding to RSV F protein | (29) |
| Pietrantoni et
al, 2003 | Adenovirus | Naked | DNA | Bovine | Binding to the
adenovirus penton base and competing with viral particles for cell
membrane HS inserted in target cell membranes | (30) |
| Lang et al,
2011 | SARS-CoV | Enveloped | RNA | Bovine | Enhancing Natural
killer cell activity and stimulating neutrophil aggregation and
adhesion, binding to the heparan sulfate glycosaminoglycan (HSPG)
and blocking the preliminary interaction between SARS-CoV and host
cells | (31) |
| Chen et al,
2017 | Dengue Virus | Enveloped | RNA | Bovine | Interacting with
Heparan Sulfate, Low-Density Lipoprotein Receptor and DC-SIGN | (32) |
| Weng et al,
2005 | Enterovirus 71 | Naked | RNA | Bovine | Binding to viral
protein 1 protein and host cells | (33) |
| Pietrantoni et
al, 2015 | Toscana Virus | Enveloped | RNA | Bovine | Binding to Heparan
Sulphate | (34) |
| Beljaars et
al, 2004 | CMV | Enveloped | DNA | Human | Inhibition of CMV
cell entry and indirect activities of lactoferrin on CMV infections
via stimulation of the immune system | (35) |
| Ammendolia et
al, 2007 | Herpes Simplex
Virus type 1 (HSV-1) | Enveloped | DNA | Bovine | Competing with
HSV-1 for heparan sulphate receptor on cell surface and affecting a
post-entry step of viral infection by preventing VP-16 from being
translocated to the nucleus | (36) |
| Ishikawa et
al, 2013 | MNV | Naked | RNA | Bovine | Inducing the
expression of anti-viral cytokine mRNA, such as IFN-a and IFN-b,
which are involved in the inhibition of MNV replication in the
early phase of infection | (37) |
COVID-19 is often characterized by an unusually long
asymptomatic stage (3-14 days), while asymptomatic patients may be
equally, if not more, contagious compared with symptomatic
patients, which makes prevention extremely difficult, particularly
during the flu season (38). The
mechanism behind the asymptomatic stage may involve the fact that
SARS-CoV-2 has developed an additional furin protease cleavage site
in the spike protein (between the S1 and S2 domains), which enables
the virus to infect and proliferate in large quantities in the
nostril, salivary glands and throat, where furin protease and ACE2
are both expressed at high levels (39). Over a period of time, the virus
proliferating in the upper respiratory tract can migrate to the
lower respiratory tract and infect others via fluid droplets. If
prophylactic measures are taken in time to reduce the virus load
and/or prevent infection of other cells, the interpersonal
infectivity and severity of later symptoms may be markedly
reduced.
From the perspective of the SARS-CoV-2 infection
process, preventing viral particles from entering the cells and
interfering with endocytic pathways, preventing post-translational
processing of multiple proteins, and targeting cell signaling
pathways, are some of the approaches that can be used to identify
effective therapies (11). In
addition, due to the similarities between SARS-CoV-2 and SARS-CoV,
drugs that have a therapeutic effect against SARS-CoV may also be
considered as a possible treatment plan. The antiviral effect of LF
is mediated through preventing the virus from binding to the target
cell surface, which would be particularly effective during the
early amplification phase of the virus in the salivary glands,
throat and upper respiratory tract (40). LF has strong and extensive antivirus
properties and therefore, it can be hypothesized the LF may be used
as a potential drug for the treatment of COVID-19.
2. Two-stage interaction with receptors on
host cells
To achieve infection, the virus must first attach to
the host cell and then penetrate the cell membrane. There is a
highly alkaline region near the N-terminal of LF, which may be
combined with a variety of negatively charged macromolecules
(41). This is an important basis
for the antiviral activity of LF, as a variety of negatively
charged macromolecules, such as glycosaminoglycans, often act as
receptors on the surface of host cells that combine with viruses
(42,43). It has been demonstrated that heparan
sulfate proteoglycans (HSPGs) serve important roles in inhibiting
human respiratory syncytial virus, Venezuelan equine encephalitis
virus (44), Echovirus (45), herpes simplex virus (HSV), dengue
virus (43) as well as other
viruses (46).
Novel coronavirus is the pathogen of SARS. Its high
infectivity, high mortality and low cure rates make it a major
threat to public health (47).
SARS-CoV is an enveloped, positive-strand RNA virus, composed of
spike, envelope, membrane and nucleocapsid protein (48). SARS-CoV attaches to host cells by
binding HSPGs (49), which are also
the binding sites for LF on host cells (50). It has been demonstrated that LF can
protect the host against a variety of viral infections by
preventing the internalization of viruses, such as HSV, and by
occupying their binding sites (51). The protective effects of LF against
SARS-CoV Pseudovirus infection of 293E/ACE2-Myc cells has been
investigated (31). It has also
been demonstrated that HSPGs (binding sites facilitating SARS-CoV
entry) are distributed on the host cell surface and LF occupies
these binding sites to prevent the internalization of SARS-CoV and
infection of host cells in the early stages. Therefore, LF may be
useful as a potential therapeutic drug candidate for protecting
host cells against SARS-CoV infections.
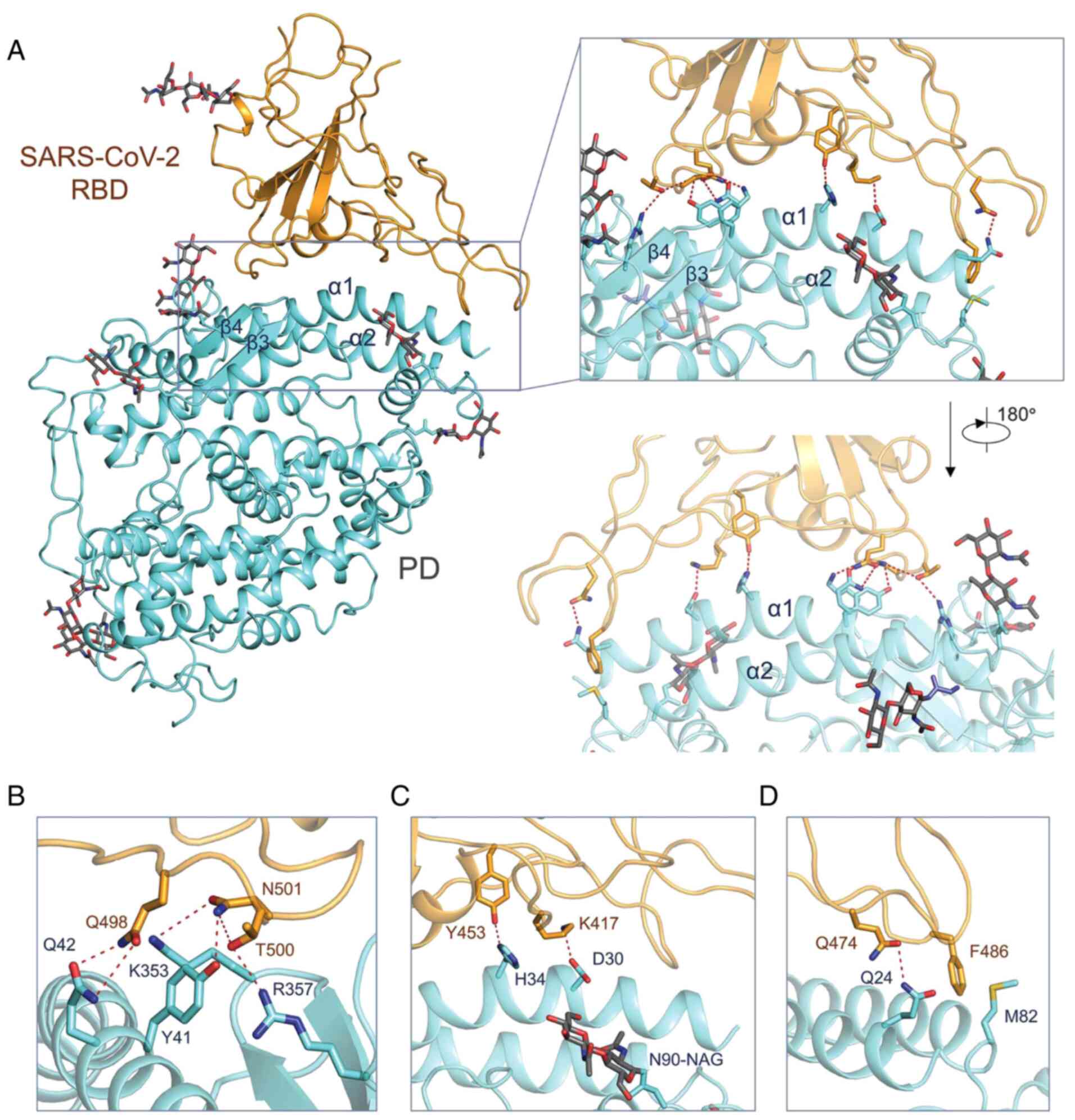
SARS-CoV-2 shares ~80% identity of the genome,
similar receptor-binding domain (RBD) structures and cellular
receptors (such as ACE2) with SARS-CoV (Fig. 2), and the α1 helix of the RBD binds
to the peptidase domain (PD) of ACE2 via polar action (52). ACE2 has been demonstrated to be the
primary receptor, while dendritic cell-specific intercellular
adhesion molecule 3-grabbing non-integrin (DC-SIGN) is another
controversial independent receptor of SARS-CoV-2 (53,54).
DC-SIGN may be a factor that promotes ACE2-mediated infection
(55). Although, to the best of our
knowledge, there are no studies demonstrating that LF can protect
host cells by binding to ACE2, it has been demonstrated that LF can
protect the host cell against dengue virus infection via binding to
sites on the cell membrane, including DC-SIGN, heparan sulfate (HS)
and low-density lipoprotein receptors (32). Therefore, it may be hypothesized
that LF can also inhibit ACE2-mediated infection by binding to
DC-SIGN. Fig. 2 presents the
interactions between SARS-CoV-2-RBD and ACE2(52).
In addition, it has been demonstrated that ACE2 is
also abundantly expressed in gastrointestinal epithelial cells
(56,57). Therefore, host cell internalization
of SARS-CoV-2 may be identified in the gastrointestinal tract, and
can lead to active infection and replication (13). Following oral administration,
abundant LF remains on the lining of the gastrointestinal tract and
protects host cells against infection by SARS-CoV-2(18).
3. Immunomodulatory effects of LF
In addition to its interaction with host cells, LF
can also enhance antiviral protection by modulating the immune
response, such as enhancing phagocytosis and inducing apoptosis,
among other functions (58). The
immunomodulatory effects of LF have attracted attention as LF
defends against infection and excessive inflammation, which is
achieved through interaction with immune cells and cytokines
(59). The immunomodulatory effects
include i) enhancing the antigen expression ability of B cells and
ii) regulating the function of T cells (60).
LF receptors (LFRs) are located on the surface of a
variety of immune cells, such as various lymphocytes, macrophages
and dendritic cells (61,62). LF can reduce the release of
inflammatory factors by promoting the differentiation of
CD4+ T cells into Th1 cells (63). In addition, LF can stimulate
neutrophil aggregation at the site of inflammation, activate
phagocytosis by polymorphonuclear leukocytes and macrophagocytes,
and increase the activity of natural killer (NK) cells. Oral
administration of LF can enhance the killing activity of NK cells
against tumor and virus-infected cells by facilitating the
production of interleukin (IL)-18(64). Furthermore, LF can increase the
level of IL-12 in macrophagocytes, which triggers the migration of
macrophages to inflammatory sites and activates CD4+ T
cells (59). On the other hand,
cytokines are important for the immunomodulatory effects of LF. LF
induces the expression of type I interferons (IFN-α/β) and inhibits
virus replication (58). IFN-α/β
are known as potent antiviral cytokines and immunomodulators, which
lead to the production of numerous antiviral bioactive compounds
and cytokines (65). In summary, LF
may be used as a natural immunomodulator for the treatment of
COVID-19(66).
4. Fusion between LF and the viral
envelope
The virus infects host cells through fusion of its
envelope with the host cell membrane, which is a key step during
viral infection. It has been demonstrated that LF binds to the
substances mediating the infection process on the virus envelope
and inhibits fusion, thus preventing infection (67). The binding sites differ among
different viruses. Hemagglutinin (HA) is the binding site on the
H1N1 virus, and LF has been demonstrated to inhibit infection via
fusion with HA (28). HA, which is
a glycoprotein expressed in the virus envelope, is a key factor in
the process of viral infection. Following LF binding to HA, the
interaction and fusion between the glycoprotein on the virus
surface and receptors on the host cell are inhibited, thereby
preventing infection. In addition, LF inhibits respiratory
syncytial virus (RSV), which is associated with a serious
respiratory disease such as otitis media and lower respiratory
tract involvement (LRTI) in infants (68), through fusion with the F protein on
the virus envelope (27). LF binds
to the F1 subunit of the F protein, thereby inhibiting the entry of
RSV into epithelial cells, preventing the inflammatory response
caused by RSV, and decreasing the infection of Hep-2 cells. LF
protects the host cell against infection by adenovirus by
specifically binding to its penton base (23). Overall, the protective activity of
LF against viral infections is notable. However, whether LF is also
effective in SARS-CoV-2 must be further investigated, and it is
necessary to identify the binding sites on SARS-CoV-2.
5. Discussion and conclusion
The rapid spread of the SARS-CoV-2 pandemic has
become a major global health concern. It is therefore urgent to
develop effective therapeutic agents to prevent and treat
SARS-CoV-2 infection. LF has exhibited extensive, broad-spectrum
antiviral activity, indicating its potential for the treatment and
prevention of SARS-CoV-2 (21,40).
For example, LF treatment on HSPGs and ACE2 can prevent SARS-CoV
from infecting host cells (31),
and LF has extensive immunoregulatory and anti-inflammatory effects
(69,70), which may prove useful in the
treatment of SARS-CoV-2 and the prevention of its devastating
effects on multiple target organs. Furthermore, compared with other
antiviral drugs, LF has a better safety profile. The use of LF may
therefore hold promise in the treatment of COVID-19 and warrants
further investigation.
However, there were certain limitations to the
current review. The aforementioned possible effects of LF on
SARS-CoV-2 are based on the effects of LF on other viruses, and
there is currently a lack of direct research on the effects of LF
on SARS-CoV-2. In addition, there remains certain problems in
applying LF in the clinical setting. For example, it remains
unknown which state of LF is more effective in treating SARS-CoV-2,
namely unsaturated vs. saturated, human-derived vs. bovine-derived,
whereas the combined metal, specific dosage and route of
administration have yet to be clearly determined, and these issues
must be considered and resolved before applying LF in the clinical
setting for the treatment of COVID-19.
In conclusion, the use of LF appears to be a
promising approach to the treatment of COVID-19, but further
investigations are required to verify its antiviral activity in
vitro and in vivo.
Acknowledgements
Not applicable.
Funding
Liaoning Province Natural Science Foundation of
China (grant no. 2020-BS-106).
Availability of data and materials
Not applicable.
Authors' contributions
YC, HW and MJ conceptualized the study. YW, PW, HW,
YL, LW performed validation, research and reviewed the data. YW and
PW wrote the manuscript. YW, PW, YC and MJ reviewed the manuscript.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
World Health Organization (WHO): WHO
Coronavirus Disease (COVID-19) Dashboard. WHO, Geneva, 2020.
urihttps://covid19.who.int/.Accessedsimplehttps://covid19.who.int/.Accessed
October 7, 2020.
|
|
2
|
Giustino V, Parroco AM, Gennaro A,
Musumeci G, Palma A and Battaglia G: Physical activity levels and
related energy expenditure during COVID-19 quarantine among the
Sicilian active population: A Cross-Sectional Online Survey Study.
Sustainability. 12(4356)2020.
|
|
3
|
Paoli A and Musumeci G: Elite Athletes and
COVID-19 lockdown: Future health concerns for an entire sector. J
Funct Morphol Kinesiol. 5(30)2020.
|
|
4
|
Maugeri G, Castrogiovanni P, Battaglia G,
Pippi R, D'Agata V, Palma A, Di Rosa M and Musumeci G: The impact
of physical activity on psychological health during Covid-19
pandemic in Italy. Heliyon. 6(e04315)2020.
|
|
5
|
Ravalli S and Musumeci G: Coronavirus
Outbreak in Italy: Physiological benefits of home-based exercise
during pandemic. J Funct Morphol Kinesiol. 5(31)2020.
|
|
6
|
Zhai P, Ding Y, Wu X, Long J, Zhong Y and
Li Y: The epidemiology, diagnosis and treatment of COVID-19. Int J
Antimicrob Agents. 55(105955)2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Chen N, Zhou M, Dong X, Qu J, Gong F, Han
Y, Qiu Y, Wang J, Liu Y, Wei Y, et al: Epidemiological and clinical
characteristics of 99 cases of 2019 novel coronavirus pneumonia in
Wuhan, China: A descriptive study. Lancet. 395:507–513.
2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Petrakis D, Margină D, Tsarouhas K, Tekos
F, Stan M, Nikitovic D, Kouretas D, Spandidos DA and Tsatsakis A:
Obesity-a risk factor for increased COVID-19 prevalence, severity
and lethality. Mol Med Rep. 22:9–19. 2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Goumenou M, Sarigiannis D, Tsatsakis A,
Anesti O, Docea AO, Petrakis D, Tsoukalas D, Kostoff R, Rakitskii
V, Spandidos DA, et al: COVID-19 in Northern Italy: An integrative
overview of factors possibly influencing the sharp increase of the
outbreak (Review). Mol Med Rep. 22:20–32. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Lai CC, Shih TP, Ko WC, Tang HJ and Hsueh
PR: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
and coronavirus disease-2019 (COVID-19): The epidemic and the
challenges. Int J Antimicrob Agents. 55(105924)2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Nitulescu GM, Paunescu H, Moschos SA,
Petrakis D, Nitulescu G, Ion GND, Spandidos DA, Nikolouzakis TK,
Drakoulis N and Tsatsakis A: Comprehensive analysis of drugs to
treat SARS-CoV-2 infection: Mechanistic insights into current
COVID-19 therapies (Review). Int J Mol Med. 46:467–488.
2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Li H, Zhou Y, Zhang M, Wang H, Zhao Q and
Liu J: Updated approaches against SARS-CoV-2. Antimicrob Agents
Chemother. 64:e00483–20. 2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Yeo C, Kaushal S and Yeo D: Enteric
involvement of coronaviruses: Is faecal-oral transmission of
SARS-CoV-2 possible? Lancet Gastroenterol Hepatol. 5:335–337.
2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Dehelean CA, Lazureanu V, Coricovac D,
Mioc M, Oancea R, Marcovici I, Pinzaru I, Soica C, Tsatsakis AM and
Cretu O: SARS-CoV-2: Repurposed drugs and novel therapeutic
approaches-insights into chemical structure-biological activity and
toxicological screening. J Clin Med. 9(2084)2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Calina D, Docea AO, Petrakis D, Egorov AM,
Ishmukhametov AA, Gabibov AG, Shtilman MI, Kostoff R, Carvalho F,
Vinceti M, et al: Towards effective COVID-19 vaccines: Updates,
perspectives and challenges (Review). Int J Mol Med. 46:3–16.
2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ren J, Zhang AH and Wang XJ: Traditional
Chinese medicine for COVID-19 treatment. Pharmacol Res.
155(104743)2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Runfeng L, Yunlong H, Jicheng H, Weiqi P,
Qinhai M, Yongxia S, Chufang L, Jin Z, Zhenhua J, Haiming J, et al:
Lianhuaqingwen exerts anti-viral and anti-inflammatory activity
against novel coronavirus (SARS-CoV-2). Pharmacol Res.
156(104761)2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Wang B, Timilsena YP, Blanch E and
Adhikari B: Lactoferrin: Structure, function, denaturation and
digestion. Crit Rev Food Sci Nutr. 59:580–596. 2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Baveye S, Elass E, Mazurier J, Spik G and
Legrand D: Lactoferrin: A multifunctional glycoprotein involved in
the modulation of the inflammatory process. Clin Chem Lab Med.
37:281–286. 1999.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lönnerdal B and Iyer S: Lactoferrin:
Molecular structure and biological function. Annu Rev Nutr.
15:93–110. 1995.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Redwan EM, Uversky VN, El-Fakharany EM and
Al-Mehdar H: Potential lactoferrin activity against pathogenic
viruses. C R Biol. 337:581–595. 2014.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Khan JA, Kumar P, Paramasivam M, Yadav RS,
Sahani MS, Sharma S, Srinivasan A and Singh TP: Camel lactoferrin,
a transferrin-cum-lactoferrin: Crystal structure of camel
apolactoferrin at 2.6 A resolution and structural basis of its dual
role. J Mol Biol. 309:751–761. 2001.PubMed/NCBI View Article : Google Scholar
|
|
23
|
González-Chávez SA, Arévalo-Gallegos S and
Rascón-Cruz Q: Lactoferrin: Structure, function and applications.
Int J Antimicrob Agents. 33:301.e1–e8. 2009.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Moreno-Expósito L, Illescas-Montes R,
Melguizo-Rodríguez L, Ruiz C, Ramos-Torrecillas J and de
Luna-Bertos E: Multifunctional capacity and therapeutic potential
of lactoferrin. Life Sci. 195:61–64. 2018.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Hao L, Shan Q, Wei J, Ma F and Sun P:
Lactoferrin: Major physiological functions and applications. Curr
Protein Pept Sci. 20:139–144. 2019.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Elass-Rochard E, Legrand D, Salmon V,
Roseanu A, Trif M, Tobias PS, Mazurier J and Spik G: Lactoferrin
inhibits the endotoxin interaction with CD14 by competition with
the lipopolysaccharide-binding protein. Infect Immun. 66:486–491.
1998.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Lu L, Hangoc G, Oliff A, Chen LT, Shen RN
and Broxmeyer HE: Protective influence of lactoferrin on mice
infected with the polycythemia-inducing strain of friend virus
complex. Cancer Res. 47:4184–4188. 1987.PubMed/NCBI
|
|
28
|
Oda H, Wakabayashi H, Tanaka M, Yamauchi
K, Sugita C, Yoshida H, Abe F, Sonoda T and Kurokawa M: Effects of
lactoferrin on infectious diseases in Japanese summer: A
randomized, double-blinded, placebo-controlled trial. J Microbiol
Immunol Infect, Feb 26, 2020 (Online ahead of print).
|
|
29
|
Sano H, Nagai K, Tsutsumi H and Kuroki Y:
Lactoferrin and surfactant protein A exhibit distinct binding
specificity to F protein and differently modulate respiratory
syncytial virus infection. Eur J Immunol. 33:2894–2902.
2003.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Pietrantoni A, Di Biase AM, Tinari A,
Marchetti M, Valenti P, Seganti L and Superti F: Bovine lactoferrin
inhibits adenovirus infection by interacting with viral structural
polypeptides. Antimicrob Agents Chemother. 47:2688–2691.
2003.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Lang J, Yang N, Deng J, Liu K, Yang P,
Zhang G and Jiang C: Inhibition of SARS pseudovirus cell entry by
lactoferrin binding to heparan sulfate proteoglycans. PLoS One.
6(e23710)2011.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Chen JM, Fan YC, Lin JW, Chen YY, Hsu WL
and Chiou SS: Bovine lactoferrin inhibits dengue virus infectivity
by interacting with heparan sulfate, low-density lipoprotein
receptor, and DC-SIGN. Int J Mol Sci. 18(1957)2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Weng TY, Chen LC, Shyu HW, Chen SH, Wang
JR, Yu CK, Lei HY and Yeh TM: Lactoferrin inhibits enterovirus 71
infection by binding to VP1 protein and host cells. Antiviral Res.
67:31–37. 2005.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Pietrantoni A, Fortuna C, Remoli ME,
Ciufolini ME and Superti F: Bovine lactoferrin inhibits Toscana
virus infection by binding to heparan sulphate. Viruses. 7:480–495.
2015.PubMed/NCBI View
Article : Google Scholar
|
|
35
|
Beljaars L, van der Strate BW, Bakker HI,
Reker-Smit C, van Loenen-Weemaes AM, Wiegmans FC, Harmsen MC,
Molema G and Meijer DK: Inhibition of cytomegalovirus infection by
lactoferrin in vitro and in vivo. Antiviral Res. 63:197–208.
2004.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Ammendolia MG, Marchetti M and Superti F:
Bovine lactoferrin prevents the entry and intercellular spread of
herpes simplex virus type 1 in green Monkey kidney cells. Antiviral
Res. 76:252–262. 2007.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Ishikawa H, Awano N, Fukui T, Sasaki H and
Kyuwa S: The protective effects of lactoferrin against murine
norovirus infection through inhibition of both viral attachment and
replication. Biochem Biophys Res Commun. 434:791–796.
2013.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Vellingiri B, Jayaramayya K, Iyer M,
Narayanasamy A, Govindasamy V, Giridharan B, Ganesan S, Venugopal
A, Venkatesan D, Ganesan H, et al: COVID-19: A promising cure for
the global panic. Sci Total Environ. 725(138277)2020.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Lan J, Ge J, Yu J, Shan S, Zhou H, Fan S,
Zhang Q, Shi X, Wang Q, Zhang L and Wang X: Structure of the
SARS-CoV-2 spike receptor-binding domain bound to the ACE2
receptor. Nature. 581:215–220. 2020.PubMed/NCBI View Article : Google Scholar
|
|
40
|
van der Strate BW, Beljaars L, Molema G,
Harmsen MC and Meijer DK: Antiviral activities of lactoferrin.
Antiviral Res. 52:225–239. 2001.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Baker EN and Baker HM: Molecular
structure, binding properties and dynamics of lactoferrin. Cell Mol
Life Sci. 62:2531–2539. 2005.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Kamhi E, Joo EJ, Dordick JS and Linhardt
RJ: Glycosaminoglycans in infectious disease. Biol Rev Camb Philos
Soc. 88:928–943. 2013.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Cagno V, Tseligka ED, Jones ST and
Tapparel C: Heparan sulfate proteoglycans and viral attachment:
True receptors or adaptation bias? Viruses. 11(596)2019.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Bernard KA, Klimstra WB and Johnston RE:
Mutations in the E2 glycoprotein of Venezuelan equine encephalitis
virus confer heparan sulfate interaction, low morbidity, and rapid
clearance from blood of mice. Virology. 276:93–103. 2000.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Goodfellow IG, Sioofy AB, Powell RM and
Evans DJ: Echoviruses bind heparan sulfate at the cell surface. J
Virol. 75:4918–4921. 2001.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Li P, Sheng J, Liu Y, Li J, Liu J and Wang
F: Heparosan-derived heparan sulfate/heparin-like compounds: One
kind of potential therapeutic agents. Med Res Rev. 33:665–692.
2013.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Zheng J: SARS-CoV-2: An emerging
coronavirus that causes a global threat. Int J Biol Sci.
16:1678–1685. 2020.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Bartlam M, Yang H and Rao Z: Structural
insights into SARS coronavirus proteins. Curr Opin Struct Biol.
15:664–672. 2005.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Belting M: Heparan sulfate proteoglycan as
a plasma membrane carrier. Trends Biochem Sci. 28:145–151.
2003.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Carvalho CAM, Sousa IP Jr, Silva JL,
Oliveira AC, Gonçalves RB and Gomes AMO: Inhibition of Mayaro virus
infection by bovine lactoferrin. Virology. 452-453:297–302.
2014.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Jenssen H and Hancock RE: Antimicrobial
properties of lactoferrin. Biochimie. 91:19–29. 2009.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Yan R, Zhang Y, Li Y, Xia L, Guo Y and
Zhou Q: Structural basis for the recognition of SARS-CoV-2 by
full-length human ACE2. Science. 367:1444–1448. 2020.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Gao C, Zeng J, Jia N, Stavenhagen K,
Matsumoto Y, Zhang H, Li J, Hume AJ, Mühlberger E, van Die I, et
al: SARS-CoV-2 spike protein interacts with multiple innate
immune receptors. bioRxiv: 2020.07.29.227462, 2020.
|
|
54
|
Brufsky A and Lotze MT: DC/L-SIGNs of hope
in the COVID-19 pandemic. J Med Virol, May 6, 2020 (Online ahead of
print).
|
|
55
|
Han DP, Lohani M and Cho MW: Specific
asparagine-linked glycosylation sites are critical for DC-SIGN- and
L-SIGN-mediated severe acute respiratory syndrome coronavirus
entry. J Virol. 81:12029–12039. 2007.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Ahlawat S and Asha Sharma KK:
Immunological co-ordination between gut and lungs in SARS-CoV-2
infection. Virus Res. 286(198103)2020.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Dai YJ, Hu F, Li H, Huang HY, Wang DW and
Liang Y: A profiling analysis on the receptor ACE2 expression
reveals the potential risk of different type of cancers vulnerable
to SARS-CoV-2 infection. Ann Transl Med. 8(481)2020.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Puddu P, Carollo MG, Belardelli F, Valenti
P and Gessani S: Role of endogenous interferon and LPS in the
immunomodulatory effects of bovine lactoferrin in murine peritoneal
macrophages. J Leukoc Biol. 82:347–353. 2007.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Puddu P, Valenti P and Gessani S:
Immunomodulatory effects of lactoferrin on antigen presenting
cells. Biochimie. 91:11–18. 2009.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Siqueiros-Cendón T, Arévalo-Gallegos S,
Iglesias-Figueroa BF, García-Montoya IA, Salazar-Martínez J and
Rascón-Cruz Q: Immunomodulatory effects of lactoferrin. Acta
Pharmacol Sin. 35:557–566. 2014.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Actor JK, Hwang SA and Kruzel ML:
Lactoferrin as a natural immune modulator. Curr Pharm Des.
15:1956–1973. 2009.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Liu KY, Comstock SS, Shunk JM, Monaco MH
and Donovan SM: Natural killer cell populations and cytotoxic
activity in pigs fed mother's milk, formula, or formula
supplemented with bovine lactoferrin. Pediatr Res. 74:402–407.
2013.PubMed/NCBI View Article : Google Scholar
|
|
63
|
MacManus CF, Collins CB, Nguyen TT, Alfano
RW, Jedlicka P and de Zoeten EF: VEN-120, a recombinant human
lactoferrin, promotes a regulatory T cell [Treg] phenotype and
drives resolution of inflammation in distinct murine models of
inflammatory bowel disease. J Crohns Colitis. 11:1101–1112.
2017.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Kuhara T, Yamauchi K, Tamura Y and Okamura
H: Oral administration of lactoferrin increases NK cell activity in
mice via increased production of IL-18 and type I IFN in the small
intestine. J Interferon Cytokine Res. 26:489–499. 2006.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Haller O, Kochs G and Weber F: The
interferon response circuit: Induction and suppression by
pathogenic viruses. Virology. 344:119–130. 2006.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Legrand D: Overview of lactoferrin as a
natural immune modulator. J Pediatr. 173 (Suppl):S10–S15.
2016.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Wakabayashi H, Oda H, Yamauchi K and Abe
F: Lactoferrin for prevention of common viral infections. J Infect
Chemother. 20:666–671. 2014.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Borchers AT, Chang C, Gershwin ME and
Gershwin LJ: Respiratory syncytial virus-a comprehensive review.
Clin Rev Allergy Immunol. 45:331–379. 2013.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Berlutti F, Pantanella F, Natalizi T,
Frioni A, Paesano R, Polimeni A and Valenti P: Antiviral properties
of lactoferrin-a natural immunity molecule. Molecules.
16:6992–7018. 2011.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Legrand D, Elass E, Carpentier M and
Mazurier J: Lactoferrin: A modulator of immune and inflammatory
responses. Cell Mol Life Sci. 62:2549–2559. 2005.PubMed/NCBI View Article : Google Scholar
|