Introduction
Recurrent spontaneous abortion (RSA), defined as two
or more consecutive pregnancy losses prior to 20 weeks of
gestation, may seriously compromise not only the physical but also
psychological well-being of women. Although parental or embryonic
karyotype anomalies, infection-associated factors, endocrine
disorders, uterine anatomic abnormalities and anti-phospholipid
syndrome have been acknowledged as the common causes of RSA,
approximately half of the cases still remain unexplained (1). The development of the allogeneic fetus
in the maternal uterus represents an immunological paradox. A
successful pregnancy requires the maternal immune system to accept
the fetus expressing allogeneic paternal antigens and provide
competent responses to infections. Thus, maternal-fetal immune
abnormalities might have an important role in the development of
RSA (2).
The modulation of the maternal CD4+
T-cell response to fetal antigens has been considered an important
component of maternal-fetal tolerance during pregnancy. Upon
encountering antigens on the surface of antigen-presenting cells or
being driven by a set of cytokines, naive CD4+ T cells
are able to differentiate into distinct subsets, including type-1
T-helper (Th1), Th2, Th17 and T-regulatory (Treg) cells (3). While a pro-inflammatory
microenvironment is required for trophoblastic growth and invasion
(4), Th1 cytokines, including tumor
necrosis factor-α and interferon-γ, have deleterious effects on
pregnancy (5). For numerous years,
it has been thought that a shift in the maternal immune response
toward a Th2 bias is crucial for maintaining a successful pregnancy
(6).
Th17 cells have a critical role in inducing
inflammation, while abnormal Th17-cell levels have been associated
with the pathogenesis of autoimmune diseases (7). Treg cells express anti-inflammatory
cytokines, including interleukin (IL)-10 and transforming growth
factor (TGF)-β1, which dampen an excessively effective immune
response (8). Recent studies have
indicated that the balance between Treg and Th17 cells is also
important for maintaining a normal pregnancy, while a shift in the
Th17/Treg ratio toward Th17 cells has been suggested to cause
several pregnancy-associated diseases, including RSA, pre-eclampsia
and gestational diabetes mellitus (9-11).
In addition to the signal from antigen recognition,
T-cell activation requires a second signal from co-stimulatory
molecules, which maybe either positive or negative (12,13).
Among the inhibitory co-stimulatory molecules, cytotoxic
T-lymphocyte-associated protein 4 (CTLA-4), T-cell immunoglobulin
mucin-3 (Tim-3) and programmed cell death-1 (PD-1) have attracted
much attention regarding their roles in regulating Th17- and
Treg-cell function to maintain a balanced immune response (14-17).
For instance, Tim-3 has been associated with a shift in the balance
from Th17 and Treg cells to Treg dominance (16). The PD-1 signaling pathway has been
demonstrated to have an important role in Th17-cell function during
pregnancy (18). Furthermore, PD-1
and CTLA-4 are critical for the suppressive activity of Treg cells
(19,20), while
PD-1+Tim-3+Treg cells exhibit an increased
effector function (21). Previous
studies by our group revealed that the expression of these three
molecules was lower in human miscarriages than in normal
pregnancies, while their blockade during the implantation window
increased maternal rejection of the fetus in CBA/Jx BALB/c matings
(22,23).
Progesterone (P4), the most common medication for
fetal protection in RSA, is a multifunctional female hormone that
promotes breast development, ovulation and pregnancy maintenance;
it is mainly secreted by ovarian granulosa cells and the corpus
luteum during non-pregnancy and by the placenta during pregnancy
(24). While the mechanisms remain
to be fully elucidated, P4 has been reported to dampen immune
responses to fetal and maternal antigens (25). As an immunosuppressant, cyclosporine
A (CsA) has been widely used in organ transplantation (26). CsA not only induces Th2
immuno-dominance at the maternal-fetal interface, but also promotes
trophoblastic proliferation and invasion, further promoting
placental formation (27). This
immunosuppressive agent, categorized as pregnancy category C by the
Food and Drug Administration, has been utilized for the treatment
of RSA at our hospital (Hospital of Obstetrics and Gynecology,
Fudan University Shanghai Medical College) since 2005.
To the best of our knowledge, studies on the effects
of P4 or CsA on the proportion of Th17 and Treg cells within the
peripheral blood of patients with RSA are rare. Therefore, the
present study aimed to investigate the effects of P4 or CsA therapy
on the Th17/Treg cell balance and the expression of associated
molecules in the peripheral blood of pregnant females with a
history of RSA.
Materials and methods
Study population
For the present study, subjects aged between 20 and
39 years were recruited at the Obstetrics and Gynecology Hospital
of Fudan University (Shanghai, China) between July 2018 and
December 2018. The clinical characteristics of the enrolled
subjects are summarized in Table I.
The cohort included 30 females with normal early pregnancy (NP
group), 25 with RSA (RSA group), 27 pregnant females with a history
of RSA receiving progesterone (P4 group) and 24 pregnant females
with a history of RSA receiving cyclosporine A (CsA group).
Subjects with RSA included those undergoing spontaneous abortion
and who also had a history of two or more consecutive spontaneous
abortions before 20 weeks (the mean pregnancy week was 6.28±0.09)
of gestation without known causes (including parental or embryonic
karyotype anomalies, uterine anatomic abnormalities,
infection-associated factors, endocrine disorders and
antiphospholipid syndrome). The subjects in the NP group (the mean
pregnancy week was 6.26±0.11) had at least one successful pregnancy
and no history of spontaneous abortions. None of the subjects had
any history of autoimmune diseases or immunotherapy, renal or liver
diseases, alcohol addiction, smoking or vaccination within 3 months
prior to consultation. Approval of the present study was obtained
from the ethics committee of the Obstetrics and Gynecology Hospital
of Fudan University (Shanghai, China) and all subjects provided
written informed consent.
 | Table IClinical characteristics of enrolled
subjects. |
Table I
Clinical characteristics of enrolled
subjects.
|
Subjectsb | NP (n=30) | RSA (n=25) | P4 (n=27) | CsA (n=24) | P-value |
|---|
| Age mean
(years)a | 28.07±0.86 | 28.96±0.98 | 29.26±0.83 | 29±1.0 | 0.80 |
| Age range
(years) | 20-39 | 22-38 | 23-38 | 21-39 | N/A |
| Previous
spontaneous abortionsa | - | 2.92±0.22 | 2.85±0.15 | 2.95±0.23 | 0.93 |
| Pregnancy week (HCG
urine test)a | - | - | 4.72±0.09 | 4.58±0.09 | 0.33 |
| Pregnancy week
(venous blood was collected)a | 6.26±0.11 | 6.28±0.09 | 6.16±0.1 | 6.0±0.09 | 0.31 |
In this open-label (i.e. non-blind) study, pregnant
females with a history of RSA were randomly allocated to the P4 or
CsA group after a positive human chorionic gonadotropin urine test.
The P4 group received dydrogesterone (Abbott) 10 mg Q8 h orally,
while the CsA group received CsA (Sanofi) 50 mg Q8 h orally. After
10 days, venous blood was collected (at this time the mean
pregnancy week of P4 group was 6.16±0.1, the mean pregnancy week of
CsA group was 6.0±0.09).
Separation of peripheral blood
mononuclear cells
Peripheral blood mononuclear cells were isolated
from 5 ml heparinized venous blood using Ficoll-Hypaque density
gradient centrifugation (573 x g at room temperature for 20 min).
Cells were collected at the interface and washed with PBS. Cells
were cultured in RPMI 1640 (HyClone; GE Healthcare Life Sciences)
supplemented with 10% fetal bovine serum (HyClone; GE Healthcare
Life Sciences), 100 U/ml penicillin, 100 µg/ml streptomycin and 1
µg/ml amphotericin B. Phorbol 12-myristate 13-acetate (PMA; 50
ng/ml; BioLegend, Inc.), ionomycin (1 µg/ml; BioLegend, Inc.) and
brefeldin A (10 mg/ml; BioLegend, Inc.) were added to the culture
for 4 h prior to intracellular cytokine analysis.
Flow cytometric analysis
Cell surface molecular expression and intracellular
cytokine production were evaluated using flow cytometry (FCM).
Alexa eFluor® 488-conjugated anti-human forkhead box p3
(Foxp3; cat. no. 320112), phycoerythrin (PE)-conjugated anti-human
CD366 Tim-3 (cat. no. 345006) or CD152 CTLA-4 (cat. no. 349906),
PE/cyanine 7-conjugated anti-human IL-17A (cat. no. 512315),
allophycocyanine-conjugated anti-human CD279 PD-1 (cat. no. 329908)
or LAP TGF-β1 (cat. no. 349608), Brilliant Violet 421-conjugated
anti-human IL-10 (cat. no. 501422) and Brilliant Violet
510-conjugated anti-human CD4 (cat. no. 317444) antibodies
(BioLegend, Inc.) were used. For intracellular staining, cells were
fixed and permeabilized using the Fix/Perm kit (cat. no. 421401/2).
The fix/perm kit and all antibodies aforementioned were purchased
from BioLegend, Inc. Flow cytometry was performed on a
Beckman-Coulter CyAn ADP cytometer and the results were analyzed
using FlowJo software (version 7.6; FlowJo, LLC).
Statistical analysis
All variables were normally distributed in this
study. Thus, variables were presented as means and standard
deviation (SD). One-way ANOVA was used to evaluate differences.
P<0.05 was considered to indicate a statistically significant
difference. In cases where P<0.05 after ANOVA, Bonferroni's post
hoc test was performed to determine differences between each group.
All analyses were carried out using the GraphPad Prism 7 software
(GraphPad Software, Inc.).
Results
CsA significantly increases the
percentage of Treg cells and decreases the percentage of Th17 cells
in the peripheral blood of pregnant females with a history of
RSA
As presented in Fig.
1, the patients from the RSA group had a significantly
decreased percentage of Treg cells
(CD4+Foxp3+ cells) and an increased
percentage of Th17 cells (CD4+IL-17A+ cells)
in the peripheral blood compared with those in the NP group. Of
note, CsA increased the percentage of Treg cells, while decreasing
the percentage of Th17 cells in the peripheral blood of pregnant
females with a history of RSA compared with the percentages in the
RSA group. However, P4 exhibited no significant effect on the
proportion of Th17 or Treg cells in pregnant females with a history
of RSA compared with the proportions in the RSA group.
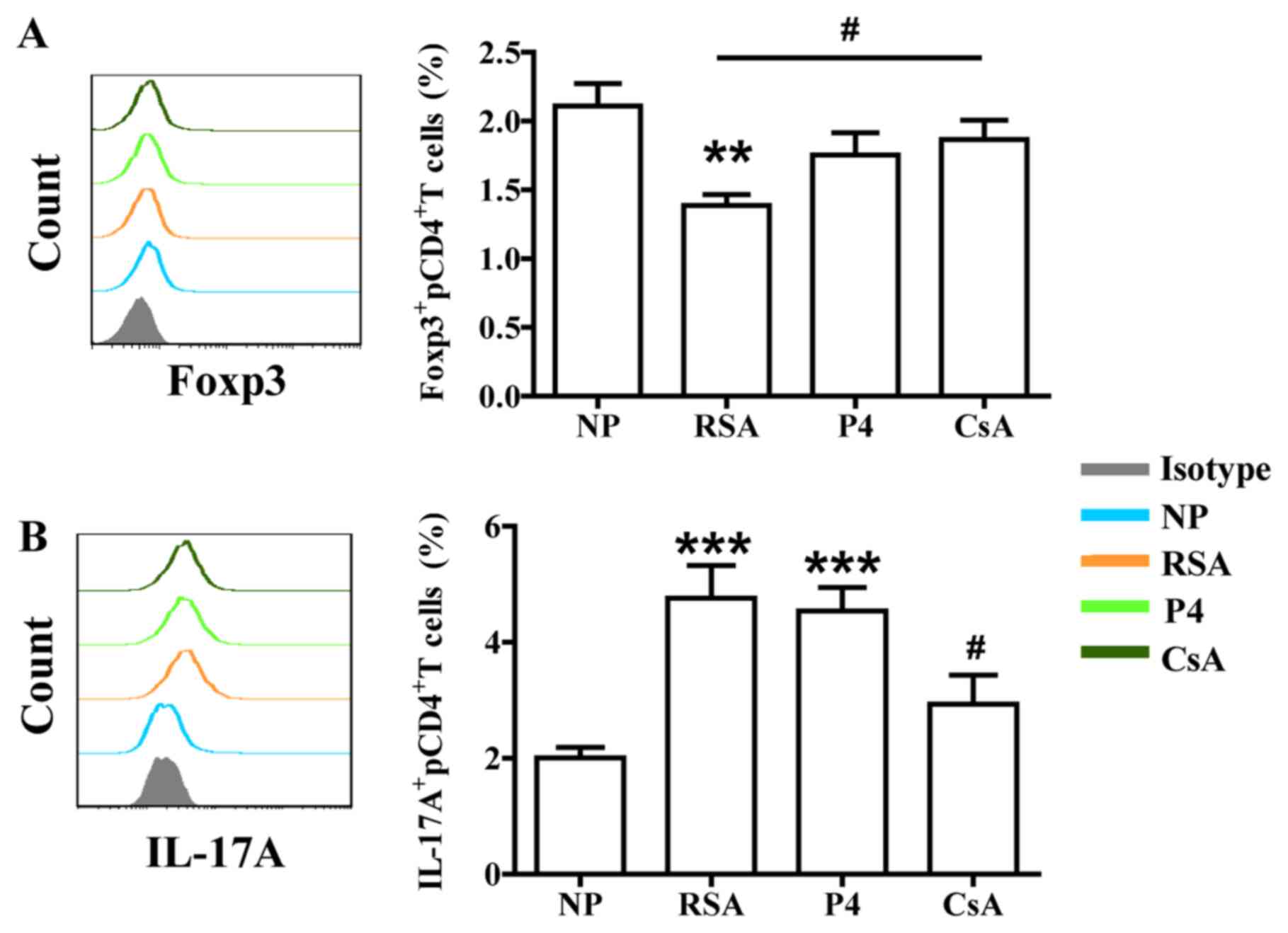 | Figure 1Effects of P4 and CsA on the
percentage of Treg and Th17 cells in peripheral blood. (A) Compared
with that in the NP group, the subjects in the RSA group had a
significantly lower percentage of Treg cells in the peripheral
blood. CsA significantly increased the percentage of Treg cells.
(B) Compared with that in the NP group, the subjects in the RSA
group had a higher percentage of Th17 cells in the peripheral
blood. CsA decreased the percentage of Th17 cells. Groups: NP,
normal early pregnancy; RSA; patients with RSA; P4, pregnant
females with a history of RSA treated with P4; CsA, pregnant
females with a history of RSA treated with CsA.
**P<0.01, ***P<0.001 vs. NP;
#P<0.05 vs. RSA. CsA, cyclosporine A; Treg cells,
T-regulatory cells; Th17 cells, type-17 T-helper cells; RSA,
recurrent spontaneous abortion; Fox, forkhead box; IL, interleukin;
P4, progesterone. |
CsA promotes TGF-β1 and IL-10
production in peripheral blood cells of pregnant females with a
history of RSA
To assess whether CsA or P4 regulates the biological
functions of Th17/Treg cells in pregnant females, the production of
cytokines (associated with Treg- and Th17-cell function) by
peripheral T cells was first analyzed. Compared with those in the
NP group, patients in the RSA group exhibited significantly lower
TGF-β1 and IL-10 expression in total peripheral (p) CD4+
T cells, pTreg cells and pTh17 cells. However, CsA increased TGF-β1
and IL-10 expression in the peripheral blood cells of pregnant
females with a history of RSA, whereas P4 promoted only TGF-β1
expression in pTh17 cells (Figs. 2
and 3).
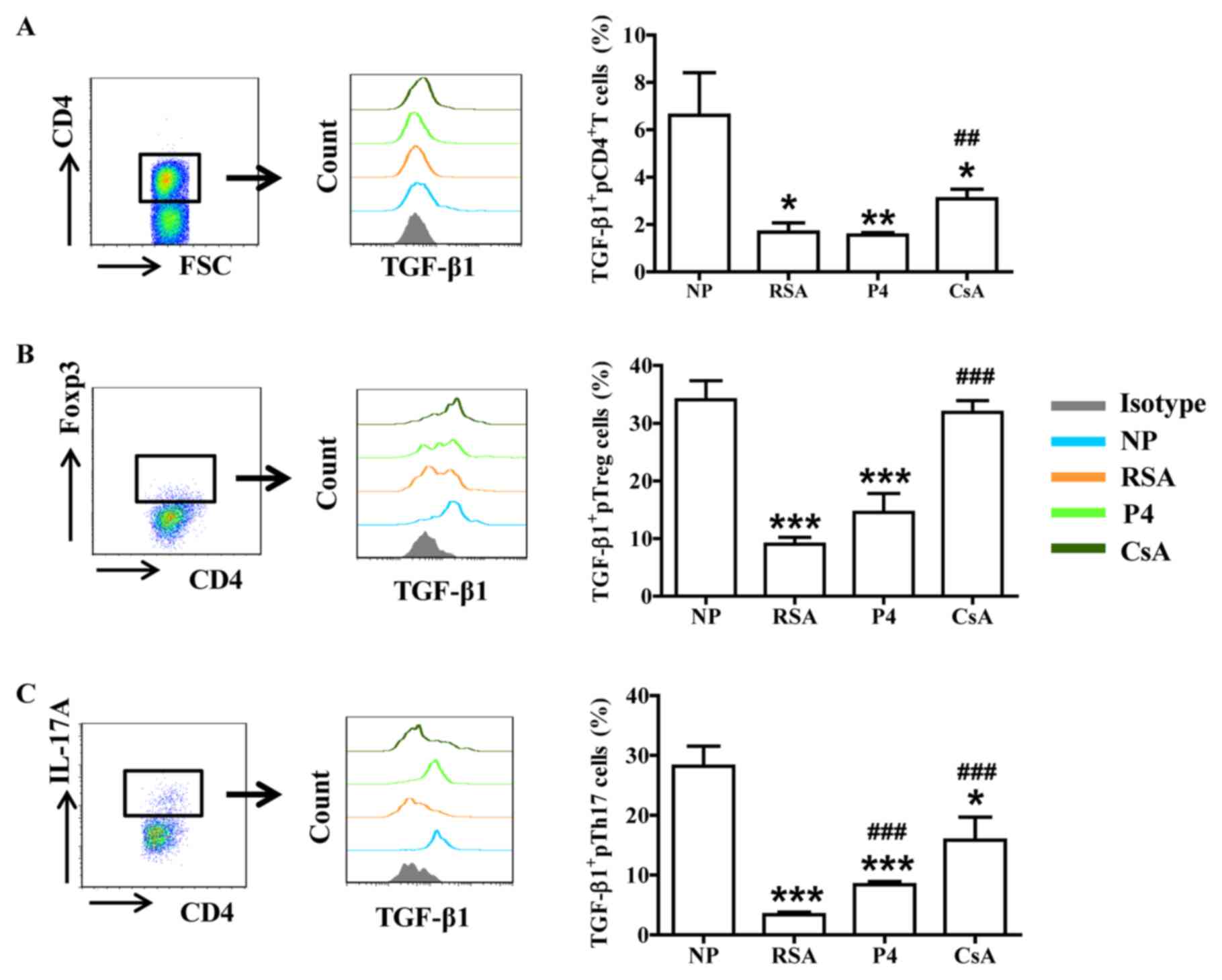 | Figure 2CsA promotes TGF-β1 expression in
peripheral blood cells of pregnant females with RSA. Compared with
that in the NP group, the production of TGF-β1in (A)
CD4+ T cells, (B) Treg cells and (C) Th17 cells in the
peripheral blood of subjects in the RSA group was decreased. While
CsA and P4 promoted the expression of TGF-β1 in Th17 cells, P4 had
no effect on TGF-β1 production by CD4+ T cells and Treg
cells. Groups: NP, normal early pregnancy; RSA; patients with RSA;
P4, pregnant females with a history of RSA treated with P4; CsA,
pregnant females with a history of RSA treated with CsA.
*P<0.05, **P<0.01,
***P<0.001 vs. NP; ##P<0.01,
###P<0.001 vs. RSA. CsA, cyclosporine A; pTreg cells,
peripheral T-regulatory cells; Th17 cells, type-17 T-helper cells;
RSA, recurrent spontaneous abortion; P4, progesterone; Fox,
forkhead box; IL, interleukin; TGF, transforming growth factor;
FSC, forward scatter. |
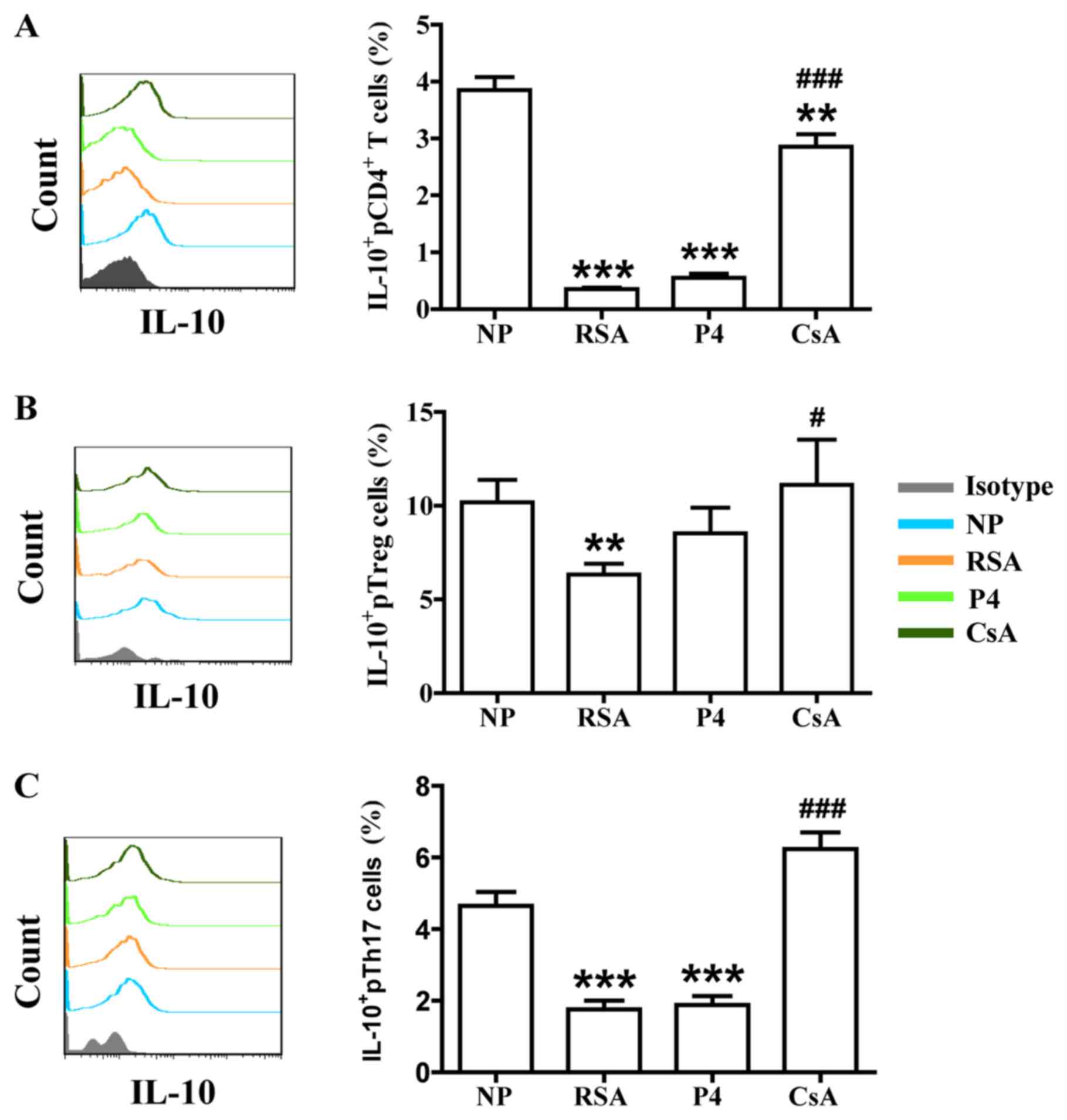 | Figure 3CsA promotes IL-10 expression in
peripheral blood cells of pregnant females with RSA. Compared with
that in the NP group, the production of IL-10 in (A)
CD4+ T cells, (B) Treg cells and (C) Th17 cells in the
peripheral blood of subjects in the RSA group was decreased. While
CsA promoted the production of IL-10, P4 had no effect on it.
Groups: NP, normal early pregnancy; RSA; patients with RSA; P4,
pregnant females with a history of RSA treated with P4; CsA,
pregnant females with a history of RSA treated with CsA.
**P<0.01, ***P<0.001 vs. NP;
#P<0.05, ###P<0.001 vs. RSA. CsA,
cyclosporin A; pTreg cells, peripheral T-regulatory cells; Th17
cells, type-17 T-helper cells; RSA, recurrent spontaneous abortion;
P4, progesterone; IL, interleukin. |
Effects of CsA and P4 on CTLA-4, Tim-3
and PD-1 expression in peripheral blood cells of pregnant females
with a history of RSA
In addition to the signal from the T-cell receptor
complex after antigen recognition, T-cell activation requires a
second signal from co-signaling molecules. Recently, the role of
co-signaling molecules, particularly co-inhibitory molecules, in
maternal-fetal immunity has been explored (28). The effects of CsA and P4 on CTLA-4,
Tim-3 and PD-1 expression in the peripheral blood cells of pregnant
females were then assessed. As presented in Figs.
4-6, the patients in the RSA group demonstrated significantly
lower CTLA-4, Tim-3 and PD-1 expression in the peripheral blood
cells, but the expression of Tim-3 and PD-1 remained unchanged on
Th17 cells, compared with those in the NP group. CsA increased
CTLA-4 expression in total pCD4+ T cells, pTreg cells
and pTh17 cells, whereas P4 only promoted CTLA-4 expression in
total pCD4+ T cells and pTh17 cells of pregnant females
with a history of RSA (Fig. 4). CsA
and P4 increased Tim-3 expression on total pCD4+ T
cells, pTreg cells and pTh17 cells (Fig. 5). Furthermore, P4 increased PD-1
expression in pTreg cells, while CsA had no effect on PD-1
expression in peripheral blood cells (Fig. 6).
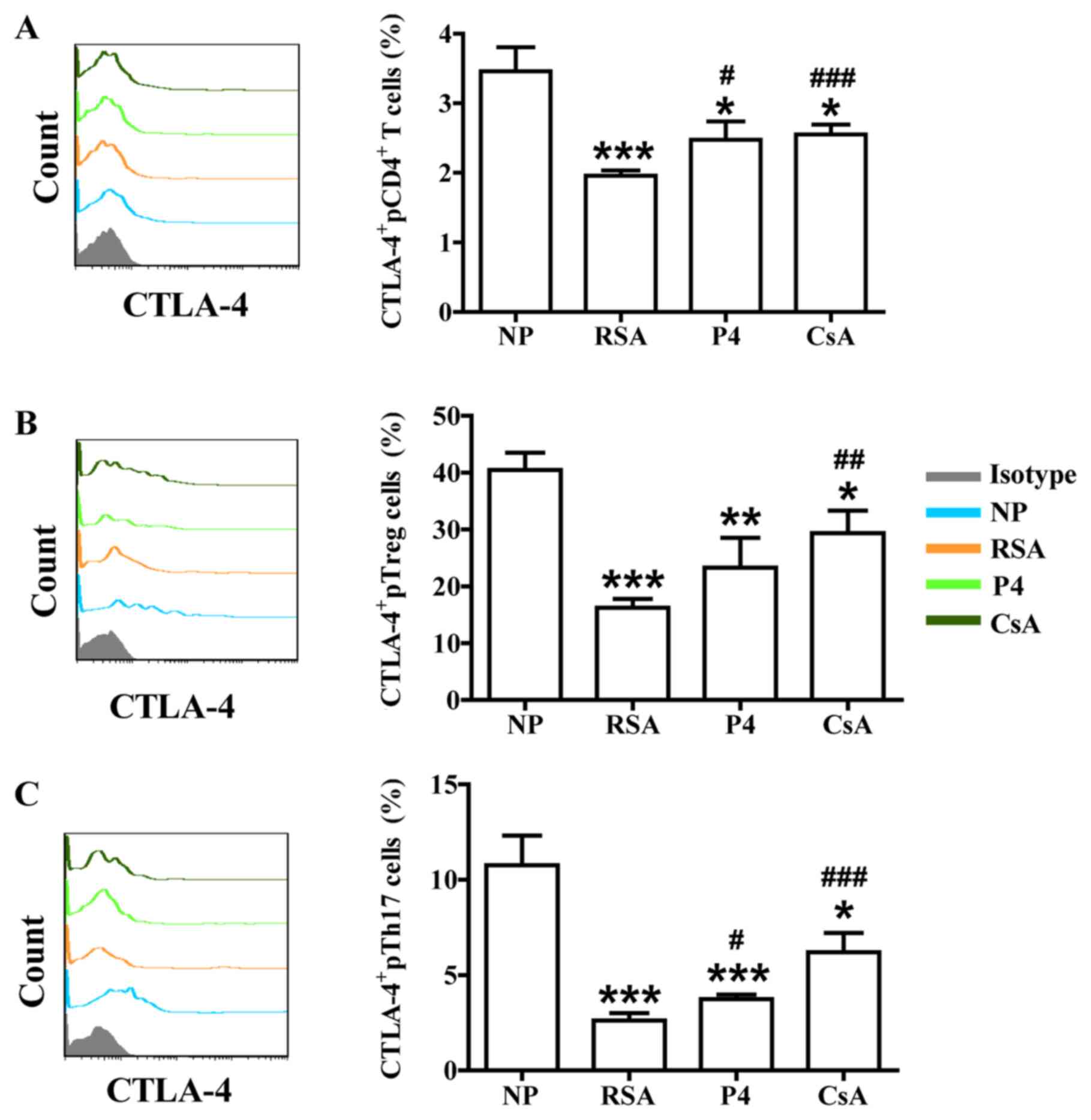 | Figure 4Effects of P4 and CsA on CTLA-4
expression in peripheral blood cells of pregnant females with a
history of RSA. Compared with that in the NP group, the production
of CTLA-4 in (A) CD4+ T cells, (B) Treg cells and (C)
Th17 cells in the peripheral blood of subjects in the RSA group was
decreased. CsA promoted the expression of CTLA-4 in all three
indicated subsets of T cells. P4 also promoted CTLA-4 expression in
total CD4+T and Th17 cells. Groups: NP, normal early
pregnancy; RSA; patients with RSA; P4, pregnant females with a
history of RSA treated with P4; CsA, pregnant females with a
history of RSA treated with CsA. *P<0.05,
**P<0.01, ***P<0.001 vs. NP;
#P<0.05, ##P<0.01,
###P<0.001 vs. RSA. CsA, cyclosporine A; pTreg cells,
peripheral T-regulatory cells; Th17 cells, type-17 T-helper cells;
RSA, recurrent spontaneous abortion; P4, progesterone; CTLA,
cytotoxic T-lymphocyte-associated protein 4. |
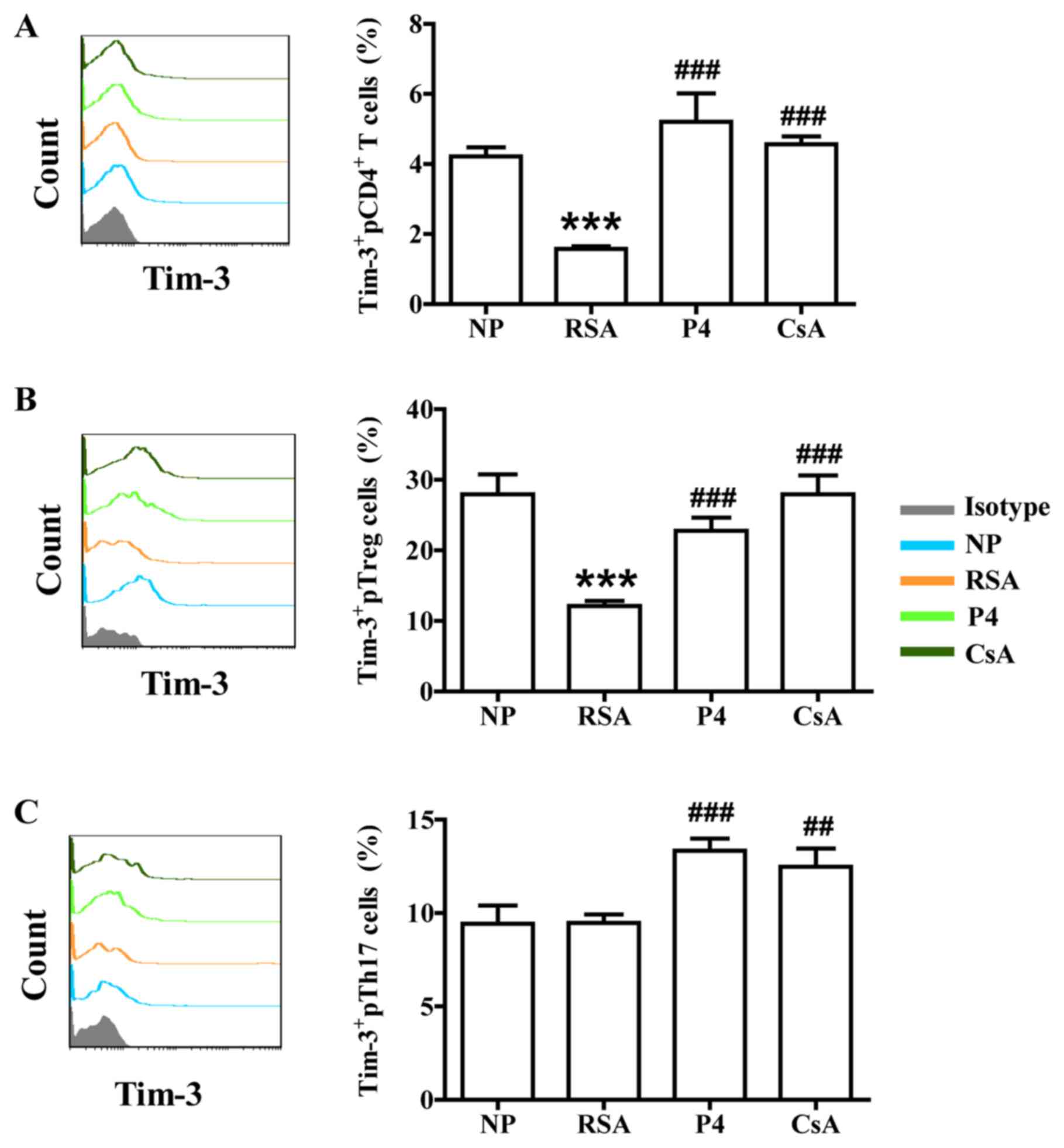 | Figure 5Effects of P4 and CsA on Tim-3
expression in peripheral blood cells of pregnant females with a
history of RSA. Compared with that in the NP group, the production
of Tim-3 in (A) CD4+ T cells and (B) Treg cells in the
peripheral blood of subjects in the RSA group was decreased. (C) In
Th17 cells in the peripheral blood, no significant difference in
Tim-3 expression between the RSA and NP group was determined. P4
and CsA promoted Tim-3 expression in all three indicated subsets of
T cells. Groups: NP, normal early pregnancy; RSA; patients with
RSA; P4, pregnant females with a history of RSA treated with P4;
CsA, pregnant females with a history of RSA treated with CsA.
***P<0.001 vs. NP; ##P<0.01,
###P<0.001 vs. RSA. CsA, cyclosporine A; pTreg cells,
peripheral T-regulatory cells; Th17 cells, type-17 T-helper cells;
RSA, recurrent spontaneous abortion; P4, progesterone; TIM-3,
T-cell immunoglobulin mucin family member-3. |
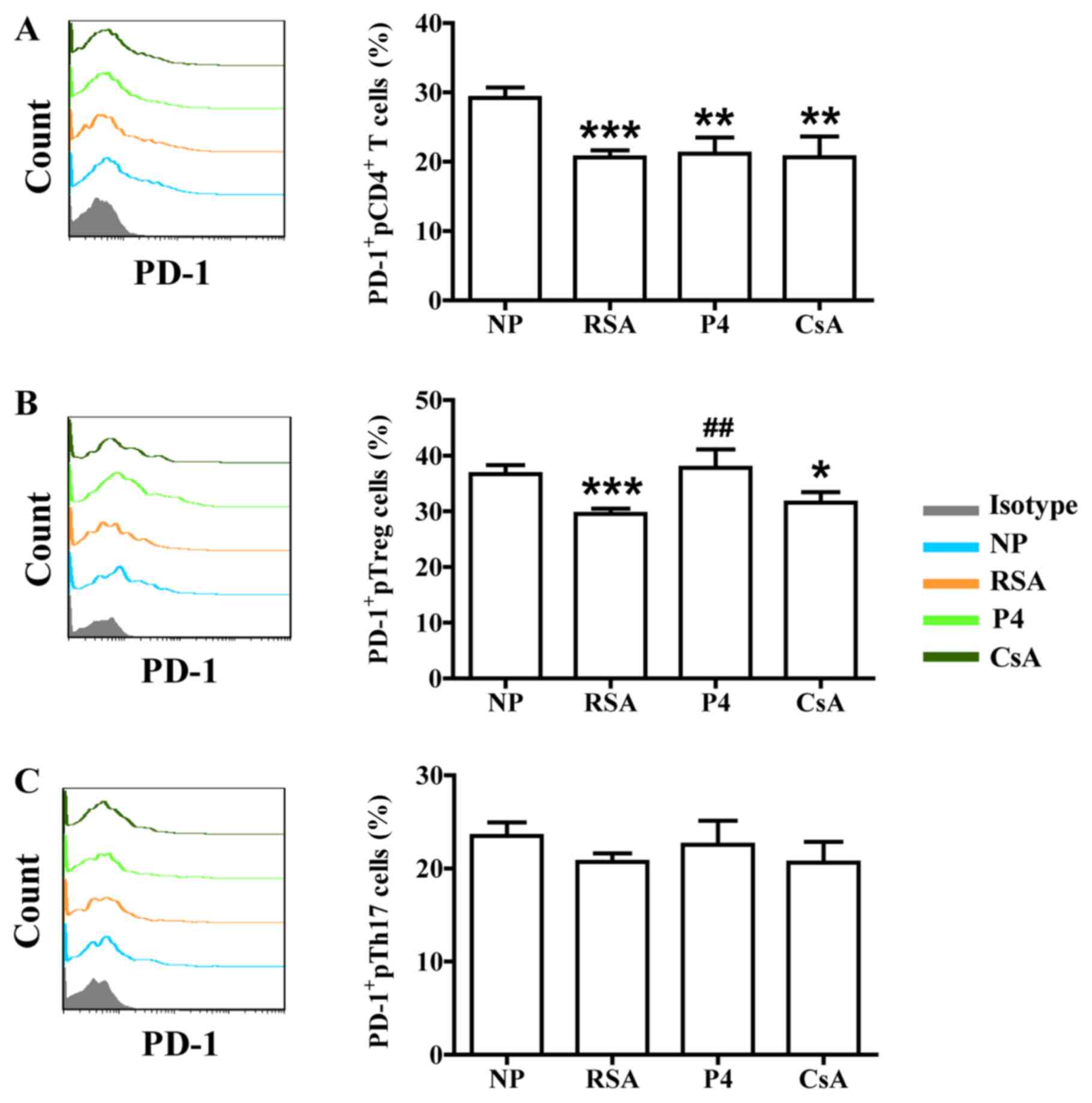 | Figure 6Effects of P4 and CsA on PD-1
expression in peripheral blood cells of pregnant females with a
history of RSA. Compared with that in the NP group, the production
of PD-1 in (A) CD4+ T cells and (B) Treg cells in the
peripheral blood of subjects in the RSA group was decreased. (C) In
Th17 cells in the peripheral blood, no significant difference in
PD-1 expression between the RSA and NP group was determined. While
P4 and CsA had no effects on PD-1 expression in total
CD4+ T cells and Th17 cells, P4 promoted PD-1 expression
in Treg cells. Groups: NP, normal early pregnancy; RSA; patients
with RSA; P4, pregnant females with a history of RSA treated with
P4; CsA, pregnant females with a history of RSA treated with CsA.
*P<0.05,**P<0.01,
***P<0.001 vs. NP; ##P<0.01 vs. RSA.
CsA, cyclosporine A; pTreg cells, peripheral T-regulatory cells;
Th17 cells, type-17 T-helper cells; RSA, recurrent spontaneous
abortion; P4, progesterone; PD-1, programmed cell death-1. |
Discussion
As a semi-allograft, the human fetus is
antigenically foreign to the mother. Accordingly, a successful
pregnancy relies on the fine maternal-fetal immune balance between
immune tolerance, allowing allogeneic fetal trophoblasts to invade
maternal tissues and immune defense against a variety of pathogens.
Disruption of this immune balance is thought to be associated with
several pregnancy-associated complications, including RSA,
preeclampsia and fetal intrauterine growth restriction (2). The present study also confirmed that
imbalance of Th17/Treg cells and associated molecule is linked to
RSA.
P4, the traditional treatment for RSA, inhibits
uterine contraction and improves luteal-phase support and
utero-placental circulation (29).
Chien et al (30) indicated
that P4 may also regulate immunity and inhibit T-cell activation
through a non-classical steroid receptor pathway during pregnancy.
In early 1995, Piccinni et al (31) proposed that P4 was beneficial to Th2
differentiation of CD4+ T cells. Furthermore, Mjosberg
et al (32) revealed that P4
regulated Treg-cell functions in human pregnancy, while Lee et
al (33) reported that P4
inhibited Th17-cell differentiation and reduced the expression of
associated functional molecules, including IL-17A. However, the
present study revealed no significant differences in the proportion
of Treg and Th17 cells in the peripheral blood between the P4 and
RSA groups. This may be due to differences in the gestational
stages tested and the fact that certain studies were performed
using established cell clones.
While certain studies have suggested the involvement
of Th17 cells in pregnancy-associated pathologies (34), a study by our group (35) and Wu et al (36) suggested that Th17 cells serve
important roles in regulating trophoblast function. It has also
been indicated that not all Th17 cells are pro-inflammatory, given
that Th17 subpopulations with diverse functions may exist (37). IL-10 has been previously associated
with non-pathogenic Th17 cells (38), while TGF-β1 may be produced mainly
by Th17 cells (39). Although P4
had no effect on IL-10 expression in all three indicated subsets of
T cells and TGF-β1 expression in pCD4+ T cells and pTreg
cells, it significantly increased the expression of TGF-β1 and
CTLA-4 in pCD4+ T cells and pTh17 cells, as well as on
Tim-3 expression in all three indicated subsets of T cells and PD-1
expression in pTreg cells. As co-stimulatory signals have important
roles in T-cell function and pregnancy maintenance (18,28),
despite the lack of evidence regarding improved outcomes following
first-trimester progesterone therapy in females with a history of
RSA (40,41), the results of the present study
suggested that P4 may also have an immunomodulatory role through
certain co-inhibitory molecules (including Tim-3, PD-1 and CTLA-4)
in the treatment of RSA.
The observed association between immunologic
abnormalities and RSA has led to the development and use of various
types of immune therapy with the objective of restoring normal
immune homeostasis during pregnancy. CsA is a previously known
immunosuppressive drug that has been used for the treatment of RSA
based on previous studies (27,42-48).
Previous studies report that CsA: i) Induced Th2 dominance and
Treg-cell proliferation during the implantation window and
significantly reduced the embryo absorption rate (27,42);
ii) downregulated CD28 expression at the maternal-fetal interface
and upregulated CTLA-4 expression in abortion-prone mice (43); iii) improved adhesion and invasion
of mouse preimplantation embryos (44); and iv) promoted trophoblastic
invasion and proliferation at low dosages (0.0001-1 µmol/l)
(45,46). Small-scale clinical observations
(47,48), in addition to unpublished data by
our group, have indicated that CsA significantly increased the live
birth rate in cases of RSA without increasing complications during
pregnancy and among neonates.
The present study suggested that CsA reduced the
proportion of Th17 cells and promoted Treg-cell dominance among
pregnant females with a history of RSA. CsA decreased the
production of IL-17A (the major effector cytokine of Th17 cells)
and also upregulated the expression of TGF-β1, IL-10, CTLA-4 and
Tim-3. These results suggest that CsA, as a trophoblast function
promoter, also restores the Th17/Treg-cell balance, while inducing
Th2 bias during pregnancy. Accordingly, future research group will
be aimed at studying the effect of P4 and CsA on other
pro-inflammatory cytokines in Th17 cells, including IL-6, IL-21 and
IL-23. Further investigations are required to explore whether
non-pathogenic Th17 subsets and pro-inflammatory Th17
subpopulations co-exist at the maternal-fetal interface, and which
mechanisms may be used to modulate Th17 subsets during
pregnancy.
To date, RSA with its underlying causes and
mechanisms has remained to be fully elucidated. Studies have
indicated that the more abortions occur, the higher the likelihood
of abortion during the next pregnancy. For instance, after two
spontaneous abortions, the risk of spontaneous abortion during the
third pregnancy is ~30%, whereas after >3 spontaneous abortions,
the risk of spontaneous abortion during the next pregnancy maybe as
high as 45% (49). Early diagnosis
and treatment of RSA has been of great significance to families.
Although previous studies have focused on the maternal-fetal
interface, non-invasive examination is of great importance in
clinical practice. The present study investigated the imbalance
between Th17 and Treg cells in the peripheral blood to improve the
current understanding of the pathogenesis of RSA. The results
confirmed that the percentage of Treg cells and the expression of
TGF-β1, IL-10, CTLA-4 and Tim-3 decreased in the peripheral blood
of RSA patients, which may provide an experimental basis for
non-invasive monitoring indicators of pregnancy. However, while the
experiments were performed using flow cytometry with PMA
stimulation, determining the serum levels of cytokines in
peripheral blood or cytokine production in different T-cell
subpopulations through ELISA or PCR may have been more
representative of the in vivo situation. Of course, further
follow-up and larger-scale studies are required to confirm whether
such molecules maybe used as monitoring indicators of pregnancy.
The present results revealed that, while CsA reduced the proportion
of Th17 cells and promoted Treg-cell dominance, P4 may also have an
immunomodulatory role through certain co-inhibitory molecules to
exert its treatment effect in RSA. However, the small sample size
and lack of follow-up of pregnancy outcomes have limited the
assessment of the effects of P4 and CSA on fetal protection in the
present study. However, follow up of the subjects of the present
study regarding pregnancy outcomes will continue and, in the
future, the sample size will be expanded.
Acknowledgements
Not applicable.
Funding
The present study was supported by grant from the
Nature Science Foundation from the National Nature Science
Foundation of China (grant nos. 31700799 to SCW, 81630036, 91542116
and 31570920 to MRD, and 81490744 to DJL), the National Basic
Research Program of China (grant no. 2015CB943300 to DJL and MRD),
the National Key R&D Program of China (grant no. 2017YFC1001403
to DJL and MRD), the Program of Shanghai Academic/Technology
Research Leader (grant no. 17XD1400900 to MRD), the
Innovation-oriented Science and Technology Grant from NPFPC Key
Laboratory of Reproduction Regulation (grant no. CX2017-2 to MRD),
the Shanghai Sailing Program (grant no. 17YF1411600 to SCW), the
Training Program for Young Talents of Shanghai Health System (grant
no. 2018YQ07 to SCW), the Development Fund of Shanghai Talents
(grant no. 2018110 to SCW) and the Shanghai Chenguang Program
(grant no. 18CG09 to SCW).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
SCW and MDL carried out the experiments. SCW, DJL
and MRD conceived experiments and analyzed data. MDL, CQC, FRS, JFY
and JFQ coordinated the sample collection, data interpretation,
literature search, and figure preparation. JFQ and SCW drafted the
manuscript. MRD revised the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Approval of the present study was obtained from the
ethics committee of the Obstetrics and Gynecology Hospital of Fudan
University (Shanghai, China) and all subjects provided written
informed consent.
Patient consent for publication
All subjects provided written informed consent for
the publication of associated data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rai R and Regan L: Recurrent miscarriage.
Lancet. 368:601–611. 2006.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Arck PC and Hecher K: Fetomaternal immune
cross-talk and its consequences for maternal and offspring's
health. Nat Med. 19:548–556. 2013.PubMed/NCBI View
Article : Google Scholar
|
|
3
|
Zeng W, Liu Z, Liu X, Zhang S, Khanniche
A, Zheng Y, Ma X, Yu T, Tian F, Liu XR, et al: Distinct
transcriptional and alternative splicing signatures of decidual
CD4+ T cells in early human pregnancy. Front Immunol.
8(682)2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Lash GE, Otun HA, Innes BA, Kirkley M, De
Oliveira L, Searle RF, Robson SC and Bulmer JN: Interferon-gamma
inhibits extravillous trophoblast cell invasion by a mechanism that
involves both changes in apoptosis and protease levels. FASEB J.
20:2512–2518. 2006.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Chaouat G: The Th1/Th2 paradigm: Still
important in pregnancy? Semin Immunopathol. 29:95–113.
2007.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Wegmann TG, Lin H, Guilbert L and Mosmann
TR: Bidirectional cytokine interactions in the maternal-fetal
relationship: Is successful pregnancy a TH2 phenomenon? Immunol
Today. 7:353–356. 1993.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Crome SQ, Wang AY and Levings MK:
Translational mini-review series on Th17 Cells: Function and
regulation of human T helper 17 cells in health and disease. Clin
Exp Immunol. 159:109–119. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Jutel M, Akdis M, Budak F,
Aebischer-Casaulta C, Wrzyszcz M, Blaser K and Akdis CA: IL-10 and
TGF-beta cooperate in the regulatory T cell response to mucosal
allergens in normal immunity and specific immunotherapy. Eur J
Immunol. 33:1205–1214. 2003.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Sheu A, Chan Y, Ferguson A, Bakhtyari MB,
Hawke W, White C, Chan YF, Bertolino PJ, Woon HG, Palendira U, et
al: A proinflammatory CD4+ T cell phenotype in
gestational diabetes mellitus. Diabetologia. 61:1633–1643.
2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Muyayalo KP, Li ZH, Mor G and Liao AH:
Modulatory effect of intravenous immunoglobulin on Th17/Treg cell
balance in women with unexplained recurrent spontaneous abortion.
Am J ReprodImmunol. 80(e13018)2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Hosseini A, Dolati S, Hashemi V,
Abdollahpour-Alitappeh M and Yousefi M: Regulatory T and T helper
17 cells: Their roles in preeclampsia. J Cell Physiol.
233:6561–6573. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Game DS and Lechler RI: Pathways of
allorecognition: Implications for transplantation tolerance.
Transpl Immunol. 10:101–108. 2002.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Khoury SJ and Sayegh MH: The roles of the
new negative T cell costimulatory pathways in regulating
autoimmunity. Immunity. 20:529–538. 2004.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Cooksley H, Riva A, Katzarov K,
Hadzhiolova-Lebeau T, Pavlova S, Simonova M, Williams R and Chokshi
S: Differential expression of immune inhibitory checkpoint
signatures on antiviral and inflammatory T cell populations in
chronic hepatitis B. J Interferon Cytokine Res. 38:273–282.
2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Zhao J, Lin B, Deng H, Zhi X, Li Y, Liu Y,
Bible PW, Li Q, Xu B, Wei L, et al: Decreased expression of TIM-3
on Th17 cells associated with ophthalmopathy in patients with
Graves' disease. Curr Mol Med. 18:83–90. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Wei CB, Tao K, Jiang R, Zhou LD, Zhang QH
and Yuan CS: Quercetin protects mouse liver against
triptolide-induced hepatic injury by restoring Th17/Treg balance
through Tim-3 and TLR4-MyD88-NF-κB pathway. Int Immunopharmacol.
53:73–82. 2017.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Zhang Y, Liu Z, Tian M, Hu X, Wang L, Ji J
and Liao A: The altered PD-1/PD-L1 pathway delivers the ‘one-two
punch’ effects to promote the Treg/Th17 imbalance in pre-eclampsia.
Cell Mol Immunol. 15:710–723. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
D'Addio F, Riella LV, Mfarrej BG, Chabtini
L, Adams LT, Yeung M, Yagita H, Azuma M, Sayegh MH and Guleria I:
The link between the PDL1 costimulatory pathway and Th17 in
fetomaternal tolerance. J Immunol. 187:4530–4541. 2011.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Liao H, Peng X, Gan L, Feng J, Gao Y, Yang
S, Hu X, Zhang L, Yin Y, Wang H and Xu X: Protective regulatory T
cell immune response induced by intranasal immunization with the
live-attenuated pneumococcal vaccine SPY1 via the transforming
growth factor-β1-Smad2/3 pathway. Front Immunol.
9(1754)2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kawai K, Uchiyama M, Hester J, Wood K and
Issa F: Regulatory T cells for tolerance. Hum Immunol. 79:294–303.
2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Gupta S, Thornley TB, Gao W, Larocca R,
Turka LA, Kuchroo VK and Strom TB: Allograft rejection is
restrained by short-lived TIM-3+PD-1+Foxp3+ tregs. J Clin Invest.
122:2395–2404. 2012.PubMed/NCBI View
Article : Google Scholar
|
|
22
|
Wang S, Zhu X, Xu Y, Zhang D, Li Y, Tao Y,
Piao H, Li D and Du M: Programmed cell death-1 (PD-1) and T-cell
immunoglobulin mucin-3 (Tim-3) regulate CD4+ T cells to induce type
2 helper T Cell (Th2) bias at the maternal-fetal interface. Hum
Reprod. 31:700–711. 2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Wang S, Chen C, Li M, Qian J, Sun F, Li Y,
Yu M, Wang M, Zang X, Zhu R, et al: Blockade of CTLA-4 and Tim-3
pathways induces fetal loss with altered cytokine profiles by
decidual CD4+ T cells. Cell Death Dis.
10(15)2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Spencer TE and Bazer FW: Biology of
progesterone action during pregnancy recognition and maintenance of
pregnancy. Front Biosci. 7:d1879–d1898. 2002.PubMed/NCBI View
Article : Google Scholar
|
|
25
|
Arck P, Hansen PJ, Mulac Jericevic B,
Piccinni MP and Szekeres-Bartho J: Progesterone during pregnancy:
Endocrine-immune cross talk in mammalian species and the role of
stress. Am J Reprod Immunol. 58:268–279. 2007.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Sketris I, Yatscoff R, Keown P, Canafax
DM, First MR, Holt DW, Schroeder TJ and Wright M: Optimizing the
use of cyclosporine in renal transplantation. Clin Biochem.
28:195–211. 1995.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Du MR, Dong L, Zhou WH, Yan FT and Li DJ:
Cyclosporin a improves pregnancy outcome by promoting functions of
trophoblasts and inducing maternal tolerance to the allogeneic
fetus in abortion-prone matings in the mouse. Biol Reprod.
76:906–914. 2007.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Xu YY, Wang SC, Li DJ and Du MR:
Co-signaling molecules in maternal-fetal immunity. Trends Mol Med.
23:46–58. 2017.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Di Renzo GC, Giardina I, Clerici G, Brillo
E and Gerli S: Progesterone in Normal and Pathological Pregnancy.
Horm Mol Biol Clin Investig. 27:35–48. 2016.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Chien EJ, Chang CP, Lee WF, Su TH and Wu
CH: Non-genomic immunosuppressive actions of progesterone inhibits
PHA-induced alkalinization and activation in T cells. J Cell
Biochem. 99:292–304. 2006.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Piccinni MP, Giudizi MG, Biagiotti R,
Beloni L, Giannarini L, Sampognaro S, Parronchi P, Manetti R,
Annunziato F, Livi C, et al: Progesterone favors the development of
human T helper cells producing Th2-type cytokines and promotes both
IL-4 production and membrane CD30 expression in established Th1
cell clones. J Immunol. 155:128–133. 1995.PubMed/NCBI
|
|
32
|
Mjosberg J, Svensson J, Johansson E,
Hellström L, Casas R, Jenmalm MC, Boij R, Matthiesen L, Jönsson JI,
Berg G and Ernerudh J: Systemic reduction of functionally
suppressive CD4dimCD25highFoxp3+ Tregs in human second trimester
pregnancy is induced by progesterone and 17beta-estradiol. J
Immunol. 183:759–769. 2009.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Lee JH, Ulrich B, Cho J, Park J and Kim
CH: Progesterone promotes differentiation of human cord blood fetal
T cells into T regulatory cells but suppresses their
differentiation into Th17 cells. J Immunol. 187:1778–1787.
2011.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Fu B, Tian Z and Wei H: TH17 Cells in
human recurrent pregnancy loss and pre-eclampsia. Cell Mol Immunol.
11:564–570. 2014.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Wang S, Qian J, Sun F, Li M, Ye J, Li M,
Du M and Li D: Bidirectional regulation between 1st trimester
HTR8/SVneo trophoblast cells and in vitro differentiated Th17/Treg
cells suggest a fetal-maternal regulatory loop in human pregnancy.
Am J Reprod Immunol. 81(e13106)2019.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Wu HX, Jin LP, Xu B, Liang SS and Li DJ:
Decidual stromal cells recruit Th17 cells into decidua to promote
proliferation and invasion of human trophoblast cells by secreting
IL-17. Cell Mol Immunol. 11:253–262. 2014.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Lee Y, Awasthi A, Yosef N, Quintana FJ,
Xiao S, Peters A, Wu C, Kleinewietfeld M, Kunder S, Hafler DA, et
al: Induction and molecular signature of pathogenic TH17 cells. Nat
Immunol. 13:991–999. 2012.PubMed/NCBI View Article : Google Scholar
|
|
38
|
McGeachy MJ, Bak-Jensen KS, Chen Y, Tato
CM, Blumenschein W, McClanahan T and Cua D: TGF-beta and IL-6 drive
the production of IL-17 and IL-10 by T cells and restrain T(H)-17
cell-mediated pathology. Nat Immunol. 8:1390–1397. 2007.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Gutcher I, Donkor MK, Ma Q, Rudensky AY,
Flavell RA and Li MO: Autocrine transforming growth factor-β1
promotes in vivo Th17 cell differentiation. Immunity. 34:396–408.
2011.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Coomarasamy A, Williams H, Truchanowicz E,
Seed PT, Small R, Quenby S, Gupta P, Dawood F, Koot YE, Bender Atik
R, et al: A randomized trial of progesterone in women with
recurrent miscarriages. N Engl J Med. 373:2141–2148.
2015.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Coomarasamy A, Williams H, Truchanowicz E,
Seed PT, Small R, Quenby S, Gupta P, Dawood F, Koot YE, Atik RB, et
al: PROMISE: First-trimester progesterone therapy in women with a
history of unexplained recurrent miscarriages-a randomised,
double-blind, placebo-controlled, international multicentre trial
and economic evaluation. Health Technol Assess. 20:1–92.
2016.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Piao HL, Wang SC, Tao Y, Zhu R, Sun C, Fu
Q, Du MR and Li DJ: Cyclosporine A enhances Th2 bias at the
maternal-fetal interface in early human pregnancy with aid of the
interaction between maternal and fetal cells. PLoS One.
7(e45275)2012.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Zhou WH, Dong L, Du MR, Zhu XY and Li DJ:
Cyclosporin a improves murine pregnancy outcome in abortion-prone
matings: Involvement of CD80/86 and CD28/CTLA-4. Reproduction.
135:385–395. 2008.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Huang Y, Ma Y, Ma L, Mao JL, Zhang Y, Du
MR and Li DJ: Cyclosporine A improves adhesion and invasion of
mouse preimplantation embryos via upregulating integrin β3 and
matrix metalloproteinase-9. Int J Clin Exp Patho. 7:1379–1388.
2014.PubMed/NCBI
|
|
45
|
Du MR, Zhou WH, Yan FT, Zhu XY, He YY,
Yang JY and Li DJ: Cyclosporine A induces titin expression via
MAPK/ERK signalling and improves proliferative and invasive
potential of human trophoblast cells. Hum Reprod. 22:2528–2537.
2007.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Zhou WH, Du MR, Dong L, Zhu XY, Yang JY,
He YY and Li DJ: Cyclosporina increases expression of matrix
metalloproteinase 9 and 2 and invasiveness in vitro of the
first-trimester human trophoblast cells via the mitogen-activated
protein kinase pathway. Hum Reprod. 22:2743–2750. 2007.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Fu JH: Analysis of the use of cyclosporina
to treat refractory immune recurrent spontaneous abortion. Clin Exp
Obstet Gynecol. 42:739–742. 2015.PubMed/NCBI
|
|
48
|
Ling Y, Huang Y, Chen C, Mao J and Zhang
H: Low dose cyclosporin a treatment increases live birth rate of
unexplained recurrent abortion-initial cohort study. Clin Exp
Obstet Gynecol. 44:230–235. 2017.PubMed/NCBI
|
|
49
|
Martínez-Zamora MÁ, Cervera R and Balasch
J: Recurrent miscarriage, antiphospholipid antibodies and the risk
of thromboembolic disease. Clin Rev Allergy Immunol. 43:265–274.
2012.PubMed/NCBI View Article : Google Scholar
|














