Introduction
Esophageal atresia (EA) is a congenital malformation
characterized by a gap in the esophagus, which ends in a closed
pouch and is not able to deliver food or saliva to the stomach.
Most commonly, instead of a simple disruption, the defect presents
as an abnormal connection between the esophagus and the trachea
known as a tracheoesophageal fistula (TOF) (1). EA with or without TOF remains the most
common congenital anomaly of the esophagus, and approximately half
of the affected fetuses present associated complications on the
vertebrae, heart, kidneys, limbs and the digestive or urinary
systems (2). It has a prevalence of
~2.44 per 10,000 births according to the pooled analysis of 18
international birth defect surveillance programs (3).
Improvements achieved in the survival of patients
with EA (~90%) can be largely attributed to advances in neonatal
intensive care, including prompt surgical interventions, which in
turn depend on early diagnosis (4).
EA is most commonly diagnosed during the first 24 h of life, but
may also be detected at other times either pre- or postnatally
(5,6). At birth, pediatricians check the
patency of the newborn's esophagus by carefully introducing a
nasogastric probe into the stomach. In cases of atresia, it is not
possible to advance the probe more than a few centimeters into the
esophagus; however, visualization of the malformation per se
and determination of the type and location of any tracheoesophageal
fistulas require radiography of the abdomen. The diagnosis of EA is
rarely confirmed before birth as it requires the use of other
approaches, such as ultrasound, amniotic fluid analysis or nuclear
magnetic resonance imaging (MRI) to study the organs in more detail
(6).
Esophageal defects are typically located at the
level of the cervicothoracic junction, and assessing this
particular area of interest is challenging due to the shadow cones
generated by bony structures, including the dorsal cervical spine
and clavicles. Routine ultrasound examinations are not able to
present the normal esophagus because of the similarity of its
collapsed lumen and tissue textures with those of surrounding
organs. Hence, ultrasound alone has been considered an
unsatisfactory diagnostic tool for the identification of EA
prenatally due to a high rate of false-positive diagnoses; however,
a suspicious ultrasound is recommended as a first-line requirement
prior to MRI or amniotic fluid analysis, which have high diagnostic
accuracies for EA (7). Accordingly,
the present study aimed to perform a methodological re-exploration
of the accuracy of ultrasonographic features for the prenatal
diagnosis of esophageal atresia and tracheoesophageal fistula.
High-performance ultrasound with parasternal and para-aortic axis
longitudinal and transverse sections was used.
Materials and methods
Informed consent and ethical
approval
The Ethics Committee of the Affiliated Hospital of
Jining Medical University approved the study protocol (approval no.
JYFY-2019-17). All pregnant women gave their informed consent prior
to the examinations. The study was conducted following the tenets
of the Declaration of Helsinki.
Study design, setting and
participants
The study was prospectively conducted in the
Affiliated Hospital of Jining Medical University (Jining, China), a
public health institution of higher education learning in Shandong
province. The participants were recruited at the Affiliated
Hospital of Jining Medical University and local referral centers
from January 2014 to June 2018.
Inclusion criteria for the study were as follows:
Pregnant women whose fetuses were suspected of presenting with
EA/TOF based on high-performance ultrasonic detection, and an
amniotic fluid index >25 cm or a fetus with no or small stomach.
Patients who did not provide informed written consent were
excluded.
Study procedure
A GE Voluson E8 or E10 ultrasonic diagnostic
apparatus (GE Healthcare) with a probe frequency of 2.5-5.0 MHz was
used to perform the examinations. Following a routine fetal
ultrasound and biological measurements, longitudinal and transverse
views were used to continuously check the esophagus and trachea.
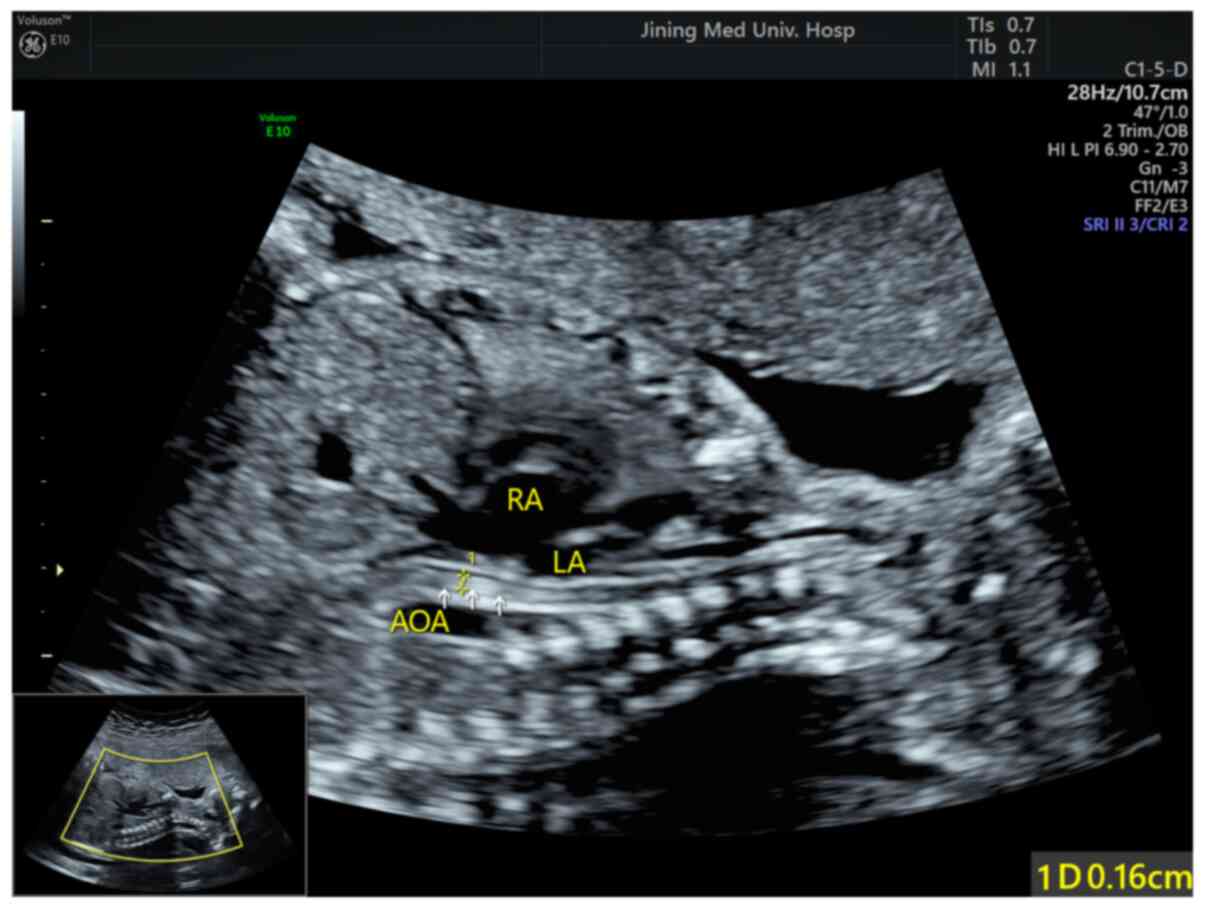
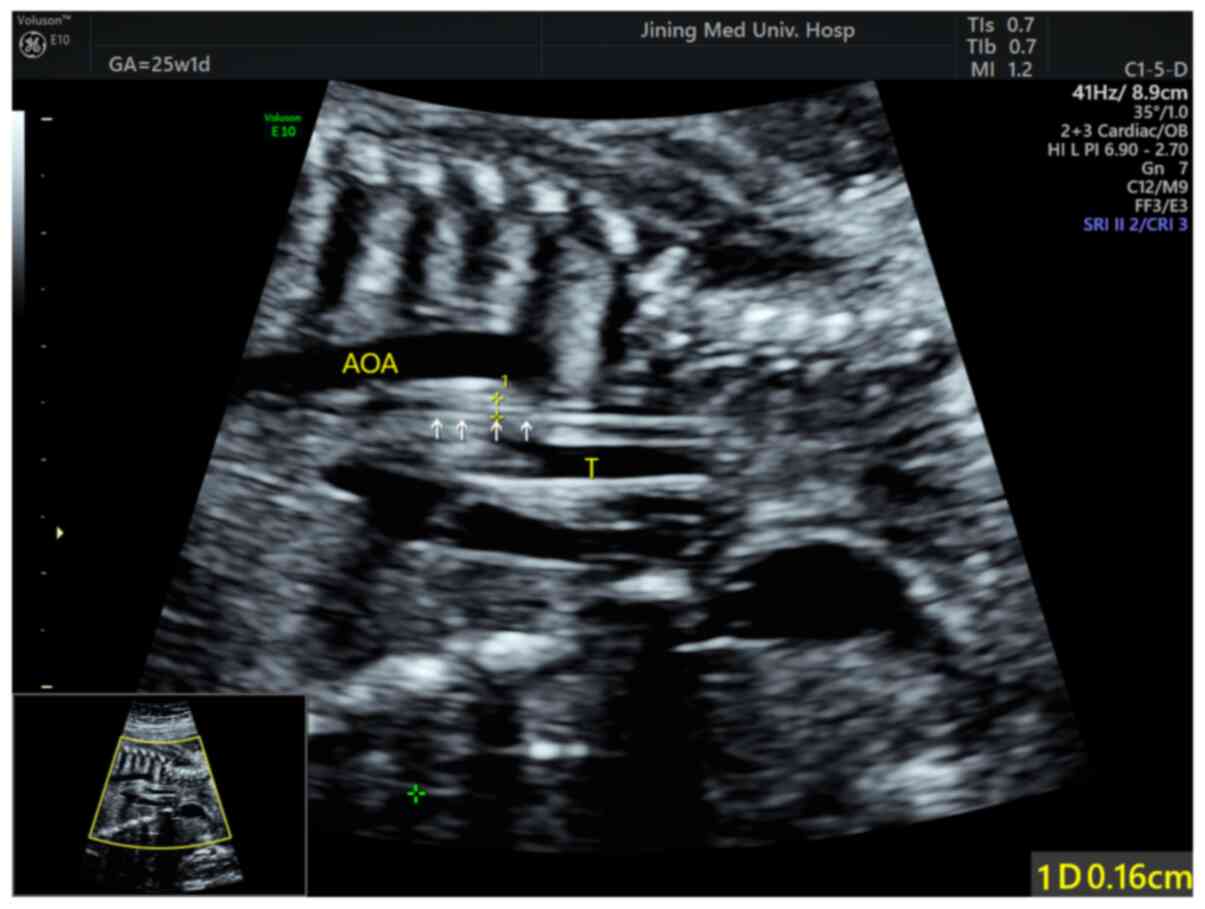
Esophageal and tracheal images were obtained from patients in the
supine position (Fig. 1) and prone
position (Figs. 2 and 3). The standard for esophageal soft tissue
thickening was considered to be that the thickness of the
esophagus, measured on both surfaces of the section, was larger
than the diameter at the beginning of the left subclavian artery
during the systolic period of the long axis of the aortic arch.
Partial echo interruption of the wall and esophageal
fistula were considered as screening indicators for suspected EA.
The cases were classified as presenting signs suspicious of EA
based on findings in the tracheal main bronchial tree (dilated
diameter of the tracheal main bronchial tree), the presence or
absence of TOF, the length of the atresia and other complications.
The shape of the esophagus was evaluated to assess the severity of
EA. Features of the suspected cases were compared with the results
of the postpartum autopsy, surgery or other examination results to
confirm the diagnosis and to assess the diagnostic accuracy of the
ultrasonographic method.
Statistical analysis
The data were analyzed using STATA software, version
14.2 (StataCorp LP). Continuous variables are presented as the mean
± standard deviation (SD). Categorical variables are presented as
proportions, with a 95% confidence interval (CI). Cohen's kappa
index was used to detect significant agreements between the
prenatal and postnatal diagnoses of EA/TOF. The diagnostic accuracy
of the prenatal ultrasonography was assessed by calculating the
sensitivity, specificity, positive predictive value and negative
predictive value based on the gold standard of postnatal
examination. In addition, positive and negative likelihood ratios
were calculated. A non-parametric estimation of the receiver
operating characteristic (ROC) curve was performed to obtain the
area under the curve (AUC).
Results
Prenatal ultrasound results
In total, 64 pregnant women were screened for
EA/TOF. The women were between 18 and 42 years old (mean ± SD,
33.24±3.22 years). The gestational age of the fetuses was between
16 and 40 weeks (mean ± SD, 26.33±3.57 weeks) (Table I). After obtaining esophageal images
through the longitudinal and/or para-aortic axis and transverse
sections with the high-frequency ultrasound (Fig. 1, Fig.
2 and 3), concordance was
observed between the prenatal and postnatal estimates of the
lengths of the esophageal defects
 | Table ICharacteristics of the study
participants (n=64). |
Table I
Characteristics of the study
participants (n=64).
| Characteristics | Data |
|---|
| Age of the mother,
years | 33.24±3.22 |
| Gestational age of
the fetus, weeks | 26.33±3.57 |
| EA/TOF incidence, n
(%) | |
|
Present | 34 (53.2) |
|
Absent | 30 (46.8) |
Among all the women screened, 16 were suspected of
carrying fetuses with EA/TOF during the prenatal ultrasonography.
In total, 34 cases of EA/TOF were confirmed among the 49 postnatal
examinations, which corresponded to an EA/TOF incidence of 53.2%
(95% CI, 40.2-65.7%). Among the remaining 15 fetuses, certain did
not exhibit symptoms for suspected EA, such as feeding difficulty,
vomiting or bucking, and the follow-up of certain fetuses was
lost.
Statistical analysis results
A weak agreement was detected between the results of
the prenatal and postnatal examinations (agreement, 53.2%; Cohen's
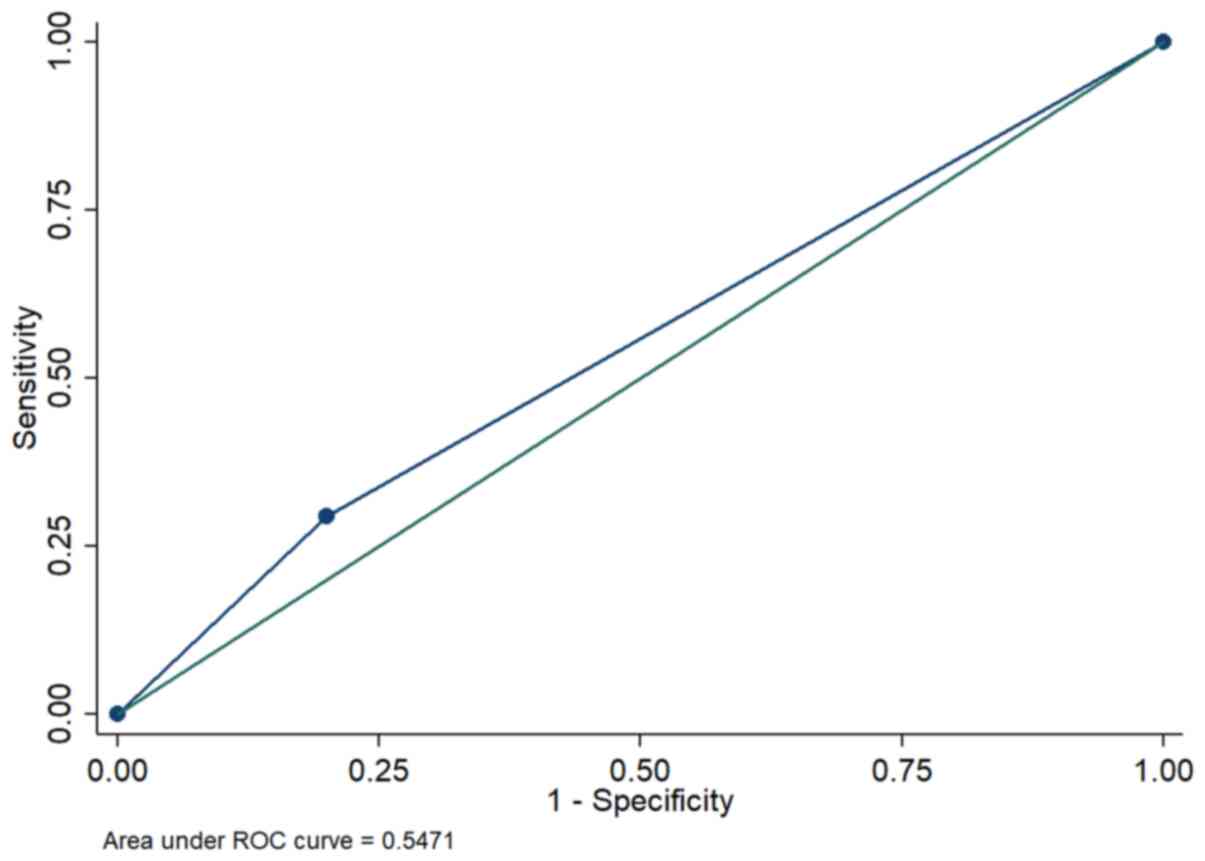
kappa=0.10, P=0.19). To determine the ability of prenatal
ultrasonography to correctly diagnose EA/TOF, its diagnostic
accuracy was determined using an ROC curve with postnatal
examination as the gold standard (Fig.
4). Table II shows the results
of the diagnostic accuracy test for prenatal ultrasonography. The
AUC was lower for prenatal ultrasonography compared with postnatal
diagnostic tests (AUC=0.55; 95% CI, 0.44-0.65).
| Table IIMeasurements of diagnostic accuracy
between prenatal ultrasonography and postnatal examinations
(n=64). |
Table II
Measurements of diagnostic accuracy
between prenatal ultrasonography and postnatal examinations
(n=64).
| Characteristics | Diagnostic accuracy
(95% CI) |
|---|
| Area under the
curve | 0.55 (0.44-0.65) |
| Sensitivity, % | 29.4 (15.1-47.5) |
| Specificity, % | 80 (61.4-92.3) |
| Positive predictive
value, % | 62.5 (35.4-82.8) |
| Negative predictive
value, % | 50 (35.2-64.8) |
| Positive likelihood
ratio | 1.47 (0.61-3.56) |
| Negative likelihood
ratio | 0.88 (0.67-1.17) |
In further analysis using postnatal examination as
the gold standard, prenatal ultrasonography was demonstrated to
have a sensitivity of 29.4% (95% CI, 15.1-47.5%), a specificity of
80% (95% CI, 61.4-92.3%), a positive predictive value of 62.5% (95%
CI, 35.4-82.8%) and a negative predictive value of 50% (95% CI,
35.2-64.8%). The positive likelihood ratio was 1.47 (95% CI,
0.61-3.56) and the negative likelihood ratio was 0.88 (95% CI,
0.67-1.17).
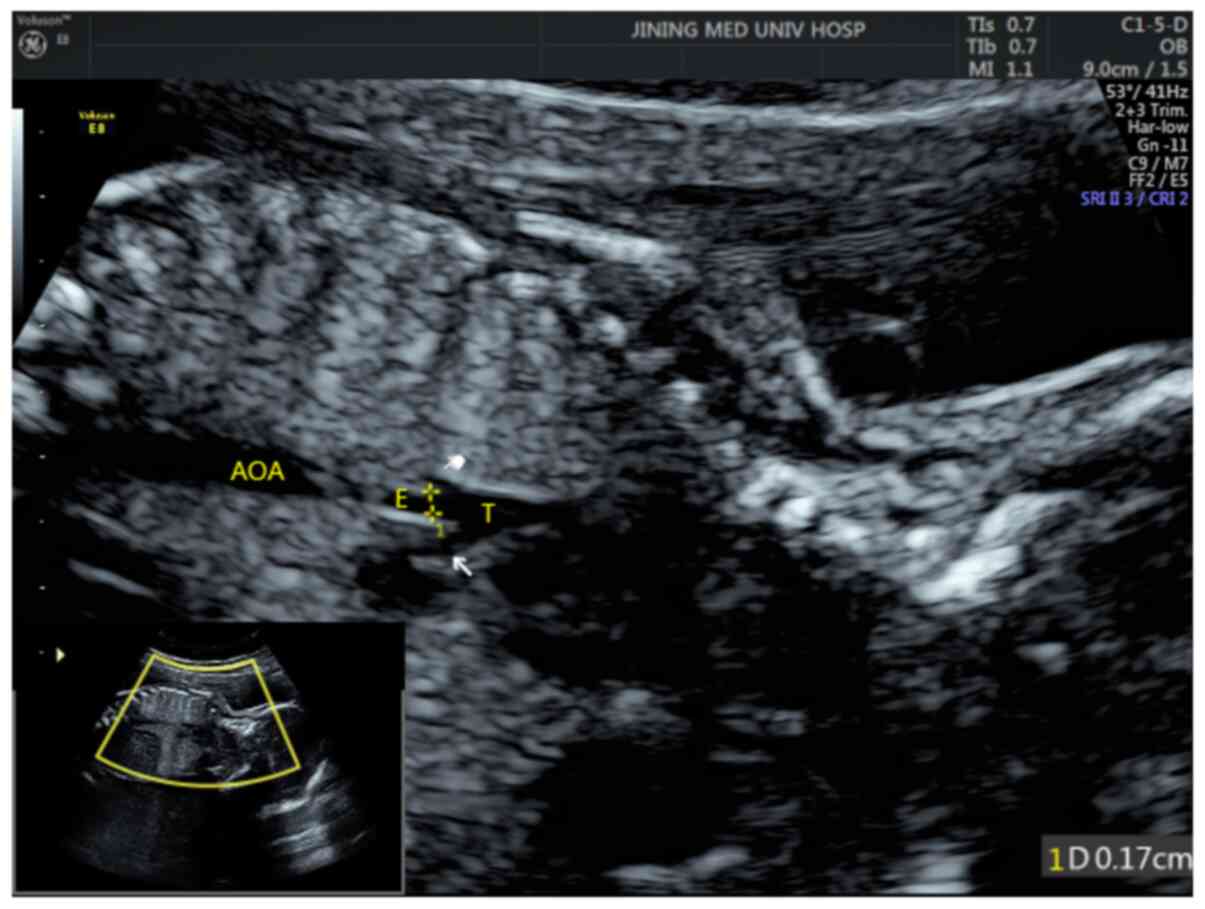
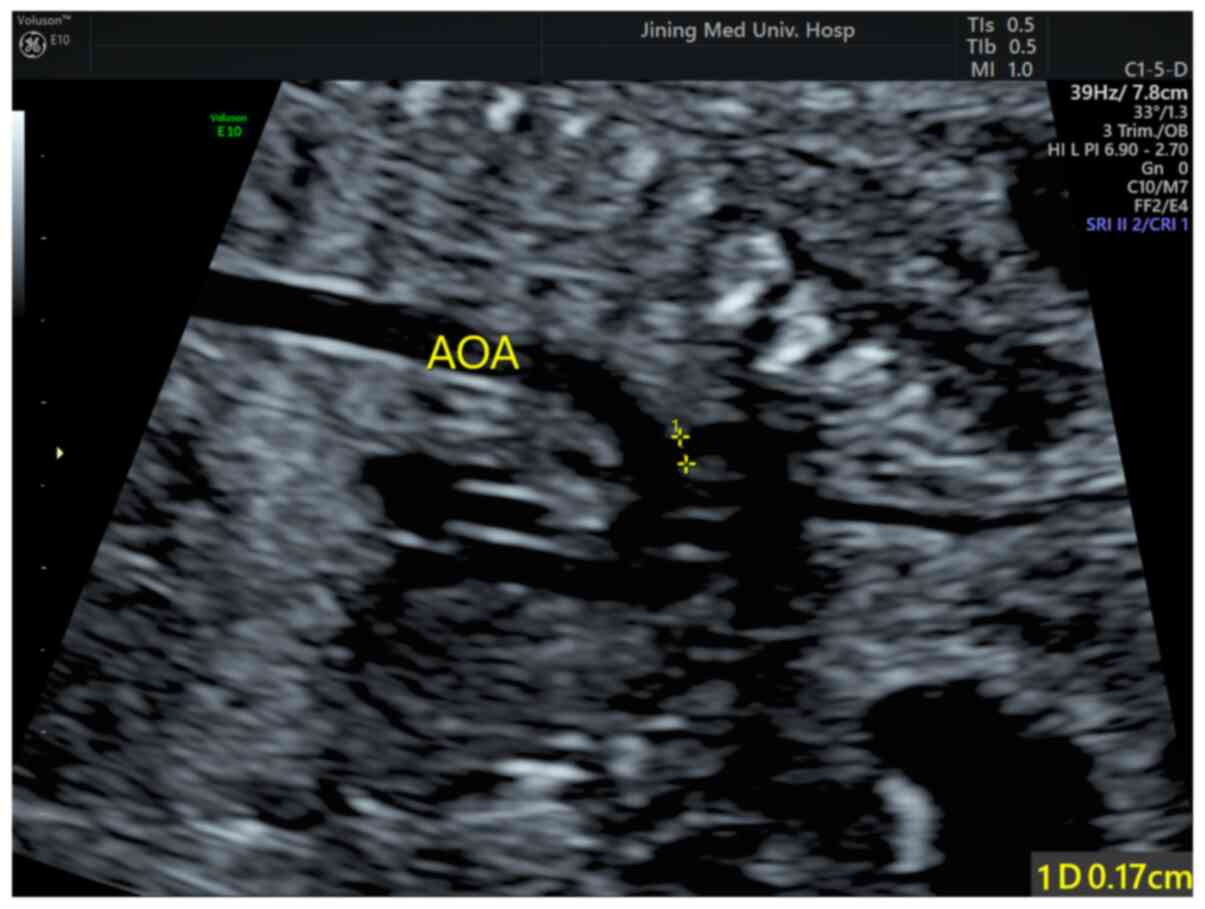
Ultrasonography revealed various changes in the
esophageal region of the fetuses. The main changes revealed by the
ultrasonography included thickened esophageal soft tissue (Fig. 5), a fistula between the esophagus
and trachea (Fig. 6) and changes in
the diameter at the beginning of the left subclavian artery
(Fig. 7). The diameter in the
beginning of the left subclavian artery was not altered. The
thickness of the esophageal soft tissue was compared with the
diameter in the beginning of the left subclavian artery. The
standard for esophageal soft tissue thickening was considered to be
that the thickness of the esophagus, measured on both surfaces of
the section, was larger than the diameter at the beginning of the
left subclavian artery during the systolic period of the long axis
of the aortic arch.
Discussion
Improving the diagnostic accuracy of prenatal EA
assessments is challenging due to the presence of associated
malformations and the limited visibility of the structures
(8,9). Therefore, the present study was
performed to assess the diagnostic accuracy of prenatal
ultrasonography for the identification of suspected EA/TOF.
A weak agreement was detected between the findings
of prenatal ultrasonography and postnatal examinations in patients
with EA/TOF. In addition, prenatal ultrasonography was demonstrated
to have poor sensitivity for the identification of EA/TOF and
moderate specificity for ruling them out. A similar study conducted
by Bradshaw et al (10) in
2016 also reported that prenatal ultrasonography has poor
sensitivity (<30%), but high specificity at 99%. The low
sensitivity may be attributed to the level of expertise of the
health professionals performing the procedure. The previous study
reported that the sensitivity of ultrasonography for the diagnosis
of EA/TOF increased by almost half when the procedure was performed
in a specialist center by professionals having a high level of
expertise (10). Another previous
study, a prospective study involving the examination of 60 fetuses
at 19-25 weeks of gestation, attempted to identify the rates of
visualization of the normal esophagus using a high-resolution
linear transducer. The study reported that complete visualization
of the normal esophagus was achieved in 86.7% of cases and at least
partial visualization was achieved in 96.7% of cases. The study
concluded that ultrasound alone is a poor diagnostic tool for the
identification of EA prenatally and has a high rate of
false-positive diagnoses (7).
However, other studies have also demonstrated that direct or
indirect sonographic assessments of the esophagus in fetuses
suspected of having EA improve the specificity of the diagnosis and
prenatal evaluation (11,12).
Despite their limitations, preoperative ultrasound
findings continue to serve a vital role in clinical practice as they
are necessary for planning the surgical strategy. A study conducted
by Su et al (11) in 2014
concluded that preoperative scan findings were useful in 25.0% of
patients. In their study, two infants were treated via a primary
cervical approach instead of a thoracotomy, and two infants who
were originally misdiagnosed due to stretched distal esophagi that
extended upward along the trachea into the proximal pouch did not
require any additional strategies.
Ultrasound technology lacks sensitivity for the
detection of EA/TOF, despite its usefulness for the prenatal
screening of other malformations, including congenital heart
disease, central nervous system anomalies, skeletal deformities and
gastrointestinal tract malformations such as a dilated cecum, which
is a potential ultrasound sign of fetal EA (13,14).
The present study has certain limitations. The study
population was relatively small and localized, so the results may
differ from those obtained in other populations or study settings.
However, the thorough statistical analysis of the diagnostic
accuracy of prenatal ultrasonography, the longitudinal nature of
the study, and the use of postnatal examination as a gold standard
are added strengths that improve its generalizability. Further
studies in other settings or regions are necessary to confirm the
findings of the present study. In addition, large-scale studies are
required to correctly determine the diagnostic accuracy and role of
prenatal ultrasonography in patients with EA/TOF.
The findings of the present study expand the limited
information available regarding the diagnostic accuracy of prenatal
ultrasonography and its application to fetuses with suspected
EA/TOF. The findings are also useful for informing clinicians about
the accuracy of prenatal ultrasonography for the screening and
early diagnosis of EA/TOF during the fetal stages. The information
obtained from a prenatal ultrasound may help clinicians to
formulate a plan for the management of fetuses with suspected
EA/TOF. However, since the results indicate that prenatal
ultrasonography lacks a strong agreement with postnatal
examinations and provides low diagnostic accuracy, it is
recommended that clinicians should explore other diagnostic
techniques to improve the accuracy of early diagnoses.
In conclusion, the results of the present study
indicate that preoperative ultrasound has poor sensitivity but very
good specificity for the diagnosis of EA/TOF. The use of ultrasound
alone would result in a high rate of a false-positive diagnoses.
However, it may be used as a preliminary screening tool to exclude
patients for suspected EA/TOF.
Acknowledgements
Not applicable.
Funding
Funding: Funding was provided by Shandong Province Traditional
Chinese Medicine Science and Technology Development Plan Project
(grant no. 2019-0478) and Jining Key R&D Plan Project (grant
no. 2019SMNS004).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CW and YD contributed to the conception and design
of the study. XN, ZZ and SW contributed to the acquisition,
analysis and interpretation of the data. CW and YD confirmed the
authenticity of all the raw data. CW drafted the manuscript and YD
revised the paper. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The Ethics Committee of the Affiliated Hospital of
Jining Medical University approved the study protocol (approval no.
JYFY-2019-17). All pregnant women provided informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Marseglia L, Manti S, D'Angelo G, Gitto E,
Salpietro C, Centorrino A, Scalfari G, Santoro G, Impellizzeri P
and Romeo C: Gastroesophageal reflux and congenital
gastrointestinal malformations. World J Gastroenterol.
21:8508–8515. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Pinheiro PFM, Simões e Silva AC and
Pereira RM: Current knowledge on esophageal atresia. World J
Gastroenterol. 18:3662–3672. 2012.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Nassar N, Leoncini E, Amar E,
Arteaga-Vázquez J, Bakker MK, Bower C, Canfield MA, Castilla EE,
Cocchi G, Correa A, et al: Prevalence of esophageal atresia among
18 international birth defects surveillance programs. Birth Defects
Res A Clin Mol Teratol. 94:893–899. 2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Tandon RK, Sharma S, Sinha SK, Rashid KA,
Dube R, Kureel SN, Wakhlu A and Rawat JD: Esophageal atresia:
Factors influencing survival-experience at an Indian tertiary
centre. J Indian Assoc Pediatr Surg. 13:2–6. 2008.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Seo J, Kim DY, Kim AR, Kim DY, Kim SC, Kim
IK, Kim KS, Yoon CH and Pi SY: An 18-year experience of
tracheoesophageal fistula and esophageal atresia. Korean J Pediatr.
53:705–710. 2010.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Valevičienė NR, Varytė G, Zakarevičienė J,
Kontrimavičiūtė E, Ramašauskaitė D and Rutkauskaitė-Valančienė D:
Use of magnetic resonance imaging in evaluating fetal brain and
abdomen malformations during pregnancy. Medicina (Kaunas).
55(55)2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Pardy C, D'Antonio F, Khalil A and
Giuliani S: Prenatal detection of esophageal atresia: A systematic
review and meta-analysis. Acta Obstet Gynecol Scand. 98:689–699.
2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Spitz L: Esophageal atresia. Lessons I
have learned in a 40-year experience. J Pediatr Surg. 41:1635–1640.
2006.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Hands LJ and Dudley NE: A comparison
between gap-length and Waterston classification as guides to
mortality and morbidity after surgery for esophageal atresia. J
Pediatr Surg. 21:404–406. 1986.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bradshaw CJ, Thakkar H, Knutzen L, Marsh
R, Pacilli M, Impey L and Lakhoo K: Accuracy of prenatal detection
of tracheoesophageal fistula and oesophageal atresia. J Pediatr
Surg. 51:1268–1272. 2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Su P, Yuan Y, Zhang Z, Huang Y and Wang W:
Application of high-frequency ultrasound in esophageal atresia with
distal fistula. Dis Esophagus. 27:325–329. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Langer J, Hussain H, Khan A, Minkes R,
Gray D, Siegel M and Ryan G: Prenatal diagnosis of esophageal
atresia using sonography and magnetic resonance imaging. J Pediatr
Surg. 36:804–807. 2001.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Spaggiari E, Faure G, Rousseau V, Sonigo
P, Millischer-Bellaiche AE, Kermorvant-Duchemin E, Muller F,
Czerkiewicz I, Ville Y and Salomon LJ: Performance of prenatal
diagnosis in esophageal atresia. Prenat Diagn. 35:888–893.
2015.PubMed/NCBI View
Article : Google Scholar
|
|
14
|
Choudhry M, Boyd PA, Chamberlain PF and
Lakhoo K: Prenatal diagnosis of tracheo-oesophageal fistula and
oesophageal atresia. Prenat Diagn. 27:608–610. 2007.PubMed/NCBI View
Article : Google Scholar
|