Introduction
Chronic obstructive pulmonary disease (COPD) affects
>65 million individuals worldwide and is to become the third
most common cause of death worldwide by the year 2030(1). The disease is characterized by
limitation of airflow and arises from an abnormal inflammatory
response of the lungs to noxious gas particles (2). COPD is also a major risk factor for
the development of nosocomial lower respiratory tract infections,
as the patient's immune system may be weakened by prolonged
corticosteroid use and reduced microbial clearance (3). During the natural course of the
disease, exacerbations and infections are common in patients with
COPD, the management of which requires assisted ventilation and
hospitalization (4).
Patients requiring prolonged duration of mechanical
ventilation in the intensive care unit (ICU) have a particular risk
of developing ventilator-associated pneumonia (VAP) (5). An estimated 10-20% of patients
receiving mechanical ventilation for >24 h are diagnosed with
VAP (6). VAP is not only associated
with increased healthcare costs but also significantly contributes
to increased in-ICU morbidity and mortality (6).
Since both COPD and VAP adversely affect lung
function, a combination of both disorders may have serious effects
on patient outcomes. The inter-relation between COPD and VAP,
however, has not been thoroughly analyzed in the literature. In a
narrative review, Koulenti et al (7) assessed the current literature on the
effects of VAP on patients with COPD and vice versa. To the best of
our knowledge, to date, no meta-analysis has analyzed outcomes of
patients with COPD and VAP. Therefore, the purpose of the present
review was to answer the following questions by pooling data from
the literature: i) whether COPD as a co-morbidity influences
outcomes of patients with VAP as compared to VAP alone; and ii)
whether the development of VAP in patients with COPD is associated
with unfavorable outcomes as compared with that in patients not
developing VAP.
Materials and methods
Search strategy
This review was conducted following the guidelines
of the Preferred Reporting Items for Systematic Reviews and
Meta-analyses statement (8). A
total of two reviewers (MY and ML) independently performed an
electronic search of the PubMed, Embase, Scopus, BioMed Central,
CENTRAL and Google scholar databases. The last search was carried
out on 15th April 2020. Both MeSH terms and free-text key words
were used for searching relevant articles. The following key words
were used: ‘Chronic obstructive pulmonary disease’, ‘chronic
obstructive lung disease’, ‘chronic obstructive airway disease’,
‘pneumonia’, ‘ventilator associated pneumonia’,
‘ventilator-associated pneumonia’, ‘mortality’, ‘death’, ‘intensive
care’ and ‘hospital stay’. The reviewers screened the search
results initially by their titles and abstracts for each database.
After identifying potentially pertinent articles, full texts of the
articles were extracted. Both the reviewers assessed individual
articles based on the inclusion and exclusion criteria. Any
disagreements were resolved by discussion. After screening, the
bibliography of included studies and review articles on the subject
were hand-searched for any missed references.
Inclusion criteria
Both prospective and retrospective observational
studies were considered for this review. For the first part, i.e.
to assess the impact of COPD on outcomes of VAP, the following
inclusion criteria were used: i) studies conducted on patients with
VAP admitted to an ICU; ii) study participants received mechanical
ventilation for >48 h for any medical or post-surgical care;
iii) patients receiving only non-invasive ventilation were
excluded; iv) the cohort was divided into patients with COPD and
those without COPD and assess at least one of the three outcomes:
Mortality, duration of mechanical ventilation and length of ICU
stay. For the second part, i.e. to assess the impact of VAP on
outcomes of patients with COPD, the following inclusion criteria
were used: i) studies on patients with COPD admitted to an ICU and
requiring mechanical ventilation for >48 h; ii) the cohort was
divided into patients with VAP and without VAP and assess at least
one of the three outcomes: Mortality, duration of mechanical
ventilation and length of ICU stay. For both groups, single-arm
studies and studies not reporting relevant data were excluded.
Data extraction and risk of bias
analysis
After mutual agreement regarding the inclusion of
studies, the two reviewers extracted data from the included studies
independently. For the first part, data including the first
author’s name, publication year, study type, sample size,
demographic details, reason for ICU admission, presence of
co-morbidities and shock, previous use of steroids and antibiotics,
disease severity scores, number of patients with VAP due to
multi-drug resistant bacteria, partial pressure of oxygen/fraction
of inspired oxygen (PO2/FiO2), clinical
pulmonary infection score (CPIS) and study outcomes were extracted.
For the second part, data including the name of the first author,
publication year, study type, sample size, demographic details,
presence of co-morbidities, simplified acute physiology score II
(SAPS II), previous use of steroids and antibiotics, number of
patients with VAP due to multi-drug resistant bacteria and study
outcomes were extracted.
Outcomes of the analysis were the same for both
parts of the review. The primary outcome of interest was mortality.
Secondary outcomes of interest were duration of mechanical
ventilation and length of ICU stay. Data were fed into
meta-analysis software and cross-checked for correctness. In the
case of missing outcome data, the corresponding author was
contacted via email.
The risk of a bias assessment tool for
non-randomized studies was used to analyze the quality of included
studies (9). Two reviewers (MY and
ML) independently assessed the quality of studies and any
disagreements were resolved after discussion. Studies were assessed
for the following items: Selection of participants, confounding
variables, measurement of intervention, blinding of outcome
assessment, incomplete outcome data and selective outcome
reporting.
Statistical analysis
Review Manager (version 5.3; Cochrane Collaboration)
was used for the meta-analysis. Categorical data of mortality were
pooled to obtain the risk ratio (RR) with 95% CI. Since the
duration of mechanical ventilation and length of ICU stay were
continuous outcomes, they were summarized using the mean difference
(MD) with 95% CI. If data were presented as the median and
interquartile range, the mean and standard deviation scores were
calculated using the method developed by Wan et al (10). A random-effects model was used to
calculate the pooled effect size for all analyses. Heterogeneity
was assessed using the I2 statistic. I2
values of 25-50% represented low, values of 50-75% medium and
>75% represented substantial heterogeneity. Due to the inclusion
of <10 studies in the review, funnel plots were not used to
assess publication bias.
Results
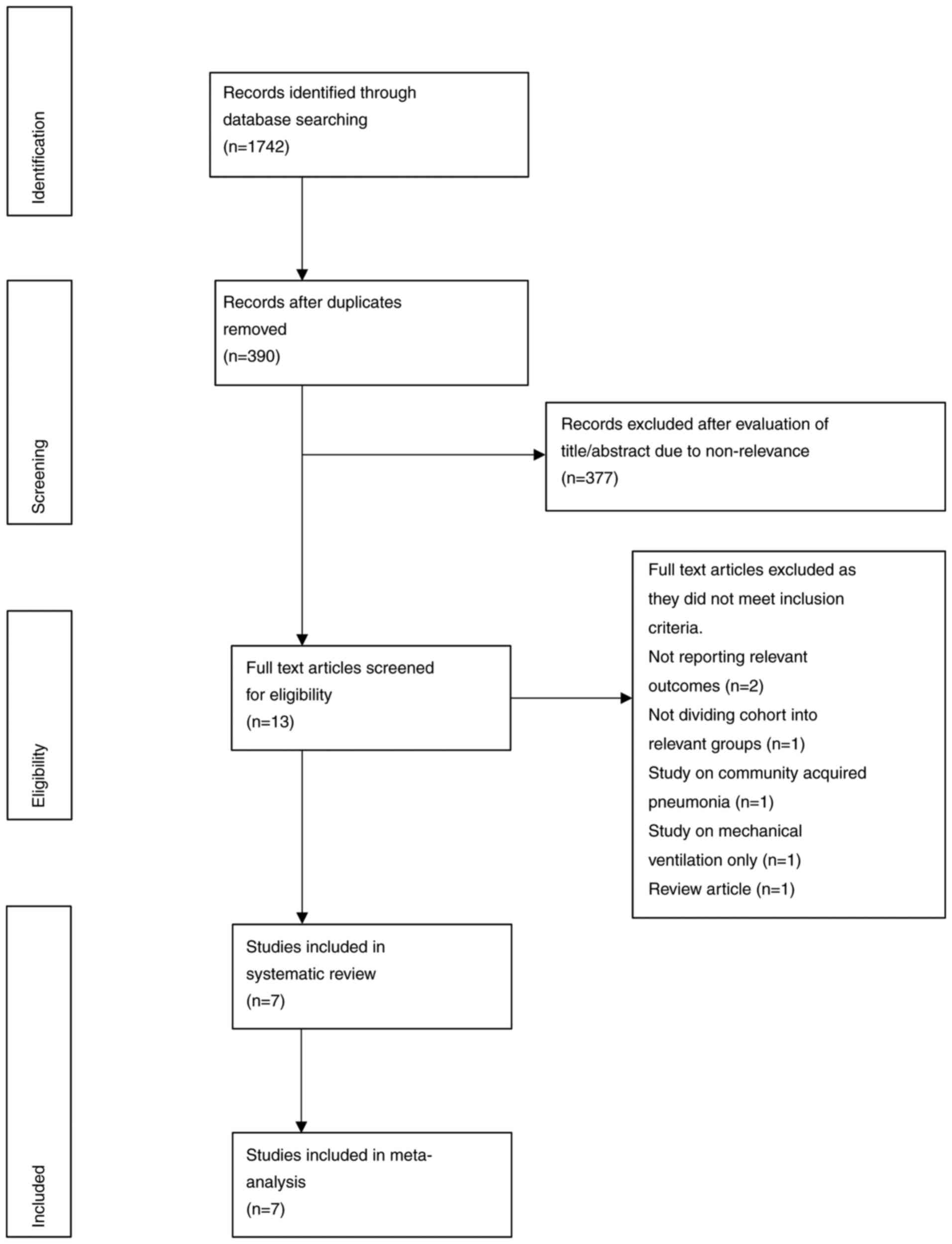
Study search and selection
A study flow chart is presented in Fig. 1. A total of 13 articles were
extracted for full-text analysis. A total of six studies were
excluded, as they did not fulfill the inclusion criteria. Finally,
7 studies were included in this systematic review and meta-analysis
(1,11-16).
Influence of COPD on outcomes of
VAP
A total of 3 studies (1,15,16)
assessed the impact of COPD on outcomes of VAP patients. Details of
these studies are presented in Table
I. All of them were prospective observational studies. The
sample size varied from 30 to 65 patients in the COPD arm and 126
to 308 patients in the non-COPD arm. Patients were admitted to the
ICUs for both medical and surgical reasons. The included studies
did not report any statistically significant differences in patient
co-morbidities between COPD and non-COPD patients, except for that
by Rouze et al (1), which
reported a significant difference in the number of diabetics.
Furthermore, disease severity was significantly higher in the COPD
group in the study of Makris et al (16). The studies did not report any
statistically significant difference in previous use of steroids
and antibiotics, presence of shock and
PO2/FiO2 between the two groups, except for
the study of Makris et al (16), wherein there was a higher incidence
of steroid use in patients with COPD. The CPIS was not
significantly different between COPD and non-COPD patients in all
three studies. Definitions of COPD and VAP in the included studies
are presented in Table II. The
definitions of COPD were based on standard American Thoracic
Society/European Respiratory Society criteria (17) and Global Initiative for Chronic
Obstructive Lung Disease (GOLD) criteria (4) in the included studies. Furthermore,
two studies (1,16) also used microbiological cultures for
confirmation of VAP.
 | Table ICharacteristics of studies assessing
the impact of COPD on outcomes of VAP. |
Table I
Characteristics of studies assessing
the impact of COPD on outcomes of VAP.
| | Author, year
(reference) |
|---|
| | Makris,
2011(16) | Rinaudo,
2015(15) | Rouzé,
2020(1) |
|---|
| Parameter | COPD | Non-COPD | COPD | Non-COPD | COPD | Non-COPD |
|---|
| Sample size | 65 | 150 | 30 | 126 | 61 | 308 |
| Mean age,
years | 68±11 | 58±17 | 71±9 | 63±17 | NR | NR |
| Reason for ICU
admission |
|
Medical | 54 | 103 | 26 | 95 | NR | NR |
|
Surgical | 11 | 47 | 4 | 31 | NR | NR |
| Co-morbidities |
|
Liver
cirrhosis | 3 | 3 | 2 | 8 | 5 | 18 |
|
Cardiac
disease | 21 | 21 | 16 | 37 | - | - |
|
Renal
failure | 4 | 4 | 4 | 8 | - | - |
|
Diabetes | 7 | 7 | 8 | 30 | 18a | 51a |
|
Alcoholism | - | - | - | - | 11 | 38 |
|
Respiratory
failure | - | - | - | - | 9 | 25 |
|
Heart
failure | - | - | - | - | 4 | 15 |
| Severity
scores | SAPS II 47±16 | SAPS II
53±18a | SOFA 7.5±3.3 | SOFA 7.5±3.2 | SOFA 8.4±3.3 | SOFA 7.9±3.6 |
| Presence of
shock | 19 | 39 | 13 | 62 | 5 | 17 |
| Previous use of
steroids | 17 | 6a | 16 | 51 | NR | NR |
| Prior use of
antibiotics | 37 | 61 | 26 | 100 | NR | NR |
| VAP due to MDR
bacteria | 39 | 86 | NR | NR | NR | NR |
|
PO2/FiO2 | 207±109 | 227±105 | 199± 64 | 211±78 | NR | NR |
| CPIS | 5.8±1.6 | 5.2±1.7 | 6.6±1.3 | 6.7±1.5 | 6 (5-8) | 7 (5-8) |
| Table IIDefinitions used by studies assessing
the impact of COPD on outcomes of VAP. |
Table II
Definitions used by studies assessing
the impact of COPD on outcomes of VAP.
| Study | Definition of
COPD | Definition of
VAP | (Refs.) |
|---|
| Makris et
al | According to
American Thoracic Society/European Respiratory Society
criteria | Presence of new or
progressive radiographic infiltrate associated with two of the
three of the following criteria: i) temperature >38.5 or
<36.5˚C; ii) leukocyte count >10,000 or <1,500/ml; iii)
purulent tracheal aspirate. In addition, a positive tracheal
aspirate culture (≥106 CFU/ml) or bronchoalveolar lavage
culture (≥104 CFU/ml) was required to confirm the
diagnosis of VAP. | (16) |
| Rinaudo et
al | According to
American Thoracic Society/European Respiratory Society
criteria | Presence of new or
progressive radiographic infiltrate associated with two of the
three of the following criteria: i) temperature of >38.5 or
<36.5˚C; ii) leucocyte count >12,000 or <4,000 cells/µl;
iii) purulent secretions. | (15) |
| Rouzé et
al | According to Global
Initiative for Chronic Obstructive Lung Disease criteria | Presence of new or
progressive radiographic infiltrate associated with two of the
following three criteria: i) temperature of >38.5 or <36.5˚C;
ii) leucocyte count >12,000 or <4,000 cells/µl; iii) purulent
secretions. In addition, all episodes of infection required
microbiological confirmation, with the isolation in the
endotracheal aspirate of at least 105 CFU/ml or in
bronchoalveolar lavage of at least 104 CFU/ml. | (1) |
Mortality data were reported by all three studies.
Meta-analysis of data from 156 COPD patients and 584 non-COPD
patients indicated that the presence of COPD significantly
increased the risk of mortality of patients with VAP (RR: 1.37, 95%
CI: 1.14-1.65, I2=3%, P=0.007; Fig. 2). Data on the duration of mechanical
ventilation and length of ICU stay were reported by two studies.
The present analysis failed to demonstrate any significant effect
of COPD on the duration of mechanical ventilation in patients with
VAP (MD: 2.37, 95% CI: -5.77 to 10.50, I2=38%, P=0.57;
Fig. 3). However, the duration of
ICU stay was significantly longer in patients with COPD and VAP as
compared to that in patients with VAP without COPD (MD: 5.53, 95%
CI: 0.73-10.33, I2=0%, P=0.02; Fig. 4).
Influence of VAP on outcomes of
COPD
A total of 4 studies (11-14)
assessed the impact of VAP on outcomes of patients with COPD.
Details of these studies are presented in Table III. Of these, 3 were prospective
studies (11-13),
while one was a retrospective study (14). The sample size of the VAP arm varied
from 35 to 92 patients and the sample size of the non-VAP arm
varied from 60 to 318. There was no significant difference in the
mean age between the study groups. None of the studies reported any
difference in patient co-morbidities and SAPS II scores.
Definitions of COPD and VAP used by the included studies are
presented in Table IV. A total of
2 studies (13,14) did not define the diagnostic criteria
for COPD and 2 studies (11,14)
used microbiological culture for diagnosing VAP.
| Table IIICharacteristics of studies assessing
impact of VAP on outcomes of COPD. |
Table III
Characteristics of studies assessing
impact of VAP on outcomes of COPD.
| | | Sample size | Mean age
(years) | Co-morbidities | SAPS II score | Past use of
steroids | Prior use of
antibiotics | | |
|---|
| Author (year) | Study type | No-VAP | VAP | No-VAP | VAP | VAP | No VAP | VAP | No VAP | VAP | No VAP | VAP | No VAP | VAP due to MDR
bacteria | (Refs.) |
|---|
| Nseir (2005) | P | 77 | 77 | 70±9 | 70±8 | Cardiac failure: 16
Renal failure: 8 Neurological disease: 3 Diabetes: 10 | Cardiac failure: 11
Renal failure: 6 Neurological disease: 2 Diabetes: 14 | 37±14 | 39±13 | 34 | 28 | 53 | 33a | 32 | (11) |
| Hadda (2014) | R | 35 | 118 | 61.1±10.7 | 61.1±12 | Present: 16 | Present: 55 | 48.9±12 | 45.9±14.5 | NR | NR | NR | NR | NR | (14) |
| Badawy (2015) | P | 92 | 60 | 56.1±15 | 59±9.5 | NR | NR | NR | NR | NR | NR | NR | NR | 34 | (13) |
| Koulenti
(2015) | P | 79 | 318 | 68.6±11 | 69.4±11.1 | Liver cirrhosis: 4
Cardiac disease: 33 Renal insufficiency: 20 Diabetes: 18 | Liver cirrhosis: 15
Cardiac disease: 125 Renal insufficiency: 53 Diabetes: 60 | 45 (34-57) | 46 (35-59) | NR | NR | NR | NR | NR | (12) |
| Table IVDefinitions used by studies assessing
impact of VAP on outcomes of COPD. |
Table IV
Definitions used by studies assessing
impact of VAP on outcomes of COPD.
| Study | Definition of
COPD | Definition of
VAP | (Refs.) |
|---|
| Nseir et
al | According to
American Thoracic Society criteria | Presence of new or
progressive radiographic infiltrate associated with two of the
following three criteria: i) temperature >38.5 or <36.5˚C;
ii) leukocyte count >10,000 or <1,500/ml; iii) purulent
tracheal aspirate. In addition, a positive tracheal aspirate
culture (≥106 CFU/ml). | (11) |
| Hadda et
al | NS | Radiographic
features suggestive of pneumonia plus presence of any two of the
following: fever, leukocytosis, purulent or change in the character
of endotracheal aspirate, isolation of the pathogen from of
endotracheal aspirate or other respiratory specimen and
hypoxemia. | (14) |
| Badawy et
al | NS | Based on the
American College of Chest Physicians criteria as an association of
a new or progressive consolidation on chest radiology plus at least
two of the following variables: fever with temperature >38˚C,
leukocytosis or leukopenia and purulent secretions. | (13) |
| Koulenti et
al | Presence of COPD
was recorded based on pulmonary function tests prior to ICU
admission where available, or on clinical criteria, medical history
(including significant smoke exposure, previous use of respiratory
medications) and evidence of hyper-inflation on chest
radiograph. | Pulmonary infection
arising ≥48 h after endotracheal intubation with no evidence of
pneumonia at the time of intubation or the diagnosis of a new
pulmonary infection if the initial admission to the ICU was for
pneumonia. | (12) |
Data on mortality were reported by all four studies.
The present meta-analysis with data of 283 patients with VAP and
573 patients without VAP indicated that the presence of VAP
significantly increased the mortality of patients with COPD (RR:
1.52, 95% CI: 1.08-2.12, I2=71%, P=0.02; Fig. 5). Data on secondary outcomes were
also reported by all four studies. Pooled analysis indicated that
the presence of VAP in patients with COPD significantly increased
the duration of mechanical ventilation (MD: 13.73, 95% CI:
7.86-19.61, I2=92%, P<0.00001; Fig. 6). In addition, patients with VAP and
COPD had a significantly longer ICU stay as compared to patients
with COPD without VAP (MD: 17.36, 95% CI: 9.55-25.17,
I2=90%, P<0.0001; Fig.
7).
Risk of bias analysis
The results of the authors' judgement of the risk of
bias in individual studies are presented in Table V. All studies included both study
and control cases from the same hospital setups and therefore had
low risk of bias for ‘selection of patients’. None of the studies
took into account all possible confounding factors. Selection bias
could not be assessed as no prior protocols were available for
comparison. The overall quality of the studies was moderate.
| Table VRisk of bias in included studies. |
Table V
Risk of bias in included studies.
| Study | Selection of
participants | Confounding
variables | Measurement of
intervention | Blinding of outcome
assessment | Incomplete outcome
data | Selective outcome
reporting | (Refs.) |
|---|
| Makris et
al | Low risk | High risk | Low risk | High risk | Low risk | Unclear risk | (16) |
| Rinaudo et
al | Low risk | High risk | Low risk | High risk | Low risk | Unclear risk | (15) |
| Rouzé et
al | Low risk | High risk | Low risk | High risk | Low risk | Unclear risk | (1) |
| Nseir et
al | Low risk | High risk | Low risk | High risk | Low risk | Unclear risk | (11) |
| Hadda et
al | Low risk | High risk | Low risk | High risk | Low risk | Unclear risk | (14) |
| Badawy et
al | Low risk | High risk | Low risk | High risk | Low risk | Unclear risk | (13) |
| Koulenti et
al | Low risk | High risk | Low risk | High risk | Low risk | Unclear risk | (12) |
Discussion
The results of the present systematic review and
meta-analysis suggested a significant inter-relation of COPD and
VAP regarding patient outcomes. The presence of COPD as a
co-morbidity in patients with VAP was significantly associated with
a higher odds of mortality and increased duration of ICU stay as
compared with those of patients without COPD. On the other hand,
the analysis also indicated that the development of VAP in a cohort
of patients with COPD admitted to the ICU significantly increased
mortality, the duration of mechanical ventilation and length of ICU
stay as compared with those of patients with COPD but without
VAP.
According to previous studies, COPD is a
common-co-morbidity in patients with VAP (18,19).
However, it was demonstrated that the presence of COPD is not
associated with a higher incidence of VAP as compared with that of
patients without COPD (1,12). Over the last decades, several
studies have attempted to assess the impact of COPD on the outcomes
of patients with VAP. However, many of these studies did not take
baseline differences and disease severity in COPD and non-COPD
patients into account while comparing mortality. A study by Rello
et al (20) on 129 patients
with VAP, including 24 patients with COPD, reported significantly
higher mortality of 33% in patients with COPD as compared to 9% in
patients without COPD. However, after taking into account other
confounding factors such as age >45 years, corticosteroid use,
presence of shock, hospital stay >9 days and prior use of
antibiotics, the authors did not identify any significant impact of
COPD on mortality of patients with VAP. By contrast, in another
study of 78 patients with VAP, Torres et al (21) reported that COPD was a significant
risk factor for mortality on multivariate analysis. In view of this
ambiguity in the literature, in the present meta-analysis, only
those studies which divided their cohort into two groups based on
the presence of COPD and reported disease severity were pooled. The
analysis indicated that the presence of COPD as a co-morbidity
leads to a 1.37-fold increased risk of mortality in patients with
VAP. The reason for this increased risk of death may be attributed
to several factors including the adverse influence of COPD on
baseline respiratory function, nutritional status of patients with
COPD or previous long-term use of corticosteroids (17,22).
An autopsy study by Scott et al (23) indicated increased injury and
collagen deposition in diaphragms of patients with COPD. This is
thought to reduce respiratory muscle function in patients with
COPD, which may contribute to higher mortality (16,23).
The reduced respiratory function of patients with COPD has also
been reported to impact outcomes of patients undergoing mechanical
ventilation without the development of VAP. A study by Rodríguez
et al (24) on 235 patients
reported that the presence of non-exacerbated COPD significantly
increased mortality of patients undergoing mechanical ventilation.
Studies have also indicated that patients with COPD developing VAP
have a high presence of multi-drug resistant (MDR) bacteria
(12,16,25).
Koulenti et al (12)
reported a significantly higher number of Pseudomonas
aeruginosa isolates in patients with COPD developing VAP as
compared to non-COPD patients. Patients with VAP due to MDR
bacteria are at a higher risk of receiving incorrect antibiotic
treatment, which may increase the mortality of such individuals
(16).
The present analysis on the influence of COPD as a
comorbidity on the duration of mechanical ventilation and length of
ICU stay only pooled two studies. While no difference in the
duration of mechanical ventilation was identified between VAP
patients with and without COPD, the presence of COPD was indicated
to significantly increase the duration of ICU stay. The association
of disease severity with these secondary outcomes was assessed by
Makris et al (16), who
indicated that the duration of mechanical ventilation and length of
ICU stay were significantly longer for GOLD stage IV COPD vs.
non-COPD VAP patients, but not for GOLD stage I-III COPD patients.
However, the authors did not assess the same relationship for
VAP-associated mortality. An important factor that may also
influence the incidence and outcomes of VAP patients is the primary
cause of ICU admission. Specific groups of patients such as those
with neurological disorders or neurosurgical patients may be at a
higher risk of developing VAP and subsequent adverse outcomes. This
may be due to several reasons such as increased risk of aspiration,
use of intravenous anesthetics and sedatives or prolonged duration
of ventilation (26). A
meta-analysis by Melsen et al (27) indicated that the attributable
mortality of VAP differs with different sub-groups of patients with
higher rates for surgical patients as compared to medical or trauma
patients. Exact details of the primary cause of ICU admission were
not available in the studies included in the review. Lack of
sufficient data preclude us from drawing strong conclusions on the
influence of COPD on secondary outcomes.
Patients with COPD frequently encounter
exacerbations during the course of the disease, which require
respiratory support and hospitalization (28). Non-invasive ventilation is usually
the standard of care during such periods, but in certain cases,
endotracheal intubation may be required to reduce mortality
(4). Invasive mechanical
ventilation may, however, be complicated by VAP. The incidence of
VAP in intubated patients with COPD may vary from 18.6% to as high
as 60% and may affect patient outcomes (12,13).
The association between the development of VAP and increased
morbidity and mortality for ICU patients has been assessed by
several studies, but with heterogenous patient populations and
inconsistent results (29-31).
In the second part of the present analysis, it was indicated that
patients with COPD developing VAP during the course of their
management had a 1.52-fold increased risk of mortality as compared
with that of patients not developing VAP. On analysis of the forest
plots in the present study, it was indicated that with the
exception of one study (14), all
other studies reported a higher risk of mortality with VAP in
patients with COPD. In the study of Hadda et al (14), the overall mortality rate in the
cohort was high (51%), which was attributed to high disease
severity of the sample, presence of type 2 respiratory failure and
hypoxemia. It should be noted that the study by Hadda et al
(14) was the only retrospective
study in the present meta-analysis, while the remaining studies
were prospective studies. The present results also indicated that
the development of VAP in patients with COPD significantly
increased the duration of mechanical ventilation by a mean of 13
days and prolonged the ICU stay by 17 days. Statistically
significant results for these secondary outcomes were reported by
all four studies included in the present systematic review.
It is important to note that several other
confounding factors may influence the outcomes of patients with
COPD developing VAP. First, numerous co-morbidities may co-exist in
patients with COPD, which can affect mortality, duration of
mechanical ventilation and length of ICU stay (32). A meta-analysis of 37 studies by
Singanayagam et al (33)
reported that low body mass index, cardiac failure, diabetes
mellitus, ischemic heart disease and malignancy are significantly
associated with increased mortality in patients with acute
exacerbations of COPD. It is also reported that the presence of
more than one co-morbidity may double the risk of COPD-associated
mortality (34). Furthermore,
similar co-morbidities are known to also influence outcomes of VAP
(18). Thus, the results of the
present analysis may have been confounded by these variables. Among
the four studies included in the present review, data on
co-morbidities were reported by all except that by Badawy et
al (13). However, none of them
reported any statistically significant differences between their
study cohorts. In addition, the management of COPD may vary
depending on the severity of the disease. The management protocol
may include short- or long-acting muscarinic antagonists,
β-agonists, inhaled corticosteroids (ICS), supplemental oxygen
therapy or combinations of these drugs (35). It was postulated that chronic ICS
use in COPD may diminish the patient's defenses, leading to a rise
in opportunistic infections such as VAP (12). Of the included studies, no study
assessing the influence of VAP on COPD outcomes analyzed the
influence of ICS on patient mortality. The study by Koulenti et
al (12) included data on
chronic steroid use in the definition of immunosuppression.
However, in their analysis, immunosuppression was not indicated to
be a significant factor increasing the prevalence of VAP in
patients with COPD. The literature on the role of ICS on outcomes
of community-acquired pneumonia is conflicting. Studies have
reported that patients with COPD receiving long-term ICS may have a
higher prevalence of community-acquired pneumonia but its effects
on patient mortality remain unclear (36,37).
The results of the present study should be
interpreted with the following limitations. First, only a limited
number of studies were available for meta-analysis. In the pooled
analysis of two outcome measures, data from only two studies were
analyzed. The lack of adequate data may have introduced bias in the
overall results. The overall quality of studies was also not high.
Furthermore, the inherent bias of the observational studies may
have skewed the outcomes. There were differences in the included
studies with respect to the exact diagnostic criteria of VAP with
few studies utilizing microbiological cultures. In addition, not
all studies reported complete data on baseline characteristics of
the study cohorts. Furthermore, data on the severity of COPD were
not available for any study and therefore, the influence of the
severity of COPD on the outcomes could not be assessed. As another
limitation, the heterogeneity in the present meta-analysis for
assessing the influence of VAP on outcomes of COPD was high. This
may be attributed to differences in the study settings and study
populations among the included studies. However, due to the limited
number of studies, it was not possible to explore the source of
heterogeneity by a sub-group or meta-regression analysis. Finally,
treatment protocols vary with patients as well as hospital setups.
Therefore, with these limited data, it may not be possible to
generalize the results of the present review.
In spite of these limitations, the present study was
the first meta-analysis to assess the inter-relationship of the
effects of VAP and COPD on patient outcomes and the results may
have implications for clinical practice. Based on the present
results, it may be suggested that prompt and thorough management is
recommended for patients with COPD developing VAP. Such patients
should be considered as having a high risk of mortality. There is
also a requirement for rigorous measures to prevent the development
of VAP in patients with COPD.
To conclude, within the limitations of the present
study, the results indicated that the combination of COPD and VAP
significantly increases patient mortality and the duration of ICU
stay. The development of VAP in patients with COPD also
significantly increased the duration of mechanical ventilation.
Further case-matched studies are required to assess the
relationship of the severity of COPD combined with VAP on patient
outcomes.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MY conceived and designed the study. MY and ML
collected the data and performed the literature search. MY was
involved in the writing of the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rouzé A, Boddaert P, Martin-loeches I,
Povoa P, Rodriguez A, Ramdane N, Salluh J, Houard M and Nseir S:
Impact of chronic obstructive pulmonary disease on incidence,
microbiology and outcome of ventilator-associated lower respiratory
tract infections. Microorganisms. 8(165)2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Tsiligianni I, Metting E, Van Der Molen T,
Chavannes N and Kocks J: Morning and night symptoms in primary care
COPD patients: A cross-sectional and longitudinal study. An UNLOCK
study from the IPCRG. NPJ Prim Care Respir Med.
26(16040)2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tantucci C and Pini L: Inhaled
corticosteroids in COPD: Trying to make a long story short. Int J
Chron Obstruct Pulmon Dis. 15:821–829. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Rabe KF, Hurd S, Anzueto A, Barnes PJ,
Buist SA, Calverley P, Fukuchi Y, Jenkins C, Rodriguez-Roisin R,
van Weel C, et al: Global strategy for the diagnosis, management,
and prevention of chronic obstructive pulmonary disease: GOLD
executive summary. Am J Respir Crit Care Med. 176:532–555.
2007.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Kallet RH: Ventilator bundles in
transition: From prevention of ventilator-associated pneumonia to
prevention of ventilator-associated events. Respir Care.
64:994–1006. 2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hellyer TP, Ewan V, Wilson P and Simpson
AJ: The Intensive Care Society recommended bundle of interventions
for the prevention of ventilator-associated pneumonia. J Intensive
Care Soc. 17:238–243. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Koulenti D, Parisella FR, Xu E, Lipman J
and Rello J: The relationship between ventilator-associated
pneumonia and chronic obstructive pulmonary disease: what is the
current evidence? Eur J Clin Microbiol Infect Dis. 38:637–647.
2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Moher D, Liberati A, Tetzlaff J and Altman
DG: PRISMA Group: Preferred reporting items for systematic reviews
and meta-analyses: The PRISMA Statement. PLoS Med.
6(e1000097)2009.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kim SY, Park JE, Lee YJ, Seo HJ, Sheen SS,
Hahn S, Jang BH and Son HJ: Testing a tool for assessing the risk
of bias for nonrandomized studies showed moderate reliability and
promising validity. J Clin Epidemiol. 66:408–14. 2013.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wan X, Wang W, Liu J and Tong T:
Estimating the sample mean and standard deviation from the sample
size, median, range and/or interquartile. range.
14(135)2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Nseir S, Di Pompeo C, Soubrier S, Cavestri
B, Jozefowicz E, Saulnier F and Durocher A: Impact of
ventilator-associated pneumonia on outcome in patients with COPD.
Chest. 128:1650–1656. 2005.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Koulenti D, Blot S, Dulhunty JM, Papazian
L, Martin-Loeches I, Dimopoulos G, Brun-Buisson C, Nauwynck M,
Putensen C, Sole-Violan J, et al: COPD patients with
ventilator-associated pneumonia: Implications for management. Eur J
Clin Microbiol Infect Dis. 34:2403–2411. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Badawy MS, Omar HM, Mohamdien HA, Moktar
EA and Deaf EA: Evaluation of risk factors of ventilator associated
pneumonia on outcome of acute exacerbation of chronic obstructive
pulmonary disease. Egypt J Chest Dis Tuberc. 64:799–803. 2015.
|
|
14
|
Hadda V, Khilnani GC, Dubey G, Nallan R,
Kumar G and Guleria R: Impact of ventilator associated pneumonia on
outcome in patients with chronic obstructive pulmonary disease
exacerbation. Lung India. 31:4–8. 2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Rinaudo M, Ferrer M, Terraneo S, De Rosa
F, Peralta R, Fernández-Barat L, Li Bassi G and Torres A: Impact of
COPD in the outcome of ICU-Acquired pneumonia with and without
previous intubation. Chest. 147:1530–1538. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Makris D, Desrousseaux B, Zakynthinos E,
Durocher A and Nseir S: The impact of COPD on ICU mortality in
patients with ventilator-associated pneumonia. Respir Med.
105:1022–1029. 2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Celli BR and MacNee W: ATS/ERS Task Force:
Standards for the diagnosis and treatment of patients with COPD: A
summary of the ATS/ERS position paper. Eur Respir J. 23:932–946.
2004.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Wu D, Wu C, Zhang S and Zhong Y: Risk
factors of ventilator-associated pneumonia in critically III
patients. Front Pharmacol. 10(482)2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
van der Kooi TII, Boshuizen H, Wille JC,
de Greeff SC, van Dissel JT, Schoffelen AF and van Gaalen RD: Using
flexible methods to determine risk factors for
ventilator-associated pneumonia in the Netherlands. PLoS One.
14(e0218372)2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Rello J, Ausina V, Ricart M, Castella J
and Prats G: Impact of previous antimicrobial therapy on the
etiology and outcome of ventilator-associated pneumonia. Chest.
104:1230–1235. 1993.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Torres A, Aznar R, Gatell JM, Jiménez P,
González J, Ferrer A, Celis R and Rodriguez-Roisin R: Incidence,
risk, and prognosis factors of nosocomial pneumonia in mechanically
ventilated patients. Am Rev Respir Dis. 142:523–528.
1990.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Ranzani OT, Ferrer M, Esperatti M, Giunta
V, Bassi GL, Carvalho CR and Torres A: Association between systemic
corticosteroids and outcomes of intensive care unit-acquired
pneumonia. Crit Care Med. 40:2552–2561. 2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Scott A, Wang X, Road J and Reid W:
Increased injury and intramuscular collagen of the diaphragm in
COPD: Autopsy observations. Eur Respir J. 27:51–59. 2006.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Rodríguez A, Lisboa T, Solé-Violán J,
Gómez F, Roca O, Trefler S, Gea J, Masclans JR and Rello J: Impact
of nonexacerbated COPD on mortality in critically Ill patients.
Chest. 139:1354–1360. 2011.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Moghoofei M, Azimzadeh Jamalkandi S, Moein
M, Salimian J and Ahmadi A: Bacterial infections in acute
exacerbation of chronic obstructive pulmonary disease: A systematic
review and meta-analysis. Infection. 48:19–35. 2020.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Wu VKS, Fong C, Walters AM and Lele AV:
Prevalence, clinical characteristics, and outcomes related to
ventilator-associated events in neurocritically Ill patients.
Neurocrit Care. 33:499–507. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Melsen WG, Rovers MM, Groenwold RH,
Bergmans DC, Camus C, Bauer TT, Hanisch EW, Klarin B, Koeman M,
Krueger WA, et al: Attributable mortality of ventilator-associated
pneumonia: A meta-analysis of individual patient data from
randomised prevention studies. Lancet Infect Dis. 13:665–671.
2013.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Kong CW and Wilkinson TM: Predicting and
preventing hospital readmission for exacerbations of COPD. ERJ Open
Res. 6:00325–02019. 2020.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Balasubramanian P and Tullu MS: Study of
ventilator-associated pneumonia in a pediatric intensive care Unit.
Indian J Pediatr. 81:1182–1186. 2014.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Karakuzu Z, Iscimen R, Akalin H, Girgin
NK, Kahveci F and Sinirtas M: Prognostic risk factors in
ventilator-associated pneumonia. Med Sci Monit. 24:1321–1328.
2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Ranjan N, Chaudhary U, Chaudhry D and
Ranjan KP: Ventilator-associated pneumonia in a tertiary care
intensive care unit: Analysis of incidence, risk factors and
mortality. Indian J Crit Care Med. 18:200–204. 2014.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Crisafulli E, Barbeta E, Ielpo A and
Torres A: Management of severe acute exacerbations of COPD: An
updated narrative review. Multidiscip Respir Med.
13(36)2018.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Singanayagam A, Schembri S and Chalmers
JD: Predictors of mortality in hospitalized adults with acute
exacerbation of chronic obstructive pulmonary disease: A systematic
review and meta-analysis. Ann Am Thorac Soc. 10:81–89.
2013.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Recio Iglesias J, Díez-Manglano J, López
García F, Díaz Peromingo JA, Almagro P and Varela Aguilar JM:
Management of the COPD patient with comorbidities: An experts
recommendation document. Int J Chron Obstruct Pulmon Dis.
15:1015–1037. 2020.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Crawley A, Laubscher T, Muddiman P and
Kosar L: Pharmacologic management of COPD: Breadth of products for
encouraging a breath of air. Can Fam Physician. 62:410–414.
2016.PubMed/NCBI
|
|
36
|
Yamauchi Y, Yasunaga H, Hasegawa W,
Sakamoto Y, Takeshima H, Jo T, Matsui H, Fushimi K and Nagase T:
Effect of outpatient therapy with inhaled corticosteroids on
decreasing in-hospital mortality from pneumonia in patients with
COPD. Int J Chron Obstruct Pulmon Dis. 11:1403–1411.
2016.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Sibila O, Soto-Gomez N and Restrepo MI:
The risk and outcomes of pneumonia in patients on inhaled
corticosteroids. Pulm Pharmacol Ther. 32:130–136. 2015.PubMed/NCBI View Article : Google Scholar
|